
Abstract
Patients with multiple myeloma are at elevated risk of venous thromboembolism (VTE), the second leading cause of death in patients with cancer, but physician adherence to VTE prevention guidelines is low. Several organizations partnered in designing and implementing a 2-year quality improvement (QI) program in a tertiary care/academic cancer center, to increase awareness of VTE prophylaxis for patients with multiple myeloma and thus improve adherence to prophylaxis guidelines and protocols. The QI arm included 2 chart audits, conducted 2 years apart, of unmatched cohorts of 100 patients with multiple myeloma. An Education arm included 2 grand rounds presentations, 3 web-based case discussions, and a patient education module. Twenty providers took part in the continuous QI arm. More than 1100 learners participated in the online cases; the patient education curriculum reached 112 multiple myeloma patients. The initiative proved helpful in defining barriers to guideline adherence and identifying data-driven practice improvement strategies for VTE prophylaxis. It also increased learner awareness of VTE guidelines, patient risk stratification, and optimal thromboprophylaxis strategies. There was a reduction in VTE events (primary clinical outcome) from 10% at baseline to 4% in the follow-up cohort, although this was not statistically significant. Higher rates of guideline-based prophylaxis were observed in low-risk patients, and a lower incidence of VTE was observed in multiple myeloma patients with a prior history of VTE. Additional research is needed to refine prophylaxis guidelines. With appropriate institutional support, this type of QI program can be readily adopted by other organizations to address practice improvement needs.
Keywords
Introduction
Patients with multiple myeloma and other plasma disorders have an elevated risk of developing venous thromboembolism (VTE) compared to the general population, due to a variety of patient-related, disease-related, and treatment-related risk factors. 1 Venous thromboembolism, which may include deep venous thrombosis and pulmonary embolism, has strong associations with short- and long-term mortality, making it the second leading cause of death among patients with cancer. 2 Additionally, VTE prophylaxis may result in other morbidities such as bleeding, especially in combination with agents that could lead to thrombocytopenia, which in turn lead to increased hospitalization rates. 3 Venous thromboembolism is therefore a condition that incurs significant cost on the health care system: a recent study showed that total all-cause health care costs in patients with cancer with VTE are approximately 80% higher compared to patients with cancer without this condition. 4
While VTE carries potentially serious consequences, it can be a preventable complication with appropriate prophylactic strategies. 5 Nevertheless, studies report low physician adherence to evidence-based VTE prevention guidelines concerning patients with cancer. For example, data from an international registry in the early 2000s report that only 45% of 1735 patients with cancer received appropriate thromboprophylaxis as recommended by the 2004 American College of Chest Physicians (ACCP) guidelines. 6,7 In 2002, the CURVE study in Canada showed that among acutely ill hospitalized patients with varying illnesses who were eligible to receive thromboprophylaxis, patients with cancer had a significantly reduced likelihood of receiving thromboprophylaxis (odds ratio = 0.40, 95% CI: 0.24-0.68). 8 The H. Lee Moffitt Cancer Center & Research Institute (Moffitt), a large nonprofit cancer treatment and research center in Tampa, Florida, receives between 400 and 500 newly diagnosed multiple myeloma patients annually, who contribute to 8000 to 12 000 hospital visits each year. Since the creation of an oncology accountable care program in 2012 in partnership with Florida Blue, Moffitt identified VTE risk management and prophylaxis as one of the top patient care priorities in the multiple myeloma patient population. As a result, Moffitt developed an internal VTE prophylaxis pathway based on expert consensus, including guidelines developed by the International Myeloma Working Group and the ACCP. 9 -11 To maximize the benefit of this pathway, Moffitt, in partnership with Florida Blue, Haymarket Medical Education, Intelligent Medical Decisions, and Educational Measures as educational partners, with grant support from Celgene, committed to a quality improvement educational program to assess and optimize pathway adherence in the real-world clinical setting.
Materials and Methods
The 2-year quality improvement educational program included 2 interdependent components: a quality improvement (QI) arm and an Education arm. The 2 arms closely interacted with each other to promote awareness of VTE prophylaxis in patients with multiple myeloma, and specifically to promote adherence to the Moffitt VTE Prophylaxis Protocol within the Moffitt system (Figure 1). The QI arm generated the real-world data that directly informed the development content for the Education arm; the Education arm disseminated key learnings to Moffitt and reinforced these learnings through case studies and other educational activities made available to Moffitt, as well as to a national audience via myCME, a global leader of continuing medical education (CME) content. The program was reviewed and considered exempt by the institutional review board of University of South Florida (approval number Pro00021903).

