
Abstract
Background:
Race, gender, insurance status, and income play important roles in predicting health care outcomes. However, the impact of these factors has yet to be fully elucidated in the setting of hepatocellular carcinoma (HCC).
Methods:
We designed a retrospective cohort study utilizing data from the Surveillance, Epidemiology, and End Results (SEER) program to identify patients diagnosed with resectable HCC (N = 28,518). Demographic factors of interest included race (Asian/Pacific Islander [API], African American [AA], Native American/Alaska Native [NA], or White [WH]) and gender (male [M] or female [F]). Insurance classifications included those having Medicare/Private Insurance [ME/PI], Medicaid [MAID], or No Insurance [NI]. Median household income was estimated for all diagnosed with HCC. Endpoints included: (1) overall survival; (2) likelihood of receiving a recommendation for surgery; and (3) specific surgical intervention performed. Multivariate multinomial logistic regression for relative risk ratio (RRR) and Cox regression models were used to identify pertinent associations.
Results:
Race, gender, insurance status, and income had statistically significant effects on the likelihood of surgical recommendation and overall survival. API were more likely to receive a recommendation for hepatic resection (RRR = 1.45; 95% CI: 1.31-1.61; Reference Race: AA) and exhibited prolonged overall survival (HR = 0.77; 95% CI: 0.73-0.82; Reference Race: AA) as compared to members of any other ethnic group; there was no difference in these endpoints between AA, NA, or WH individuals. Gender also had a significant effect on survival: Females exhibited superior overall survival (HR = 0.89; 95% CI: 0.85-0.93; Reference Gender: M) as compared to males. Patients who had ME/PI were more likely than those with MAID or NI to receive a surgical recommendation. ME/PI was also associated with superior overall survival. Conclusions: Race, gender, insurance status, and income have measurable effects on HCC management and outcomes. The underlying causes of these disparities warrant further investigation.
Introduction
Hepatocellular carcinoma (HCC) is responsible for significant morbidity and mortality worldwide, representing the sixth most commonly diagnosed cancer and fourth leading cause of cancer-related death. 1 In the United States, the incidence rate of HCC has increased nearly 5-fold over the past 40 years, from 1.4/100,000 cases/year in the 1970s to 6.2/100,000 cases in 2011. 2 Several populations are known to be dispoportionately affected by HCC: Asians, males, and low income individuals. 3 -5 Fortunately, patient outcomes are steadily improving across all demographics; 5-year survival rates have increased by greater than 60% since 1975. 3
The most common global risk factor for HCC is the hepatitis B virus (HBV). In the United States, the hepatitis C virus (HCV) represents the most common causative agent. The distribution of HCC parallels that of hepatotropic viruses, and thus the disease burden is highest in areas with endemic HBV infection, such as Eastern Asia and sub-Saharan Africa. 6 Other common risk factors include alcohol-related cirrhosis, nonalcoholic fatty liver disease (NAFLD), obesity, and diabetes. 7 Prognosis is largely dependent on the stage at diagnosis and can be improved with early detection. In the United States, 5-year survival is approximately 38%, 36%, 26%, and 19% for American Joint Committee on Cancer (AJCC) stage IA, II, IIIA, and IIIB disease, respectively. 8 Surgical resection/ablation and liver transplantation represent the mainstays of treatment for non-metastatic disease and the best interventions to ensure long-term survival. However, the majority of affected individuals are ineligible for operative management due to impaired liver function and/or delayed diagnosis. 9
Sociodemographic factors are important predictors of HCC incidence and outcomes. Asians and Pacific Islanders are the most frequently affected ethnic groups, and males are 2 to 4 times more likely than females to receive a diagnosis of HCC. 3,4 There is also a strong negative correlation between income and the risk of developing HCC; it has been hypothesized that this reflects the prevalence of HCC risk factors—such as hepatitis infection, alcoholism, and obesity—among those of low income. 5 Furthermore, insurance status has a significant effect on HCC management, as patients with private insurance are more likely to undergo curative therapies as compared to those with Medicaid. 10 The relationship between sociodemographic characteristics and HCC outcomes is complex and nuanced, however. We therefore sought to examine the effects of race, gender, insurance status, and income on both the approach to management and overall survival among individuals with HCC in the United States.
