
Abstract
Background:
An increasing amount of attention has been paid to minimally invasive function-preserving gastrectomy, with an increase in incidence of early gastric cancer in the upper stomach. This study aimed to compare oncological outcomes, surgical stress, and nutritional status between robot-assisted proximal gastrectomy (RAPG) and laparoscopy-assisted proximal gastrectomy (LAPG).
Methods:
Eighty-nine patients were enrolled in this retrospective study between November 2011 and December 2013. Among them, 27 patients underwent RAPG and 62 underwent LAPG. Perioperative parameters, surgical stress, nutritional status, disease-free survival, and overall survival were compared between the 2 groups.
Results:
Sex, age, and comorbidity were similar in the RAPG and LAPG groups. There were also similar perioperative outcomes regarding operation time, complications, and length of hospital stay between the groups. The reflux esophagitis rates following RAPG and LAPG were 18.5% and 14.5%, respectively (P = .842). However, patients in the RAPG group had less blood loss (P = .024), more harvested lymph nodes (P = .021), and higher costs than those in the LAPG group (P < .001). With regard to surgical stress, no significant differences were observed in C-reactive protein concentrations and white blood cell count on postoperative days 1, 3, and 7 between the groups (Ps > .05). There appeared to be higher hemoglobin levels at 6 months (P = .053) and a higher body mass index at 12 months (P = .056) postoperatively in patients in the RAPG group compared with those in the LAPG group, but this difference was not significant. Similar disease-free survival and overall survival rates were observed between the groups.
Conclusions:
RAPG could be an alternative to LAPG for patients with early gastric cancer in the upper stomach with comparable oncological safety and nutritional status. Further well-designed, prospective, large-scale studies are needed to validate these results.
Keywords
The prevalence of early gastric cancer (EGC) in the upper location has been increasing. 1,2 The standard treatment for proximal EGC is total gastrectomy, but the postoperative nutritional status of patients is not satisfactory. For cT1 tumors, proximal gastrectomy with proper lymph node dissection is acceptable according to the Japanese gastric cancer treatment guidelines (third edition). 3 After proximal gastrectomy, patients suffer a reduction in volume of food intake and indigestion syndromeless frequently compared with patients undergoing total gastrectomy. 4,5 This leads to a potentially better nutritional status postoperatively. Since Uyama et al 6 first reported laparoscopy-assisted proximal gastrectomy (LAPG) in 1995, an increasing number of surgeons have performed this function-preserving and minimally invasive surgery. 7 -10 A recent study also showed that LAPG may have advantages of less surgical invasiveness and postoperative nutritional benefit over laparoscopy-assisted total gastrectomy (LATG) for upper EGC. 11
Robotic surgical systems have advanced minimally invasive surgery to a new stage. Robot-assisted surgery is characterized by tremor filtration and the ability to scale motion and stereoscopic vision, which facilitate precision surgery and accurate lymph node dissection. 12 Robotic systems are widely used for urinary carcinoma, cardiovascular disease, and gynecological tumors. 13 -15 With regard to gastric cancer, Suda and colleagues reported that robotic radical gastrectomy might improve short-term postoperative outcomes compared with the conventional laparoscopic approach because it potentially reduces surgery-related complications. 16 However, the superiority of robotic surgery over laparoscopic gastrectomy has not been clarified because there have not been any prospective, randomized clinical trials. 17,18 Additionally, there is little evidence regarding the comparison of robot-assisted proximal gastrectomy (RAPG) and LAPG for EGC in the upper location.
Therefore, the present study aimed to compare the short- and long-term oncological outcomes, surgical stress, and nutritional status between RAPG and LAPG. We also evaluated the financial costs for these procedures.
Materials and Methods
Patients
Between November 2011 and December 2013, a total of 89 patients (27 in the RAPG group and 62 in the LAPG group) with clinical stage I gastric cancer were identified from a prospectively maintained database at the Department of General Surgery, Chinese PLA General Hospital. All of the patients received a preoperative examination, including endoscopic biopsy and ultrasound, and abdominal and pelvic computed tomography. Tumors were classified according to the Japanese classification of gastric carcinoma. 19 After preoperative assessment, patients who requested for minimally invasive surgery made their decisions to receive RAPG or LAPG after a detailed explanation on each procedure. Patients were dichotomized into RAPG and LAPG group based on the type of operative procedures. All patients provided written informed consent. The inclusion criteria were as follows: (i) EGC was diagnosed as a <5-cm-diameter cT1N0 lesion in the upper location, (ii) RAPG or LAPG was performed for proximal tumors where more than half of the distal stomach was preserved, (iii) there was no conversion to open surgery (incisions that extended for 8 cm were defined as open surgery), and (iv) complete perioperative data were obtained. The study has been approved by Chinese People’s Liberation Army General Hospital Research Ethics Committee (no. 201700231).
