
Abstract
Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (IHC) are primary liver cancers where all or most of the tumor burden is usually confined to the liver. Therefore, locoregional liver-directed therapies can provide an opportunity to control intrahepatic disease with minimal systemic side effects. The English medical literature and clinical trials were reviewed to provide a synopsis on the available liver-directed percutaneous therapies for HCC and IHC. Locoregional liver-directed therapies provide survival benefit for patients with HCC and IHC compared to best medical treatment and have lower comorbid risks compared to surgical resection. These treatment options should be considered, especially in patients with unresectable disease.
Keywords
Introduction
Minimally invasive liver-directed therapies have been a topic of increasing interest due to the severe prognostic implications of a malignant liver tumor and the lower comorbid risk of these procedures compared to surgical resection. 1,2 Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (IHC) are primary liver cancers where all or most of the tumor burden is usually confined to the liver. 3,4 Therefore, locoregional liver-directed therapies can provide an opportunity to control intrahepatic disease progression and improve survival in patients who are not surgical candidates. Locoregional liver-directed therapies include percutaneous ablations and transarterial catheter-directed therapies. Transarterial therapies have 4 major types: intrahepatic chemoinfusion, transarterial embolization with microspheres, transarterial chemoembolization (TACE) with chemotherapy-loaded drug-eluting beads (DEBs) or lipiodol, and transarterial radioembolization (TARE) with Yttrium 90 (Y90)-labeled microspheres. The aim of this article is to highlight the results of the most relevant literature regarding liver-directed therapies of HCC and IHC. Transarterial chemoinfusion is not commonly used, and this treatment modality is not discussed in this article.
Evolution of Transarterial Embolization Treatments for HCC
In the mid-20th century, treatment options for HCC were severely limited. There was no cross-sectional imaging, hepatitis C had not yet been identified—patients with hepatitis without serologic evidence of hepatitis A or B virus infection were said to have “non-A/non-B” hepatitis—and even the sequelae of chronic active hepatitis B remained undefined. Surgical techniques were rudimentary, and there was no effective chemotherapy. In 1952, Markowitz 5 determined that ligation of the hepatic artery in humans was probably safe and in 1954 Breedis and Young, 6 in a series of very elegant investigations, demonstrated that the dominant blood supply to both primary and metastatic liver tumors was derived from the hepatic artery while the portal venous system provided trophic blood supply to the normal liver parenchyma. In 1972, based on the work of Breedis and Young, a surgeon from Malaysia reported on “complete de-arterialization” as treatment for 24 patients with HCC. 7 Although follow-up biopsy demonstrated extensive necrosis in large tumors, more than half of the patients died within 6 months. McDermott et al 8 reported on a similar procedure in 1979 and, despite beneficial results in 3 of the 5 patients, extensive collaterals developed postoperatively that resupplied the tumors. By 1981, using a “catheter as a scalpel” had been proposed by Charles Dotter, 9 and Chuang and Wallace 10 described encouraging results embolizing a variety of liver tumors with gelfoam and coils. They commented on the need for smaller and more permanent embolic agents to cause a more “peripheral” and “sustained” occlusion, focused on the importance of enhancing ischemia. There were no such agents at that time and instead people began to “add” thing to the embolic mix in an effort to improve results. In 1983, the same group reported on the use of both a 5-day hepatic artery triple drug chemotherapy hepatic artery infusion (HAI) regimen and hepatic artery embolization (HAE) with either gelfoam or Ivalon in 24 patients with HCC. 11 The HAI method involved 5 days in hospital with a catheter in the hepatic artery. Catheter position was checked daily and the patients received doxorubicin, mitomycin, and floxuridine, with doxorubicin and mitomycin administered once and the floxuridine given daily. Each patient received 2 courses of treatment. The embolized patients were treated 4 weeks apart, particularly those who had bilobar disease. The median overall survival (OS) was 12.3 months for the HAI regimen and 17.4 months for the embolized patients.
In 1985, Nakakuma et al 12 proved that lipiodol was retained by liver tumors both in the VX-2 rabbit model and in man and was associated with extensive tumor necrosis. Rather than thinking of lipiodol as an agent that could penetrate those distal small tumor vessels providing a “more peripheral embolization” enhancing ischemia, lipiodol was embraced as a potential “carrier” of chemotherapeutic agents and the era of “conventional trans-arterial chemoembolization (cTACE)” was born. In 1989, Nakamura reported on 100 patients treated with this new method that he called “oily chemoembolization” using doxorubicin, lipiodol, and gelfoam and comparing them to a historical control group treated with doxorubicin and gelfoam before 1983. 13 He described improved survival in the “oily chemoembolization” group, ignoring the potential confounding factors inherent in the use of historical control groups, most notably lead time bias. Despite the only difference being whether or not lipiodol was used, the authors attributed the improved therapeutic effect to retention of doxorubicin, although enhanced ischemia resulting from the use of lipiodol seems an equally plausible explanation; cTACE was now “in style.”
Many papers subsequently appeared describing results of multiple homegrown methods of hepatic chemoembolization, none documenting a survival advantage as a result of the treatment. That changed in 2002 when 2 landmark papers appeared describing the results of randomized trials in Asia and Europe and providing level 1 evidence of a survival advantage for patients treated with chemoembolization. The Barcelona group randomized patients to 3 arms: chemoembolization with doxorubicin, lipiodol and gelfoam, embolization with gelfoam alone, and best supportive care. 14 This trial continues to be misinterpreted as showing a survival benefit for chemoembolization compared to both embolization alone and best supportive care. In fact, the triangular sequential design of the trial allowed it to be stopped any time a significant difference was detected between either of the treatment groups and best supportive care. This occurred on the 9th sequential analysis when a survival benefit was demonstrated in the chemoembolization group and the trial was stopped. At that time, comparing embolization with best supportive care, the authors reported that the “plot line remained within the boundaries indicating the need to recruit additional patients to achieve a valid conclusion.” When the trial was stopped, survival was similar in both the chemoembolization and embolization groups, with 1- and 2-year survival of 82% and 63% and 75% and 50%, respectively. This finding is all the more notable since gelfoam is not the ideal agent for HAE alone, where a more permanent and smaller agent is typically used to maximize ischemia. Interestingly, more radiographic responses in the embolization group were also noted.
The issue of the role of the chemotherapeutic agent in chemoembolization remained unresolved. In 2005, the first drug-eluting embolic became available in Europe (DC Bead, Biocompatibles UK, Farnham, Surrey, United Kingdom) and in 2008 in the United States (LC Bead, Biocompatibles UK, Farnham, Surrey, United Kingdom). Contemporary TACE has since crystallized into 2 principal incarnations, dubbed conventional TACE (cTACE) and TACE with drug-eluting beads (DEBs-TACE), following several pivotal clinical trials 14 -22 and the development of drug-eluting microspheres and microcatheter technologies.
Investigations into the use of Y90-labeled microspheres dates back to the early 1960s when they were tested in canine prostate. 23 In 1965, the initial results on the role of Y90 microspheres for the treatment of inoperable primary pancreatic and liver cancer were reported. 24 It was not until the late 1980s when the safety and feasibility of intra-arterial Y90 radiation therapy for hepatic malignancies was tested in a canine liver model. 25,26 In 1989, Houle et al 27 reported the results of a pilot study on 7 patients with HCC treated with Y90 glass microsphere embolization. In 1992, Shepherd et al 28 conducted a seminal phase I dose-escalation study of Y90 glass microspheres in 10 patients with primary HCC. This study provided the safety data that paved the road for outcome studies using Y90-labeled particles for TARE of HCC.