Moffitt venous thromboembolism prophylaxis pathway (2015). Copyright© 2011 H. Lee Moffitt Cancer Center & Research Institute Inc. All rights reserved. Palumbo A, Rajkumar SV, Dimopoulos MA, et al; International Myeloma Working Group. Prevention of thalidomide and lenalidomide-associated thrombosis in myeloma. Leukemia. 2008; 22(2):414-423.
Quality Improvement Arm
The chosen methodology for the QI arm was adapted from the Institute for Healthcare Improvement’s recommendation of the Model for Improvement. 12,13 The model was based on forming a QI team, setting QI aims, establishing QI measures, selecting proposed improvement changes based on current practice, testing the outcomes of the changes, implementing successful changes, and spreading the changes throughout the system.
Kicking off this QI arm was an audit and feedback process grounded in a formal electronic medical record chart audit of 100 patients with multiple myeloma. Patient inclusion criteria and a subset of risk factor variables commonly associated with VTE are listed in Table 1. The chart audit was conducted by 3 pharmacists, who used a data collection form to standardize data abstraction. The audit served multiple purposes: First, it provided a gap analysis of how current practices in Moffitt compared to guideline recommendations; second, it established a local baseline of relevant process/clinical QI measures, against which final program outcomes were evaluated; third, it served as a critical starting point from which subsequent QI activities were developed; fourth, it informed core educational content delivered through the various activities in the Education arm.
Patient Selection Criteria for Baseline and Follow-Up Chart Audits, and Key Risk Factor Variables.
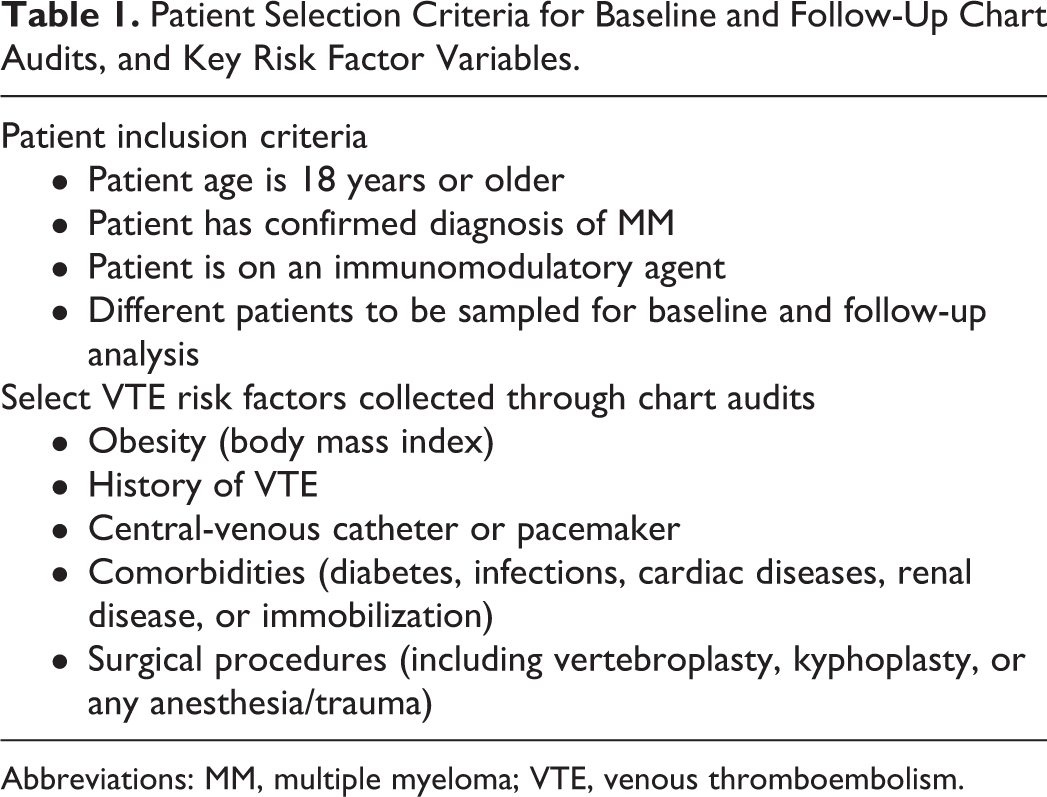
Abbreviations: MM, multiple myeloma; VTE, venous thromboembolism.
