
Abstract
Only limited data are available concerning the long-term outcomes of imatinib treatment among Vietnamese or Asian patients with unresectable or recurrent gastrointestinal stromal tumors (GISTs). Our study, which was conducted in 188 patients, aimed to assess the efficacy of imatinib mesylate against unresectable or recurrent GISTs. Imatinib had a high response rate and long survival. Some predictors favorable for progression-free survival and overall survival are good performance status and response with imatinib. Findings are discussed in relation to clinical practice in low- and middle-income country.
Introduction
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal neoplasms of the gastrointestinal tract. 1 Epidemiological data of GISTs have thus not been available all over the world. 2 Some country reported extreme differences in incidences from lowest (5.2 in 1,000,000) in Czech Republic 3 to highest (21.1 in 1,000,000) in China. 4 In Vietnam, no data of GISTs incidence have been reported. Gastrointestinal stromal tumors express the cell surface transmembrane receptor kit with a tyrosine kinase activity. There are frequent gain-of-function mutations of kit in GISTs. 5 These mutations result in constitutive activation of kit signaling, which leads to uncontrolled cell proliferation and resistance to apoptosis. 5 Prior to 2001, there was no known effective therapy for unresectable or metastatic GISTs. 6 However, the association between constitutively activated KIT and platelet-derived growth factor receptor A signaling and GISTs oncogenesis provided justification for testing a small-molecule tyrosine kinase inhibitor in this tumor type. 5 Imatinib mesylate (IM) selectively inhibits certain protein tyrosine kinases: intracellular ABL kinase, chimeric BCR-ABL fusion oncoprotein of chronic myeloid leukemia, transmembrane receptor KIT, and PDGFRs. Since the initial report of a patient with rapidly progressive GISTs exhibited a dramatic response, 7 several trials have shown a promising effect of this target therapy. 8,9 Imatinib mesylate has revolutionized the treatment of GISTs and become standard of care in unresectable or recurrent stage in adjuvant setting.
Imatinib mesylate has been used in Vietnam to treat GISTs since 2009, based on the support of the Max Foundation. However, no previous study has evaluated the long-term impact of IM on patient response and survival in Vietnam, also in other low- and middle-income countries. Nor has any previous study evaluated predictors for favorable progression-free survival (PFS) and overall survival (OS) of Vietnamese patients with GISTs receiving IM. We retrospectively collected the data from a decade of use of IM in a large single institute, including 188 patients with unresectable or recurrent GISTs. The objectives of this study were to (1) evaluate the efficacy and survival outcomes of imatinib treatment for Vietnamese patients with unresectable or recurrent GISTs and (2) identify the variables predictive of survival.
Methods
From January 2009 to September 2018, a retrospective, cross-sectional study was conducted to evaluate the effect of IM in inducing an objective response or stable disease (SD) in Vietnamese with unresectable or recurrent GISTs. The study was conducted at Vietnam National Cancer Hospital—K Hospital, the only 1 hospital that has the team of experts who treat patients with GISTs in the North Region of Vietnam.
Patients Selection
Eligibility criteria included adults with histologically confirmed, unresectable, or recurrent GISTs that expressed the CD117 antigen (as a marker of the KIT receptor) and with measurable lesions based on Response Evaluation Criteria in Solid Tumors (RECIST). 10 Other eligibility criteria included an Eastern Cooperative Oncology Group (ECOG) performance score of 3 or less. Patient must had the following laboratory values confirmed within 14 days prior to first dose of imatinib study drug: total bilirubin <1.5 × upper limit of normal (ULN), alanine aminotransferase and aspartate transaminase <2.5 × ULN, creatinine <1.5 × ULN, absolute neutrophil count >1.5 × 109/L, and platelets > 100 × 109/L. Patients were excluded if they exhibited class 3 or 4 cardiac problem or any severe medical condition. Patients could not be pregnant or nursing.
One hundred eighty-eight patients were administered 400 mg of IM in 100 mg capsules, taken orally daily with food. Patients were treated until disease progression or unacceptable toxicity. Patients had regular physical examinations, evaluations of performance status, body weight, complete blood count, and serum chemistry twice monthly for the first 2 months and then monthly times, 6 then every 3 months. Standard computed tomography was performed at the end of month 2 and then every 3 months thereafter to assess the patient’s response. Responses were assessed by RECIST. 10 If progression was documented, patients offered continued best supportive care or another drug followed local standard.
