
Abstract
Background:
Breast self-examination (BSE) is one of the most feasible methods of screening for early stages of breast cancer. However, the practice rate is insufficient in many low and middle-income countries including Ethiopia. Hence, this study aimed to estimate the pooled prevalence of BSE practice among female university students in Ethiopia.
Methods:
PubMed, Cochrane Library, Scopus, and Google Scholar were searched for studies that assessed BSE practice among female students in Ethiopian universities. The study included articles published from January 1st, 2010 to June 16th, 2020. The Cochran’s Q chi-square and the respective I2 test statistics were used to check heterogeneity among the included studies. To assess publication biases, the funnel plot and Egger’s regression tests were employed. Subgroup analysis was done by using different characteristics of studies. Sensitivity analysis was also run to assess the effect of a single study on the pooled outcome. STATA™ Version 14 software packages were employed for data analysis.
Results:
Sixteen (n = 16) studies with 5,743 participants were included to estimate the pooled prevalence of BSE practice. The prevalence of regular BSE practice reported in the studies ranges from 0% to 26.4%. The estimated pooled prevalence of regular BSE practice among university students in Ethiopia is 11.23% which is very low. The prevalence of BSE practice was high, 13.6% in studies published before 2015, 12.0% among health science students, and 12.6% in studies with a sample size of 384 participants and above. In addition, the estimated pooled prevalence of irregular self-breast-examination practice was 33.28%.
Conclusion:
The rate of BSE practice among female university students is low. Thus, awareness strategies need to be designed to increase the practice rate among women in the country as BSE is one of the most feasible strategies in early detection of breast cancer if properly implemented.
Background
Breast cancer is one of the most common types of cancer and the leading cause of cancer-related deaths among women worldwide. There were an estimated 1.7 million breast cancer cases and 521,900 deaths due to the disease in 2012. This accounted for 25% of all the cancer cases and 15% of cancer-related deaths. 1,2 In 2013, there were an estimated 1.8 million new breast cancer cases and 464,000 deaths worldwide. 3
Breast cancer mortality burden is very high in many LMICs and it accounts for around 70% of the deaths. 4 Breast cancer accounts for 1 in 10 of all the new cases of cancers diagnosed worldwide each year. In addition, it is also the main cause of death among women from cancer-related deaths on the global level. 5
The incidence of female breast cancer is increasing in low and middle-income countries (LMICs) including Africa due to the increasing trends of urbanization and Western lifestyles. 4,6 On the other hand, its burden is reduced in developed countries. 7 Its nature of early detectability and the high probability of curability has been mentioned as the major reasons for the reduction in the burden of breast cancer in developed countries. 8
In contrast, women in LMICs almost always present with the advanced stages of breast cancer. As a result mortality rate from breast cancer is high in these countries indicating an intense need in promoting breast cancer screening and early detection programs. 9 There are various proven and cost-effective interventions for early detection and treatment of breast cancer. However, the high burden of breast cancer among women in low resource settings receives less community support, funding, and government attention in many LMICs compared to high-income countries. 10,11
Sufficient referral system, diagnosis, and treatment programs are recommended to be in place before the development of any type of early detection tests to ensure whether high-risk groups of women identified through the screening and early detection programs have had access to the high-quality diagnostic services including imaging and pathologic tests or not. 9 However, access to breast cancer screening and other prevention programs is beyond reach for many women and most die from the advanced stage of the disease. 12,13 These inequalities indicate the need for LMICs to invest in the early detection and control programs of breast cancer. 13
Investing in health care for women is also an investment in the development of nations and their futures. 14 However, interventions on breast cancer are not adequately translated into actions in LMICs. 15,16 The discrepancies in breast cancer screening and other prevention programs might be justified by the existence of multiple health problems among women in many LMICs that need priority when compared with breast cancer. 7,11
Mammographic screening, clinical breast examination, and BSE are some of the interventions for early detection of breast cancer and decreasing breast-cancer related mortality in developing countries. 17 However, BSE remains an important method of screening to consider especially in resource-limited settings due to its feasibility nature. 17,18
Nevertheless, awareness programs on breast cancer screening and other prevention methods are nonexistent and, or limited in many LMICs resulting in a low prevalence of knowledge or compliance with the screening. For example, 75% of the women perform BSE in the United States, in contrast only 30.3% of the females from Saudi Arabia had heard about it. 19 Furthermore, a study published in 2012 has indicated that only 2.2% of 40-69 years aged women had received breast cancer screening in developing countries. 20
The low rate of BSE practice in LMICs is suggested to be related to a lack of knowledge about the methods of breast cancer screening. Hence, BSE practice among women requires enhanced awareness creating campaigns, and building a positive attitude towards it emphasizing its benefit of detecting early stages of breast cancer. 21
Family history, nulliparity, early age at menarche, alcohol drinking, physical inactivity, overweight/obesity, the use of exogenous hormones such as oral contraceptives and menopausal hormone replacement therapy are some of the known risk factors that can increase the risk of breast cancer among the young and older women. 22,23
Female students are one of the primary targets for sexual and reproductive health services in Ethiopia. 24 Cancer prevention and treatment is also one of the components in sexual and reproductive health services. 25 Therefore, people might expect that as a target group university students will have a better BSE practice.