Surgical Approach
All operations were performed by L.C. and B.W. Except for robotic instruments, the surgical procedures of RAPG and of LAPG for gastric cancer were similar. Under general anesthesia, the patients were placed in the reverse Trendelenburg position with legs apart. Pneumoperitoneum was established through a subumbilical, 12-mm port with carbon dioxide to maintain a pressure of 12 to 15 mm Hg. After exploration of the abdominal cavity to confirm the absence of any lymph node enlargement or any suspected metastasis, 2 trocars were inserted on the left and right sides of the abdomen. The placement of trocars in RAPG and LAPG was almost the same, but the size of the trocar was different between the procedures. 20 D1+ lymphadenectomy for proximal gastrectomy, including dissection of nos 1, 2, 3a, 4sa, 4sb, 7, 8a, 9, and 11p, was performed according to the Japanese guidelines. 3 Initially, the gastrocolic ligament was divided up to the lower pole of the spleen. The gastric body and gastrocolic ligament were held to keep the field open. The left gastroepiploic vessels were divided, and no. 4sb lymph nodes were dissected. The gastrosplenic ligament was then divided up to the left side of the esophageal hiatus by dividing the short gastric vessels and dissecting the no. 4sa lymph nodes, after which the no. 2 lymph nodes were dissected. The stomach and the greater omentum were lifted to expose the superior border, and the common hepatic artery was exposed toward the root of the left gastric artery. This was followed by dissection of no. 8a lymph nodes and the right side of no. 9 lymph nodes. The left gastric vessels were subsequently exposed and divided with clips at the root, and the no. 11p lymph nodes and the left side of no. 9 lymph nodes were dissected. The right side of the cardia was exposed and the regional lymph nodes were then dissected. The anterior and posterior vagal nerves were resected in most cases. Finally, the esophagus was exposed and transected for creation of an esophagogastric anastomosis. The abdominal esophagus was preserved as much as possible to preserve the lower esophageal sphincter. The anvil of a circular stapler was placed into the esophagus transorally.
After intracorporeal lymph node dissection, gastrectomy and esophagogastrostomy (EG) were performed extracorporeally through an approximately 7-cm incision in the upper abdomen. After the vessels of the lesser and greater curvatures were divided, the gastric body was transected using a linear stapler. The resection line was approximately 5 cm distal to the tumor distal margin. A 4-cm vertical incision was made on the anterior wall of the residual stomach, through which the circular stapler was inserted. The center rod was pierced through the posterior wall of the residual stomach and docked with the anvil in the esophagus. The opening of the residual stomach was sutured manually under direct vision through the midline minilaparotomy.
Perioperative Data
Information on baseline characteristics of the patients, including sex, age, body mass index (BMI), physical status, and comorbidity, was collected. Surgical and pathological data were also collected. Short-term outcomes, such as morbidity and postoperative hospital stay, were recorded. Morbidity was classified into early and late complications. Complications greater than or equal to grade II according to the Clavien-Dindo classification 21 at 30 days postoperatively were defined as early complications. Late complications occurred after 30 days. Reflux esophagitis was diagnosed endoscopically and was graded according to the Los Angeles classification as follows 22 : grade A, 1 or more mucosal breaks <5 mm in maximal length; grade B, 1 or more mucosal breaks >5 mm, but without continuity across mucosal folds; grade C, mucosal breaks continuous between >2 mucosal folds, but involving less than 75% of the esophageal circumference; and grade D, mucosal breaks involving more than 75% of the esophageal circumference.
For potential predictors of postoperative complications, 23,24 C-reactive protein (CRP) levels and the white blood cell (WBC) count were determined at postoperative days (PODs) 1, 3, and 7 to evaluate acute inflammatory responses after RAPG or LAPG. Additionally, postoperative nutritional status was assessed by hemoglobin levels, albumin levels, total lymphocyte count, 25 ] and BMI at 6, 12, and 24 months.
