
Abstract
Purpose
Since protein arginine methyltransferase 5 (PRMT5) is abnormally expressed in various tumors, in this study we aim to assess the association between PRMT5 and clinicopathological and prognostic features.
Methods
Electronic databases including PubMed, Web of Science, Scopus, ScienceDirect, and the Cochrane Library were searched until July 25, 2021. The critical appraisal of the eligible studies was performed using the Newcastle–Ottawa Quality Assessment Scale. Pooled hazard ratios (HR) and pooled odds ratios (OR) were calculated to assess the effect. Engauge Digitizer version 12.1, STATA version 15.1, and R version 4.0.5 were used to obtain and analysis the data.
Results
A total of 32 original studies covering 15,583 patients were included. In our data, it indicated that high level of PRMT5 was significantly correlated with advanced tumor stage (OR = 2.12, 95% CI: 1.22-3.70, P =.008; I2 = 80.7%) and positively correlated with poor overall survival (HR = 1.59, 95% CI: 1.46-1.73, P < .001; I2 = 50%) and progression-free survival (HR = 1.53, 95% CI: 1.24-1.88, P < .001; I2 = 0%). In addition, sub-group analysis showed that high level of PRMT5 was associated with poor overall survival for such 5 kinds of cancers as hepatocellular carcinoma, pancreatic cancer, breast cancer, gastric cancer, and lung cancer.
Conclusion
For the first time we found PRMT5 was pan-cancerous as a prognostic biomarker and high level of PRMT5 was associated with poor prognosis for certain cancers.
Background
As a major public health issue, malignant tumor has become the focus of attention. The latest global cancer data showed that cancer burden rose to 19.3 million new cases and 10.0 million cancer deaths in 2020. 1 Although various therapeutic procedures appeared to control the development of cancers, the survival rates remained dismal, which might be relevant to the lack of early diagnostic and efficient prognostic biomarkers. That’s the reason why we need to develop novel molecular biomarkers for the prediction of the survival outcome for patients.
Protein arginine methyltransferases (PRMTs) are a family of enzymes that methylate the guanidino group of the arginine using S-adenosyl methionine (SAM) as a methyl donor, producing mono- or dimethylated arginine residues and S-adenosyl-L-homocysteine. 2 By altering the stability, localization, or activity of the substrate, PRMTs regulate a variety of intracellular functions that are essential for survival. 3 In addition, PRMTs are involved in cancer development through oncogenic signal transduction, cancer stem cell maintenance, and epithelial-mesenchymal transition (EMT). 4 PRMT5 belongs to the type II PRMT family which is responsible for the generation of monomethylated arginine and enantiomeric dimethylarginine. 5 Studies have shown that PRMT5 could inhibit the transcription of tumor suppressors to provide essential conditions for tumor occurrence,6,7 such as p53, cell cycle related transcription factor E2F-1, tumor suppressor gene ST7, tumor metastasis suppressor gene NM23, apoptosis related protein CASP4, etc. Moreover, studies have shown that the abnormal expression of PRMT5 is closely related to the occurrence and development of a variety of diseases, and the higher expression of PRMT5 appears in such human malignancies as breast cancer, colon cancer, lung cancer, pancreatic cancer, chronic lymphocytic leukemia, and so on.8-10 Meanwhile, high level of PRMT5 is relevant to survival outcome in cancer patients. For example, based on 118 epithelial ovarian cancer tissues, 20 benign ovarian tumor and 12 normal ovary samples, PRMT5 was reported to be highly expressed in epithelial ovarian cancer, meanwhile the level of PRMT5 was correlated with the proliferation activity and the survival of ovarian cancer patients. 11 For hepatocellular carcinoma, the members of the high-PRMT5 group were more likely to have a worse prognosis comparing with those in the low PRMT5 group (5-year overall survival rates, 53 and 76%, respectively). 12 Vinet, M. reported high-PRMT5 expression was associated with lower probabilities of overall survival but had no influence on distant metastasis‐free survival. 13
However, so far no study has systematically evaluated the clinicopathological and prognostic value of PRMT5 in cancers. In this study, we conducted the systematic analysis to evaluate the clinicopathological and prognostic value of PRMT5 in different malignant tumors, and for the first time we found PRMT5 is pan-cancerous as a prognostic biomarker.