Materials and Methods
This is a retrospective cohort study using the Surveillance, Epidemiology, and End Results (SEER) database from all the registries captured in the SEER 18 program. The SEER program collects and publishes cancer incidence and survival data using population-based cancer registries that include approximately 38% of the population of the United States. Information on patient demographics, tumor sites, tumor morphology, staging, surgical treatment, and follow-up is publically available. SEER site code C22.0 was used to identify patients who received a histologic diagnosis of HCC between January 1, 2007 and December 31, 2015.
The SEER registries continuously code and submit AJCC 6th and 7th edition stages for all cancers diagnosed in 2010 and beyond. Patients diagnosed before 2010 are staged using the AJCC 6th edition only. Therefore, the AJCC 6th edition was used in order to include all patients diagnosed between 2007 and 2015. Eligibility criteria included an age of 18 years or older and a diagnosis of clinical stage I, II, or IIIA HCC. Individuals with unresectable tumors—stage IIIB (defined as having invaded the portal or hepatic vein) and stage IV HCC—were excluded from the analysis. Exclusion criteria are further detailed in Figure 1.

Eligibility and exclusion criteria. Eligiblity criteria included an age of 18 years or older and a diagnosis of stage I, II, or IIIA HCC. Individuals with unresectable tumors—stage IIIB (defined as having invaded the portal or hepatic vein) and stage IV HCC—and those who had previously been diagnosed with other cancers were excluded from the analysis.
The American Community Survey (ACS) database was used for the analysis of patient educational level and median household income. Educational level was calculated using county-level data obtained between 2012 and 2016 that detailed the percentage of individuals who had less than a high school education; this was divided into quintiles. Median household income was divided into 5 quintiles, as follows: first quintile—$43,700 USD or lower; second quintile—$60,240 USD; third quintile—$64,500 USD; fourth quintile—$73,370 USD; and fifth quintile—$91,570 USD or higher. In the analysis of race and ethnicity, patients were categorized into one of 4 demographic groups: African American [AA], Asian/Pacific Islander [API], Native American/Alaska Native [NA], or White [WH]. Gender was categorized as male [M] or female [F]. Insurance status was classified as insured (Medicare or private insurance), Medicaid, and uninsured. Lastly, patients were stratified based on intervention: hepatic resection; liver ablation or local destruction (photodynamic therapy, electrocautery, fulguration, cryosurgery, or laser therapy); and no intervention.
Primary endpoints included: (1) overall survival (OS); (2) likelihood of receiving a recommendation for surgical intervention; and (3) specific surgical intervention performed. OS was estimated in months from the date of diagnosis to the end of the follow-up period (for survivors) or the date of death (for non-survivors). The data that support the findings of this study are de-identified and publically available in the SEER database. Therefore, no Institutional Review Board (IRB) approval was required.
Statistical Analysis
The baseline characteristics and group differences for HCC AJCC stages were compared using Pearson’s Chi squared test for proportions. Univariate and multivariate multinomial logistic regression models were used to assess associations of insurance, race, gender, and median household income with different treatment modalities. “No surgical intervention” was used as the base outcome in the multinomial model. Relative Risks Ratios (RRR) were used to measure pertinent associations, allowing for simultaneous comparison of hepatic resection, ablation/local treatment, and no surgical intervention. RRR were also used for a comparison of patients who received a recommendation for surgery versus those who received no surgical recommendation and in whom surgery was contraindicated. Model selection was done using Akaike information criterion (AIC), and the model with the lowest AIC selected. 11
The Kaplan-Meier method was used for survival analysis and the log rank test for equality of survival functions. Model selection was done using the stepwise forward method for Cox regression. Variables included in the adjusted models had a p-value < 0.05 for the outcome of interest in the univariate analysis. These variables remained in the final model if they were still significant at p < 0.05 in the final adjusted model. A p-value < 0.05 was used for statistical significance in this study. To assess if the model was correctly specified, we used restimation techniques with “linktest” 12 ; prediction squared did not demonstrate explanatory power (p > 0.05). All statistical analyses were performed using Stata version 14.2 (StataCorp, College Station, TX, USA) and R version 3.6.1.
