
Abstract
In the last few years, the treatment of spinal metastases has significantly changed. This is due to the advancements in surgical technique, radiotherapy, and chemotherapy which have enriched the multidisciplinary management. Above all, the field of molecular biology of tumors is in continuous and prosperous evolution. In this review, the molecular markers and new approaches that have radically modified the chemotherapeutic strategy of the most common metastatic neoplasms will be examined together with clinical and surgical implications. The experience and skills of several different medical professionals are mandatory: an interdisciplinary oncology team represents the winning strategy in the treatment of patients with spinal metastases
Keywords
Introduction
In recent years, the treatment of spinal metastases has changed significantly due to the advancements in surgical technique, radiotherapy, and chemotherapy which have enriched the now-essential multidisciplinary management of these patients. The development of new minimally invasive surgical techniques has reduced complications related to surgery, even in more aggressive approaches. 1 Stereotactic radiotherapy has taken a leading role compared to traditional radiation techniques. 2 Finally, and probably most importantly, chemotherapy has evolved, providing greater efficacy in durable control of systemic disease, thus changing the paradigm of management. 3
The identification of multiple molecular markers, which can be exploited as therapeutic targets, has led to a more tailored approach, with tangible improvements in overall survival (OS), progression-free survival (PFS), and quality of life. The field of molecular biology of tumors is in continuous and prosperous evolution. This review will examine the molecular markers and novel approaches that have radically modified the chemotherapeutic strategy of the most common metastatic neoplasms. The most recent literature updates will be examined for each tumor type, and clinical implications will be discussed.
Methods
A comprehensive search was performed on PubMed, ClinicalTrials.gov, and oncology conference websites, using the search terms “lung cancer,” “breast cancer,” “prostate cancer,” “melanoma,” “renal cell cancer,” “thyroid cancer,” “hepatocellular carcinoma,” “colorectal cancer,” “metastases,” “spine metastases,” “molecular markers,” “targeted therapy,” “immunotherapy,” and “immune checkpoint inhibitors.” Only papers published in English were reviewed. Papers were included if they related to the scope of this review.
Tumor types
Lung Cancer
Lung cancer is the most common neoplasm, and metastatic disease is very frequent at diagnosis. 4 Histologically, lung cancer is broadly divided into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC).
Medical treatment for NSCLC improved dramatically during the last few years, thanks to the discovery of new molecular targets. 4,5 It has been reported that up to 60% of lung adenocarcinomas and 50% to 80% of lung squamous cell carcinomas harbor gene mutations in protein kinases or other membrane receptors. 5 New therapies have thus been developed in the form of tyrosine kinase inhibitors (TKIs) and monoclonal antibodies directed against specific receptors.
The mutation of epithelial growth factor receptor (EGFR) is a known predictor of clinical benefit in patients with NSCLC. 4 -11 Epithelial growth factor promotes cellular proliferation and contrasts apoptosis. The EGFR TKIs (Gefitinib, Erlotinib, Afatinib, and Osimertinib), in patients with specific mutations, enhance apoptosis while conversely decreasing cell growth, metastases, and angiogenesis. 12 Mutation in EGFR is more common in adenocarcinomas, nonsmokers, Asian patients, and females. 13 The TKIs (eg, Gefitinib) ensured a longer PFS compared to traditional chemotherapy; without EGFR mutation, PFS was longer in the chemotherapy group. 13,14 Median OS improved up to 24 to 36 months with EGFR inhibitors. 15
A common drug resistance mechanism is the T790M secondary mutation of EGFR. 16 Afatinib was developed as a second-generation inhibitor against EGFR and human epidermal growth factor receptors 2 and 4 (HER2 and HER4), but its effectiveness was not superior to previous EGFR TKIs. 17 A third-generation EGFR TKI, Osimertinib, was effective in T790M+ advanced NSCLC. 18