Long-Term Outcome
Patients were followed up postoperatively and the long-term outcomes, including overall survival (OS) and disease-free survival (DFS), were obtained. The last follow-up was on January 2017. Overall survival was defined as the period from the date of completion of the operation to the date of death or the date of the last follow-up. Disease-free survival was defined as the period from the date of completion of the operation to the date of recurrence or death, whichever occurred first.
Statistical Analysis
To compare oncological safety, surgical response, and nutritional safety between RAPG and LAPG, the unpaired t test and χ2 test were used for continuous variables and categorical variables, respectively. Data for continuous variable were presented as mean (standard deviation). Kaplan-Meier survival curves were plotted for both OS and DFS, and comparison between curves was analyzed using the log-rank test. Statistical analyses were performed by SPSS version 22.0 for Windows (IBM Inc). A 2-sided P value <.05 was considered statistically significant.
Results
Baseline Characteristics of Included Patients
As shown in Table 1, 27 patients with EGC in the upper location underwent RAPG and 62 patients underwent LAPG. The mean age of patients in the RAPG group was 59.7 ± 11.6 years and that in the LAPG group was 56.6 ± 12.2 years (P = .262). There were no differences in sex, BMI, physical status, comorbidity, rate of a previous abdominal operation, and tumor size between the 2 groups (Ps > .05). At preoperative evaluation, 63% of patients in the RAPG group and 59.7% of patients in the LAPG group were diagnosed with clinical T1a tumors. The remaining 37% and 40.3% of patients were diagnosed with clinical T1b tumors in the RAPG and LAPG groups, respectively. Pathologically, there were 21 patients with stage Ia, 3 with stage Ib, 2 with stage IIa, and 1 with stage IIb in the RAPG group. There were 44 patients with stage Ia, 17 with stage Ib, and 1 with stage IIa in the LAPG group. There was no significant difference in pathological stage between the groups (P = .089).
Baseline Characteristics of Patients Who Underwent RAPG and LAPG.

Abbreviations: RAPG, robot-assisted proximal gastrectomy; LAPG, laparoscopy-assisted proximal gastrectomy; BMI, body mass index; ASA-PS, American Society of Anesthesiologists physical status; pTNM, pathological tumor node metastasis.
Perioperative Outcomes and Surgical Response
All included patients had R0 resection and D1+ lymph node dissection (Table 2). The operation time was calculated from the beginning of the incision to the closure of the incision. The LAPG group had a similar operation time to the RAPG group (218.3 ± 54.5 vs 224.8 ± 43.6 minutes, P = .585). Despite significantly less intraoperative estimated blood loss (227.8 ± 47.9 vs 203.2 ± 43.2 mL, P = .024), the blood transfusion rate was comparable between the groups (P = .272). With regard to lymphadenectomy, the RAPG group had significantly more lymph nodes retrieved than the LAPG group (30.3 ± 6.2 vs 26.9 ± 6.3, P = .021). The mean proximal resection margin was 3.3 ± 1.7 cm for the RAPG group and 3.8 ± 2.4 cm for the LAPG group (P = .330), and the mean distal resection margin was 4.0 ± 1.4 cm for the RAPG group and 4.3 ± 2.7 cm for the LAPG group (P = .587). The mean postoperative hospital stay was 10.8 ± 4.2 days and 11.1 ± 7.8 days in the RAPG and LAPG groups, respectively (P = .851). Patients in the RAPG group had significantly higher medical costs than did those in the LAPG group (122 247 ± 17 473 vs 91 812 ± 19 454 ¥, P < .001).
Short-Term Outcomes of Patients Who Underwent RAPG and LAPG.