In December 1999, the US Food and Drug Administration (FDA) approved Y90 glass microspheres (TheraSphere, MDS Nordion, Canada acquired by BTG, UK in 2013) under humanitarian device exemption (HDE), for radiation treatment or as a neo-adjuvant to surgery or transplantation in patients with unresectable HCC. 29 This approval was expanded in 2007 to patients who also have partial or branch portal vein thrombosis (PVT) 30 because the antitumoral effect of radioembolization relies predominantly on the radiation effect, with a minor contribution from microembolization. 31
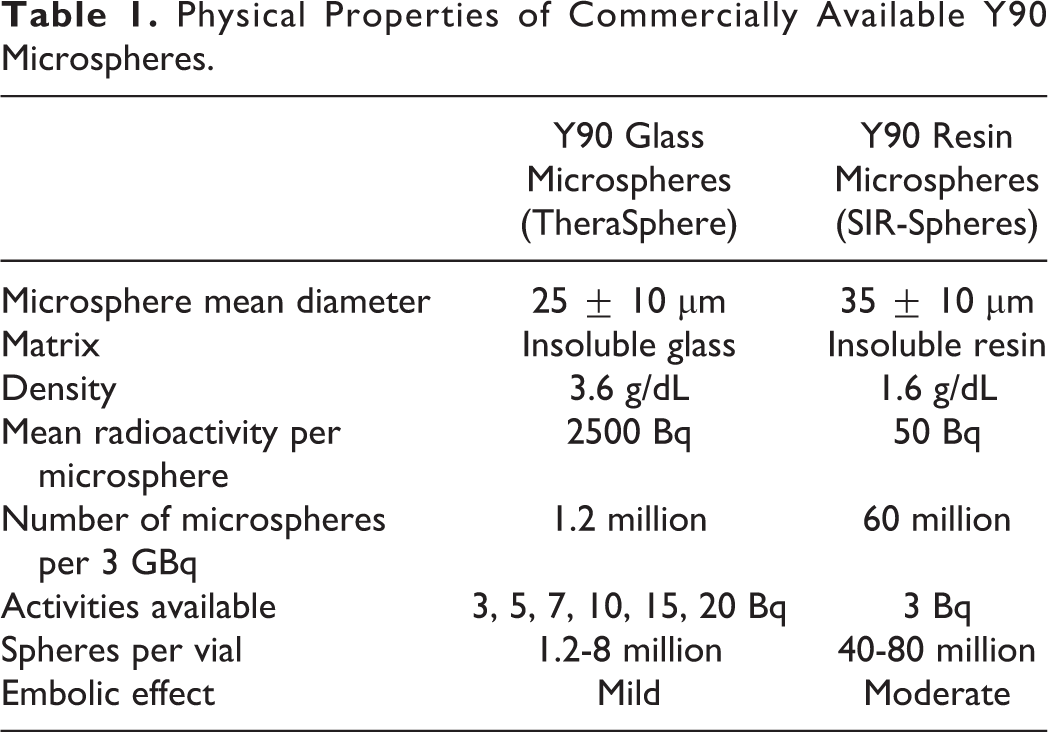
Currently, there are 2 commercially available Y90 microsphere devices for TARE: Y90 glass microspheres where Y90 is an integral part of the glass and Y90 resin microspheres where Y90 is attached to the resin. The FDA approved the use of Y90 resin microspheres (SIR-Spheres, Sirtex, Australia) in 2002 via a premarket approval for the treatment of unresectable metastatic liver tumors from primary colorectal cancer with adjuvant intrahepatic transarterial chemotherapy of 5-fluorodeoxyuridine (Floxuridine). 32 The characteristics of the 2 clinically approved Y90 microspheres are presented in Table 1.
Physical Properties of Commercially Available Y90 Microspheres.
Transarterial Bland Embolization Treatment for HCC
The development of DEB technology provided the ideal platform for a randomized controlled trial designed to treat patients with HCC. Such a trial could be constructed so that the only variable was whether or not the bead was loaded with doxorubicin. In 2009, Malagari et al 33 reported results of a randomized multicenter trial (level 1) comparing patients treated with a doxorubicin-loaded DEB-TACE compared to the unloaded bead. Patients were treated with either 100 to 300 or 300 to 500 micron embolics and in some cases the beads were mixed. They described a significant improvement in overall response at 9 months only and improved time to progression (TTP) in the DEB group (42.4 weeks compared to 36.2 weeks), but no difference in OS, suggesting that the results, not reported on intent to treat basis, favored the use of DEBs.
In 2016, Brown et al 34 reported the intent to treat results of a single center randomized controlled trial (level 1 evidence). This randomized controlled trial compared the outcome of embolization using microspheres alone with chemoembolization using doxorubicin-eluting microspheres. Brown et al 34 found no difference in response at any time point, toxicity, progression-free survival, or OS. When analyzed separately, there was also no difference in any of these measures in the treated patients.
This evidence supports the supposition of Chuang and Wallace 10 in 1981 that ischemia is the prime effector of response following HAE. Smaller particles that can more efficiently and effectively cause tumor ischemia should be used for the best results making the addition of a chemotherapeutic agent unnecessary. There also appears to be a lower incidence of vessel occlusion following embolization when chemotherapeutic is not used. 35 Given the comparable safety profile, progression rate, and survival, bland embolization should continue to be considered a reasonable therapeutic option and an alternative to embolization with doxorubicin-loaded microspheres. Cost, ease of use, and toxicity profile including systemic effects, hepatic toxicity, and subsequent vessel occlusion should be considered when choosing.
TACE Treatment for HCC
Since the early 2000s, TACE has become the standard of care therapy for patients with intermediate-stage HCC, with a proven survival benefit. 14,17,19,20 Nearly half of all HCC patients undergo TACE during the course of the disease. 36,37 In the following sections, we describe the biological rationale and technical considerations of TACE, followed by a review of the current clinical data supporting the use of TACE in all stages of HCC.
Rationale and Technical Considerations for TACE
All intra-arterial therapies for HCC are predicated upon the fact that the liver benefits from a dual blood supply. The HCC is primarily nourished by branches of the hepatic artery. 6,38 Thus, by occluding the feeding artery or arteries, complete tumor ischemia can potentially be achieved. In TACE, coincident with the delivery of embolic material is the administration of a chemotherapeutic agent. Direct intra-arterial delivery increases drug concentration within the target area; moreover, for chemotherapies with a high “first pass” effect, the systemic toxicities are diminished. 39
Beyond the independent antitumoral effects of chemotherapy and embolization, there are several theoretical advantages to their simultaneous delivery. By reducing/obliterating intratumoral blood flow, embolization prolongs the dwell time of chemotherapy within the tumor, facilitating its target localization and further minimizing the systemic dose. Preclinical data also suggest that embolization, by decreasing interstitial fluid pressure, improves intratumoral penetration of chemotherapeutic agents. 40
Modern TACE can be segregated into 2 technical approaches: cTACE and DEB-TACE. cTACE bears the closest resemblance to the techniques used in the landmark clinical trials described subsequently that demonstrated a survival benefit with TACE 14,17,19,20 and remains the most popular method for TACE globally. In cTACE, a water-soluble chemotherapeutic (typically doxorubicin) is emulsified in ethiodized oil (Lipiodol, Guerbet, Paris, France) and injected intra-arterially followed by particle embolization (examples include gelatin sponge, polyvinyl alcohol particles, or calibrated microspheres). Some providers add the embolization particles to the chemotherapeutic–lipiodol emulsion and inject them together. The adjuvant particle embolization decreases forward flow and prevents the washout of the chemotherapeutic–lipiodol emulsion from the embolized territory. Lipiodol serves multiple purposes in the cocktail: (1) as an iodinated compound, it can be easily visualized under fluoroscopy, (2) as an oil, it emulsifies the chemotherapeutic and serves as a vehicle for drug delivery, and (3) as a viscous fluid, it can function as a microembolic agent itself.