Anaplastic lymphoma kinase (ALK), another tyrosine kinase receptor, is fused in a small percentage of cases with NSCLC (3%-7%) to the echinoderm microtubule-associated protein-like 4 (EML4) creating the so-called ALK-EML4 fusion oncogene or ALK rearrangement, which promotes cell growth and proliferation. 16 In these cases, a new generation of ALK inhibitors (after Crizotinib) is available (Ceritinib, Brigatinib, and Alectinib) and has become the treatment of choice. 5 This mutation is usually detected in younger patients who have never smoked and in patients with adenocarcinomas. 5,16
Angiogenesis is a hallmark of most neoplasms. In lung cancer, Bevacizumab, inhibiting the vascular endothelial growth factor A (VEGF-A), is the most effective of all angiogenesis inhibitors and promotes tumoral cavitation. 19 In squamous cell carcinomas, it increases the risk of hemorrhage, so it is contraindicated. Bevacizumab promotes a significant improvement in PFS and OS in patients with NSCLC. 7,20,21
Rat sarcoma (RAS) membrane proteins, encoded by multiple genes including Kirsten rat sarcoma virus, are involved in growth signal transduction, and their mutations (detected in 25%-40% of NSCLCs) occur most commonly in adenocarcinomas. 15 Historically, their targeting has not been successful. 5,16 Gainor et al described the mutual exclusivity between mutations in EGFR, ALK rearrangements, and RAS mutations. 22,23
As for immunotherapy, Pembrolizumab and Nivolumab, monoclonal antibodies directed against the programmed death 1 receptor (anti-PD1), have been approved for the treatment of NSCLC. Two phase III clinical trials, the CheckMate 17 and CheckMate 057, showed better results in OS compared to Docetaxel in patients who progressed after platinum-containing chemotherapy as the first line of treatment. 24,25 Pembrolizumab has been approved as a first-line treatment in patients with metastatic NSCLC overexpressing PD-ligand 1 (L1) and is associated with significantly longer PFS and OS and with fewer adverse events than platinum-based chemotherapy. 26 –28 Atezolimumab is an anti-PD-L1 agent recently approved for metastatic NSCLC and disease progression after or during chemotherapy with platinum derivatives. 5 The addition of Ipilimumab, a cytotoxic T-lymphocyte associated protein 4 (CTLA 4) inhibitor, to first-line chemotherapy failed in a phase III trial to prolong OS compared to chemotherapy alone. 29 –31
Other agents currently studied are mitogen-activated protein kinase 2 (MEK) inhibitors, BRAF inhibitors, and vaccines. 7
SCLC is highly radiochemosensitive, but its prompt response to treatments is usually also followed by early recurrence. Effective molecular therapies for this disease are still lacking. A possible approach is based on delta-like 3 (DLL3) targeting: DLL3 is highly expressed by SCLC, and treatment with an antibody–drug conjugate therapy has shown some initial promising results, but clinical efficacy still has to be investigated in larger trials. 32 Main mutations and treatments are summarized in Table 1.
Lung cancer.

Abbreviations: ALK, Anaplastic lymphoma kinase; CTLA, a cytotoxic T-lymphocyte associated protein 4; EGFR, epithelial growth factor receptor; EML4, echinoderm microtubule-associated protein-like 4; HER, human epidermal growth factor receptors; PD1, programmed death 1 receptor; TKI, tyrosine kinase inhibitors; VEGF, vascular endothelial growth factor.
Breast cancer
Breast cancer (BC) is the second cause of cancer-related death among women.
33
Its heterogeneous nature is well known and influences therapeutic strategies. The most important classification of BC is based on the expression of hormone receptors (HRs) and on the amplification/expression of the HER2 gene/protein;
34
these molecular subtypes are: luminal A (HR+/HER2−), slow growing, and less aggressive than the others; luminal B (HR+/HER2+), with poorer prognosis than luminal A; HER2 type (overexpression of HER2/ERBB2 oncogene); and triple negative (HR−/HER2−), more aggressive, and difficult to treat because of early resistance despite its initial sensitivity to chemotherapy.
