
Abstract
Background:
We studied the clinical characteristics, diagnosis, treatment, and prognosis of secondary tumors of the thyroid (STTs) and analyzed this rare phenomenon based on our clinical experience.
Methods:
We reviewed 16 000 malignant thyroid tumors diagnosed at 2 medical centers in China from 1978 to 2018, including 55 patients with STTs.
Results:
The most frequent primary tumor sites included lung (21.8%), gastrointestinal (18.2%), breast (14.5%), and kidney (12.7%). The median age at STT diagnosis was 56 years. The time from diagnosis of primary tumor to metastases to the thyroid ranged from 0 to 108 months, with the longest interval being for renal cell carcinoma (RCC; mean: 49 months). There were 22 cases of single metastatic foci and 33 cases of multiple metastatic foci. At the time of STT diagnosis, 42 patients had multiple organ metastases and 13 patients had only thyroid metastases. Thyroid function was examined in 50 patients, including 23 with Hashimoto’s thyroiditis. Metastases were diagnosed histologically and confirmed by negative immunohistochemistry for thyroid markers. Twenty-one patients were treated with resection, including total thyroidectomy in 14 and unilateral lobectomy in 7. Thirty-four patients were treated without resection, but 2 were treated with tracheotomy. The median survival time of all patients with metastasis was 10 months (range: 1-96 months). Patients with primary RCC had the best prognosis (median survival time: 52 months), followed by patients with breast cancer (33 months). Patients who underwent thyroid surgery had a better prognosis than patients without thyroid surgery. Patients with single metastatic foci or single organ metastases had a better prognosis than patients with multiple metastatic foci or multiple organ metastases.
Conclusions:
Metastasis to the thyroid is a rare clinical phenomenon, and sometimes a diagnosis of STT is difficult; so, we need to pay more attention to it. While prognosis appears to be related to surgery or some characteristics of metastatic spread, these data suggest it is more complex. Tumor biology is king; in fact, prognosis was mainly related to the biological behavior of the primary tumor. We cannot only opt for surgery; thus, case selection is important, and the treatment strategy for STT patients should be determined individually according to their specific biological behaviors.
Introduction
Metastasis to the thyroid from nonthyroid malignancies is a rare clinical phenomenon, although the blood supply to the thyroid is second only to that of the adrenal gland. Only 1.4% to 3% of primary non-thyroidal tumors metastasize to the thyroid, accounting for a small percentage of all clinically reported malignant thyroid tumors, although the incidence is 1.9% to 24% in autopsy studies. 1 Most studies of secondary tumors of the thyroid (STTs) are case reports. 2 The diagnosis, treatment, and prognosis of STTs have recently attracted increasing attention from imaging doctors, surgeons, physicians, and pathologists. 3 We performed a retrospective cross-sectional study to examine the clinical and biological characteristics of STTs in 55 patients from 2 large medical centers in China during a 40-year period from 1978 to 2018.
Materials and Methods
Patients
Fifty-five patients were diagnosed with STTs at Tianjin Medical University Cancer Hospital and Fujian Medical University Cancer Hospital between 1978 and 2018. We retrospectively reviewed and analyzed these patients’ records to report outcomes. Institutional review board approval was obtained for this study. The criteria for diagnosis of STTs involved screening 16 000 specimens of malignant thyroid tumors and excluding primary tumors and malignant lymphomas of the thyroid as well as tumors in adjacent organs, such as the hypopharynx, larynx, trachea, and esophagus, which could directly invade the thyroid. We exclude patients with incomplete case data and follow-up information. Finally, 55 patients were eligible. All fine-needle aspiration (FNA) and paraffin tissue sections were reexamined by 2 pathologists. This study was approved by the research ethics committee of Fujian Medical University Cancer Hospital (The approval number given by the ethical board: SQ2019-019-01) and the research ethics committee of Tianjin Medical University Cancer Institute and Hospital (The approval number given by the ethical board: EK2019105). Written/oral consent was obtained from all patients or their parents/caregivers.
Statistical Analysis
Statistical analyses were performed to examine outcomes in patients with metastases to the thyroid gland. Survival was calculated using Kaplan-Meier analysis. Survival curves were compared between groups with and without thyroid surgery and between patients with simultaneous and heterochronous metastasis using log-rank tests. Prism 6.0 Software (GraphPad, Inc) was used for statistical analyses.