However, findings from small studies on the prevalence of BSE practice among female university students in Ethiopia are inconsistent. The prevalence of regular BSE practice among university students reported in the country ranges from 0% 26 to 26.4%. 27 Hence, this systematic review and meta-analysis aimed to determine the pooled prevalence of BSE practice among university students in Ethiopia.
Methods
Literature Search Strategy
Firstly, Joanna Briggs Institute (JBI), the Cochrane Library, and PROSPERO databases were searched to check whether a systematic review and meta-analysis studies exist or for the presence of ongoing projects related to BSE among female university students in Ethiopia. The articles included in this study were retrieved using PubMed, Scopus, Google Scholar, and African journals online.
The following key terms were used to identify the necessary articles: “Breast self-examination,” “self-breast examination,” “practice,” “factors,” “university” and “students.” The Boolean operators of “OR” and “AND” were used to combine the key terms. Grey literature’s like academic dissertations, surveillance reports, and conference proceedings were also included. In addition, an ancestry approach that is the reference lists of included articles in this systematic review and meta-analysis were hand-searched to identify the presence of any relevant additional articles.
Eligibility Criteria
Studies were included in this systematic review and meta-analysis if they followed the following guidelines: (1) all observational study designs (cross-sectional, case-control, and cohort studies) that reported the prevalence of BSE practice among female university students; (2) published from January 1, 2010 to June 16, 2020; (3) published in the English language; (4) abstract and, or full text available for the review process; and (5) conducted in Ethiopia. Studies were excluded if they: (1) possessed a poor quality score as per the JBI’s quality assessment criteria; and (2) failed to report the desired outcome (BSE practice among female university students in Ethiopia).
Outcomes of Interest
The main outcome of interest was the prevalence of BSE among female university students reported in the original papers either as a percentage or as the number of cases (n)/total number of study participants (N). These 2 parameters were necessary to calculate the pooled prevalence of BSE practice among university students in the meta-analysis. Therefore, in situations, where the included studies fail to report the prevalence of BSE practice in percentage, the prevalence rate was calculated by dividing the number of individuals who practiced BSE by the total number of study participants (sample size) multiplied by 100.
The outcome variable of interest that is BSE practice was categorized as regular and irregular. Regular BSE practice is the regular examination of once own breasts monthly to detect lumps or other changes that may need to be further evaluated as part of screening for early detection of breast cancer. On the other hand, BSE was leveled as irregular if it is not performed monthly or if it is performed sporadically. 28
Data Extraction
First, a data extraction platform was developed on the excel sheet by the authors. The author’s name, year of study, publication year, study design, and population were included in the platform in consideration of health and non-health-related fields, sample size, and prevalence of BSE practice among female university students. The data extraction sheet was piloted using 5 randomly selected papers. Then, the extraction form was adjusted after having the piloted template of the 5 studies.
All the necessary data were extracted from each study using the data extraction format by 2 of the authors independently. The correctness of the data extracted by the first 2 authors was also checked by the third author independently. When any disagreement was raised between the authors who extracted the data, it was resolved through discussions with the third reviewer and fourth reviewer.
Quality Assessment
Two authors assessed the methodological quality of all of the potential studies independently. Disagreements in assessing the methodology quality of articles between the authors were resolved through discussion. In case when a consensus was not reached between the first 2 authors, a third independent was involved in consultation with the author. The quality of each article included in this study was assessed using the JBI quality appraisal checklist for cross-sectional studies. 29 Additional details are available somewhere else. 30
Patient and Public Involvement
No patient or public was involved.