Luminal A and B
Endocrine therapy is the mainstay for treatment. Drugs are generally used in combination. Tamoxifen blocks estrogen receptors; aromatase inhibitors (letrozole, anastrozole, exemestane) deplete estrogens by blocking conversion from androgens; luteinizing hormone–releasing hormone (LHRH) analogs (leuprolide and goserelin) suppress ovarian production of estrogen; and fulvestrant is a selective estrogen degrader. 34
New agents have been developed to reverse endocrine resistance that usually develops in metastatic BC. Some tumors, after development of hormonal resistance, depend on the CDK4/6–cyclin D1 complex for proliferation. Following Food and Drug Administration (FDA) approval, Palbociclib, Ribociclib, Abemaciclib, and CDK4/6 inhibitors are currently used in combination for advanced BC, prolonging PFS. 35 -39 When mutated, phosphatidylinositol 3-kinase-catalytic subunit p110 α is an important target for combination therapy in advanced BC: Buparlisib, Alpeisib, Talesisib, and Pictillisib show promising effects and are currently under investigation. 40 -44
Entinostat and Vorinostat, histone deacetylase (HDAC) inhibitors, are thought to reverse hormone resistance mediated by the loss of ER expression; they are still under investigation with potential efficacy, if proven, when used in combination in advanced BC. 45 –47 A steroid sulfatase inhibitor, Irosustat, showed clinical benefit when administered in association with an aromatase inhibitor: Steroid sulfatase enzymes are indeed well expressed in hormone-dependent tumors. 48 Everolimus, an mammalian target of rapamycin (mTOR) inhibitor, has received FDA approval for combination therapy in advanced BC. 49
Human epidermal growth factor receptors 2 type
The mainstay of treatment includes anti-HER2 monoclonal antibodies, such as, Trastuzumab and Pertuzumab, which act on different binding sites. Ado-Trastuzumab emtansine is a complex of Trastuzumab and a microtubule inhibitor. Lapatinib is a TKI that blocks HER2 and EGFR pathways. 34 These drugs are used alone or in combination. Novel therapies have been developed against acquired resistance to Trastuzumab. Buparlisib and Pilaralisib, phosphoinositide 3-kinase (PI3K) inhibitors, showed efficacy when administered in combination in advanced BC. The mTOR inhibitors, such as Everolimus, Ridaforolimus, and Sirolimus, and Akt inhibitors, such as MK-2206, revealed promising activity in resistant HER2+ BC. 34 Other targeted therapies include inhibitors of HER-family receptors, such as Neratinib (TKI of HER1/HER2/HER4), Patritumab (anti-HER3 monoclonal antibody), Margetuximab (anti-HER2), and Lonafarnib (Farnesyl transferase Inhibitor). 50 -57
As for immunotherapy, Nelipepimut-S is a peptide derived from HER2 used as a vaccine to prevent recurrence; it is being studied in a phase IIb trial in association with Trastuzumab. 58,59 Recombinant HER2 protein is a protein vaccine under investigation for adjuvant and advanced treatments. 60 -62
Triple negative
It is theoretically the most responsive to chemotherapy but the most difficult to treat because of the lack of targeted therapies and the early resistance to treatments. Chemotherapy usually involves the use of anthracyclines, taxanes, and platinum, sometimes in combination with Bevacizumab. 63
Novel therapeutic strategies, still experimental for now, include poly(ADP-ribose) polymerase inhibitors, probably the most important advancement, such as Olaparib, Talazoparib, Veliparib, Niraparib, and Rucaparib 34 ; EGFR inhibitors such as Cetuximab 64 ; new monoclonal antibodies such as Glembatumumab; 65 and TKIs such as Dasatinib. 66 Main mutations and treatments are summarized in Table 2.
Breast cancer.

Abbreviations: dHER2, recombinant HER2 protein; EGFR, epithelial growth factor receptor; HER, human epidermal growth factor receptors; mTOR, mammalian target of rapamycin; PI3K-CA, phosphatidylinositol 3-kinase-catalytic subunit.