Progression-free survival was defined as no progression after administration of IM and was calculated from the date of the start of IM treatment to the date of the most recent follow-up, or progression, or death due to the disease. Overall survival was calculated from the date the start of IM treatment to the date of the most recent follow-up or death due to the disease.
Toxicities were assessed using the National Cancer Institute Common Toxicity Criteria, version 2.0 (NCI-CTCAE v.2.0 criteria). Imatinib was withheld in the event of any clinically significant grade 3 toxicity, until resolution to grade 1 (except as noted in “hematologic toxicity”), imatinib could be reintroduced at the same dose, whereas any grade 4 toxicities required mandatory dose reduction on restarting imatinib (400 mg reduced to 300 mg daily). For third time dose interruption, grade 3 or 4 appeared, a dose reduction required. A second dose reduction following similar rules was allowed (to 200 mg daily, respectively). The treatment dose below 200 mg/d was not allowed. No dose delays or modifications were required for hematologic grade 2 toxicities. The use of growth factors was permitted but not recommended. Other medications for management adverse events were permitted.
The study was approved by the local institutional review board of Vietnam National Institute for Cancer Control and National Cancer Hospital, and written informed consent for drug administration was obtained independently from each patient.
Data Analysis and Statistical Methods
Baseline characteristics of the patients and their tumors were presented as percentages (categorical variables) or means with standard deviation (continuous variables). Survival analyses were performed using Kaplan-Meier methods. Cox proportional hazard models were used to evaluate the relationship between potential prognostics variables and PFS and OS. The following potential prognostic variables were investigated: age (<65 years vs ≥65 years), sex, ECOG performance status (score ≤1 vs >1), summed diameter of 5 target tumor lesions (<10 cm vs ≥10 cm), response (complete response [CR] + partial response [PR]), disease control (CR + PR + SD vs progressive disease [PD]). Two versions of Cox models were analyzed. Model 1 was an unadjusted model to evaluate each potential prognostic factor. Model 2 included all potential prognostic factors that were statistically significantly associated with risk in model 1 and which remained after an enter-selection procedure was applied to select the most relevant prognostic factors. Only factors that remained significant at the .05 level during the selection procedure were included in the final model. All statistical analyses were performed using SPSS computer software package (version 16.0; SPSS, Inc, Chicago, Illinois). P < .05 was considered statistically significant.
Results
Characteristics of the Patients and Their Tumors
Table 1 summarizes the characteristics features of 188 patients with unresectable/recurrent GISTs treated with IM. There were 122 men and 66 women, with a median age of 55.8 years (range = 25-84 years). The median tumor size before IM treatment was 11.3 cm (range = 3.5-30.0 cm). Stomach was the most common site for GISTs treated with IM (81/188, 43.1%), followed by small intestine (56/188, 29.8%). The most common symptom for presentation with advanced stage of GISTs was abdominal pain.
Characteristics of 188 Vietnamese With Unresectable/Recurrent GISTs.

Abbreviations: GISTs, gastrointestinal stromal tumors; IM, imatinib mesylate.
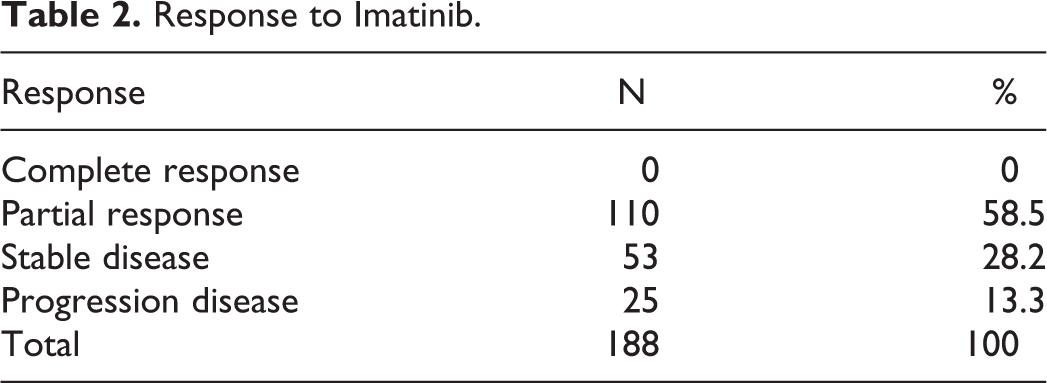
Response
Overall, none of patients had CR, 110 (58.5%) had PR, 53 had SD (28.2%), and 25 had PD (13.3%). Of all patients, 86.7% had a clinical benefit.