The gap analysis involved an assessment of current (baseline) performance against guideline-directed performance and a discussion of the steps or actions needed to achieve the recommended standard—that is, to improve the quality of care by preventing VTE in patients with multiple myeloma. The chart audit and gap analysis were informed by electronic medical records data that included 51 variables, such as age, gender, ethnicity, race, height, weight, functional status, past or present history of VTE, serum/urine proteins, and history of treatment with immunomodulatory agents, steroids, anticoagulants, or other medications. The data also included other risk factors such as comorbid conditions (diabetes, infections, renal disease, immobilization), the presence of central venous catheters or pacemakers, any history of surgical procedures (eg, vertebroplasty, kyphoplasty, or any anesthesia/trauma), or the existence of inherited blood disorders. A multidisciplinary QI team reviewed the gaps, discussed potential interventions to close the gaps, formulated a plan for improvement, and selected objective criteria for determining whether the improvement goals were being met and sustained over time.
Once a baseline was established, a cross-disciplinary QI team composed of Moffitt, Florida Blue, Haymarket Medical Education, and Intelligent Medical Decisions team members was assembled to represent various stakeholders in the care delivery process and to champion subsequent QI activities. Specifically, this QI team engaged in workshops that leveraged chart audit data to conduct root cause analysis, which helped pinpoint local barriers to optimal care. In the months that ensued, the team iteratively prioritized and implemented, where possible, key improvement strategies most applicable to Moffitt. At the end of this iterative process, a follow-up chart pull of 100 unmatched patients was conducted to capture any changes in key QI measures.
Education Arm
The Education arm included 2 live grand rounds–style meetings, 3 web-based educational interventions, and a patient education module. The 2 grand rounds, as part of the audit and feedback process, occurred at the beginning and end of the program. The first session introduced the activity and laid the groundwork for the chart pull, while the second session focused on discussing the findings of the chart review and developing next steps. The grand rounds audience included physicians, nurse practitioners, and pharmacists on the cancer care team.
Based on outputs from the QI arm, the Education meeting content was tailored to the needs of Moffitt providers to address knowledge and attitudinal barriers related to guideline adherence. The meetings combined didactic presentations with interactive use of Audience Response System keypads and concluded with an open forum for questions and answers. Participants completed a postmeeting evaluation survey to assess the impact of the program, with additional information on outcomes gathered via Audience Response System polling before and after the presentation. Educational materials, substantiated by evidence from chart audits, were championed by local clinical leaders and grounded in system-specific practice insights. This closed-system approach was key to providing the necessary motivation, empowerment, and tools to enable changes in practice behavior.
In addition, 3 web-based case clinic articles were rolled out to a broader audience, including but not limited to all providers within Moffitt. Each case introduced a patient with a different presentation of multiple myeloma who might need VTE prophylaxis. Varying degrees of patient-, disease-, and treatment-related risk factors were discussed among the 3 cases to further emphasize the complexities that providers may face in a clinical setting. These case-based articles featured information and support for clinical decision-making using realistic patient scenarios to reinforce specific educational messages. The case clinics were also made available online via myCME to the greater national health care provider community for 1 year following the original posting date.
To supplement the various provider education components, a patient-directed educational curriculum was delivered using 50 iPads provided to Moffitt clinicians. The iPads contained survey questions for patients to answer in the waiting room prior to their visit with a physician, such as whether they were newly diagnosed and not yet on treatment, diagnosed and responding to treatment, or relapsed following a period of treatment. Patients could choose from a menu of 4 modules, each 5 minutes in length, that focused on understanding multiple myeloma, describing the risk of VTE associated with cancer in general and multiple myeloma in particular and recognizing the warning signs and symptoms associated with VTE. The modules incorporated slides and videos, information on helpful patient resources, and a number of polling questions evaluating the impact of the education. The modules were designed to engage patients in the educational program, heighten their awareness of multiple myeloma and the risk of VTE, and foster a more fruitful discussion with the care team. A nurse practitioner was assigned to manage iPad use by patients.
Evaluation Methods
The primary outcomes of the QI arm were evaluated through a pre-/poststudy design with unmatched patient cohorts. Data were collected from retrospective chart audits of 100 patients with multiple myeloma in 2015 and a separate cohort of 100 multiple myeloma patients in 2017. These primary outcomes included a mix of process and clinical measures, developed based on the existing Moffitt Pathway, with input from Moffitt clinicians. Key process measures included VTE risk assessment, patient risk stratification, and appropriate use of VTE prophylaxis regimens. The main clinical outcomes metric was the incidence of VTE events within 6 months of data collection. Evaluation of didactic educational content leveraged pre-/postintervention surveys and open-ended questions to capture improvements in awareness and intention to change. In addition, an extensive secondary analysis was undertaken to assess whether guideline-recommended risk factors or treatment strategies could reliably predict the likelihood of future VTE events.