Results
Study Population and Patient Characteristics
A total of 28,518 patients were included in the final analysis (Table 1). The racial distribution was as follows: AA—3,739 (13.1%); API—4,768 (16.7%); NA—377 (1.3%); and WH—19,634 (68.9%). The stage distribution was as follows: stage I—52.05%; stage II—27.5%; and stage IIIA—20.45%. A total of 11,058 patients (38.8%) received a recommendation for surgical intervention; among these individuals, 11.6% were AA, 19.8% were API, 1.3% were NA, and 67.3% were WH. For the entire cohort, 20.7% underwent hepatic resection, 14.7% underwent local treatment/ablation, and 65.2% received no surgical intervention.
Demographics and Clinical Characteristics of the Cohort.
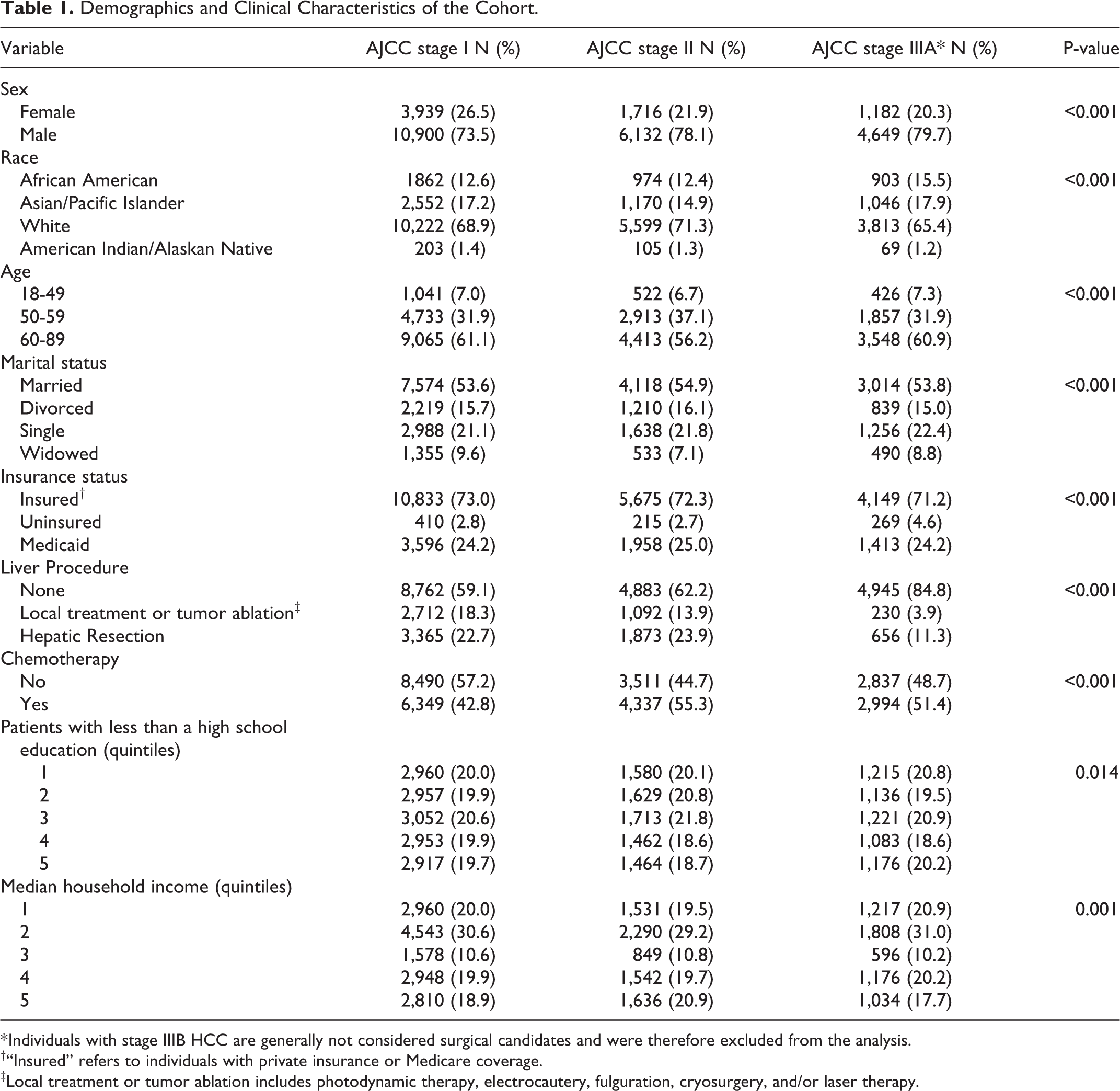
* Individuals with stage IIIB HCC are generally not considered surgical candidates and were therefore excluded from the analysis.