Prostate Cancer
In men, prostate cancer (PC) is the second most common cause of death as it is a neoplastic disease. 4,67 Its increasing incidence has been explained not only by improvements in diagnostic methods but also by poorly defined environmental factors; moreover, androgen hormones have a prominent role in the development of PC. 68 Androgen deprivation therapy is indeed the mainstay of treatment, used as first-line approach for patients with advanced and metastatic PC. 69 Blockade of androgen pathways can be obtained with 3 different treatments 70,71 : (1) LHRH ligands, in the form of agonists downregulating LHRH receptors (Goserelin, Leuproline, and Triptorelin) or antagonists such as Abarelix and Degarelix; (2) blockade of androgen synthesis, mostly inhibiting the upregulated enzyme CYP17 with abiraterone or with Ketoconazole; (c) antiandrogens that antagonize the androgen receptor (AR), such as cyproterone acetate, bicalutamide, flutamide, nilutamide, and enzalutamide. The use of these agents in combination with Docetaxel has recently shown benefit in terms of OS. 72
Tumor progression to the androgen-resistant (or castration-resistant) stage is generally lethal and characterized clinically by bone metastases. 73 The mechanisms of resistance generally involve androgen pathways and include the overexpression and/or mutation of the AR, the upregulation of AR coactivators, the activation of AR by tyrosine kinase receptors linking the androgen-regulated pathway with the growth factor signaling pathways and the intratumoral synthesis of active androgens. 68 In Docetaxel-resistant PC, Cabazitaxel showed promising results in terms of OS when compared to Mitoxantrone. 74 Some new options for therapy of metastatic tumor have been specifically targeted to bone lesions, which are the most common PC metastases. Bisphosphonates inhibit osteoclast activity and bind hydroxyapatite, preventing loss of bone structure and reducing resorption. Thus, they are able to delay clinical consequences of bone involvement. 75 Denosumab inhibits osteoclast proliferation, function, and survival by binding to the receptor activator of nuclear factor kappa-B ligand, therefore delaying functional consequences of bone involvement. 76 A radiomolecule, radium 223, binds to bone and promotes apoptosis in the tumor, improving OS. 77
The era of immunotherapy also involved PC. Vaccine-based strategies are currently under investigation. Sipuleucel-T is the first FDA-approved vaccine that uses prostatic acid phosphatase as tumor antigen. Survival improvement ranges from 4 to 13 months. 78 -81
Checkpoint inhibition is another focus for immunotherapy. Primary targets are CTLA-4 (Ipilimumab), PD1, and the PD1 ligands PD-L1/PD-L2 (Nivolumab, Pembrolizumab, and Atezolizumab). 82 In 2017, pembrolizumab was approved for the treatment of solid metastatic tumors with mismatch repair impairment. Cetuximab, Gefitinib, Erlotinib, and Lapatinib have also been studied. 4 New immunotherapy strategies use engineered immune cells already successful in patients with leukemia or lymphoma: Immune cells are isolated from the patient, engineered to express a chimeric protein composed by a tumor-recognizing antibody region and a T-cell activation domain and then grafted back into the patient (Chimeric Antigen Receptor T cell [CAR-T] therapy). 82,83 Trials with engineered cells for PC are now underway. 84,85 Liver X receptors have recently been proposed as therapeutic targets in resistant PC because of their ability to control apoptosis and modulate androgen and estrogen receptors, with promising results in cell lines and animal models. 82 Main mutations and treatments are summarized in Table 3.
Prostate cancer.

Abbreviations: CTLA, a cytotoxic T-lymphocyte associated protein 4; LHRH, luteinizing hormone–releasing hormone; PD1, programmed death 1 receptor.