Chart abstraction was managed in Microsoft Excel, and analysis was conducted in the R software environment for statistical computing. 14 Key outcomes and patient variables such as conformance to clinical guidelines or patient risk stratification were measured as categorical data and summarized using univariate population statistics. Differences between categorical variables and outcomes were expressed as contingency tables and tested using the χ2 test. Correlation between patient characteristics and current VTE events was modeled using logistic regression models.
Results
Program Participation
The components of this program were designed to achieve system-specific QI goals in VTE prophylaxis while at the same time raising awareness within a broader audience. Between June 2015 and June 2017, approximately 20 Moffitt providers actively participated in the 2-year continuous QI arm, incorporating, where relevant, practice improvement recommendations into clinical care. These providers included all physicians involved in the care of patients with multiple myeloma at Moffitt as well as a number of physician assistants, nurse practitioners, nurses, and pharmacists. In addition, over 1100 learners, including Moffitt providers, participated in the 3 online cases. The patient education curriculum reached a total of 112 unique multiple myeloma patients who completed at least 1 of the study modules over the course of 9 months.
Root Cause Analysis and Practice Improvement Strategies
Through facilitated discussions during QI workshops, the QI team identified several local barriers that hinder adherence to guidelines:
Documentation of aspirin, which is indicated for low-risk patients (≤2 VTE risk factors), may be inconsistent, as aspirin is an over-the-counter drug.
Evidence supporting the effectiveness of VTE prophylaxis was perceived as not being strong enough when considering its potential adverse effects in this patient population (eg, risk of bleeding in patients with thrombocytopenia).
Providers have very limited influence on patient factors such as adherence, health literacy, and other socioeconomic factors.
For complex patient populations such as multiple myeloma patients, VTE prophylaxis may not be perceived as a high priority compared to other clinical challenges and may not receive the necessary attention for guideline compliance.
In response to these barriers, several practice improvement strategies were identified as impactful to Moffitt and implemented within usual care where appropriate (Table 2; Figure 2). In identifying barriers and matching them to appropriate interventions, we followed the Model for Improvement approach to QI (Plan-Do-Study-Act) developed by Associates in Process Improvement and used by the Institute for Healthcare Improvement. 13
Practice Improvement Strategies Identified by the Moffitt QI Team.

Abbreviations: MM, multiple myeloma; QI, quality improvement; VTE, venous thromboembolism.

Updated Moffitt venous thromboembolism prophylaxis pathway (2016 and beyond). Note: Carfilzomib should be regarded separately from immunomodulatory agents as it is known to cause microangiopathy but not thrombosis. Carfilzomib was added to the pathway at a time when the possible mechanisms of its thrombogenicity were starting to be recognized but were not fully elucidated. Copyright© 2011 H. Lee Moffitt Cancer Center & Research Institute Inc. All rights reserved. Palumbo A, Rajkumar SV, Dimopoulos MA, et al; International Myeloma Working Group. Prevention of thalidomide and lenalidomide-associated thrombosis in myeloma. Leukemia. 2008; 22(2):414-423.
Provider Awareness
Through the lens of Moore Patient interviewing: obtain a complete history of VTE, inquire about and document aspirin use, and improve patient education Guideline-based treatment: conduct appropriate risk assessment, individualize care plans, and intensify treatment in high-risk patient populations Venous thromboembolism prophylaxis as a priority: assess VTE risk in all multiple myeloma patients and ensure appropriate treatment is initiated in appropriate patient populations.
Patient Empowerment
As noted, a total of 112 multiple myeloma patients reviewed the patient education materials to varying degrees of completion. When given a choice of topics, 58% of patients selected “Module 1: What are blood clots, or VTE,” indicating a general lack of understanding or awareness of this condition. Other choices included “Preventing blood clots” and “VTE in multiple myeloma.” More than 1 (28%) in 4 of surveyed patients indicated that they had not received VTE or blood clot education from their providers. After completing the module, 85% of patients said they were extremely likely or very likely to talk with their doctors about blood clots.