The DEB-TACE was developed more recently with the advent of drug-eluting microspheres. The concept for DEB-TACE is founded upon the principle that sustained release of a drug over a protracted length of time is more effective than bolus doses; this “reservoir effect” permits deeper diffusion of the drug beyond the perivascular space and into the tumor. 41,42 Moreover, by coupling chemotherapeutics with calibrated microspheres of reproducible size, the execution of TACE can be standardized to facilitate interpretation of outcomes across patients and institutions with less concern for biases based upon technical variability.
Several trials have investigated the efficacy of cTACE versus DEB-TACE. PRECISION V 43 was a phase II study that showed nonsignificantly higher complete response rates in the DEB-TACE arm; subset analyses, however, showed a significant improvement in response rates with DEB-TACE in patients with Child-Pugh score B and in patients with bilobar disease. Additionally, systemic toxicities of doxorubicin, including cardiovascular dysfunction and alopecia, as well as liver toxicity, were lower in the DEB-TACE arm. 44 Sacco et al 45 performed a prospective trial of 60 patients randomized to either DEB-TACE or cTACE; this study did not find a significant difference in TTP or OS between the 2 techniques. A meta-analysis of the extant prospective and retrospective data suggests that the pooled odds ratio for survival at 2 years favors DEB-TACE, with similar rates of adverse events for the 2 groups. 46 Nonetheless, given the challenges of stratifying against every intraprocedural technical variable in a clinical trial setting, neither technique has conclusively demonstrated superiority over the other, and the selection of TACE methodology is best left to the discretion of the interventionalist.
TACE for Intermediate-Stage HCC
The Barcelona Clinic Liver Cancer (BCLC) staging defines intermediate-stage HCC (BCLC B) as the subset of patients who are not candidates for curative surgical therapies (thermal ablation, surgical resection, and transplantation) but whose liver function and performance status are preserved. Certainly, these criteria circumscribe a highly heterogeneous group of patients, and this heterogeneity is an often-levied criticism of the BCLC classification system. Nonetheless, as the BCLC system is the only algorithm that stratifies patients based upon outcome and provides treatment options based upon disease classification, it remains the most commonly used staging system. For patients with BCLC B, TACE is regarded the standard of care therapy. Although multiple therapeutic interventions have been evaluated for BCLC B patients, TACE is the only therapy to have consistently demonstrated a survival benefit. 47 As a result, TACE has been endorsed by numerous clinical guidelines for patients with intermediate-stage HCC. 48 -54
While experimentation with TACE for HCC began in the 1970s, it was not until 2002 that a firm, evidence-based foundation for this procedure was established. In that year, 2 landmark randomized, controlled trials 14,20 were published, both demonstrating a survival benefit for patients undergoing TACE versus best supportive care. It is important to note that while TACE is the standard of care for patients with intermediate-stage HCC, proper patient selection for TACE remains essential. Given the heterogeneity in tumor burden, liver function, and clinical status, not all patients who fit the broad inclusion criteria of BCLC B will benefit from this procedure. Ideal candidates for TACE have preserved liver function (typically Child-Pugh B7 or better), have solitary or paucifocal tumors without vascular invasion, and have preserved functional status. With such strict selection criteria, median survival rates as high as 47.7 months for patients with intermediate-stage HCC undergoing TACE have been reported. 55 Realistically, however, a recent meta-analysis that included studies with less restrictive inclusion criteria established the OS rate following TACE to be approximately 19.4 months. 36
TACE for Early-Stage HCC
Early-stage HCC patients, as defined by the BCLC A classification, are patients with solitary or paucifocal tumors and preserved liver function who are candidates for potentially curative interventions including thermal ablation, surgical resection, and transplantation. Strictly considering the guidelines, TACE is not a recommended therapy for patients in this category. However, in modern practice, TACE is commonly performed in early-stage HCC patients; typically, these are patients whose tumors are not amenable to ablation/surgical resection and are not transplant candidates due to comorbidities or patients on the transplantation waiting list who require bridging therapy to maintain transplant candidacy.
Patients with centrally located tumors or tumors larger than 3 cm may not be suitable candidates for ablation due to the potential for injury to central bile ducts or ablation zone size limitations of current technology, respectively. For these patients, TACE represents an effective treatment option. The relative efficacy of TACE, thermal ablation, and surgical resection for solitary HCC lesions measuring 3 cm or smaller was recently compared in a retrospective study. 56 After accounting for the contribution of underlying liver disease, the 5-year survival rate for patients undergoing TACE (81%) was not significantly different from those patients who underwent surgical resection or thermal ablation. Given recent technological advances allowing for the superselective catheterization of subsegmental arteries supplying tumoral lesions during TACE, it is not impractical to consider TACE as a locally curative therapy in selected patients.
Liver transplantation is considered the only truly curative therapy for patients with HCC. However, scarcity of organ availability has led to prolonged transplantation waitlist times. To maintain transplant candidacy, most patients undergo some form of locoregional therapy, typically thermal ablation or TACE, to locally eradicate tumors and prevent tumoral growth above transplantation criteria thresholds. Some centers prefer TACE over thermal ablation for transplant candidates, given the small risk of tumoral tract seeding associated with percutaneous interventions. Additionally, tumoral response to TACE has been proposed as a biomarker for tumor biology: tumors that do not demonstrate a complete response to the initial TACE procedure may be more biologically aggressive, an association that may affect the risk of recurrence following transplantation. 57,58
TACE for Advanced-Stage HCC
The only standard of care therapy for patients with advanced-stage HCC, characterized by diminished performance status, tumoral invasion of hepatic vasculature, or extrahepatic metastases, is the multi-kinase inhibitor sorafenib. 59 However, given the modest survival benefit afforded by sorafenib in this patient population, 59 multiple efforts to combine sorafenib with locoregional therapies such as TACE have been pursued. This combination in appropriately selected patients has been shown to be safe 60,61 in single-arm studies. Likewise, in a large, global registry, the combination of TACE and sorafenib was well tolerated. 60 Moreover, the combination may be potentially complimentary. Tumoral resistance to TACE therapy is in part driven by tumor neoangiogenic factors, including vascular endothelial growth factor (VEGF), which has been shown to increase following TACE. As one of sorafenib’s targets is the VEGF pathway, the combination of TACE and sorafenib may lead to improved outcomes. In a recent randomized trial of patients with intermediate-stage HCC, the combination of TACE with sorafenib was not found to improve TTP compared to TACE alone (SPACE trial). 36 On the other hand, in a global registry analysis, the concomitant administration of sorafenib and TACE resulted in the best OS rate. Additionally, several retrospective studies have suggested a potential benefit for the combination approach in patients with advanced-stage HCC. 29,62,63
TARE Treatment for HCC
Current clinical indications for Y90 radioembolization in patients with HCC include patients with advanced HCC (BCLC C) due to partial or branch PVT, patients with intermediate HCC (BCLC B) who are poor candidates for TACE due to large tumor size, multifocal disease and advanced age, patients who didn’t respond to prior TACE, and patients who are not eligible for potentially curative treatments such as thermal ablation, transplant, or surgery, but could become eligible as a result of a reduction in tumor burden or downstaging of disease. 64 -69
Rationale and Technical Considerations for Y90 Radioembolization
Y90 is a pure β-emitting isotope with a physical half-life of 64.2 hours. 70 The average β-emission is 0.9367 MeV, with a mean tissue penetration of 2.5 mm and maximum tissue penetration of 11 mm, 71,72 allowing delivery of high radiation doses to hepatic tumors with a “cross-fire” mechanism between the Y90 microspheres, while limiting the radiation dose to the surrounding liver parenchyma. 73 The antitumoral effect of Y90 is thought to be secondary to irreversible damage to tumor epithelial, stromal, and endothelial cells. 74 The absorbed dose of Y90 microspheres in the liver may be heterogeneous as it depends on hemodynamics and intratumoral vessel density. 75 The injected microspheres implant mostly in the terminal arterioles of tumors 73 in a 3:1 to 20:1 ratio compared to normal liver, with a preferential deposition in the tumor periphery. 76 Our main focus in this review is Y90 glass microspheres (TheraSphere), which is currently the only radioembolization device that is FDA approved for the treatment of HCC under HDE.