Melanoma
Incidence rates of melanoma are still increasing, with excessive ultraviolet radiation exposure as the only known environmental risk factork. 86 Genetic factors also play a crucial role in determining individual risk. 87,88
Only 10 years ago metastatic melanoma was, among the most common types of cancer, the one with the poorest prognosis because of the lack of therapeutic strategies and effective chemotherapeutic drugs. New targeted therapies have revolutionized prognosis in these patients achieving a longer survival and greater control of the disease. 89
A real milestone has been the discovery of BRAF gene mutation (V600) in more than half of melanoma cell lines. 90 The BRAF V600 mutation determines constitutive MAPK pathway activation and proliferation, a key point for tumor growth. 89
In patients with BRAF mutation, the use of BRAF inhibitors (Vemurafenib and Dabrafenib) has thus changed therapeutic strategies. 91,92 Recently, a new BRAF inhibitor, Encorafenib, showed greater benefits compared to Vemurafenib. 93 A combination of BRAF inhibitors with mitogen-activated protein kinase kinase (MEK) inhibitors—like Trametinib, Cobimetinib, or Binimetinib—resulted in longer PFS and OS, compared to BRAF inhibitors alone, and also reduced their toxicity. In a quarter of patients, this new strategy is able to offer even a very long control of the disease (2-3 years in advanced disease) before drugs resistance arises. 94 -98
As for immunotherapy, Ipilimumab (anti-CTLA-4) was shown to improve OS in patients with metastatic melanoma, and it thus received regulatory approval in 2011. 99,100 Long-lasting survival was observed in 20% of cases, even when no complete response was reported, highlighting the potentially curative efficacy of immunotherapy as never described before. 101 Later, in 2014, Nivolumab and Pembrolizumab (anti-PD-1) were approved as first-line treatment for patients with wild-type BRAF and as first or second line for patients with BRAF mutation. This is due to the promising results of 2 phase III studies comparing Nivolumab to Dacarbazine and Pembrolizumab to Ipilimumab, showing better control of the disease in both cases. 102,103 Anti-CTLA-4 and anti-PD-1 drugs have also been studied in combination, with better results in terms of PFS and OS than with each drug alone. 104 Because of toxicity, further studies are needed to define which patients would really benefit from the combination and which would experience increased adverse effects without a significant clinical benefit.
Another field of therapy is that of oncolytic viruses, which reaches in melanoma its most advanced example. Talimogen laherparepvec (T-VEC) is a herpes simplex virus type 1 able to promote, after genetic engineering, tumor cells lysis and immune responses after antigen release and granulocyte-macrophage colony-stimulating factor. It was approved in 2015 for local treatment of recurrence after surgery. 105 Optimization of therapy with T-VEC in combination with immunotherapy has been explored with promising results. Other oncolytic viruses, vaccines, and a metabolic modulation approach (epacadostat) are currently under investigation. 106 -109 Main mutations and treatments are summarized in Table 4.
Melanoma.

Abbreviations: CTLA, a cytotoxic T-lymphocyte associated protein 4; PD1, programmed death 1 receptor; T-VEC, Talimogen laherparepvec.
Renal Cell Cancer
Renal cell carcinoma is a common cause of widespread metastases at diagnosis. 110 The median OS was very poor before the introduction of targeted therapy, when interleukin-2 and interferon α were used as immunotherapy. The scenario dramatically changed in the mid-2000s with the introduction of targeted therapy against VEGF: new strategies included TKIs such as Sunitinib (the most frequently used), Pazopanib, Axitinib, or Sorafenib or monoclonal antibodies such as Bevacizumab. 110 -115 Other studies concentrated on Temsirolimus or Everolimus. 116,117
In the last few years, new trials investigated immunotherapy. CheckMate 214 showed better results in terms of objective response rate, PFS, and OS with the use of Nivolumab plus Ipilimumab compared to Sunitinib. 118 CABOSUN 119 -121 revealed benefits with the use of Cabozantinib. Many trials are currently underway, with other new regimens involving the mentioned drugs or others such as Atezolizumab, Pembrolizumab, Avelumab, or Lenvatinib. 122 Vaccines are also being studied with different targets. 123,124 Main mutations and treatments are summarized in Table 5.