Statistical Analysis
The pooled prevalence of BSE practice among female university students in Ethiopia was estimated using the random-effects model meta-analysis. 31 Cochran’s Q chi-square statistic and the I 2 tests were run to assess the random variations between the primary studies. 32 Subgroup and sensitivity analyses were run to identify the possible sources for the heterogeneity. Additional details about the methods of analysis are found somewhere else. 30
Publication Bias
The techniques of avoiding publication biases such as identifying and including unpublished studies, conference proceedings, and academic dissertations were considered and included. In addition, potential publication biases were assessed by visually inspecting the funnel plots that is the distribution of the included studies on the funnel plot and objectively by using Egger’s bias tests. 33 The trim and fill analysis was also done to assess for and adjust any publication biases based on the assumption that the effect sizes of all the studies regarding the prevalence of BSE practice and the effect of knowledge on it among female university students in Ethiopia are normally distributed around the center of a funnel plot in the absence of publication biases. 34 The meta-analysis was performed using the STATA™ Version 14 software program. 35 A P-value of less than 0.05 was considered to declare statistically significant values.
Presentation and Reporting of Results
The results of this systematic review and meta-analysis are reported based on the Preferred Reporting Items for Systematic Review and Meta-Analysis statement (PRISMA) guideline. 36 The entire process of study selection, screening, inclusion, and exclusions are shown with the support of a PRISMA flow diagram.
Results
Search Results
Eighty-five (85) articles were retrieved from various international databases and gray literature. In the first step, 73 studies that were published from 2010-2020 were retrieved from 4 international databases. Thirty-one (31) of them were retrieved from the PubMed database and the remaining 30 were retrieved from the other 3 databases. On the other hand, 12 studies were accessed from other sources including gray literatures.
Among the 85 retrieved articles, 16 duplicate records were identified and after removing the duplications, a total of 69 articles have remained for screening. Then, from the 69 remained articles, 51 studies were excluded after reading their title and, or the abstract. The articles were excluded if they fail to report the desired outcomes or were not conducted in Ethiopia.
Finally, 18 studies were screened for full-text review and, 16 articles (n = 5,743 participants) were selected to estimate the pooled prevalence of BSE practice among female university students in Ethiopia. The remaining 2 studies were excluded because only the abstract part of conference proceedings was available online for these articles, and the authors failed to respond and provide the full text for the author’s 2 consecutive email requests. The detailed steps in the screening, inclusion, and exclusion process of studies are shown in the PRISMA flow chart of the study selection (Figure 1).

PRISMA flow chart of study selection for the prevalence of BSE practice among female university students in Ethiopia.
Baseline Characteristics of Included Studies
In this meta-analysis, 16 studies with 5,743 study participants were included to estimate the pooled prevalence of BSE practice among female university students in Ethiopia. All of the studies included in this review were cross-sectional. The studies included in this systematic review and meta-analysis vary significantly in terms of sample size ranging from 61, the smallest 37 to 803, the largest. 38
Overall information regarding the prevalence of BSE practice among female university students was obtained from various provinces of Ethiopia. Four of the studies were conducted in universities found in the Amhara region, 38 -41 3 from SNNPR, 37,42,43 7 from Oromia, 26,44 -49 1 from Tigrai universities, 27 and 1 from Addis Ababa University. 50
Regarding sampling, all of the studies had used the probability sampling technique. Moreover, the quality score of each study evaluated based on the JBI’s quality appraisal criteria for cross-sectional studies showed no considerable risk of biases. Hence, all the articles were included in this systematic review and meta-analysis (Additional file 1).
The Pooled Prevalence of Regular BSE Practice
Fifteen studies (n = 15) had reported the prevalence of regular BSE practice among female university students in Ethiopia (Supplemental file). The prevalence of regular BSE practice reported in the studies included in this systematic review and meta-analysis ranges from 0% 26 to 26.4%. 27 In this meta-analysis, the random-effects model analysis revealed that the estimated pooled prevalence of regular BSE practice among university students in Ethiopia was 11.23% (95% CI: 7.67, 14.78) but with a significant level of heterogeneity among the studies (I 2 = 97.4%; P ≤ 0.001) (Figure 2).

Forest plot for the prevalence of regular BSE practice.