Materials and Methods
This meta-analysis followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) criteria. 14 The protocol of this systematic review was registered on the PROSPERO—International Prospective Register of Systematic Reviews (registration number: CRD42021268881).
Study Strategy
We totally searched 5 electronic databases including PubMed, Web of Science, Scopus, ScienceDirect, and the Cochrane Library. Two independent reviewers (LIANG ZZ and MA SM) searched for literatures from January 1, 2000 to July 25, 2020, with search terms “Neoplasm”, “PRMT5,” and their entry words. Detailed search strategies were shown in Supplementary Table S1. Additionally, the references of relevant literature and Supplementary Materials were also screened manually to identify missing relevant publications.
Select Strategy
All articles were screened according to the inclusion and exclusion criteria by 2 independent reviewers. The inclusion criteria were as follows: (1) original studies; (2) papers published in English and focused on human beings; (3) studies performed to investigate the relationship between PRMT5 and any types of survival outcomes, which included overall survival (OS, period from diagnosis to death due to any reason); progression/disease free survival (PFS/DFS, period from first treatment to identification of cancer progression or death); relapse/recurrence free survival (RFS, period between cure from cancer and identification of cancer progression/recurrence), metastasis-free survival (MFS/DMFS, period from diagnosis cancer to diagnosis a (distant) metastatic event); (4) the levels of PRMT5 were measured through any quantitative analysis, and were divided into 2 levels: high and low; and (5) pooled hazard ratio (HR) and corresponding 95% confidence interval (CI) should be provided, or there should be sufficient data through which HR and 95% CI could be calculated.
The exclusive criteria were as follows: (1) studies without control groups; (2) studies using duplicated data; (3) studies unable to get full-text.
Data Extraction
Main characteristics of literatures included.
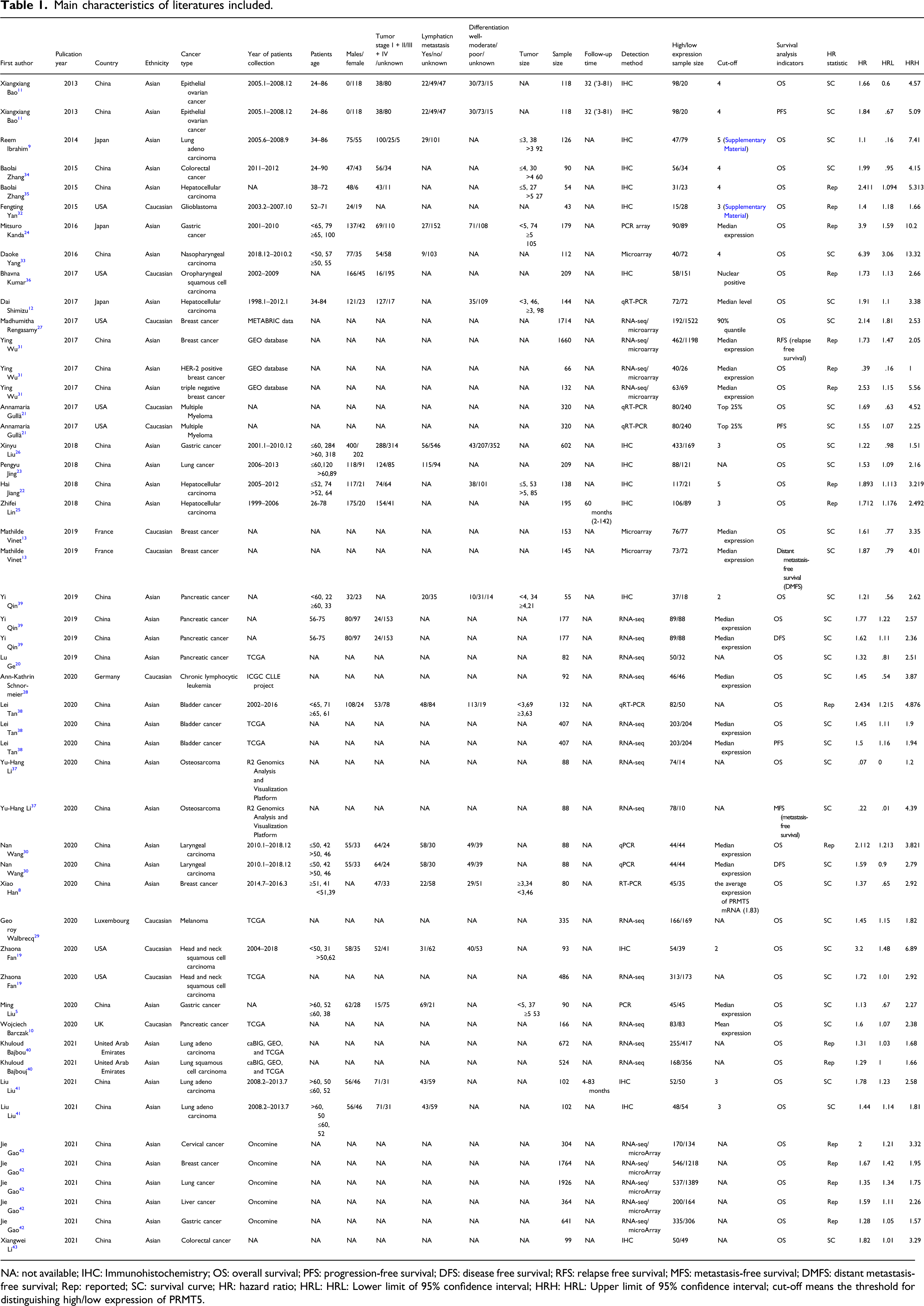
NA: not available; IHC: Immunohistochemistry; OS: overall survival; PFS: progression-free survival; DFS: disease free survival; RFS: relapse free survival; MFS: metastasis-free survival; DMFS: distant metastasis-free survival; Rep: reported; SC: survival curve; HR: hazard ratio; HRL: HRL: Lower limit of 95% confidence interval; HRH: HRL: Upper limit of 95% confidence interval; cut-off means the threshold for distinguishing high/low expression of PRMT5.
Statistical Analysis