Renal Cell cancer.
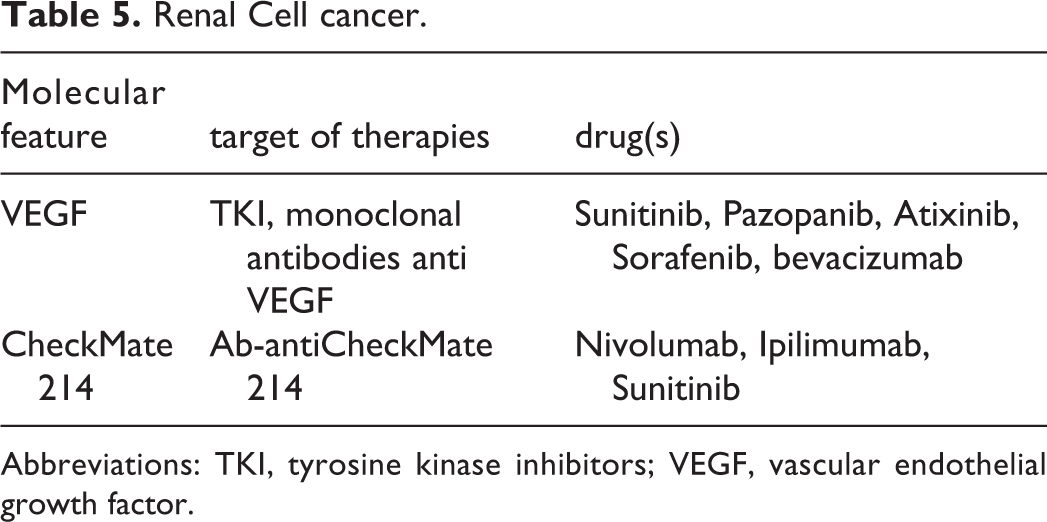
Abbreviations: TKI, tyrosine kinase inhibitors; VEGF, vascular endothelial growth factor.
Other Tumors
Thyroid cancer
A small percentage of patients with differentiated thyroid carcinoma (DTC, 15%-20%), anaplastic carcinoma, and medullary thyroid carcinoma (MTC, 30%) could experience resistance after standard therapy. 125 The use of Sorafenib and Lenvantinib for DTC and Vandetanib and Cabozantinib for MTC, with their ability to block the MAPK pathway, has changed their prognosis. 125 -127 However, further resistance to these drugs has been recorded and explained with the activation of parallel pathways. After scientific advances regarding the understanding of these mechanisms, new strategies are currently under investigation, such as targeting the PI3K pathway, ALK translocations, HER2/3 receptors, the restoration to radioactive iodine sensitivity, immunotherapy (anti CTLA-4 and anti-PD-1), or vaccines. 125 Main mutations and treatments are summarized in Table 6.
Thyroid cancer.

Abbreviation: MAPK, mitogen-activated protein kinase.
Hepatocellular carcinoma
Sorafenib was approved in 2007 and remained the only treatment for advanced hepatocellular carcinoma until the approval of Lenvatinib. 128 -130 For second-line therapies, only in the last 2 years, new strategies have become the standard of care, with the recent introduction of Regorafenib and Nivolumab. Cabozantinib and Ramucirumab (that bind to VEGFR-2) also showed benefits in advanced disease. 131 Various clinical trials with immunotherapy are currently underway. CAR-T therapy has shown promising, although only preliminary, results. 132,133 Main mutations and treatments are summarized in Table 7.
Hepatocellular carcinoma.

Abbreviations: MAPK, mitogen-activated protein kinase; VEGFR, vascular endothelial growth factor receptor.