The Pooled Prevalence of Irregular BSE Practice
Sixteen studies (n = 16) had reported the prevalence of ever practicing BSE among the students in the universities of Ethiopia (Supplemental file). The prevalence of irregular BSE practice reported in the universities ranges from 15.5% 44 to 83.4%. 51 In the random-effects model analysis, the estimated pooled prevalence of irregular practicing of BSE among university students was 33.28% (95% CI: 25.09, 41.48) but with a high level of heterogeneity among the studies (I 2 = 98.0%, P ≤ 0.001) (Figure 3).

Forest plot for the prevalence of irregular BSE practice.
Subgroup Analysis
Subgroup analysis was done through stratification using study year, participant’s discipline, and sample size due to the presence of a high level of heterogeneity among the primary studies included in this systematic review and meta-analysis. In the subgroup analysis, the prevalence of regular BSE practice among the students in the universities of Ethiopia was found to be higher in studies published before 2015 (13.58%), with 11.96% in studies conducted among health science students, and 12.56% in studies with a sample size of 384 participants and above compared to their counterparts in the subgroup.
Similarly, the prevalence of irregular BSE practice was found to be 33.5% in studies published since 2015, with 34.14% in studies conducted among health science students only, and 35.88% in studies conducted with a sample size of 384 participants and less (Table 1).
BSE Practice Prevalence After Subgroup Analysis by the Study Characteristics Included.

Abbreviation: BSE, Breast Self-Examination.
Sensitivity Analysis for Regular BSE Practice
A sensitivity analysis was done using the random-effects model for the purpose of evaluating the effect of individual studies on the pooled prevalence of regular BSE practice. However, the result has revealed that no single study has influenced the pooled estimated prevalence of regular BSE practice among universities in Ethiopia. The pooled estimated prevalence of regular BSE practice among university students in Ethiopia varied between 9.96% (95% CI: 6.94, 12.98)
27
and 12.07% (95% CI: 8.28, 15.85)
26
after the deletion of a single study

Sensitivity analysis of the 15 studies in the meta-analysis of regular BSE practice.
Sensitivity Analysis for Irregular BSE Practice
A sensitivity analysis done using the random-effects model to check the effect of individual studies on the pooled prevalence of irregular BSE practice has revealed that no study has influenced the pooled estimate of irregular BSE practice among university students in Ethiopia. The pooled estimated prevalence of irregular BSE practice ranged from 29.91% (95% CI: 24.17, 35.64)
51