We used pooled OR and corresponding 95% CI to estimate the relation of PRMT5 and the clinicopathological features; and used pooled HR and corresponding 95% CI to estimate the relation of PRMT5 and the survival outcomes in cancers. We extracted HRs on the basis of the methods reported in several articles.17,18 If HRs were reported in the studies, we extracted the HRs directly. If both of the data from univariate analysis and multivariate analysis could be extracted, we chose multivariate analysis to improve data accuracy. If there was no direct information about HRs, then we retrieved HRs by extracting some survival rates at specified times from Kaplan-Meier Curves using Engauge Digitizer version 12.1. When pooled HR>1, we could reach the conclusion that the aberrant level of PRMT5 was associated with poor prognosis.
As included studies showed differences in some characteristics, we used the random-effects model to calculate pooled effect sizes. Publication bias was assessed by Begg’s funnel plots asymmetry test and Egger’s test, if the Begg’s Funnel plot graphics were symmetrical and P > .05, it suggested no significant publication bias. Forest plots were used to display the results and sensitivity analyses were also performed to assess the effect of each study. Heterogeneity was evaluated by P-value of Cochran-Q test and I-square statistic. If P-value> .05 and I2 <50%, studies were thought to be free of significant heterogeneity; If P-value < .05 and I2 >50%, studies were thought to be of heterogeneity, and sub-groups analyses were performed to seek covariates that contributed to heterogeneity. Statistically significance was considered whenever P-values < .05. Engauge Digitizer version 12.1, STATA version 15.1 and R version 4.0.5 were used to obtain the data and analysis above.
Results
Study Selection
According to the search strategy, 3816 articles were found, including 387 from PubMed, 436 from Web of Science, 2017 from Scopus, 973 from ScienceDirect, and 3 from Cochrane Library. After elimination of 1159 duplications, 2657 were left. 2492 of them were removed after title and abstract scan according to inclusion and exclusion criteria. 165 of them were eliminated after full-text scan according to inclusion and exclusion criteria. 122 articles were eliminated for insufficient data. Among the left 35 articles, 3 articles could not be used to extract HRs and 95% CIs from the survival curves. Finally, 32 articles were included,5,8-13,19-43 those articles were published between January 1, 2013 and July 25, 2021. The flow diagram was shown in Figure 1. Flow diagram of the study selection in the meta-analysis.