Safety and Tolerability
Imatinib was reasonably well tolerated overall, although mild-to-moderate toxicities were common. Grade 3-4 adverse events occurred less than 10%, except anemia 12.8% (Table 2). The most common adverse effects were periorbital edema, diarrhea, neutropenia, and anemia.
Response to Imatinib.
Dose Modifications/Delivered Dose Intensity
In all, 39 (20.7%) patients had at least one-time delay and 9 (4.8%) patients had dose reduction, due to grade 3-4 adverse events (Appendix).
Survival analysis for 188 patients with unresectable or recurrent GISTs receiving imatinib
The median follow-up period after IM was 40.8 months (range = 2.0-113 months), no patient lost at follow-up. Of these 188 patients, 117 (62.2%) developed progression and 86 (45.7%) died due to GISTs. The 188 patients with unresectable or recurrent GISTs had a median PFS of 45.5 months (Figure 1) and OS of 62.2 months (Figure 2).

Progression-free survival of 188 Vietnamese with unresectable or recurrent GISTs treated with IM. GISTs indicates gastrointestinal stromal tumors; IM, imatinib mesylate.

Overall survival of 188 Vietnamese with unresectable or recurrent GISTs treated with IM. GISTs indicates gastrointestinal stromal tumors; IM, imatinib mesylate.
Predictors of PFS
Associations between potential predictors of PFS and OS are presented in Tables 2 and 3, respectively. Although sex, the size of the tumor prior to treatment, and the anatomical origin of the tumor were associated with risks of PFS or OS in initial models, they were not independently associated after adjustment for other factors. Age greater than 65 was independently associated with a nearly 2-fold increased risk of PFS after adjustment for other factors (hazard ratio [HR]: 1.91; 95% CI [confidence interval]: 1.12-3.06) (Table 4) but was not associated with OS. However, both ECOG status and response were independently and strongly associated with both PFS (Table 4) and OS (Table 5). A poorer ECOG status was associated with increased risk of PFS (HR: 2.67; 95% CI: 1.77-3.90) and increased risk of OS.
Grade 3-4 Adverse Events Related to Treatment.

Prognostic Factors for PFS Among Vietnamese Patients With Unresectable or Recurrent GISTs Treated With IM.

Abbreviations: CI, confident interval; ECOG, Eastern Cooperative Oncology Group; GISTs, gastrointestinal stromal tumors; IM, imatinib mesylate; NA, not applicable; PD, progression disease; PFS, progression-free survival; PR, partial response; SD, stable disease.
a Derived from an unadjusted Cox proportional hazard model.
b Derived from a Cox proportional hazards model including all factors in the table which were significantly associated with risk in model 1.
Prognostic Factors for OS Among Vietnamese Patients With Unresectable or Recurrent GISTs Treated With IM.

Abbreviations: CI, confident interval; ECOG, Eastern Cooperative Oncology Group; GIST, gastrointestinal stromal tumor; IM, Imatinib mesylate; OS, overall survival; PD, progression disease; PR, partial response; SD, stable disease.
a Derived from an unadjusted Cox proportional hazard model.
b Derived from a Cox proportional hazards model including all factors in the table which were significantly associated with risk in model 1.
Discussion
Limited data are available concerning the long-term outcomes of imatinib treatment in Vietnamese or Asian patients with unresectable or recurrent GISTs. In our study, we observed a median PFS of 45.5 months and OS of 62.2 months. Our result suggested that IM is equivalently effective in this setting in Vietnam.
The length of survival in our study is superior to other studies, which have reported PFS or OS in other populations. The B2222 study, 11 which was conducted in the United States and Finland, reported a median PFS of 24 months and OS of 57 months. 11 Thus, in the B2222 study, a large number of patients were treated with combined chemotherapy regimens or radiation therapy unlike our study in which all patients were treated with IM in first-line settings.