Patients are not considered good candidates for radioembolization with decreased performance status (ECOG ≥ 2), Child-Pugh class C (score ≥ 10), elevated baseline bilirubin level (>2 mg/dL), elevated alanine aminotransferase or alanine aminotransferase level (>5× upper limit of normal), tumor burden >70% of the target liver volume, or tumor nodules too numerous to count and tumor volume >50% liver volume combined with an albumin <3 g/dL. If the patient is determined to be a candidate for radioembolization, a treatment planning angiogram is performed 1 to 2 weeks before the radioembolization treatment according to published guidelines. 72 During the planning angiography, the tumor feeding vessels and anatomic variants are identified and technetium-99 labeled macroaggregated albumin (99mTC-MAA) is injected into the hepatic arteries to determine the magnitude of hepatopulmonary shunting with scintigraphy immediately after the planning angiogram. 77 Embolization of extrahepatic visceral collaterals (ie, gastroduodenal artery, right gastric artery) may be necessary to prevent nontarget radioembolization of bowel loops or the stomach. 72,78,79 The diameter of 99mTC-MAA particles is in the range of 30 to 90 μm, which is similar in size to Y90 microspheres. Significant hepatopulmonary shunting with an estimated radiation dose to the lungs over 30 Gy in a single treatment or over 50 Gy in multiple treatments and inability to prevent deposition of Y90 microspheres in the gastrointestinal tract are absolute contraindications for the use of Y90 radioembolization.
Treatment Outcomes of Radioembolization
The current evidence that supports the use of radioembolization to treat HCC is based on retrospective series or noncontrolled prospective studies. The most comprehensive study by Salem et al reported the long-term outcomes of 291 patients with intermediate- and advanced-stage HCC who underwent radioembolization. 65 The median OS was 17.2 months for Child-Pugh A patients and 7.7 months for Child-Pugh B patients. Child-Pugh B patients with PVT had a median OS of 5.6 months. The overall TTP was 7.9 months. 65 A prospective phase 2 study including 52 patients with intermediate (17 patients) and advanced stage (35 patients) HCC who were treated with radioembolization reported 15 months median OS. 64 Sangro et al 80 reported 12.8 months OS in a study including 325 patients. The OS varied significantly by disease stage, as it was 24.4 months for BCLC A, 16.9 months for BCLC B, and 10.0 months for patients with BCLC C. Consistent with these findings, survival varied significantly by ECOG status, hepatic function, tumor burden, and presence of extrahepatic disease.
No randomized controlled trials have been published until very recently comparing TARE with other locoregional or systemic therapies to confirm efficacy and potential survival benefits. Salem et al 81 reported the first prospective randomized controlled trial comparing TARE to cTACE which is the standard of care for intermediate HCC. 19 Patients in the Y90 radioembolization group had significantly longer median TTP (>26 months) than patients in the cTACE group (6.8 months). However, the median OS was not significantly different; it was 17.7 months for the cTACE group and 18.6 months for TARE group. They concluded that Y90 radioembolization provides better tumor control and could reduce dropout from transplant waitlists. 81 Recent meta-analysis of 8 studies including a total of 1499 patients reported significantly better in OS, TTP, and hospitalization time for TARE compared to TACE. 82 In 2013, a study by Salem et al 83 demonstrated that TARE outperformed TACE by validated quality-of-life measures. The prospective study of 56 patients with HCC who underwent TARE (29 patients) versus TACE (27 patients) showed that although patients who received TARE had a larger tumor burden, they had higher quality-of-life scores in comparison to patients who received TACE. 83 Lance et al 84 reported that postembolization syndrome was significantly more severe in patients who underwent TACE resulting in increased total hospitalization rates. In another study, 85 patients who received TARE reported more fatigue, but they had less fever and required less hospitalization than patients treated with TACE. Based on these studies, TARE is better tolerated than TACE with shorter length of hospital stay and milder postembolization symptoms.
Sorafenib is the standard of care for patients with advanced HCC. 59 No results from randomized controlled trials comparing TARE to sorafenib are currently available. It is difficult to compare the efficacy of TARE to sorafenib in advanced HCC due to the significant crossover. Hilgard et al 67 in their observational cohort study showed that in comparison to the SHARP trial 59 which led to the approval of sorafenib, the median OS in patients with advanced stage HCC treated with Y90 glass TARE is longer (16.4 months) 67 than that in patients with advanced-stage HCC treated with sorafenib (10.7 months). 59 The main obvious disadvantage of sorafenib compared to TARE are the significant side effects, which results in treatment discontinuation in 44% and dose reduction, or withdrawal in 64% of cases. 59,86
The PVT develops in approximately one-third of all patients with unresectable HCC. 66 These patients are usually excluded from embolic liver-directed therapies since the normal liver parenchyma exclusively relies on blood flow from the hepatic arteries when the portal vein is occluded. However, Y90 glass microspheres are found to be safe for use in this group of patients, as these microspheres are minimally embolic. 87 The study of Mazzaferro et al 64 demonstrated the safety and feasibility of TARE in patients with PVT. The median OS was 9 months in patients with main PVT and it was 17 months in patients with left or right portal vein or segmental branch PVT. 64 Two very recent studies reported significant advantage of TARE over sorafenib treatment in patients with PVT. 88,89 In the study of de la Torre et al, 88 the median OS was 8.8 months in the TARE group and 5.4 months in the sorafenib group. Edeline et al 90 reported a retrospective study of 151 patients with PVT; median OS was 18.8 months after TARE and 6.5 months with sorafenib treatment. Propensity score analysis of the data showed even larger difference between TARE and sorafenib groups (26.2 vs 8.7 months). 89
Another potential use of TARE is in downstaging as a bridge to liver resection or transplantation in selected candidates. Kulik et al 91 retrospectively analyzed 150 patients with unresectable HCC who were treated with Y90 glass microspheres. A total of 19 out of 34 (56%) patients were successfully downstaged from United Network for Organ Sharing (UNOS) T3 stage to T2, and of these patients, 8 (23%) underwent liver transplantation. Twenty-three of the 35 were downstaged to either percutaneous ablation eligible T2 status with lesions 3.0 cm or less, or resection. Lewandowski et al 69 compared the outcome of 86 patients treated with either TACE (43 patients) or TARE (43 patients) with similar median tumor size (TACE: 5.7 cm, TARE: 5.6 cm). In this study, TARE outperformed TACE in downstaging HCC in patients from UNOS T3 to T2 (58% vs 31%, respectively). Ibrahim et al 92 reported that 4 of the 8 patients with unresectable caudate lobe HCC were downstaged to within transplantation criteria after using Y90 glass microspheres. In the retrospective review by Tohme et al 93 of 20 consecutive patients with HCC who were listed for liver transplant and were treated with TARE as a bridging therapy, all 14 patients meeting the Milan criteria at the time of the first TARE remained within the criteria, and 2 of 6 patients who did not initially meet the criteria (33%) had their disease successfully downstaged.