Study Characteristic
A total of 50 studies were included in the 32 articles. Among them, 13 articles provided relatively complete clinicopathological data, which was enough to obtain a pooled OR to assess the relationship between PRMT5 and tumor stage, lymphatic metastasis and degree of differentiation.
The survival indicators involved in the 50 studies included OS, PFS, RFS, DFS and DMFS (42 studies were OS, 3 studies were PFS, 2 studies were DFS, 1 study was RFS, 1 study was MFS, and 1 study was DMFS). Of all the 50 studies, for the detection of PRMT5 16 studies used immunohistochemistry (IHC), 17 studies used PCR technology (RT-PCR, qPCR, and microarray), 11 studies used The Cancer Genome Atlas (TCGA) data which took RNA-Seq as PRMT5 detection method, 1 study used METABRIC data, 2 studies used caBIG, TCGA, and Gene Expression Omnibus (GEO) database simultaneously, and 3 studies used 26 datasets from GEO. The sample size of each study is between 43 and 1926. Among the 50 studies, 7 studies were about breast cancer, 7 studies were about lung cancer, 5 studies were about hepatocellular carcinoma, 5 studies were about pancreatic cancer, 4 studies were about gastric cancer, and so on. As for the study location, excluding studies based on TCGA, GEO, METABRIC data, caBIG data, or ICGC CLLE project, the remaining 30 studies include 20 from China, 3 from Japan, 5 from the United States, and 2 from France. Detailed information was shown in Table1 and Supplementary Table S2.
Assessment of Methodological Quality
The ranking of each study is shown in Supplementary Table S3. The NOS scores in the column titled “Comparability of Cohorts on the Basis of the Design or Analysis” indicate that some of the studies provided details regarding their design. In the studies by M Rengasamy, 27 Y Wu, 31 Lu Ge 20 , YH Li, 37 AK Schnormeier, 28 G Walbrecq, 29 W Barczak, 10 Bajbouj K, 40 and Gao J, 42 authors used RNA-Seq data from public database, such as TCGA, GEO, METABRIC data, but the authors did not provide study design of the included patients as well as the follow-up time, hence, a star could not be awarded. According to the assessment results, the studies included in this meta-analysis were considered high-quality studies.
Publication Bias and Heterogeneity
In this study, only when the number of studies on survival indicators is greater than or equal to 3, we conduct a meta-analysis. Thus, we only conducted on OS and PFS.
Publication bias was evaluated by Begg’s Funnel plot and the Egger’s test when the number of studies included was over 10. However, the number of studies on PFS was less than 10, which was not suitable for publication bias testing. Therefore, we only tested the OS publication bias. Begg’s Funnel plot graphics were symmetrical and P > .05, which suggested no significant publication bias. (Figure 2) Begg’s Funnel plot for publication bias.
For heterogeneity, there was moderate heterogeneity in OS group for I2 = 50.0% and P < .001, and no significant heterogeneity was found in the group of PFS for I2 = 0% and P = .926.
PRMT5 and Clinicopathological Parameters
Among the 32 articles, 11 articles investigated the associations between PRMT5 and tumor stage. There were 832 cases with high level of PRMT5 and 664 cases with low level of PRMT5. Of all the 832 PRMT5-overexpressed patients, 434 patients were of III-IV stage and 241 patients were of III-IV stage among 664 PRMT5 low expressed patients (Supplementary Table S2). The pooled data showed that high level of PRMT5 was significantly associated with advanced tumor stage (OR = 2.12, 95% CI: 1.22-3.70, P = .008) (shown in Figure 3A). Similarly, 11 researches investigated the associations between PRMT5 and lymphatic metastasis. And 9 researches investigated the associations between PRMT5 and tumor differentiation. The pooled results showed that PRMT5 has no significant correlation with positive lymph node metastasis and tumor differentiation (OR = 1.58, 95% CI: .97-2.59, P = .069; OR = .72, 95% CI: .39-1.33, P = .297). (shown in Figure 3B and C) Forest plot of studies evaluating the associations between the PRMT5 high level and clinicopathological and prognostic features. A. tumor stage; B. lymph node metastasis; C. tumor differentiation; D. overall survival; E: progression-free survival.