Venous Thromboembolism Prophylaxis Outcomes
Patient characteristics
Patient chart abstraction for baseline was completed between June 2015 and September 2015, while follow-up chart abstraction was completed between June 2017 and October 2017. Patient characteristics at baseline (n = 100) and follow-up (n = 100) are summarized in Table 3. At the time of chart abstraction, all patients were actively being treated with immunomodulatory drugs including lenalidomide, pomalidomide, or thalidomide. Mean age, gender, body mass index distribution, and prior VTE events were comparable between baseline and follow-up and consistent with multiple myeloma demographics. 15
Key Patient Characteristics at Baseline and Follow-Up.

Abbreviations: Ig, immunoglobulin; IMiD, Immunomodulatory Imide Drugs; ISS, International Staging System; NR, not recorded; VTE, venous thromboembolism.
However, it is important to note that the risk mix of the 2 patient samples differed appreciably pre- and postintervention. Per the Moffitt Pathway definition, patients with <2 VTE risk factors are defined as low risk, while those with ≥2 risk factors are defined as high risk. While only 32% of patients were considered high risk at baseline, 71% of patients in the follow-up sample were considered high risk. Since the 2 patient samples were unmatched and the sample sizes small, this difference was most likely attributable to chance imbalance and not related to any changes in clinical or patient behavior.
Guideline-Based VTE Treatment
Based on the number of risk factors and corresponding treatments for each patient, we could infer whether a patient received optimal VTE prophylactic treatments commensurate with their risk category, as recommended by the Moffitt Pathway. Optimal prophylaxis was defined as low-risk patients receiving antiplatelet agents such as aspirin or clopidogrel and high-risk patients receiving anticoagulants such as warfarin, low-molecular-weight heparin, or rivaroxaban. Similarly, patients were defined as “undertreated” if they received no treatment at all or, for high-risk patients, received antiplatelet agents only. [Note: while clopidogrel is not included in guidelines for VTE prophylaxis, we recognized that some patients were already receiving clopidogrel for other indications (such as the presence of a coronary stent) and that dual antiplatelet or clopidogrel and anticoagulant may be associated with increased bleeding risk. Accordingly, we included clopidogrel to account for such instances.]
At baseline, 55% of the patient sample received optimal prophylaxis, and 37% of patients were undertreated. High-risk patients (75%) were significantly more likely to be undertreated than low-risk patients (19%; Figure 3). A significant number of these undertreated high-risk patients were on antiplatelets rather than anticoagulants as recommended by the Moffitt Pathway. It is possible that some of these patients had contraindications that prevented them from receiving anticoagulants, but collected chart data limited our ability to identify these contraindications.
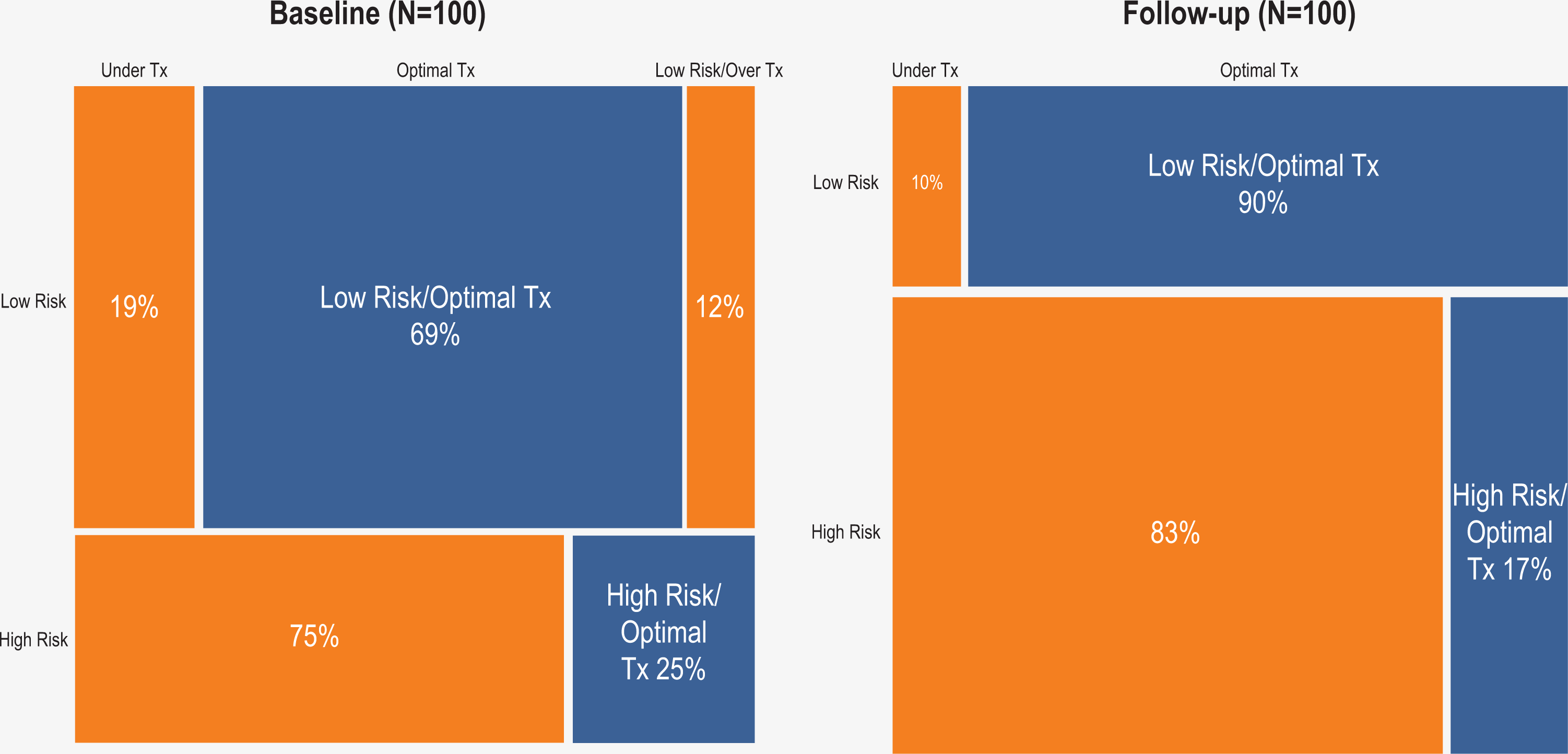
Optimal treatment (optimal tx), undertreatment (under tx), and overtreatment (over tx) at baseline and follow-up, stratified by patient risk.