Side Effects of Radioembolization
Despite being performed on patients with moderate liver dysfunction, TARE is a safe outpatient procedure with low hepatoxicity, especially when treatments are delivered superselectively. 94 The most common side effect is postradioembolization syndrome (PRS), which can occur in 10% to 70% of patients. 30,94 The PRS usually lasts 1 to 2 of weeks and consists mostly of fatigue, but patients can also have nausea, vomiting, abdominal pain, and cachexia. The PRS is usually self-limited and treated conservatively.
Radioembolization-induced liver disease (REILD) is a serious complication ranging from 0% to 4% of cases, secondary to radiation exposure of healthy hepatic parenchyma. 30,95,96 The REILD consists of hepatomegaly, ascites, jaundice, and abnormal liver function test (elevated serum transaminases and alkaline phosphatase) and it can occur as late as 1 to 2 months postradioembolization. 96 Treatment is conservative, mainly aimed at relief of ascites-related symptoms. 96 The REILD may occur in up to 20% of patients who had undergone chemotherapy either before or after TARE. 97
Extrahepatic microsphere deposition that may result in radiation pneumonitis, radiation-induced gastric or duodenal ulcer (<5% of cases), acute pancreatitis, or radiation dermatitis (via the falciform artery) is rare, as it is usually prevented by meticulous work up angiogram, review of Tc-99 m MAA scintigraphy, careful dosimetry, and coiling of extrahepatic vascular collaterals. 30,71,98 Other rare complications include lymphopenia, thrombocytopenia, and arteriogram-related risks include vascular injury, contrast-induced nephrotoxicity, and allergic reaction to iodinated contrast media. 30 Biliary complications following TARE occur in less than 10% of patients, but patients who had prior biliary enteric interventions with nonfunctioning papilla of Vater are at higher risk. 30,99 In summary, the side effects of TARE are significantly better tolerated than other types of embolization, such as TACE, with a better quality of life. 83
Novel Concepts in Radioembolization: Radiation Segmentectomy and Radiation Lobectomy
The concept of radiation segmentectomy was first introduced by Riaz et al 100 as an alternative to ablation or surgical resection in patients who were not candidates secondary to tumor location, insufficient liver reserve, and comorbidities. A total of 84 patients with HCC were treated with high dose of Y90 glass microspheres administered into a selected segmental artery supplying the tumor. 100 The median dose delivered to the segment(s) assuming uniform distribution was 521 Gy, and when accounting for tumor hypervascularity and nonuniform distribution, the median dose delivered to the tumor and normal hepatic volume was 1214 Gy and 210 Gy, respectively. Response by necrosis guidelines was seen in 81% of patients, with a median TTP of 13.6 months and median OS of 26.9 months. Nine percent of patients exhibited grade 3 or 4 biochemical toxicities. A smaller retrospective study by Padia et al 94 included 20 patients with unresectable HCC who underwent superselective TARE targeted to a single liver segment using Y90 glass microspheres. Median dose to the treated segment was 254 Gy, and median dose to the tumor was 536 Gy. No clinically significant grade hepatotoxicity occurred. Complete necrosis was noted in 19 out of 20 patients (95%) and stable disease in 1 of 20 patients (5%). 94 Vouche et al 101 reported radiation segmentectomy using a median radiation dose of 242 Gy in 102 patients with treatment-naive, unresectable, solitary HCC ≤5 cm not amenable to ablation. By using mRECIST criteria, complete response, partial response, and stable disease were 47%, 39%, and 12%, respectively. In all, 33 patients were transplanted with pathology revealing 100% necrosis in 17 patients (52%) and 50% to 99% necrosis in 16 patients (48%).
Radiation lobectomy is an alternative to portal vein embolization (PVE) to increase the volume of the future liver remnant (FLR) in patients who are deemed unresectable due to small FLR. Radiation lobectomy is lobar injection of Y90 microspheres into the tumor containing right lobe leading to its atrophy and concomitant hypertrophy of the untreated left lobe. Several studies reported approximately 30% hypertrophy of FLR following TARE. 102 -106 In a matched-pair analysis comparing the capacity for hypertrophy induction of TARE using Y90 resin microspheres and PVE, Garlipp et al 103 found that FLR volume increase from baseline to follow-up after PVE or after TARE was significant in both groups but PVE produced significantly more FLR hypertrophy than TARE (61.5% vs 29%). 103 In this study, an interval of 6 weeks between TARE and follow-up imaging was considered appropriate. It is possible that TARE would have compared more favorably to PVE if more time was allowed between treatment and follow-up imaging. Although the hypertrophy of FLR occurs at a faster pace following PVE, several studies reported increased tumor growth in the embolized lobe. 107 -110 Besides inducing FLR hypertrophy, TARE also provides tumor control in the treated lobe. Lewandowski reported >50% pathologic necrosis in 92% of resected tumors following TARE. 104 Further prospective studies need to validate this concept, but the present data show that TARE has added benefit over PVE since it offers tumor control in the treated lobe in addition to FLR hypertrophy before curative surgical resection.