Results
Clinical Characteristics
The patient cohort included 21 (38.2%) men and 34 (61.8%) women. The median age at diagnosis of clinically significant metastases to the thyroid was 56 years (range: 42-75 years). The most frequent primary tumor sites included the lungs (n = 12, 21.8%), gastrointestinal (n = 10, 18.2%), breast (n = 8, 14.5%), and kidney (n = 7, 12.7%). There were 22 cases of single and 33 cases of multiple metastatic foci. The diameter of the metastases ranged from 0.6 to 5.6 cm (mean: 2.6 cm). At the time of diagnosis, 42 patients had multiple organ metastases and 13 had only thyroid metastases, but all cases developed other organ metastases during follow-up. The time from initial diagnosis of the primary tumor to the detection of thyroid metastases ranged from 0 to 108 months (mean: 55 months), with the longest interval being for RCC, which had a mean of 49 months. Most patients had a palpable, painless neck mass, but there were a few patients with obvious dyspnea and dysphagia. Thyroid function was examined in 50 patients, including 23 (46%) with Hashimoto’s thyroiditis. Patient data and the clinical characteristics of STTs are summarized in Table 1.
Clinical Characteristics of Patients With Secondary Tumors of Thyroid.

Diagnosis
Fine-needle aspiration biopsy (FNAB) was performed in 33 patients, 24 underwent 18F-fluorodeoxyglucose positron emission tomography (FDG PET)/computed tomography (CT), 36 underwent CT detection, and 45 underwent ultrasonography. All diagnoses were confirmed by immunohistochemistry. Metastases were diagnosed histologically and confirmed by negative immunohistochemistry for thyroid markers.
Treatment
Prior to the diagnosis of STTs, 48 patients underwent chemotherapy or targeted therapy, 21 were treated with resection, including total thyroidectomy in 14 and unilateral lobectomy in 7. Thirty-four patients were treated without resection, but 2 were treated with tracheotomy. Central lymph node dissection (CLND) was performed in 8 patients. No central lymph node metastasis was found in patients who underwent CLND. No one had a recurrence to the thyroid or central region after surgery.
Prognosis
Patients were followed-up until August 1, 2019, and no patients were lost to follow-up (follow-up: 100%). Twelve patients remained alive, including 5 with primary renal cell carcinoma (RCC), 4 with breast cancer, 2 with head and neck cancer, and 1 with cervical carcinoma. No patient died as a result of neck compression by the STT. The median survival time among all patients with STTs was 10 months (range: 1-96 months). Patients who underwent thyroid surgery had a better prognosis than patients without thyroid surgery (log-rank test, P < .0001; Figure 1). Patients with single metastatic foci had better prognosis than patients with multiple metastatic foci (log-rank test, P < .0001; Figure 2). Patients with single organ metastases had better prognosis than patients with multiple organ metastases (log-rank test, P < .0001; Figure 3). Patients with primary RCC had the best prognosis (median survival time: 52 months), followed by patients with breast cancer (33 months); patients with lung cancer and gastrointestinal cancer had the worst prognosis (log-rank test, P = .0004; Figure 4).
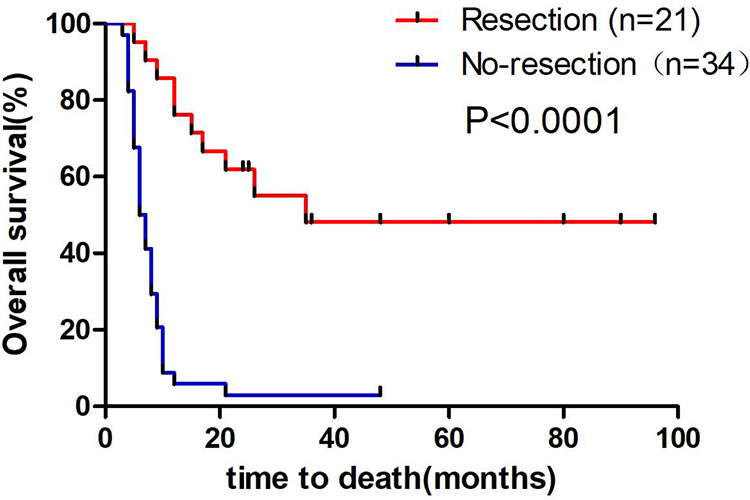
Comparison between the survival of patients with and without resection. The median survival for patients with resection was 24 months (range: 5-96 months), whereas the survival in patients without resection was 7 months (range: 3-48 months, log-rank test: P < .0001).