Overall Survival Analysis
There were 42 studies, comprising a total of 13371 patients, provided data for us to analyze the correlation between PRMT5 and OS. As shown in Figure 3D, the data indicated that the high level of PRMT5 had an obvious impact on OS (HR = 1.59, 95% CI: 1.46–1.73). And the pooled estimated HR for all studies showed a significant difference (z = 10.57, P < .001). The overall results suggested that high-PRMT5 expression is an indicator of poor OS in patients with cancer.
Progression-Free Survival Analysis
HRs for PFS were available in 3 studies for a total of 845 patients. As shown in Figure 3E, the data indicated that the high expression of PRMT5 had an obvious impact on PFS (HR = 1.53, 95% CI: 1.24–1.88). And the pooled estimated HR for all studies showed a significant difference (z = 4.02, P < .001). The overall results suggested that high-PRMT5 expression was an indicator of poor PFS in patients with cancer.
Sub-group Analysis for Overall Survival
The Prognostic Effects of Sub-Groups About Overexpression of PRMT5 and OS for Cancer Patients.
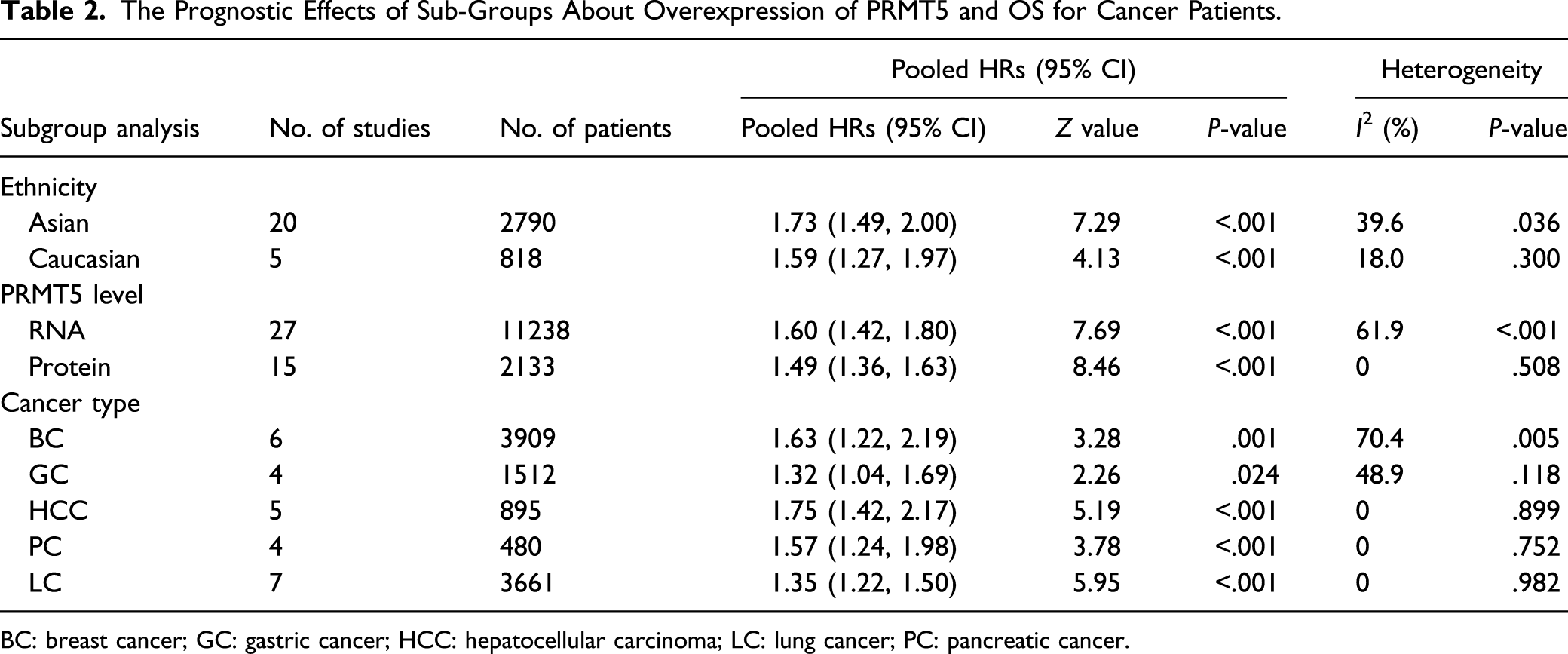
BC: breast cancer; GC: gastric cancer; HCC: hepatocellular carcinoma; LC: lung cancer; PC: pancreatic cancer.