Transarterial Embolization Therapies for IHC
The IHC is an epithelial cell malignancy with pathologic features of cholangiocyte differentiation. The tumor is located proximally to the second degree bile ducts within the liver. 111 Morphologically, it can be classified by growth pattern as mass-forming, periductal infiltrating, and intraductal subtypes. 112 It is the second most common primary liver cancer after HCC and its incidence is more than doubled during the last few decades. 3
The IHC has a poor prognosis with a median OS with palliative treatment alone is 3 months 113 and less than 10% of all patients survive more than 5 years regardless of treatment. 114 Complete surgical resection is the only established potentially curative option for patients with IHC; 114 however, only 12% of patients has resectable disease at presentation because of advanced stage of the disease, anatomic location, limited hepatic function, or significant comorbidities. 115 Despite the attempted curative resection, the recurrence rate is high. A recent analysis of an international surgical database of 563 patients with IHC who underwent curative-intent surgical resection demonstrated 71% recurrence rate, and 85.5% of the recurrence involved the liver and 14.5% of patients had extrahepatic only recurrence. 116 Postoperative complication rates are high, ranging from 11% to 58%. 114
Patients who are not surgical candidates may receive palliative systemic chemotherapy. The available systemic chemotherapies and targeted therapies have limited success in IHC, and approximately 40% of patients are experiencing grade 3 or 4 toxicities. 117 The standard of care first-line treatment is gemcitabine–cisplatin combination which resulted in a prolonged median OS of 11.7 months, compared to 8.1 months with gemcitabine alone. 118 The highly desmoplastic nature of cholangiocarcinoma, its rich tumor microenvironment in the liver, and its profound genetic heterogeneity, are contributing factors to its therapeutic resistance. 111
Transarterial embolization therapies work best on hypervascular tumors, like HCC, where the hypervascular nature ensures efficient delivery of the embolization microspheres to the tumor parenchyma. Unlike HCC, IHC is not overtly hypervascular on computed tomography (CT) and magnetic resonance imaging (MRI) studies. The typical presentation of IHC on cross-sectional imaging is irregular peripheral enhancement and central hypoenhancement in arterial phase with delayed enhancement of the tumor center. 112 Histologic analysis showed that viable tumor cells are usually located at the periphery of IHC and corresponds to the area of early arterial enhancement and rapid washout, whereas the central area is composed mainly of loose connective tissue with an abundant intercellular matrix which shows enhancement on delayed phase images. 119 On angiography tumor enhancement is frequently seen in IHC indicating relative hypervascularity of the tumor compared to the normal liver parenchyma. 120 Based on these findings, transarterial treatment of IHC is not unreasonable. Several studies reported the use of transarterial embolization to treat unresectable IHC with promising results as detailed below.
TACE Treatment for IHC
TACE is the most commonly reported liver-directed therapy in IHC patients. Park et al demonstrated considerable survival benefit in the group of 72 IHC patients treated with cTACE compared to the control group of 83 patients who received supportive care only; the median OS was 12.2 months in the cTACE group and 3.3 months in the control group. 121 The largest TACE series included 115 patients who were treated with cTACE involving various chemotherapy protocols (gemcitabine alone, gemcitabine and mitomycin C with or without cisplatin) during the 11-year period of the study. 122 The median OS was 13 months from the start of the TACE treatments, and there was no statistically significant difference between the different chemotherapy protocols. On the contrary, Gusani et al 123 demonstrated better survival when cTACE was performed with gemcitabine and cisplatin or oxaliplatin combination compared to gemcitabine alone (13.8 vs 6.3 months). Another large series of 62 IHC patients treated with cTACE (cisplatin, doxorubicin, and mitomycin C) reported similar OS of 15 months from the start of the treatment. 124 Shen et al 125 reported the use of cTACE in an adjuvant setting after hepatic resection and reported that cTACE could not delay IHC recurrence but could prolong OS.
The DEB-TACE was also successfully used to treat IHC. Schiffman et al 126 used irinotecan or doxorubicin-loaded LC beads in 24 patients with unresectable IHC and reported 17.5 months median OS (it was not specified whether the survival was calculated from the time of diagnosis or from the first treatment). A smaller study including 11 patients treated with doxorubicin-loaded DEB reported 13 months median OS from the treatment. 127 Kuhlman et al 128 reported increased OS of 11.7 months in 26 patients treated with irinotecan DEB-TACE compared to 5.7 months in patients treated with cTACE (mitomycin C), but DEB-TACE was not superior compared to the 11 months OS of patients treated with systemic chemotherapy with gemcitabine and oxaliplatin.
Meta-analysis of 16 studies reporting cTACE and/or DEB-TACE treatment of IHC patients showed 13.4 months OS from the time of the first TACE treatment. 129 The 30-day mortality was 0.7%, but the complication rate was relatively high with severe toxicities reported in 18.9% patients. It was concluded that TACE confer a survival benefit of 2 to 7 months compared with systemic chemotherapy. 129 The meta-analysis revealed 18.9% severe toxicities (≥grade 3) following TACE procedures. It should be noted that most of the TACE studies are retrospective in nature and used a wide range of chemotherapeutics and different embolization materials and nonstandardized treatment schedule.
TARE Treatment for IHC
Radioembolization offers an alternative transarterial treatment for IHC patients. The largest published series included a retrospective analysis of 46 IHC patients from a single institution who underwent radioembolization with Y90 glass microspheres during an 8-year period. 130 Overall survival for the entire group was not reported. Stratified survival analysis showed 15.6 months OS from the start of the treatment in patients with mass-forming tumor morphology compared to 6.1 months in patients with infiltrative tumor morphology. The most common clinical toxicity was fatigue in 54% of patients and transient, vague abdominal pain in 28% of patients. Four patients experienced grade 3 albumin toxicity and 3 patients experienced grade 3 bilirubin toxicity. 130 Hoffman et al 131 reported 22 months median OS from start of the treatment in 33 patients treated with Y90-loaded resin microspheres. Patients included in this study had no significant extrahepatic disease, which may explain the excellent survival results. Five other studies reported the treatment of patients with IHC (18-26 patients/study) using Y90 resin microspheres, and OS from the time of treatment ranged between 9.3 to 16.3 months. 132 -136 Multi-institutional analysis by Hyder et al 137 reported 11.3 months survival following Y90 radioembolization in 46 patients. Unfortunately, the details of the Y90 treatments were not reported, but the study likely included patients treated with either resin or glass Y90 microspheres.
TACE Versus TARE for the Treatment for IHC
A recent review by Seidensticker et al 138 summarized the prognostic factors of TACE and TARE in patients with IHC. They pointed out that good liver function, tumor hypervascularity, solitary disease, tumor size less than 8 cm, and previous systemic chemotherapy were positive prognosticators when patients were treated with TACE. In patients who underwent radioembolization, good performance status (ECOG 0), mass-forming tumor morphology, solitary disease, low tumor burden, the absence of PVT, and previous treatment with TACE were associated with improved survival.
The effectiveness of different transarterial treatments of IHC has not been studied in randomized controlled trials. All of the abovementioned studies demonstrated increased survival of unresectable patients with IHC treated using either TACE or TARE. However, the heterogeneity of the patient populations, the small sample sizes, and the retrospective nature of most of the transarterial treatment studies make the interpretation of the results difficult. Since transarterial treatments were mostly used in salvage situations when other therapies failed, the interpretation becomes even more complicated. Transarterial chemoembolization and TARE may have a role beyond palliative settings. Several study reported patients who were successfully downstaged by TACE or TARE treatments and were able to undergo resection or liver transplant. 120,126,130
There is no direct comparison between TACE and TARE in patients with IHC. The patient selection criteria to different types of transarterial treatments are unclear and likely influenced by the institutional availability of embolic materials, operator experience and preference, and patient’s comorbid conditions. Because TARE is generally better tolerated by patients and its side effects are generally lower compared to TACE, 129,139 radioembolization may be considered as first choice transarterial treatment over TACE in patients with unresectable IHC.
In summary, the results reported across a wide variety of studies demonstrated survival benefit of transarterial treatments for patients with unresectable IHC. These therapies can have a role in treatment protocols of patients with unresectable IHC. Multi-institutional randomized controlled trials are needed to provide level 1 evidence of the efficacy of TACE and TARE in this patient population.