At follow-up, the proportion of patients receiving optimal prophylaxis decreased from 55% to 38%, while the proportion of undertreated patients increased from 37% to 62%. While this was not the anticipated outcome, it is important to note that the large imbalance in risk mix between the 2 patient cohorts may have confounded these results. Nevertheless, there was an improvement in prophylaxis for the low-risk patient population, where the likelihood of undertreatment decreased from 19% to 10%. This could be partially attributable to more thorough documentation of over-the-counter treatments, which was identified as a practice improvement focus area by the QI team. Additionally, it should be noted that overtreatment of low-risk patients decreased from 12% to 0%.
These numbers are within the range reported by several published sources in the literature in this area. A systematic review of VTE guideline adherence improvement strategies reported that adherence at baseline ranged from 6.25% to 70.4%, and adherence postintervention ranged from 36% to 100%. 16,17
While we saw mixed results in the process metric of appropriate prophylactic treatments, there was a noticeable reduction in VTE events in the follow-up cohort. At baseline, 10% of patients were identified with a current VTE, comparable to published literature on similar populations. 18 In the follow-up cohort, only 4% of patients had a VTE event—a large reduction from baseline, even though this cohort included more high-risk patients. Due to the relatively small sample size and the rare incidence of VTE events, these pre-/postintervention changes in VTE rates were not statistically significant.
Notably, this improvement was seen in a specific subgroup of high-risk patients—those with prior VTE history. Among the 16 patients with VTE history in the baseline cohort, 6 had a subsequent recurrence of VTE event; in comparison, among the 18 patients with VTE history in the follow-up cohort, none experienced such a recurrence (Figure 4). This result was encouraging because this high-risk patient subgroup was identified as a key focus for the QI team. Analysis of baseline data revealed that while VTE history was one of many key risk factors, it was the only factor with statistically significant predictive power for subsequent VTE events. However, in the follow-up cohort, VTE history did not maintain statistically significant predictive power for subsequent VTE events.

Incidence of VTE event within 6 months of data collection at baseline and follow-up, stratified by patient history of VTE events. VTE indicates venous thromboembolism.
A secondary analysis was conducted to investigate whether other factors, in addition to prior VTE history, could reliably predict the likelihood of future VTE events in these patient cohorts. Of interest was the predictive power of patient risk categories (high/low risk) and guideline-based VTE prophylaxis (optimal vs undertreatment). Logistic regression fitting VTE events against these variables found no correlation between these variables and the outcome of interest. In other words, VTE events were no more likely to occur in high-risk patients compared to lower risk patients, or in undertreated patients compared to optimally treated patients. Other risk factors such as obesity, comorbidities, and surgical procedures were also nonpredictive of VTE events.