Meta-analysis results for the overall survival of sub-groups. A: detection method; B: ethnicity; and C: different caner type.
Sensitivity Analysis
Sensitivity analysis was performed to assess the influence of sequential omission of each individual study on the overall survival. The results suggested that there was no significant influence of the pooled HR by removing any study, indicating our analysis was robust (shown in Figure 5). Sensitivity analysis for the evaluation of survival outcomes.
Discussion
Why Is PRMT5 Chosen?
PRMT5 is an enzyme which is acquiring increased prominence in cancer. 44 It is the major symmetric arginine methyltransferase in mammalian cells, and has been reported to be a novel therapeutic target molecule for human tumors. 45 PRMT5 could be regulated the expression of a wide spectrum of cellular events, including cell growth/proliferation, 46 cell invasion/metastasis, 47 epithelial-mesenchymal transition, 20 alternative splicing, 48 altering DNA replication and genomic instability 49 and dysregulation of cell cycle progression. 50 PRMT5 was considered to be involved in the occurrence and development of tumors, and high level of PRMT5 was thought to be associated with aggressive clinicopathological parameters, such as poor differentiation, higher incidence of vein invasion and larger tumor size. 51 Thus, as an oncoprotein, PRMT5 has gained increasing attention in terms of cancer prevention and therapy in recent years. Meanwhile, PRMT5 is under investigation as a potential therapeutic target for cancer in clinical practice. 8 In addition, we also found that the level of PRMT5 in whole blood is related to the prognosis of liver cancer in our multi-center study of liver cancer cases. Considering the important role of PRMT5, we searched for studies on PRMT5 and found that there are many literatures reporting the relationship between PRMT5 and clinical features or patient survival outcomes, then we did this systematic review and meta-analysis to clarify the relationship between the level of PRMT5 and the clinicopathological features and prognostic value of patients with tumors comprehensively and systematically.
What Did We Find and the Significance of the Phenomena
In this study, we included 32 articles with a total of 15583 patients to clarify the relationship between PRMT5 and tumor prognosis. We confirmed that (1) there were remarkable positive associations between PRMT5 and advanced clinical tumor stage; (2) high level of PRMT5 was related to poor OS and PFS, and increased the risk of death in cancer patients. These results indicated that PRMT5 might serve as a clinicopathological and prognostic biomarker for malignancy. Furtherly, by sub-group analysis, we found that in breast cancer, the relationship between PRMT5 and tumor prognosis is quite heterogeneous and it has good consistency in the prognosis of liver cancer, pancreatic cancer and lung cancer. Through tracing the original researches, the main reason, to some extent, attributes to sub-types of breast cancer. Some of the included literatures are for triple negative breast cancer, some are HER-2 positive breast cancer, and some do not specifically list the sub-types; in addition, PRMT5 expression based on protein level detection, compared with RNA level, has a more consistent effect on the prognosis of cancer patients, which might be derived from the reason that the detection of RNA are diverse (RNA-Seq, qPCR, RT-PCR, and microarray) and the detection results have a wide distribution range, while protein detection has only one method of IHC, and the score distribution range is narrow. All in all, these results indicated that PRMT5 might serve as a clinicopathological and prognostic biomarker for malignancy, but the detection method of PRMT5 and tumor types, especially breast cancer subtyping, have a great impact on the relationship between PRMT5 and OS.
As above-mentioned, tumors are still a major global public health problem. With the development and the advancement of medicine, cancer treatment methods have become more diverse, but the incidence and mortality of malignant tumors have not been well controlled. From 10 million new cases, 6 million deaths, and 22 million people living with cancer in 2000 52 to an estimated 19.3 million new cancer cases and almost 10.0 million cancer deaths occurred in 2020, 1 cancer is still the main killer threatening the lives and health of all human beings. The proposal of precision medicine makes clinicians pay more attention to individualized prevention, treatment and disease monitoring. This requires more biomarkers to feed back the patient’s condition in a timely and effective manner, and to change prevention or treatment measures as soon as possible. In our study, by summarizing the data of various original studies, we have clarified that the high level of PRMT5 is related to tumor stage, poor OS and PFS. This provides a basis for tumor monitoring.