†“Insured” refers to individuals with private insurance or Medicare coverage.
‡Local treatment or tumor ablation includes photodynamic therapy, electrocautery, fulguration, cryosurgery, and/or laser therapy.
Associations of Surgical Treatment of HCC by Race, Insurance, and Marital Status
Table 2 displays the multivariate multinomial logistic regression model used to assess factors associated with the implementation of different surgical treatment modalities. API were significantly more likely to receive a recommendation for hepatic resection than individuals in any other ethnic group (RRR = 1.45; 95% CI: 1.31 -1.61; Reference Race: AA). API were also more likely to undergo hepatic resection (RRR = 1.61, 95% CI: 1.43 -1.82) and local treatment/ablation (RRR = 1.43; 95% CI; 1.24 -1.66) as compared to their AA counterparts. There was no significant difference in treatment modality beween AA and WH individuals.
Multivariate Multi Nominal Regression Analysis for Tumor Characteristics and Socioeconomic Factors Associated With Treatment Allocation Compared With No Surgical Treatment in HCC Patients.

* The base outcome for multinomial regression is “no liver procedure.”
The overall rate of hepatic resection decreased among all ethnic groups between 2007 and 2015. Nevertheless, API individuals were consistently more likely to undergo hepatic resection as compared to their AA, NA, and WH counterparts; NA were less likely than members of any other group to undergo hepatic resection. Furthermore, as compared to API and WH individuals, AA and NA were significantly less likely to receive any surgical intervention. Interestingly, the overall rate of local treatment or ablation was found to have steadily increased since 2007 among all ethnic groups. The relationship between race and HCC intervention is illustrated in Figure 2.

Panel A. predicted probability of intervention based on race. Over time, the likelihood of undergoing hepatic resection decreased while the likelihood of receiving local destruction/ablation or no intervention increased among all races. Figure 2, Panel B. predicted probability of intervention based on race. The race effect plot demonstrates that API were significantly more likely than individuals in any other ethnic group to undergo hepatic resection.
Insurance status and median household income also influenced treatment strategies. Uninsured patients (RRR = 0.42; 95% CI: 0.34-0.53) and those with Medicaid coverage (RRR = 0.54; 95% CI: 0.50-0.59) were less likely to undergo hepatic resection or local treatment/ablation than individuals with private insurance or Medicare (Table 2). Interestingly, there was a negative correlation between income and likelihood of hepatic resection: patients in the fifth quintile of median household income were less likely to undergo hepatic resection than low income individuals (RRR = 0.86; 95% CI: 0.77-0.96). Individuals in this cohort, however, were also significantly more likely than those in the bottom 4 quintiles to undergo local treatment/ablation (RRR = 1.21; 95% CI: 1.05 -1.38). It therefore appears likely that less invasive treatment modalities are favored among individuals of the highest income strata, who are more likely than their lower income counterparts to present with potentially-resectable disease (Table 3).
Sociodemographic and Tumor Characteristics Associated With OS for Patients With Resectable HCC.