Discussion
Venous thromboembolism is a common complication and a leading cause of death in patients with cancer. Reported rates of VTE in patients with multiple myeloma range from 2.4% to 9.9% 19,20 and increase from 2.1% at year 1 post-diagnosis to 4.5% at year 10. 21 In a recent review of hospitalized patients with cancer, the average rate of VTE in patients with multiple myeloma was 3.5%, rising to 4.4% in patients who received chemotherapy during their hospital stay. 22
Our program leveraged a multimodal approach to address key system barriers related to guideline adherence for VTE prophylaxis in patients with multiple myeloma. To define and improve the clinical landscape for VTE prophylaxis at Moffitt, we undertook an extensive analysis of current VTE management and outcomes by conducting chart reviews of 100 patients with multiple myeloma in 2015 and with a separate unmatched cohort of 100 patients in 2017. The QI and Education arms of this program were designed to systematically target clinical processes, knowledge gaps, attitudinal blind spots, practice barriers, and patient health literacy over this same feedback period, with the goal of reducing VTE event rates and improving guideline-recommended VTE prophylaxis.
This rigorous approach allowed the QI team to successfully identify local barriers and develop data-driven practice improvement strategies to improve clinical care processes. These strategies focused on high-risk patients with prior VTE events, better documentation of over-the-counter treatments, and the incorporation of an evidence-based checklist into usual practice.
Comparison of pre-/postintervention chart data from unmatched patient cohorts indicated a positive primary outcome, with an observed VTE event rate reduction from 10% to 4%. While not statistically significant, this improvement was clinically meaningful. The reduction in incidence of VTE cannot be directly attributed to the QI project and could have been influenced by other factors such as differences in disease stage (pre-cohort vs post-cohort), changes in therapy trends, and uncaptured use of over-the-counter medications. There were demographic and length-of-treatment differences between the pre- and post- groups of patients with VTE that might have influenced the observed pre- and post- differences in outcomes.
The sample size was underpowered to show that the pre- and post- observed improvement was statistically significant; the post hoc power analysis to detect a difference was only 38%. Sample size was determined by the budget available for data extraction. For the observed difference in VTE to be statistically significant, about 425 patients would have been needed in each cohort. While it would be ideal to look at a more uniform population of newly diagnosed patients, only one-third of the patients in this initiative were newly diagnosed and on first-line therapy. Selecting an even smaller patient subsample for analysis would not have produced statistical or clinical significance. Future studies may benefit from an approach based on selecting more uniform cohorts.
The program achieved mixed results in improving process metrics such as guideline-based VTE prophylaxis. While there was an unattributable decrease in guideline adherence between the 2 cohorts, there was a measurable improvement in guideline-based prophylaxis in the lower-risk population. This result aligns with the Moffitt QI team’s focus on improving documentation for over-the-counter treatments such as aspirin.
This QI educational program had several limitations. First, temporal trends were not addressed as is the usual practice in QI models. Temporal information for this program was not available, per the Moffitt legal department, as dates are considered protected health information under the Health Insurance Portability and Accountability Act. The lack of temporal data did not allow us to assess whether compliance with recommended clinical guidelines at Moffitt was stable or changing over time; statistical process control analyses over time would have been a useful tool to quantify this variance. Second, the lack of patient adherence data may falsely confound our process measurement, as patients may not be fully adhering to prescribed treatments. Third, the relatively small number of patients in our sample sets along with the low incidence of VTE did not have sufficient statistical power to control for all measured variables. Thus, while the QI interventions were well-chosen and led to clinical process improvements and an observed decrease in VTE, the small inpatient population size and low event frequency did not show statistical significance. Continued QI monitoring of VTE events over future years is needed to show statistical and clinical improvement and to guide additional QI initiatives to reduce VTE. To be effective, a QI program needs to be systematic and not episodic, by providing continuous process and outcome monitoring of the QI goal as well as establishing a QI team to implement additional improvements or intervene, when needed, to reduce the gap between current and optimal outcomes. With this objective in mind, the QI team proposed several recommendations to guide future research and investigation. First, there was a desire to develop a better VTE risk stratification framework for patients with multiple myeloma, as current risk factors had very limited predictive power for future VTE events. Specifically, the team suggested several additional risk factors that may be more predictive of VTE risk in multiple myeloma patients—such as number of prior therapies, serum beta-2 microglobulin level, and functional risk factors including frailty and fitness. Second, it is worth investigating whether the literature and the real-world evidence strongly support anticoagulation over antiplatelet treatment among high-risk patients as endorsed by current guidelines. Third, it may be important to better understand whether VTE prevention strategy should vary for multiple myeloma patients in different disease stages—from newly diagnosed to relapsed or refractory patients, or in the maintenance setting. Specifically, there was interest in conducting a follow-up study that stratifies patients by these stages, including patients on maintenance therapy.