Percutaneous Image-Guided Ablation of HCC
Patients with BCLC very early stage (single tumor ≤2 cm in size) and early stage (up to 3 tumors less ≤3 cm in size) HCC can benefit from curative treatments including liver transplantation, surgical resection, or ablation. 140 Liver transplantation is considered the best option, because it treats both the tumor and the underlying liver disease, but it is severely limited by a shortage of liver donors. 141 Currently, surgical resection is regarded as the treatment of choice for very early and early stage HCC. 140 However, resection is not an option for 90% of patients because of the location of the lesion, significant portal hypertension, impaired liver function, or concurrent medical conditions. 49 Nowadays, image-guided ablation is a standard alternative option for patients who are not surgical candidates. Moreover, thanks to advancement of ablation technologies, the most recent data indicate that outcomes of percutaneous ablation are comparable to or in some cases better than surgical resection which may change the treatment paradigm of very early and early stage HCC in the near future. 4
For many years, percutaneous ethanol injection (PEI) was the primary image-guided ablation treatment for HCC. Ethanol induces cellular dehydration, protein denaturation, and occlusion of small vessels leading to cell necrosis. In cases of nodular HCC, complete necrosis was achieved in 70% of small lesions. 142 There is no randomized controlled trial comparing PEI to surgical resection; however, 1 retrospective study and 2 cohort studies failed to demonstrate survival benefit of resection compared to PEI despite the fact that patients in the surgery group had better underlying liver function. 143 -145 The PEI is associated with high local recurrence rates, especially in tumors larger than 3 cm where 1- and 2-year recurrence rates were 40% and 67.5%, respectively. 146
In recent years, there has been significant advancement and development of energy-based ablative technologies, including radiofrequency ablation (RFA), microwave ablation (MWA), cryoablation, irreversible electroporation (IRE), laser ablation, and high-intensity focused ultrasound (HIFU) ablation. Energy-based ablative techniques have shown higher efficacy, better disease control, and better survival compared to PEI for lesions larger than 2 cm; and these techniques have now largely replaced PEI. 147,148
The RFA represents the oldest and most studied energy-based percutaneous ablation modality. The RFA uses high-frequency alternating electric current. The mechanism of cell death in RFA is based on electric power dissipation as frictional heat. Therefore, the effectiveness of RFA depends on the conductivity of the tissues, which is strongly correlated with water content. 149 Temperatures above 100°C lead to tissue dehydration and carbonization, which is an intrinsic barrier to further RFA heating. 150 This temperature threshold limits the heating capacity of an RFA probe and also makes RFA sensitive to heat sink effects of flowing blood in adjacent vessels. 151 To achieve larger ablation volumes, multiple RFA probes can be used.
Three randomized controlled trials could be found in the literature comparing RFA with surgery for early stage HCC, the results of which are mixed. Two studies showed that OS and disease-free survival were similar, 152,153 with overall 1-, 2-, and 3-year survival rates of 97.5%, 91.2%, and 82.5% for the ablation group, respectively, and 93.7%, 86.2%, and 77.5% for the surgical resection group, respectively (P = .207). In this same study, local recurrence rates were noted to be 37% for the ablation group and 35% for the surgical resection group. Another study showed lower OS and disease-free survival in the RFA group with 1- and 5-year OS rates of 87% and 55%, respectively, for the RFA group and 98% and 76%, respectively, for the surgical resection group (P = .001). In this same study, 1- and 5-year overall recurrence rates were 17% and 63%, respectively, for the ablation group, and 12% and 42% for the resection group, respectively. 154 Notably, all 3 randomized controlled trials demonstrated significantly shorter hospital stays and lower complication rates for the RFA group as compared to the surgery group (5.2 days for RFA vs 19.1 for surgery). In addition, it is important to note an inherent selection bias within several of these studies that compare surgical resection to RFA, particularly the retrospective studies. In a large number of these studies, RFA patients had worse baseline clinical characteristics as compared to surgical resection patients; for example, synthetic liver function 155 and Child-Pugh scores were worse in the RFA population. 156 This selection bias exists because at most institutions, patients with very early and early stage HCC are referred for surgical resection first and only referred for ablation if they are not considered good surgical candidates, thus introducing inherent selection bias into these retrospective studies. Finally, because of the lack of randomized controlled trials and various problems with retrospective studies evaluating RFA versus surgery, numerous meta-analyses have been undertaken. One wide-scale review evaluated 18 meta-analyses 157 and demonstrated mixed results regarding OS, disease-free survival and recurrence, with some favoring surgery, some favoring RFA, and some demonstrating no significant difference. 157 It is clear that even large meta-analyses offer mixed results comparing RFA to surgical resection. 158 Interestingly, even the quality of these reviews has been a topic of study. One study evaluated the quality of 19 systematic reviews of RFA versus surgery. 159 This study concluded that 3 randomized controlled trials were low in quality based on the Risk of Bias Tool in the Cochrane Handbook for Systematic Reviews of Interventions, 35 nonrandomized controlled trials were of moderate quality, and that the overall quality of systematic reviews comparing the efficacy of RFA versus surgery for early HCC was poor.
An MWA has emerged as an alternative method to RFA that appears to overcome many limitations of RFA. Microwave technology deposits energy into tissues through electromagnetic radiation-induced rotation of dipole molecules, such as water, resulting in frictional heat. 160 Microwave technology generates higher temperatures than RFA in a short time leading to larger ablation zones and less susceptibility to heat sink effects of adjacent blood vessels. 161 Unlike RFA, MWA can be effective in tissues with high impedance such as charred desiccated tissue.
Despite these theoretical technical advantages, initial studies did not show superiority of MWA over RFA in the treatment of HCC. 162,163 This may be due to the use of older, less-advanced MWA technologies in these studies. The most recent study comparing MWA to RFA demonstrated significantly lower local tumor progression in patients treated with MWA, and improved survival although this was not statistically significant. 164 The largest study to date of MWA for treatment of HCC included 1363 tumors in 1007 patients with a mean tumor size of 2.9 cm and mean follow-up of 17.3 months. 165 This study demonstrated an overall local tumor progression rate of 5.9%, which was considerably better than the results reported by Kim et al 166 who evaluated RFA of 1502 early stage HCC with an observed 19.4% local tumor progression rate. In the MWA study of Liang et al, the 1-, 3-, and 5-year cumulative survival rates were 91.2%, 72.5%, and 59.8%, respectively. 165 This 5-year survival result is comparable to that of surgical resection. 167 Takami et al 168 compared MWA with hepatic resection and demonstrated no difference in OS, disease-free survival, or local recurrence rates in patients with fewer than 3 lesions, each less than 3 cm in size. Shi et al 169 also reported that for solitary HCC smaller than 3 cm, the effectiveness of MWA was same as surgical resection.