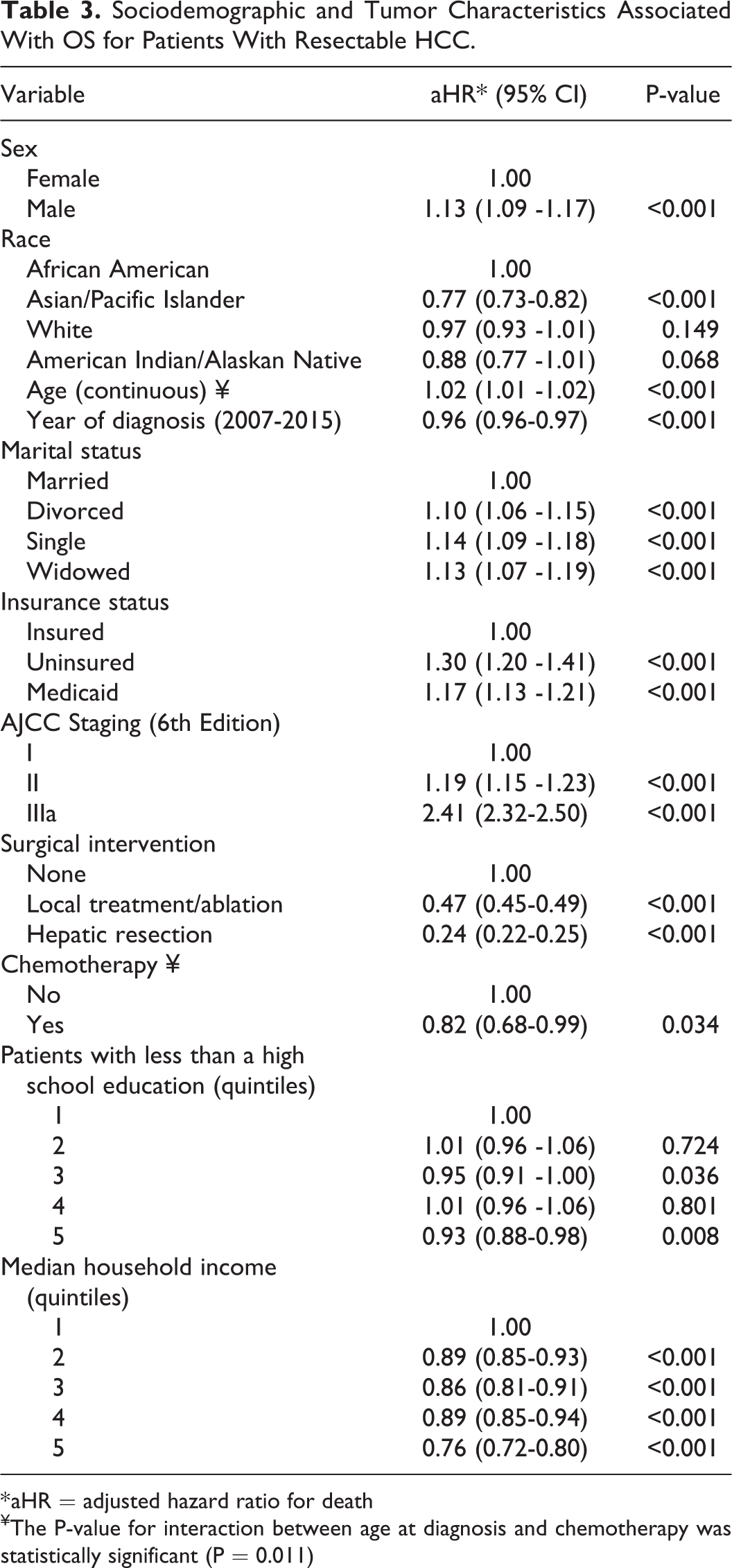
* aHR = adjusted hazard ratio for death
¥The P-value for interaction between age at diagnosis and chemotherapy was statistically significant (P = 0.011)
Lastly, there was a significant association between marital status and intervention: as compared to single or divorced individuals, those who were married were more likely to undergo hepatic resection. Interestingly, however, marital status had no significant effect on the likelihood of undergoing ablation (Table 3).
Hepatocellular Carcinoma Survival
The median OS for all patients diagnosed with HCC during the study period was 23 months. Individuals who underwent hepatic resection exhibited prolonged survival (median OS: 96 months) as compared to those who received no surgical treatment (median OS: 14 months) or local treatment/ablation (median OS: 40 months). The 3- and 5-year survival rate for the entire cohort was 38.5% (95% CI: 37.9-39.1) and 28.2% (95% CI: 27.6-28.9), respectively.