Two new risk models for VTE in patients with multiple myeloma were published in 2019. 23,24 A group of US researchers, using a nationwide sample of patients with multiple myeloma, developed and validated a VTE risk stratification score based on 9 variables in patients with newly diagnosed multiple myeloma who were beginning chemotherapy. Predictors of VTE included use of an immunomodulatory drug; body mass index ≥25 kg/m2; pelvic, hip, or femur fracture; use of an erythropoiesis-stimulating agent, doxorubicin, or dexamethasone; history of VTE prior to multiple myeloma; and presence of a tunneled line or central venous catheter. Factors protecting against VTE included use of thromboprophylaxis and Asian/Pacific Islander ethnicity. The score, known as IMPEDE, outperformed the risk stratification in the International Myeloma Working Group guidelines. 23
A second risk assessment model, developed and validated by another group of US researchers, identifies patients with a 2-fold increase in the risk of VTE associated with the use of immunomodulatory drugs. 24 The SAVED model includes 5 variables: surgery within 90 days, Asian race (protective factor), VTE history, Eighty (age >80 years), and Dexamethasone dose. The authors report that this model had greater discriminative power than consensus guidelines recommended by the National Comprehensive Cancer Network. 24
Conclusion
This 2-year QI initiative effectively combined 2 interdependent educational components (QI arm and Education arm)—leveraging electronic medical records audit and feedback, QI pilots, provider education, and patient education—and achieved moderate improvement in VTE prophylaxis outcomes in 2 subpopulations of multiple myeloma patients. Specifically, higher rates of guideline-based prophylaxis were observed in low-risk patients, and a lower incidence of VTE events was observed in patients with prior VTE history. While the reduction in VTE rate was not statistically significant, it is nonetheless noteworthy considering a higher proportion of high-risk patients in the follow-up cohort. In addition, the program was successful in raising provider and patient awareness around issues related to elevated VTE risk in multiple myeloma patients and the need for preventive efforts. Analysis of EMR data revealed limited predictive power of current VTE risk factors and demonstrated the need for additional research to continually refine current VTE prophylaxis guidelines.
The design and implementation of our program is highly scalable and—with appropriate institutional support—can be adopted by other health systems and specialties to address their practice improvement needs. Continuous real-time data monitoring systems for process and outcomes measures, other than the mandated reporting of established quality assurance metrics, are not easily implemented or widely used in health care systems. Similarly, establishing broadly based institutional continuous quality improvement programs has been an ongoing challenge, competing with many other priorities. Successful continuous quality improvement requires executive and clinical leadership commitment, staff QI training and support, development and support of multidisciplinary teams, commitment to process analysis and redesign, and policies recognizing medical staff for QI work. 25
Footnotes
Authors’ Note
This Quality Improvement and Educational program was reviewed and considered exempt by the University of South Florida Institutional Review Board (approval number Pro00021903).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Among the planners of this QI initiative, Beth Finley, BSN, RN, OCN, Moffitt Cancer Center, Patient Education, is on the advisory board of Celgene Corporation and serves on the speaker’s bureau for Amgen and Celgene Corporation; Greg Liptak, IMD, QI study team, discloses that his wife works for Janssen Pharmaceuticals. The following members of the planning team have nothing to disclose: From Moffitt Cancer Center: Viet Ho, Pharm D, BCOP; Benjamin Djulbegovic, MD, PhD; from the QI study team: Elise Furman, RN; from the CME office of USF: Jaclyn Melton, CMP-HC; Cindi Hughlett, CMP; from Haymarket Medical Education: Lynne Callea, CHCP; Scott Scire; Jeff Forster; from Educational Measures: Tyler Nelson.
Correspondng Author Rachid Baz, MD. has received Grant/Research Support from Celgene, Takeda, Karyopharm, Sanofi, AbbVie, Merck, and Bristol-Myers Squibb. Co-authors Roy Furman, MD, PhD; Katherine Simondsen, PharmD, BCOP; and Christine Stone, PhD, MBA, have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The quality improvement initiative was jointly provided by USF Health and Haymarket Medical Education and supported by an independent medical educational grant from Celgene Corporation. Grant ID# 13511.