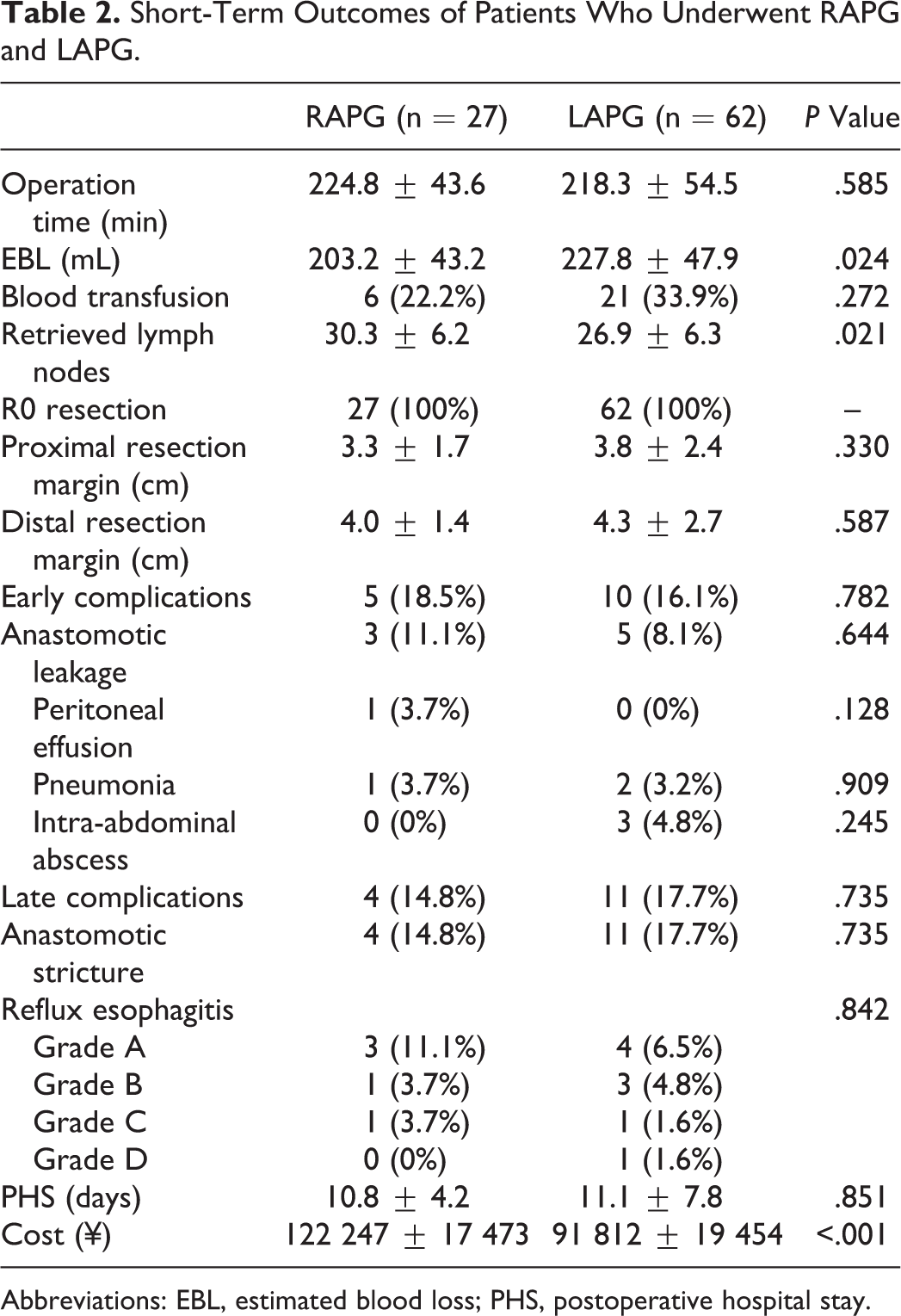
Abbreviations: EBL, estimated blood loss; PHS, postoperative hospital stay.
Pre- and postoperative CRP levels and WBC count at PODs 1, 3, and 7 are shown in Figure 1. There were no significant differences in postoperative CRP concentrations and the WBC count between the groups (Ps > .05).

CRP levels and the WBC count preoperatively and at PODs 1, 3, and 7 following gastrectomy among patients who received RAPG and LAPG. CRP indicates C-reactive protein; WBC, white blood cell; PODs, postoperative days; RAPG, robot-assisted proximal gastrectomy; LAPG, laparoscopy-assisted proximal gastrectomy.
Five (18.5%) patients in the RAPG group suffered from early complications, including three (11.1%) who had anastomotic leakage, one (3.7%) with pneumonia, and one (3.7%) with peritoneal effusion. Ten (16.1%) patients in the LAPG group had early complications, including five (8.1%) with anastomotic leakage, two (3.2%) with pneumonia, and three (4.8%) with intra-abdominal abscess. There were no significant differences in the rates of these complications between the 2 groups. The late complication rates were 14.8% and 17.7% for the RAPG and LAPG groups, respectively (P = .735). All of the late complications were anastomotic stricture, which was treated by endoscopy. No postoperative mortality was observed.