to 34.49% (95% CI: 26.10, 42.88)
44
after the deletion of a single study

Sensitivity analysis of the 16 studies in the meta-analysis of irregular BSE practice.
Publication Bias Assessment
There was a publication bias among the included studies in the prevalence of both regular and irregular BSE practices among university students as elucidated by the asymmetrical distribution of the funnel plot tests (Figures 6 and 7).
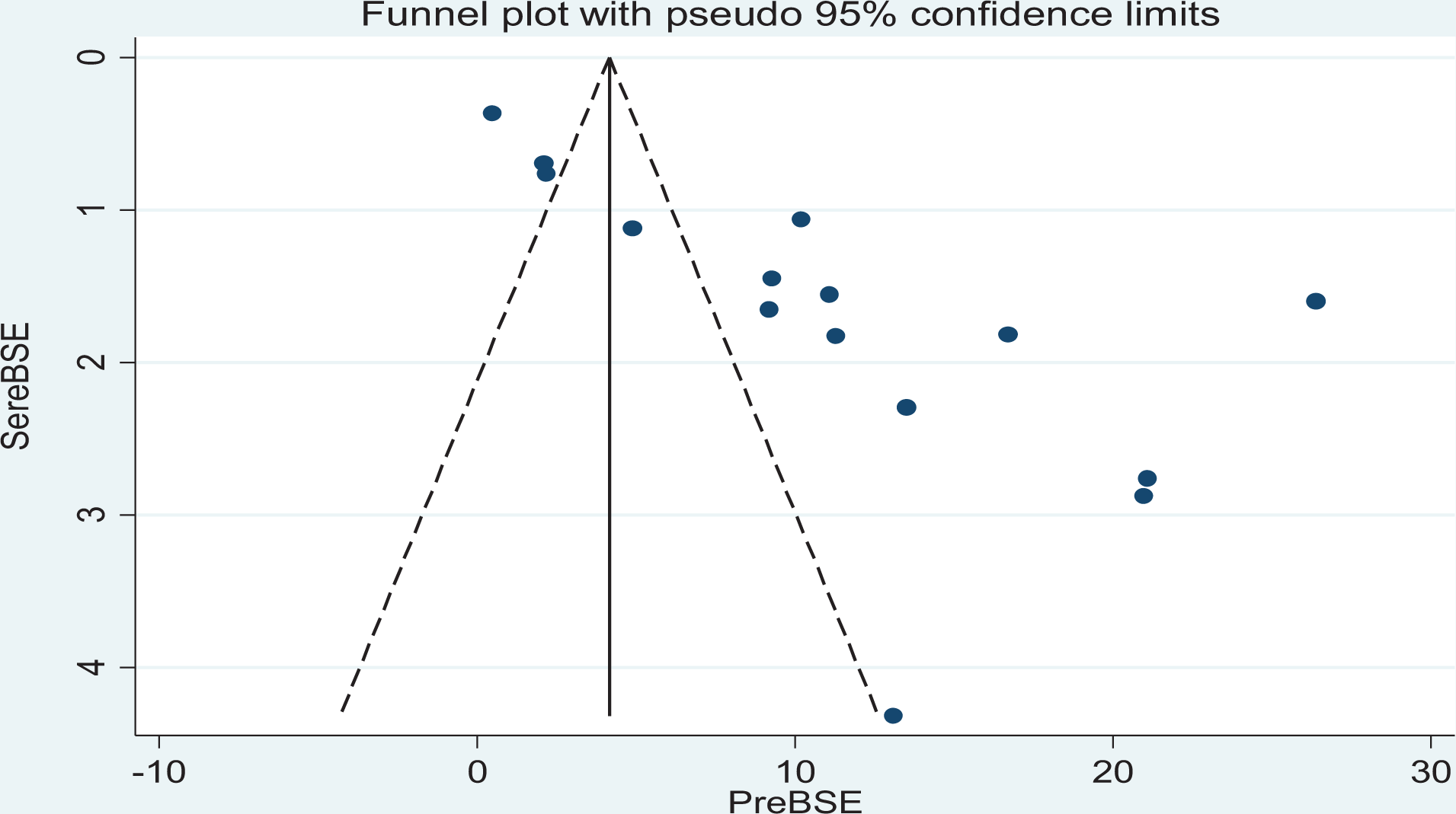
Distribution of studies included in regular BSE practice analysis.

Distribution of studies included in irregular BSE practice analysis.
Publication Bias Test for Regular BSE Practice
In addition to the subjective tests, the result of Egger’s test for the funnel plot was statistically significant for the presence of publication bias for regular BSE practice among university students in Ethiopia (P ≤ 0.001) (Figure 8).

Egger
Publication Bias Test for Irregular BSE Practice
Unlike, the regular BSE practice, the result of the Egger’s test for the funnel plot has shown that no publication bias was found in the studies included to estimate the pooled prevalence of irregular BSE practice among university students in Ethiopia (P = 0.588) (Figure 9).

Egger’s test of publication bias for studies in irregular BSE practice.
Trim and Fill Analysis
The trim and fill analysis were done for estimation of the number of missing studies that might exist due to publication biases for regular BSE practice among the students. However, during analysis, no study was imputed for missing studies. After adjustment for the publication bias, the estimated pooled prevalence of regular BSE practice among female university students in Ethiopia appeared to be the same with the unadjusted prevalence rate that is 11.23% (95% CI: 7.67, 14.78) but with a moderate level of heterogeneity among the included studies (I 2 = 45.72%; P ≤ 0.001) (Figure 10).

Trim and fill analysis for the prevalence of regular BSE practice.
Discussion
In this systematic review and meta-analysis, the prevalence of regular BSE practice reported in the studies included ranges from 0% 26 to 26.4%. 27 This discrepancy might be due to differences in the study period because unlike the first study which was conducted after 2015, the second study was done before 2015. This finding is supported by subgroup analysis using study year which has indicated that the pooled prevalence of regular BSE practice among university students was higher in studies conducted before 2015 compared with the studies conducted since 2015. This might perhaps suggest that the awareness programs towards BSE screening tests are not reaching the university students. Furthermore, awareness programs about BSE in Ethiopia are insufficient.