Possible Mechanism of PRMT5 as a Tumor Biomarker
There is evidence indicating that PRMT5 can silence tumor suppressor genes and act as an oncogene, accelerating tumor growth and metastasis. 23 This may explain why PRMT5 can act as a biomarker for advanced stage tumors and lymphatic metastasis. Mechanistically, PRMT5 is a pleiotropic enzyme involved in diverse processes. (1) It is an established regulator of RNA biogenesis, in particular RNA splicing, which frequently becomes aberrant in cancer. 10 For example, PRMT5 regulates DNA repair by controlling the alternative splicing of histone-modifying enzymes 53 ; PRMT5 deficiency mainly interferes with the deletion of introns. This impaired splicing affects proliferation genes, meanwhile, its down-regulation is consistent with cell cycle defects and apoptosis. 54 (2) PRMT5 performs its function mainly through epigenetic silencing or direct methylation of histone and non-histone molecules, 55 thereby regulating cellular processes, including transcription, proliferation, apoptosis and metabolism. 56 For example, PRMT5 regulates cell invasion by inducing transcriptional activation and inhibition through methylating histones H3 and H4 57 ; PRMT5 enhances the methylation of PDCD4, thereby promoting tumor cell viability, allowing the tumor to grow more aggressively 58 ; Inhibition of PRMT5 changes the methylation status of E2F-1, leading to attenuated DNA damage repair, cell cycle arrest, and increased apoptosis flux 59 . In addition, as a co-factor in a DNA damage responsive co-activator complex that interacts with p53, PRMT5 is responsible for methylating p53. PRMT5 depletion triggers p53-dependent apoptosis. 60
Above all, PRMT5 is related to cell death, overexpression of PRMT5 enhances the cell proliferation and weakens the ability of apoptosis, and high level of PRMT5 is associated with poor prognosis, which makes PRMT5 a potential prognostic biomarker.
Limitations
There are several limitations in this study that should be acknowledged. Firstly, the articles included in the meta-analysis were from only 5 available databases (PubMed, Web of Science, Scopus, ScienceDirect, and Cochrane Library) and limited to written in English, thus, the data collection might be incomplete. Although we tried to include all published literatures, and there was no significant publication bias, most of the articles included were from Asian, which might attribute to the decreased generality and heterogeneity; Secondly, different criteria were applied in these studies for defining PRMT5 high or low level, because of the lack of uniform cut-off values in PRMT5 detection. This makes it impossible for us to give a clear threshold for distinguishing high level of PRMT5 in our study; Thirdly, HRs with 95% CIs were calculated by digitizing and extracting from the survival curves in most of the including papers, which inevitably brought minor statistical deviations. Furthermore, the effects of some factors, such as treatment strategy and family history, were not considered in this analysis due to the insufficient data. Therefore, high-quality studies are urgently needed to draw more accurate conclusions.
Our meta-analysis provided credible evidence that high level of PRMT5 was significantly related to advanced tumor stage and the poor prognosis for cancer patients. In addition, given the important prognostic factor of survival for cancer patients, PRMT5 might serve as an attractive therapeutic target in the treatment of malignant tumors.
Conclusion
For the first time we found PRMT5 was pan-cancerous as a prognostic biomarker, and high level of PRMT5 was associated with poor prognosis for certain cancers.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748211050583 – Supplemental Material for Clinicopathological and Prognostic Significance of PRMT5 in Cancers: A System Review and Meta-Analysis
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211050583 for Clinicopathological and Prognostic Significance of PRMT5 in Cancers: A System Review and Meta-Analysis by Zhenzhen Liang, Lianchang Liu, Chaowei Wen, Heya Jiang, Tianxia Ye, Shumei Ma and Xiaodong Liu in Cancer Control
Footnotes
Author Contributions
Liang Z was in charge of the writing of manuscript. Liu L and Wen C were in charge of editing the manuscript. Jiang H and Ye T were in charge of data analysis. Ma S was in charge of the revision of manuscript. Liu X conceived and designed this study, reviewed the manuscript and was responsible for the overall content as guarantor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (81972969, 81872558, 81773363, and 81673092). The funding body had no role in the design of the study, collection, analysis, and interpretation of the data, or preparation of the manuscript.
Ethical approval
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.