Reflux Esophagitis and Nutritional Status
Five (18.5%) patients in the RAPG group and nine (14.5%) in the LAPG group had reflux esophagitis (P = .842; Table 2). Los Angeles grade B (Figure 2) or higher (severe) reflux esophagitis was observed in 2 (7.4%) patients in the RAPG group and 5 (8.0%) patients in the LAPG group.

The typical photographs of reflux esophagitis.
Chronological changes in hemoglobin levels, albumin levels, total lymphocytes, and BMI, which reflect the nutritional status, are shown in Figure 3. Hemoglobin levels at 6 months and BMI at 12 months postoperatively appeared to be slightly higher in the RAPG group compared with baseline values. However, there were no significant between-group differences regarding these variables (Ps > .05).

Chronological changes in hemoglobin levels, albumin levels, total lymphocyte count, and BMI between the RAPG and LAPG groups. All postoperative data are expressed as values relative to preoperative data. M indicates month after surgery; BMI indicates body mass index; RAPG, robot-assisted proximal gastrectomy; LAPG, laparoscopy-assisted proximal gastrectomy.
OS and DFS
The median follow-up time was 52 months (18-61 months). By the last follow-up, 13 patients in the LAPG group and 7 in the RAPG group had recurrence of tumors in the residual stomach, peritoneum, or liver. Among these patients, 6 in the LAPG group and 5 in the RAPG group died of tumor recurrence. Kaplan-Meier analyses of OS and DFS are shown in Figure 4. The 5-year survival rates were 74.1% and 85.5% in the RAPG and LAPG groups, respectively. The OS (P = .12) and DFS (P = .47) were similar between the 2 groups.

Comparison of disease-free survival (A) and overall survival (B) between the 2 groups.
Discussion
Proximal gastrectomy is an acceptable procedure for patients with EGC in the upper location. 19 Preservation of the gastric reservoir maintains secretion of gastric acid and intrinsic factors, which can improve patients’ quality of life postoperatively. In the era of minimally invasive surgery, RAPG or LAPG is theoretically a superior choice over other procedures, such as LATG, open total gastrectomy, and open proximal gastrectomy, for treating proximal EGC, advantages of minimal invasiveness, and preservation of function. The feasibility and safety of RAPG compared with LAPG has not been previously reported. To the best of our knowledge, this is the first study to show that RAPG could be an alternative to LAPG with comparable oncological safety and nutritional status.
Our study showed that there were no differences in perioperative outcomes between the RAPG and LAPG groups, except for intraoperative blood loss, retrieved lymph nodes, and medical costs. Despite significantly less blood loss in the RAPG group than in the LAPG group, the blood transfusion rate was comparable between the 2 groups. This finding suggests that blood loss in both procedures has the same degree of severity. Greater lymph node retrieval was observed in the RAPG group compared with the LAPG group. A greater amount of retrieved lymph nodes facilitates accurate staging and prognostic assessment and also leads to a potentially superior prognosis. 26,27 The articulating instrument used in the RAPG group may have been responsible for more retrieved lymph nodes because it enables the surgeon to reach deep areas that would be otherwise unreachable with laparoscopic straight forceps. 28 Specially, articulating instruments facilitate delicate manipulation without injuring blood vessels in suprapancreatic lymph node dissection, which is technically demanding in LAPG. A previous study also reported the merits of robotic gastrectomy regarding reduction in blood loss and lymph node dissection. 20 With regard to the total financial expenditure, the RAPG group had a significantly higher medical cost than that in the LAPG group because the government does not currently reimburse robotic procedures. However, this cost difference should not be problematic in the future. This is because much of the robot-related premium cost is related to depreciation and maintenance costs, which are currently expensive. 29 Use of original domestically produced Chinese surgical robotic systems may lower this cost. 30
Surgery-related stress responses disturb homoeostasis, which increases the risks of postoperative complications. 31 Surgical stress is considered to be proportional to the extent of operative trauma. Kosuga and colleagues showed that CRP levels at PODs 3 and 7 were significantly lower with LAPG than with laparoscopic-assisted total gastrectomy. 11 Therefore, to compare the surgical response after RAPG and LARG, we measured CRP levels and the WBC count postoperatively. These variables are inflammatory mediators, as well as potential predictors of complications. 23,24 However, we found no differences in CRP levels and the WBC count between the 2 groups, which indicated that there was comparable surgical invasiveness. These findings are also consistent with postoperative performance in that there was a similar incidence of complications between the groups. The early complication rates were 18.5% and 16.1% for the RAPG and LAPG groups, respectively. Recent studies have reported that complications after LAPG range from 8.0% to 33.0%, 11,32 which are consistent with our study.