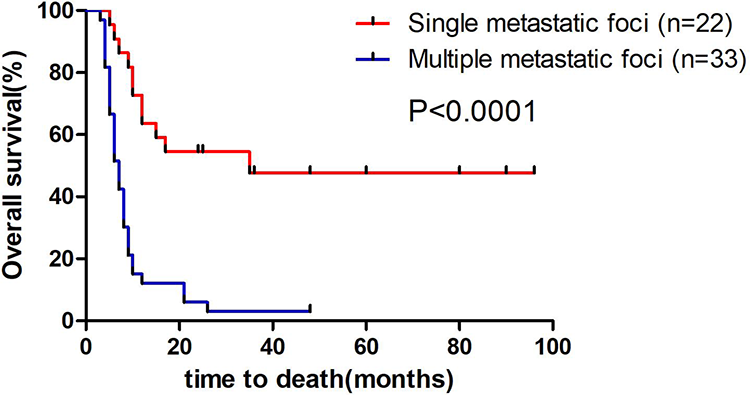
Comparison between the survival of patients with single metastatic foci and multiple metastatic foci. The median survival of patients with single metastatic foci was 24 months (range: 5-96 months), whereas the survival of patients with multiple metastatic foci was 7 months (range: 3-48 months; log-rank test: P < .0001).

Comparison between the survival of patients with single organ metastases and multiple organ metastases. The median survival of patients with single organ metastases was 35 months (range: 7-96 months), whereas the survival of patients with multiple organ metastases was 8 months (range: 3-48 months; log-rank test: P < .0001).

Comparison between the survival of patients with primary lesions of the lung, gastrointestinal, breast, and kidney. Patients with primary RCC had the best prognosis (median survival time: 52 months), followed by patients with breast cancer (33 months); patients with lung cancer and gastrointestinal cancer had the worst prognosis (log-rank test: P = .0004).
Discussion
Clinical Characteristics
Although the blood supply to the thyroid is inferior only to that of the adrenal gland, the incidence of STTs is very low. Previous studies have indicated that this is due to the rapid arterial blood flow and high concentrations of oxygen and iodine, which can prevent tumor cells from anchoring and growing. 4 As early as 1931, Willis proposed that rapid arterial blood flow in the thyroid would prevent the anchoring of circulating tumor cells, while high concentration of oxygen and iodine would prevent the growth of malignant tumor cells. 5 Among our cases, 46% of patients had Hashimoto’s thyroiditis, suggesting that STTs were more likely to occur in patients with Hashimoto’s thyroiditis, and furthermore, that changes in the thyroid microenvironment may be an important factor in the metastasis of STTs. The median time from primary tumor to metastasis to the thyroid in the current study was 55 months, with the longest interval being for RCC (49 months), which is in accordance with the literature. 6 The main primary tumor sites in this study were the lung (20%), gastrointestinal (18.2%), breast (14.5%), and kidney (12.7%); however, a recent review of the literature found that in the non-East Asian population, the most common primary site was the kidney (41.57%), followed by lung (11.61%), gastrointestinal (10.11%), and breast (9.36%). 1,7 This discrepancy may be related to the respective epidemiology of these primary tumors; additionally, the incidences of lung and gastrointestinal cancer are higher in China, while the incidences of RCC and breast cancer are higher in non-East Asian countries. 8,9 Primary thyroid tumors are more common in women; however, there is debate about gender advantage in terms of thyroid metastasis. Some studies have shown a higher incidence in women, while others have reported the opposite results; our data support the former. 10 Additionally, our data showed that at the time of diagnosis, 42 (76.4%) patients had multiple organ metastases (lung, liver, bone, and brain), which was similar (35%-80%) to previous results. 11 It has been reported that STTs from renal and breast cancer are usually single metastatic foci, which are consistent with our data. 12
Diagnosis
The results of this study suggest that the detection rate of STTs has increased significantly in the recent years, closely related to improvements in diagnostic techniques such as pathology and imaging. 13 The FNAB may have some omissions because patients with STTs usually have multiple nodules. Therefore, we suggest that multiple punctures under ultrasound guidance should be done in FNAB to avoid omitting any foci. However, cytological examination is difficult because STTs are often mistaken for primary thyroid tumors, especially thyroid anaplastic carcinoma. 14 -16 Immunohistochemistry can be used to accurately diagnose STTs. STTs are negative for thyroglobulin, while primary thyroid tumors are positive. 17 Thyroid transcription factor-1 (TTF-1) is also an important biomarker, although expression of TTF1 is notably also positive in lung cancer. According to the literature, on ultrasound images, STTs show uneven hypoechoic or obvious hypoechoic masses in the thyroid with fuzzy edges. 7 Computed tomography shows low-density lesions, and magnetic resonance imaging shows a low signal on T1 weighted and a slightly high signal on T2 weighted. 18 Figure 5 shows a case of STT with colon as the primary site; the thyroid gland is abnormal in shape, enlarged in volume, unsmooth in capsule, thickened in a spot, inhomogeneous in diffuse distribution of echo, a low echo with unclear boundary can be seen, and the blood flow signal in substance is more normal and abundant (Figure 5A and B). A CT scan shows the nodular low-density lesions in both sides of the thyroid gland, with slight enhancement (Figure 5C). A CT scan of thyroid papillary adenocarcinoma will have obvious enhancement, and it is easy to see microcalcifications, cystic changes, and enhanced mural nodules. In these tissue samples, hematoxylin and eosin staining showed obvious morphological characteristics of colon adenocarcinoma in thyroid tissue. Immunohistochemistry further confirmed the diagnosis, as the thyroid-specific markers thyroglobulin and TTF-1 were negative, and the colon adenocarcinoma specific marker CDX-2 was positive (Figure 5D). It is worth mentioning that this case had only a single organ metastasis to the thyroid; even in the later follow-up, there was no liver metastasis, and the patient is still alive which is very rare.