The prevalence of irregular BSE practice reported in the universities ranges from 15.5% 44 to 83.4%. 51 This difference might be due to differences in the discipline of the study participants among the studies. Unlike the first study which was conducted in both health science and non-health science students, the second study was conducted only among health science students who are expected not only to do BSE but also to teach others about it. Furthermore, enhancing breast cancer awareness and practical skills among health care workers can also serve as a major tool in improving BSE practice awareness among the general population. 52
Regarding the pooled estimate, the random-effects model analysis has revealed that in this meta-analysis the estimated pooled prevalence of regular BSE practice among female university students in Ethiopia was 11.23%. This finding is in line with a study finding among female university students across 24 LMICs which has reported that 9.1% of students were practicing BSE monthly. According to the study, the higher practice of monthly BSE (above 20%) was observed in Nigeria and Laos, and the lowest that is below 2% in India, Singapore, Russia, Bangladesh, and South Africa. 53 This difference might emanate from the countries' health care policy because it is known that cancer in general is not a priority health problem for many LMICs. 54,55
However, it is lower than a study conducted at a Ugandan University which has revealed that 14% of female university students performed BSE regularly. 56 It is also lower than other studies conducted in LMICs, 17.4% in Yemen, 57 19.0% in Nigeria, 58 31% in Ghana, 59 and 45.4% in Greece. 60 These variations might be due to differences in the discipline of study participants, the countries’ health care policy, and the developmental level of the countries. For example, the Greece study was conducted among midwifery professionals who have an intense background on BSE techniques and its benefits in the early detection of breast cancer cases. 60
In addition to regular BSE practice, the prevalence of irregular practicing of BSE among the students in the universities of Ethiopia was determined using the random-effects model. The prevalence of irregular BSE practice reported in the universities ranges from 15.5% 44 to 83.4%. 51 In this meta-analysis, the estimated pooled prevalence of ever practicing BSE among university students was 33.28%. This finding is consistent with the study finding of the Ugandan study that 30% of the participants had ever performed BSE irregularly. 56 Similarly, the study conducted among female university students across 24 LMICs has indicated that 31.6% of the students had irregular self-breast-examination practices. 53
A significant level of heterogeneity was found between the primary studies included in this systematic review and meta-analysis. As a result, subgroup analysis was done by stratifying the studies using study year, participant’s discipline and sample size to identify the sources of heterogeneity for the prevalence of BSE practice among female university students in Ethiopia. In the subgroup analysis, the prevalence of regular BSE practice among the students in the universities of Ethiopia was found to be higher (13.58%) in studies published before 2015 and with health science students. Similarly, the prevalence of irregular BSE practice was found to be a little bit higher (33.5%) in studies published since 2015 and 34.1% among health science students only.
These differences in the prevalence of BSE practice among students might be due to differences in the knowledge of study participants because health science students are the first beneficiaries in getting knowledge regarding breast cancer early detection methods. A systematic review conducted on health promotion interventions aiming to increase breast cancer screening utilization including BSE has revealed that the majority of the studies included in the review showed promising results after the health promotion programs including improvements in the women’s knowledge and view of breast screening and BSE practices. 61
Strength and Limitation of the Study
The study has used pre-specified protocols for searching strategy and data abstraction. Furthermore, internationally accepted tools were also used for critical appraisal of individual studies. However, 2 studies were excluded after the authors failed to respond to our 2 consecutive requests for the full text for their articles. Hence, the exclusion of the 2 articles may affect the pooled outcomes of this study.
Conclusion
The prevalence of BSE practice among female university students is low in Ethiopia compared with developed and some developing countries. Furthermore, the rate of regular breast self-examination practice is very low compared with the irregular practice rate. Therefore, awareness strategies need to be designed to increase the practice of breast self-examination among university students in the country as breast self-examination is the most feasible strategy in early detection of breast cancer if properly implemented.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211019137 - Breast Self-Examination Practice Among Female University Students in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211019137 for Breast Self-Examination Practice Among Female University Students in Ethiopia: A Systematic Review and Meta-Analysis by Ayelign Mengesha Kassie, Biruk Beletew Abate, Mesfin Wudu Kassaw and Wondimeneh Shibabaw Shiferaw in Cancer Control
Footnotes
Authors’ Note
The data used during this systematic review and meta-analysis is available within the article and the supporting file. AMK and BBA developed the study protocol and were involved in the design, selection of study, data extraction, statistical analysis, and writing the initial drafts of the manuscript. MWK and WSS were involved in data extraction, quality assessment, statistical analysis, and revising. AMK and BBA prepared and edited the final manuscript. All authors have read and approved the submission of the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.