Our study showed that the late complication rate was similar between RAPG and LAPG groups. Anastomosis-related late complications, including reflux esophagitis and anastomotic stricture, are the main concerns after proximal gastrectomy. Various reconstruction techniques have been attempted to prevent anastomosis-related complications. 33 However, a consensus on optimal reconstruction has not been reached. In our study, we adopted the end-to-side EG reconstruction method using a circular stapler because of its simplicity and for saving time. A previous study reported that the incidence of anastomotic stricture was 16.0% after LAPG with EG reconstruction, 11 which is consistent with our findings (RAPG: 14.8% vs LAPG: 17.7%). Jejunal interposition improves reflux esophagitis compared with EG. 34 However, jejunal interposition has not yet gained wide acceptance because of its technical complexity and its requirement for a large number of anastomoses, which involve a longer operation time. Kinoshita et al reported that the median operation time for LAPG with jejunal interposition reconstruction was 233 minutes, which was longer than that for open surgery. 35 A recent study reported a novel technique of intracorporeal double-tract reconstruction after LAPG using linear staplers with clinically satisfactory results. 36 To facilitate decision making in the clinical setting, a randomized clinical trial, KLASS-05 (NCT01433861), which aims to compare LAPG with double-tract reconstruction to LATG, is currently underway. However, all of these abovementioned studies investigated these various reconstruction methods only in laparoscopic surgery. These reconstruction techniques need to be attempted with a robotic system.
Recently, some retrospective studies have reported that patients receiving double-flap reconstruction may suffer less risk of anastomotic leakage and reflux esophagitis. 37 For double-flap reconstruction, the distal esophagus and anastomotic site were implanted in the submucosal layer and covered by the seromuscular double flap created on the gastric remnant in an H-shape (double-flap technique). This procedure needs double-flap creation at the anterior of the gastric remnant and hand-sewn suturing of anastomosis, which is technically demanding and time-consuming intracorporeally. Prospective randomized studies are needed to validate the better quality-of-life benefit after double-flap reconstruction compared with other reconstructive methods.
Studies that compared nutritional status following LAPG and LATG have shown inconsistent results, 11,38 which might be attributed to different reconstruction methods following gastrectomy. In our study, a similar postoperative nutritional status was observed between the RAPG and LAPG groups. This finding suggests that there is comparable food intake and digestive and absorptive functions between RAPG and LAPG. Additionally, survival analysis showed that, after RAPG, patients could achieve similar long-term outcomes to patients undergoing LAPG. Six patients in the LAPG group and five in the RAPG group died of tumor recurrence. Three of these patients who were diagnosed with preoperative cT1N0 tumors had locally advanced tumors with positive lymph nodes pathologically. Therefore, proximal gastrectomy might be insufficient for these patients. To overcome this problem, preoperative diagnostic accuracy should be emphasized. Sentinel node navigation surgery may also be helpful. 39 In this situation, robotic systems could function as a surgical information hub to integrate imaging devices for improved surgery.
The present study has several limitations. First, this was a retrospective study with a small sample size. Because of inevitable bias, the data should be interpreted with caution. Second, we did not assess the quality of life of the patients using a validated questionnaire. Third, initial cases in the learning curve were included. However, to the best of our knowledge, this is the first study to compare RAPG and LAPG among patients with EGC in the upper location. These preliminary findings suggest that prospective, randomized trials are required to establish a higher level of evidence for the use of RAPG in upper EGC.
In conclusion, RAPG is an alternative to LAPG with comparable oncological safety and nutritional status. A well-designed, large-scale, prospective, randomized controlled study is needed to validate our findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded partly by the National Nature Science Foundation of China (nos. 81672319 and 81602507), the National Key Research and Development Plan (no. 2016YFC0905302), the Beijing Municipal Science and Technology Plan projects (no. Z161100000516237), and the Special Project for Military Healthcare (no. 16BJZ10).