There were significant racial disparities in OS. API were found to have the highest median OS survival at 35 months; this was followed by WH and NA, both of whom had a median OS of 22 months. Median OS was the shortest among AA at 18 months. The relationship between race and HCC management and outcomes is illustrated in Figure 2. In addition, significant gender disparities were observed: females exhibited superior OS as compared to males (aHR = 0.89; 95% CI: 0.85-0.93; Reference Gender: M), and the 5-year survival rate was 31.0% in women versus 27.4% in men.
Median OS was also affected by income, educational level, insurance, and marital status. There was a distinct survival advantage for individuals residing in geographic regions in which the median household income was in the fifth quintile, and there was a direct correlation between level of education and median OS. Individuals with private insurance or Medicare demonstrated prolonged OS as compared to those with Medicaid. Outcomes were significantly worse among the uninsured (Figure 3). Lastly, marriage conferred a significant survival advantage; overall survival was poorer among patients who were single, divorced, or widowed.

Panel A. Kaplan–Meier (K-M) survivor function for difference in overall survival by race. A greater proportion of Asian Americans (API, indicated by the red curve) were living throughout the time period in which the analysis was conducted as compared to Whites (green curve), Native Americans (yellow curve) and African Americans (AA, blue curve). Figure 3, Panel B. Kaplan–Meier (K-M) survivor function for difference in overall survival by sex. A greater proportion of women (blue curve) were living throughout the time period in which the analysis was conducted as compared to men (red curve). Figure 3, panel C. Kaplan–Meier (K-M) survivor function for difference in overall survival by insurance status. A greater proportion of individuals with Medicare or private insurance (blue curve) were living throughout the time period in which the analysis was conducted as compared to those with Medicaid (green curve) or no insurance (red curve). Figure 3, Panel D. Kaplan–Meier (K-M) survivor function for difference in overall survival by liver procedure. A greater proportion of patients who underwent hepatic resection (green curve) were living throughout the time period in which the analysis was conducted as compared to those who underwent local destruction/ablation (red curve) or no surgical intervention (blue curve).
Lastly, treatment modality had a significant effect on OS. The best outcomes were seen among patients who underwent hepatic resection, in whom the risk of death was significantly lower than individuals who underwent local treatment/ablation or no surgical intervention (aHR = 0.24; 95% CI: 0.22-0.25; Reference: “No Treatment”). Indeed, in comparing OS, hepatic resection was far superior to local treatment/ablation. The effect of treatment modality on OS is further detailed in Table 3.
Discussion
Sociodemographic characteristics have a significant effect on health care access, delivery, and outcomes. Indeed, it has been definitively established that an individual’s race, gender, insurance status, and wealth can influence his or her care and clinical course. The effect of sociodemographic factors on patient care is perhaps most evident in the setting of malignancy. African Americans with resectable gastric cancer, for example, are more likely to receive a recommendation against surgery than their White and Asian counterparts. 13 The female sex favors prolonged survival in numerous malignancies, including head and neck cancers, melanoma, and leukemia. 14 Low income individuals tend to fare substantially worse than the wealthy across a range of health-related outcomes, including quality of life and overall survival. 15,16 In the setting of cancer, low income is associated with inferior survival among both children 17 and adults. 18 Insurance status may also affect patient outcomes, as previous investigations have revealed that individuals with government-funded insurance are less likely to undergo curative therapy than those with private insurance. 10 The preponderance of the evidence indeed suggests that health care outcomes vary significantly based on immutable demographic and sociodemographic variables. The underlying causes of these disparities remain to be established. However, it is conceivable that there are multiple contributory elements, including lifestyle factors, health care access, implicit bias, environmental influences, and biological differences that exist between races and genders.