Colorectal cancer
Conventional chemotherapy still retains its role and efficacy in slowly progressing or metastatic disease as first-line treatment and involves the use of fluoropyrimidine, oxaliplatin, and irinotecan. 134 Strong evidence suggests that biological agents, targeting VEGF or EGFR pathways (Bevacizumab; Cetuximab, and Panitumumab), also constitute a valuable option for first-line treatment in combination with conventional chemotherapy. The RAS mutation status is a routinely used test to investigate the efficacy of anti-EGFR antibodies. TAS102 is a synthetically engineered fluoropyrimidine that showed to prolong PFS and OS. 135 New targeted strategies include analysis of mismatch repair function to predict benefits using checkpoint inhibitors, BRAF mutations, and HER2 amplifications. 133 Current studies investigate Regorafenib, Nivolumab, Pembrolizumab, Ipilimumab, Trastuzumab, and Pertuzumab. 134,136 -142 Main mutations and treatments are summarized in Table 8.
Colorectal cancer.
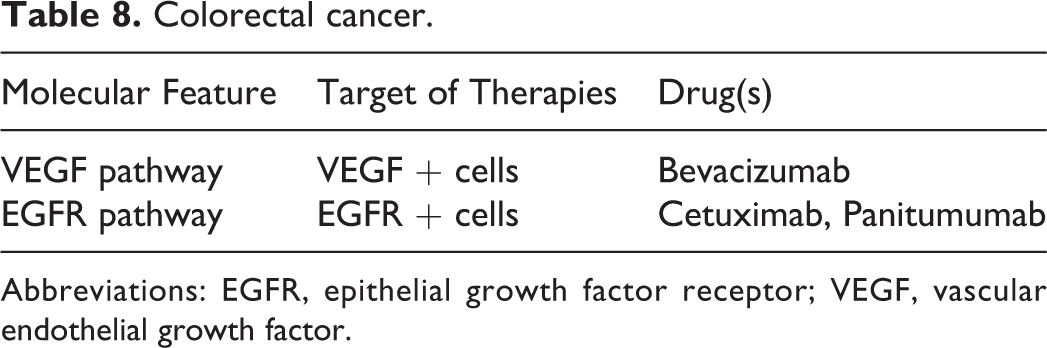
Abbreviations: EGFR, epithelial growth factor receptor; VEGF, vascular endothelial growth factor.
Lymphohematopoietic malignancies
Even if not strictly considered as metastases, spinal localizations of myeloma and non-Hodgkin (NH) lymphoma deserve a concise discussion about therapeutic advancements.
Myeloma
Significant advancements improved the outcome of patients with myeloma in the last decade. 143 The development of proteasome inhibitors (Bortezomib, Carfilzomib, and Ixazomib) and immunotherapy significantly changed survival and helped improving depth and duration of response. 144,145 One of the first immunotherapies in myeloma was allogenic stem cell transplantation, associated with a high rate of treatment-related mortality. 143 This is why novel and well-tolerated forms of immunotherapies have been approved and currently used while others are under clinical investigations. Among them, immunomodulatory drugs (such as Thalidomide, Lenalidomide, and Pomalidomide, respectively first, second, and third generation) are currently used in several treatment combinations. 146 -150 Two main monoclonal antibodies have been studied 143,151 -154 : Elotuzumab, against the signaling lymphocytic activation molecule F7 (SLAMF7), has been studied in combination with Bortezomib and Dexamethasone resulting in improved OS. Daratumumab, against CD38, is currently approved as monotherapy in relapsed/refractory myeloma or in combination with Bortezomib–dexamethasone, Pomalidomide–dexamethasone, or with Bortezomib–Melphalan–Prednisone. Novel immunotherapies, currently under investigations with promising results, involve chimeric antigen receptor T cells (anti-BCMA CAR T-cells), bispecific antibodies such as bispecific T-cell engagers, immune checkpoint inhibitors (PD-1/PD-L1 inhibitors like Pembrolizumab), and dendritic cell vaccination. 143,155 -157 Main mutations and treatments are summarized in Table 9.
Myeloma.