A and B, Ultrasound showing that the thyroid gland is abnormal in shape, enlarged in volume, unsmooth in capsule, thickened in a light spot, inhomogeneous in diffuse distribution of echo, a low echo with unclear boundary can be seen, and the blood flow signal in the substance is more normal and abundant. C, Computed tomography (CT) scan showing low-density nodular lesions in both sides of the thyroid gland, with slight enhancement. D, Hematoxylin and eosin staining showed the obvious morphological characteristics of colon adenocarcinoma in thyroid tissue. Immunohistochemistry showed that thyroglobulin (TG) and thyroid transcription factor-1 (TTF-1) were negative, while CDX-2 was positive.
Treatment
According to the literature, treatment for a primary tumor, such as chemotherapy, can change the microenvironment of the target organ, 19 thus promoting metastasis formation. Among our 55 cases with STT, 87.2% (48) had received chemotherapy or targeted therapy before diagnosis, but this is very speculative. Whether there is a relationship between chemotherapy and STTs still needs further study. To avoid treatment, primary tumors have to find a more suitable organ, and the microenvironment of the thyroid gland is also affected by chemotherapy, so it becomes a target organ in the process of primary tumor transformation. As for the treatment of STTs, we focus on the indications and methods of operation. As only 3.6% (2/55) of patients underwent tracheotomy due to dyspnea, we do not recommend prophylactic thyroidectomy for STTs, which is consistent with other current studies that have shown that only 10% of patients died of tracheal compression caused by STTs. 14 When STTs cause compression symptoms, we suggest thyroidectomy or tracheotomy to relieve these symptoms and improve quality of life. Because STTs are a circulatory-derived metastasis of a primary tumor, they commonly occur as multiple metastatic foci. When patients need thyroidectomy, we suggest total thyroidectomy but do not recommend CLND because our data showed that 8 patients with CLND did not have lymph node metastasis. According to the literature, the rate of lymph node metastasis in patients with STTs treated with CLND is only 3%. 14
Prognosis
This study showed that patients who underwent thyroid surgery had a better prognosis than patients who did not. Additionally, patients with single metastatic foci or single organ metastases had a better prognosis than patients with multiple metastatic foci or multiple organ metastases. Similar conclusions have been made in other studies. 20 -22 However, this is only a superficial phenomenon, and we should think about it more deeply. In fact, what really determines the prognosis of STTs is the biological behavior of the tumors. It is not that surgery leads to an improvement in the prognosis of the tumor, rather it is that the biological behavior of the tumor makes some patients have the opportunity and indications for surgery. As our research shows, the prognosis of renal cancer and breast cancer is the best, but in fact, the proportion of patients with renal cancer and breast cancer who undergo surgery is also the highest (Table 1). Therefore, we think that tumor biology is king and is the key to formulating a treatment strategy for STTs. Due to the limited number of cases, there are some limitations in this study. We hope that more researchers will be interested in this topic and share their own cases in the future so as to enrich this study.
Conclusion
In this study, we summarized the clinical characteristics of STTs in a Chinese population from 2 large medical centers and compared our data to that in the literature. Although this phenomenon is rare, we should also pay attention to it to avoid incorrect diagnosis and treatment. Many studies of STTs are keen to discuss the treatment strategy and whether surgery is needed. They ignore that STTs are only a stage of advanced tumor development and that the biological behavior of the primary tumor is the key to treatment.
Footnotes
Authors’ Note
Yu Wu and Kai Huang contributed equally to this work. This study was approved by the Research Ethics Committee of Fujian Medical University Cancer Hospital (The approval number given by the ethical board: SQ2019-019-01) and the Research Ethics Committee of Tianjin Medical University Cancer Institute and Hospital (The approval number given by the ethical board: EK2019105). Written/oral consent was obtained from all patients or their parents/caregivers.
Acknowledgments
The authors thank Mark Abramovitz, PhD, and Susan Furness, PhD, from Liwen Bianji, Edanz Editing China (www.liwenbianji.cn/ac), for editing the English text of drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Natural Science Foundation of Fujian Province (Grant number: 2019J01190), and Fujian Provincial Health Technology Project (Grant number: 2019-ZQNB-4-2019-CXB-7).