The Effect of Race on HCC Management and Outcomes
The relationship between race and health care outcomes has been studied extensively. Data suggest that African Americans are disproportionately affected by racial disparities and are undertreated to a greater extent than members of any other ethnic group. 19 -21 Previous investigations have demonstrated that health care inequality is particularly pronounced in the fields of hematology and oncology. African Americans with prostate cancer, for example, are significantly less likely to receive definitive therapy than their White counterparts. 22 Preventive cancer care is also suboptimal; African Americans are one-third less likely than Whites to receive a recommendation for colorectal cancer screening, 23 and mammography rates among African American women are significantly lower than any other ethnic group. 24 It has been postulated that these health care disparities can be attributed to various factors that affect the African American community, including limited access to health care, distrust of the medical establishment, and implicit bias. 13
Our investigation revealed several compelling findings that contribute to the ongoing discussion on race and health care disparities. Of particular interest is the narrowing health care gap between African Americans and other ethnic groups. Indeed, in a comparison of African American, White, and Native American/Alaskan Native individuals with resectable HCC, we found no significant differences in the likelihood of surgical recommendation or overall survival. The absence of any racial disparities between African Americans and Whites represents an important observation that is consistent with other recent findings pertaining to race and health care outcomes.
In a landmark 2017 study published in Morbidity and Mortality Weekly Report, authors noted that the racial disparity gap in all-cause mortality rates narrowed from 33% in 1999 to 16% in 2015. 25 Other analyses have reported similar findings. A recent article on racial disparities in surgical mortality revealed that gaps between African Americans and Whites declined during the early-2000s; over the 9-year study period (2004-2015), authors observed a significant decrease in the mortality differential between African Americans and Whites. Furthermore, they found that the mortality trend was improving at a more rapid rate for African Americans than for Whites. 26 The narrowing health care gap has also been reported in the setting of oncology, wherein racial disparities in cancer death rates have sharply declined in recent years. 27 These findings represent a marked improvement as compared to 2 decades ago. Indeed, between 1998 and 2015, the African American-to-White overall mortality ratio decreased from approximately 1.56 to 1.16. 25,28
Our analysis of HCC management and outcomes contributes to the growing body of evidence indicating that the racial disparity gap is rapidly narrowing in the United States. We found that African Americans were equally likely to receive a recommendation for surgery as their White and Native American/Alaskan Native counterparts. In addition, overall survival was equivalent between all 3 ethnic groups (Table 2). The underlying reasons for the narrowing racial disparity gap remain to be established, but it has been postulated that a dual strategy of universal and targeted interventions has played an important role in improving health care outcomes among African Americans. 25 Other investigators have proposed that the narrowing racial disparity gap can be explained simply by general changes in risk exposure and disease incidence that have occurred over time. 29 Notably, however, improved health care outcomes among African Americans are not universal across all conditions, and marked disparities still exist in the setting of gastric adenocarcinoma, 13 non-small cell lung cancer, 30 squamous cell carcinoma, 31 and many other malignancies.
Gender and HCC
Gender has a marked effect on both HCC incidence and outcomes. Not only are women 4 to 8 times less likely to develop HCC than men, but our analysis revealed that females with resectable tumors exhibit superior overall and 5-year survival. These findings are similar to those described by other authors. 32 In an analysis of SEER data collected between 1988 and 2010, Yang et al. observed superior overall survival among females as compared to males. Notably, investigators adjusted for race, stage of disease, tumor size, tumor grade, and year of diagnosis. The Yang group postulated that estrogen is protective against hepatocarcinogenesis; this hypothesis was supported by the observation that there is an inverse relationship between age at menopause and HCC risk. Moreover, the greatest gender disparity in overall survival was noted among women aged 18 to 44 years, in whom estrogen levels are presumably the highest. Previous studies have also demonstrated that use of hormone replacement therapy is associated with a lower risk of HCC. 33 Favorable prognostic factors that are more commonly observed among women with HCC—as compared to men—include smaller tumor size, lower bilirubin levels, and decreased frequency of venous invasion. 34
We postulate that the improved survival observed among women with resectable HCC is related to both sex hormones and behavioral risk factors. In addition to the aforementioned estrogen effects, data suggest that androgen/androgen receptor signaling promotes hepatocarcinogenesis and HCC development. 35 Furthermore, as compared to women, men are more likely to smoke cigarettes, drink alcohol, and present with HBV and HCV coinfection; all of these factors are associated with a poor prognosis. 36
The Effect of Insurance on HCC Prognosis
It has been definitively established that individuals receiving government-funded insurance experience worse health care outcomes than those with private insurance. Indeed, in a 2019 study by Sobotka et al., authors concluded that patients with HCC who were on Medicaid, as compared to those with private insurance, were more likely to: (1) present with decompensated liver disease and other comorbidites; (2) have difficulty accessing specialists; (3) present with metastatic disease; (4) experience a lower quality of life; and (5) exhibit higher mortality. 10 In addition, patients with Medicaid were less likely to undergo HCC treatment, and those who did receive treatment were less likely to undergo expensive interventions, such as transarterial chemoembolization (TACE) and liver transplantation.