The time between progression and death in our study is shorter than the studies in upper-, middle-, or high-income country. According to Casali et al’s study done in high-income countries, the median PFS and OS is 1.9 and 3.9 years, respectively. 12 This is likely due to a lack of access to other subsequent therapy alternatives for patients in Vietnam, including tyrosine kinase inhibitors or intensive surgery. In our setting, all of the patients receive increased doses of IM when their disease progresses.
We also noticed that survival tended to be better in this study. Several explanations may account for the longer survival of the patients in the current study. First, the mean body weight (58 kg) of our patients is lower than that of patients in the imatinib trials conducted in Western countries. 11,12 In pharmacokinetic models, high clearance of imatinib correlates, especially with high body weight among demographic parameters. 13 Therefore, the lower body weight in Asian populations may alter the pharmacokinetic distribution of imatinib and consequently contribute to differences in outcome compared to Western cohorts. Demetri et al demonstrated that higher imatinib trough levels (1100 ng/mL) were associated with a significantly better clinical benefit in patients with GISTs. 14 Although our study had not analyzed plasma imatinib concentration, we assumed that our population has the same body weight in Japanese or Korean. Two studies in Japan and Korean showed that with a normal dose 400 mg/d, the trough levels exceeded 1000 ng/mL in all cases, 15 and the efficacy was higher than that in Western countries. 15,16 Thus, imatinib dose escalation (600 or 800 mg/d) is a choice of treatment after failure with standard-dose (400 mg/d) imatinib.
We also evaluated factors associated with PFS and OS among our population of patients treated with IM. Lee et al presented and discussed prognostic nomograms for GISTs and found that response status was most strongly associated with survival. 17 Some studies also found out that patients who had best response will live longer and who had progressed will have shorter survival time. 11,12,18
Blanke et al and Patel conducted randomized control trial and meta-analysis and observed that ECOG status was associated with PFS and OS . 11,12,19 Theoretically, patients who has poor performance status (ECOG ≥2) have more difficulty tolerating cancer treatments. These patients have less favorable outcomes than more fit patients with better performance status, regardless of the treatments given.
Demetri et al and Blanke et al also identified some predictors and did not show that sex as well as other laboratory data were independently associated with either PFS or OS, similar to our study. Our study is limited by its retrospective design and the data were collected in one location. However, the study cohort of 188 patients was not really small when one considers the low prevalence of GISTs and is likely representative of Vietnamese population. The mutation status of tumor is identified as the most relevant to GISTs prognostic, although it was not analyzed in this study. This could affect to our Cox model analysis. The role of tumor mutation status on this population needs further investigation in the future.
To the best of our knowledge, this is one of the largest series evaluating predictors for PFS and OS among patients treated for unresectable or recurrent GISTs with IM in Vietnam. Although it is the first report from Vietnam, we were limited in the sample size for some analyses as well as for the availability of some characteristics. However, a strength of our study is that it was conducted in a single center in which treatment is used routinely.
In conclusion, the median PFS and OS of 188 patients with unresectable or recurrent GISTs who are older than 65 years are 45.5 and 62.2, respectively; poor performance with ECOG 2 or 3; and primary resistance were independently associated with an unfavorable PFS. Regarding OS, good performance status and good response were independent favorable predictors. The findings from this study may be useful for understanding prognosis for GISTs after treatment with IM in a developing country like Vietnam and other similar settings in the world. The current study suggests that survival outcomes with imatinib may differ somewhat from those observed in European and the United States. Racial differences in the pharmacokinetic distribution of imatinib and in the relationship between treatment outcomes and gene mutations need to be explored in future studies.
Footnotes
Appendix
Authors’ Note
The study was approved by Vietnam National Cancer Hospital and Vietnam National Institute for Cancer Control and informed consent for drug administration was obtained independently from each patient. All patients had complete rights to withdraw from the study at any time without any threats or disadvantages. Ethical approval for this study was obtained from Vietnam National Institute for Cancer Control review board (IRB-VN 01034).
Acknowledgments
The authors thank GIPAP program that is being implemented by Max Foundation for providing access to Glivec (imatinib) for patients in Vietnam. The authors thank Professor Shrubsole Martha from Vanderbilt University Medical Center for editing language contents of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.