Abbreviation: PD1, programmed death 1 receptor.
Non-Hodgkin Lymphoma
The vast majority of mortality in NH Lymphoma is caused by aggressive subtypes of B- and T-cell NH Lymphoma. These diseases are very heterogeneous in their molecular pattern. This is why novel therapies provide only limited benefits since now despite the acquisition of knowledge of a large number of molecular targets. Nevertheless, new studies seem to identify subtypes able to respond differentially to specific therapies for NH Lymphoma. 158
New agents have been developed following different pathways and depending on the unique biology of the tumors 157 -167 : Among the others, Fostamatinib and Ibrutinib target the B-cell receptor (Syk and Btk); Venetoclax acts in the apoptosis process (BCL-2 as target); Nivolumab (anti-PD-1 monoclonal antibody) works as a checkpoint inhibitor; Duvesilib, MK2206, and Everolimus target the PI3K/AKT/mTOR complex; and RG6146, Tazemetostat, and Romidepsin work modifying the epigenetic regulation (BET BRD, EZH 2, and HDAC). These agents showed promising results in different trials. Probably, different molecular aberrations and biological subgroups, as well as the understanding of their role in the single patients, will provide a better rationale for therapy in the next years. 158 Main mutations and treatments are summarized in Table 10.
Non-Hodgkin Lymphoma.

Abbreviations: mTOR, mammalian target of rapamycin; PD1, programmed death 1 receptor; PI3K, phosphatidylinositol 3-Kinase.
Conclusion
Changing Approach in Spine Metastases
Since patients with cancer are living longer, it is well known that the number of patients with spinal metastases will continue to grow. The advent of targeted therapy in the last 10 years has revolutionized the life expectancy of these patients, and further improvements are expected in the coming decades. The goal for the cancer team is to not neglect the clinical and radiological status of patients with spinal metastases. Surgical treatment and radiotherapy of spinal metastases play a crucial role in the therapeutic approach as confirmed by several authors which collected clinical results of this last decade of targeted strategies. Furthermore, complications related to spinal metastases often limit further treatments because of the resulting significant clinical impairment.
The implications of the remarkable therapeutic novelties in the treatment of spinal metastases are large, according to the existing literature. 2,168 -170 These patients should receive the maximal safe treatment to improve the quality of their potentially still long residual life, taking into account their clinical conditions and systemic status. Patients treated for spinal metastases should be referred to centers with sufficient experience and interdisciplinary networks. The experience and skills of several different medical professionals are mandatory: An interdisciplinary oncology team represents the winning strategy in the therapeutic approach.
As about surgery, every effort must be focused on preventing spinal cord damage in the affected segments and pathological collapses due to instability, since paraplegia dramatically reduces prognosis representing thus a defeat for the oncology team. Based on the histopathology and the molecular pattern of the tumor, different surgical strategies could be performed. Separation surgery is a valid and recognized therapeutic step in case of epidural compression to allow the best radiation treatment for high radiosensitive tumors or before radiosurgery. The feasibility and the oncological meaning of aggressive cytoreductive procedures such as en bloc corpectomies in single locations and in patients with a favorable tumor profile should be further investigated to strengthen evidence and should be compared to radiosurgical treatments. More aggressive treatments could also be justified with the increase in life expectancy to face spinal instability and prevent mechanical damage.
Modern technological aids available for surgery helped to reduce postoperative complications and hospitalization. Every modern spinal oncological surgical center should consider and promote the use of the most innovative techniques: instruments for minimally invasive approaches, percutaneous and transfascial systems, and navigation. Among new strategies, carbon fiber instrumentation represents an excellent synthesis between surgical and radio therapeutic needs and should be adopted by all centers supported by long-term studies.
Footnotes
Acknowledgments
This study was produced in the Dept. of Neuroscience “Rita Levi Montalcini” and was supported by Ministero dell’Istruzione, dell’Università e della Ricerca—MIUR project “Dipartimenti di eccellenza 2018-2022.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.