Interestingly, although it has been hypothesized that the poor outcomes associated with Medicaid merely reflect the sequelae of poverty, we adjusted for median household income in our analysis and nevertheless found markedly poorer survival among individuals on Medicaid as compared to those with Medicare or private insurance.
The factors underlying poor outcomes among the Medicaid population remain to be established. One important aspect identified by the Sobotka group is HCV, which represents the most common risk factor for HCC in the United States. Individuals on Medicaid are less likely to have access to curative treatment for HCV and are therefore more likely to go on to develop HCC than their privately-insured counterparts. Furthermore, in a recent study by Duma et al., investigators reported that individuals on Medicaid were more likely to refuse cancer treatment as compared to those with private insurance. 37 It is conceivable that this is fueled by a general sense of skepticism toward the medical community that is pervasive among the Medicaid population.
Income and HCC
Income has a significant effect on HCC survival. Our analysis revealed a strong survival advantage for individuals in the top 20% of median household income as compared to those of low income. Furthemore, high income patients were significantly more likely than those in the bottom 4 quintiles of median household income to undergo local treatment/ablation.
The relationship between income and HCC outcomes has been previously investigated. In a 2017 retrospective analysis by Shen et al., authors evaluated the effect of household income on HCC mortality and survival rates. 38 Household income was stratified into 3 groups: low (<$50,000 per year), moderate ($50,000-$200,000), and high income (>$200,000). The Shen group observed a higher 30-day mortality rate in the low-income group as compared to the moderate and high-income groups. The highest income patients also had a significantly better prognosis than the moderate and low-income groups with a median survival of 46 months versus 37 months and 34 months, respectively.
The underlying cause of income inequality in HCC survival remains to be established. However, Shen et al. reported that low-income individuals were more likely than their high-income counterparts to have a low educational level and live in a rural area. Low-income patients also presented with more advanced disease than either moderate or high-income groups, and high-income individuals had better Child-Pugh scores at admission than those in either of the other 2 groups. The major risk factor that disproportionately affects those of low income therefore appears to be late diagnosis.
Limitations
Our study provides important insight into various sociodemographic characteristics that may predict outcomes in HCC. However, there are several limitations inherent to its design.
First and foremost, the analysis was retrospective in nature and therefore cannot demonstrate causality. Second, there is no transplant data available through the SEER program. Third, the SEER program does not provide information pertaining to liver function or MELD scoring. Fourth, specific treatment information, such as chemotherapy data, is not available in the SEER database. Lastly, we we did not have baseline data on comorbidities. Despite these limitations, we were able to adjust for most variables pertinent to HCC outcomes.
Conclusion
Health care equality in the setting of HCC represents an ambitious challenge. A dual strategy of universal and targeted interventions can be effective in reducing racial disparities. Gender disparities may be improved by promoting healthy lifestyle habits among men. The inferior outcomes observed among uninsured individuals and those on Medicaid may need to be addressed through comprehensive health care reform. As economic inequality remains at the forefront of our national dialogue, community investment should target low-income districts to improve screening and access to consultative care. Furthermore, understanding the biologic basis for the higher survival observed in Asians will hopefully translate into improved care for minorities and low income individuals. We believe that our analysis provides a framework for future avenues of research that will help improve HCC outcomes among the most underserved segments of the population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.