An MWA is generally safe with very low mortality and major complication rates. Notably, because it is based on heating technology, which is coagulative, bleeding risk is inherently very low. A multicenter study that included 736 patients with 1.037 lesions reported 0% mortality, 2.9% major complications rates, and 7.3% minor complications rates. 170
Cryoablation is an established technology that leads to cell death via application of temperatures of less than −20°C. Current devices circulate high-pressure argon gas through the cryoprobe, to an expansion chamber in the needle tip. The resulting Joule-Thomson effect allows the probe to reach temperatures as cold as −160°C. Helium gas is circulated to enable the thawing process. Applying at least 2 freeze-thaw cycles leads to intra and extracellular ice crystal formation, dehydration, osmotic pressure change, cell membrane, and intracellular organelle damage and ultimately cell death. 171 The developing ice ball is easy to visualize with CT or MRI, which is the major advantage over RFA and MWA. The sharply delineated edge of the ice ball corresponds to the zero degree isotherm. Cryoablation has been preferred to RFA and MWA for ablation of masses adjacent to critical structures such as the diaphragm, 172 major blood vessels, 173 and gallbladder. 174 It should be mentioned that the safety of RFA ablation adjacent to the hepatic, nonperitonealized surface of the gallbladder has also been reported. 175,176 Cryoablation has been associated with less procedural and postprocedural pain as compared to other heat-based ablation technologies. 177 Cryoablation is also subject to heat sink effects of blood vessels, but some authors suggest that this is not as significant as during RFA. 178 The limitations of cryoablative technology include increased procedural time due to the typically larger number of probe insertions and longer ablation times (a typical freeze–thaw–freeze–thaw cycle lasts for 30-40 minutes). Another concern is the risk of “cryo-shock,” a phenomenon, resulting in multiorgan failure and disseminated intravascular coagulation after cryotherapy. 172 Cryoshock is presumably a systemic immunologic response to the release of necrotic cellular products and antigens into the blood pool. 179 Notably, complication rates in recent percutaneous image-guided cryoablation series are much lower than those reported in the era of surgical cryoablation. 180,181 Chen et al 182 reported cryoablation of 76 unresectable primary HCCs in 40 patients and 76 recurrent HCCs in 26 patients. The overall complication rate was 12.1%. Patients with unresectable HCC had 1- and 3-year OS rates of 81.4% and 60.3%, while the disease-free survival rates at 1 and 3 years were 67.6% and 20.8%, respectively. Patients with recurrent HCC had 1- and 3-year OS rates of 70.2% and 28.8%, while the disease-free survival rates at 1 and 3 years were 53.8% and 7.7%, respectively. 182 A randomized controlled trial including 180 patients in each group compared cryoablation to RFA and demonstrated significantly lower local tumor progression for cryoablation than RFA (local tumor progression rates at 1, 2, and 3 years were 3%, 7%, and 7% for cryoablation and 9%, 11%, and 11% for RFA, respectively), but the survival rates were similar (1-, 3-, and 5-year tumor-free survival rates were 89%, 54%, and 35% in the cryoablation group and 84%, 50%, and 34% in the RFA group). 183 Similarly, Ei et al 178 demonstrated significantly improved local control with cryoablation for the treatment of primary HCCs of less than 2 cm in size compared with RFA and MWA. Despite these promising results, cryoablation is less popular than RFA and MWA for hepatic ablation which is likely due to the cost, increased procedure time, relatively common postprocedure thrombocytopenia which requires overnight observation and sometimes platelet transfusion, and increased risk of bleeding complications. 184
Irreversible electroporation (IRE) is the latest addition to the armamentarium of ablation technologies. The IRE delivers 70 to 90 microseconds pulses of high-voltage (up to 3000 V) electric currents that create permanent nanopores on cell membranes disrupting the cellular homeostasis and leading to apoptotic cell death. 185 IRE is performed under general anesthesia with complete neuromuscular blockade to prevent muscle contractions triggered by the high-voltage currents. To prevent ventricular arrhythmias, the ablation pulses are electrocardiogram gated and delivered during the absolute refractory period of the cardiac cycle. 186 Studies have demonstrated that IRE can be used safely adjacent to blood vessels and bile ducts. 187 -189 Since IRE is a predominantly nonthermal ablation technology, it is not affected by the heat sink effect of adjacent blood vessels. Based on these potential advantages, IRE can be considered for ablation of central liver tumors and tumors adjacent to sensitive structures (gallbladder, major bile ducts, and bowel loops).
Limited data are available on the efficacy of IRE to treat HCC due to the relative novelty of this ablation technique. Thomson et al reported 82.3% complete response rate following IRE ablation of 17 HCC lesions in 10 patients. 190 Cheung et al 191 reported IRE ablation of 17 HCC in 11 patients and found 73% complete response overall, and 93% complete response of tumors smaller than 3 cm. The reported complication rate in both studies was minimal. Although the local tumor control achieved with IRE appears inferior when compared to RFA and MWA, a review concluded that IRE is safe and effective for ablation of tumors adjacent to blood vessels and bile ducts where other ablative techniques cannot be used. 192
Laser ablation is a novel ablative technique that uses laser devices that transform electrical energy into light energy, which in turn interacts with tissue to produce heat and cause cell death. 193 Although little data have been produced on laser ablation, several small retrospective studies have demonstrated favorable OS rates. 194 In the only randomized prospective trial comparing laser ablation with RFA, OS and median time to tumor recurrence were not significantly different between the 2 groups. 195 Overall, laser ablation is an ablative technique that requires further evaluation. 196
An HIFU is a new technology that uses multiple acoustic transducers to focus beams of ultrasounds into a small area where the mechanical vibrational energy produces heat to destroy tissue. 197 There are no data comparing HIFU to other ablative techniques for early stage HCC. Only 1 study combines HIFU with TACE and compares it to TACE alone, demonstrating improved OS for the combined group. 198
In conclusion, percutaneous ablation of HCC is less expensive and less invasive than surgical resection and is associated with lower complication rates, greater preservation of liver parenchyma, and shorter hospital stays; therefore, ablation is increasingly considered the first-line option in the potentially curative treatment of very early and early stage HCC. 2 The ongoing technical developments in the field of percutaneous image-guided tumor ablation will likely further improve local tumor control rates and the ability to successfully ablate even larger tumors in the near future.
Percutaneous Image-Guided Ablation of IHC
An IHC is usually diagnosed in an advanced stage, and most patients are not eligible for percutaneous ablation. A few studies have reported the use of RFA to treat primary IHC and even the largest study included only 17 patients. 199 -203 One study reported the RFA treatment of 20 patients with recurrent IHC after curative surgical resection and found good local disease control with local tumor progression-free survival of 74%, 74%, and 74%, and cumulative OS of 70%, 60%, and 21% at 1, 2, and 4 years, respectively. 204 The local recurrence rate appears higher compared to HCC, which may be due to the more infiltrative growth pattern of IHC. Padia 205 recommended generous ablative margins of at least 10 mm around IHC lesions to minimize local tumor recurrence. A recent meta-analysis of 7 observational studies comprising 84 IHC patients reported the pooled 1-, 3-, and 5-year survival rates as 82%, 47%, and 24%, respectively. 206 The studies are very limited, but the reported results of ablation are similar or better than results of surgical resection with curative intent. 114 Only 1 study reported the use of MWA for IHC and found cumulative OS of 60.0%, and 60.0%, at 1 and 2 years after MWA ablation of IHC in 15 patients. 207 The available data suggest that percutaneous ablation can be considered for the primary treatment of IHC in eligible patients.
Conclusion
The HCC and IHC are primary liver cancers where all or most of the tumor burden is usually confined to the liver. Therefore, locoregional liver-directed therapies can provide an opportunity to control intrahepatic disease progression with minimal systemic side effects. This review demonstrates that liver-directed therapies provide survival benefit for appropriately selected patients with HCC and IHC compared to best medical treatment and have lower comorbid risks compared to surgical resection. Percutaneous liver-directed treatment options should be considered especially in patients with unresectable disease.
Footnotes
Authors’ Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.