
Abstract
The aim of this study was to explore if turn duration and the performance of step parameters during segments of the Timed Up and Go (TUG) test with and without cognitive dual-tasking (TUGdt) can discriminate between individuals with different cognitive ability. Participants were divided into groups (dementia = 57, mild cognitive impairment = 126, subjective cognitive impairment = 71, and controls = 50) and performed TUG and TUGdt (naming animals and reciting months in reverse order, respectively). Turn duration and forward and return walk (step parameters) were compared between adjacent groups for all conditions. Results were analyzed with logistic regression models, presented with standardized odds ratios, and generally showed longer turn duration during TUGdt for groups with lower levels of cognitive ability, whereas a small tendency was observed for step length/body height. While these results need to be confirmed, they may indicate the potential of assessing TUG segments, particularly turn duration, to identify risk of cognitive impairment.
Trial registration number
NCT05893524.
Introduction
Cognitive deterioration and impairment are highly debilitating conditions, ranging from subtler impairment (such as subjective cognitive impairment) to more severe impairment, in the form of dementia disorders. Whereas dementia disorders are considered a global public health priority by the World Health Organization (“Global Status Report on the Public Health Response to Dementia,” 2021), both the diagnoses of subjective cognitive impairment (SCI) and mild cognitive impairment (MCI) have been identified as potential precursors of this disease (Mendonca et al., 2016). However, several modifiable dementia risk factors have been identified (Dukelow et al., 2022) and supported by health-promoting and disease-managing interventions. To enable the initiation of such interventions at the earliest possible stage, it is therefore of utmost importance to explore novel methods of identifying risk of cognitive decline.
Increasing evidence has shown associations between cognitive and motor decline (Leroy et al., 2023; Montero-Odasso et al., 2012; Mullin et al., 2022; Verghese et al., 2013), and deviant gait has even been found to precede objectively identified cognitive decline by several years (Skillback et al., 2022). Although it is well established that gait disturbances occur among individuals with dementia, more recent findings have also identified the deterioration of specific step parameters, such as step length, step time, swing time, and stance time. In addition, a recent meta-analysis (Salzman et al., 2025) found that gait speed during dual-task gait (i.e., simultaneously performing an additional task while walking) (McIsaac et al., 2015) discriminated between individuals with SCI and MCI, although there were no differences between individuals with SCI and controls. Contrasting this, emerging research investigating specific step parameters has found indications of decreased performance among individuals with SCI in comparison with controls (Löfgren et al., 2025), findings that highlight the importance of exploring the discriminatory capacity of subtler step parameters.
Studies (Katsumata et al., 2011; McGough et al., 2011) have also shown that reduced cognitive ability is associated with poorer performance of the Timed Up and Go (TUG) test (Podsiadlo & Richardson, 1991). The TUG test is an easily administered and well-established clinical test entailing: rising from a standard chair with armrests, walking 3 m, completing a 180-degree turn, walking back, and sitting down again. As a test constituting several segments, TUG challenges motor planning and executive functions (Herman et al., 2011), and the time to complete it has been widely investigated in various populations. However, along with technological advances in recent years, increased research interest has been directed toward exploring if the performance of specific segments of TUG may reveal subtle but important information of clinical relevance. Due to the multifaceted characteristics of TUG, this test increases demands on different cognitive and functional domains as the different segments occur (Sunderaraman et al., 2019). Primarily, the 180-degree turn has been investigated, where results indicate an added capacity for identifying a history of falls (Brauner et al., 2022). However, also the two different walking segments (prior and post the turning point) have been investigated with regard to its discriminatory capacity, as well as an outcome in exercise interventions (Bottinger et al., 2024; Ortega-Bastidas et al., 2023). As TUG performance under dual-task conditions (TUGdt) has been found to correlate with cognitive decline and is considered a potentially valuable clinical tool in this population (Lima et al., 2015), it may be of particular importance to explore if the performance during different segments during TUG and TUGdt conditions might discriminate between individuals with different cognitive ability.
Motor outcomes have previously been found to discriminate between individuals with dementia and cognitively less affected groups, whereas results between adjacent groups are more rare. This supports the exploration of subtler outcomes during attention demanding situations. The aim of the current study was therefore to explore if the performance of step parameters during different segments of the TUG and TUGdt, including the duration of the 180-degree turn, can discriminate between adjacent groups of individuals with dementia, MCI, SCI, and controls.
Method
We conducted an observational cohort study as part of an ongoing longitudinal study. The Regional Ethical Review Board in Uppsala and the Swedish ethical review authority approved this study, and informed consent was obtained from all participants prior to study commencement. We report how we determined all manipulations and all measures in the study.
Participants
Patients were recruited during the years 2015–2017 when undergoing memory assessment at two specialist clinics. The procedure for cognitive diagnosis followed established criteria (Chui et al., 1992; McKeith, 2006; McKhann et al., 2001, 2011) was part of the clinical routine for patients assessed for memory impairment and was conducted by a clinical geriatrician specializing in cognitive impairment and dementia. The assessment included careful evaluation of the patient’s history, structural brain imaging, and cognitive testing. The cognitive tests included the Clock Drawing Test, the national version of the Mini-Mental State Examination (MMSE-SR) (Palmqvist et al., 2013), the Verbal Fluency Test, and the Trail Making Test A and B. Supplemental assessments such as neuropsychological testing and cerebrospinal fluid analysis were carried out when considered relevant. Participants who complained about cognitive decline and had taken part in full cognitive assessment where clinical evaluation and objective measures did not indicate cognitive impairment were diagnosed with SCI (Jessen, 2014). Exclusion criteria for patients were inability to walk 3 m back and forth or to rise from a sitting position, indoor use of a walking aid, current or recent hospitalization (within 2 weeks prior to the assessments), or need of an interpreter to communicate. In addition, a sample of 50 cognitively healthy individuals was recruited as controls through advertisements and flyers (May 2017 to March 2019). The inclusion criteria for controls were subjective perception of normal cognitive function and an MMSE-SR score >26, while the exclusion criteria were the same as for the patients.
Data Collection
Data collection for all participants was carried out by a trained physiotherapist and followed the procedure that has previously been described in detail (Y. Cedervall, Halvorsen & Åberg, 2014; Y. Cedervall, Stenberg, et al., 2020). Reported demographic characteristics included educational level (university education or not) and civil status. The assessments were carried out in the following order: first, TUG as a single task, entailing rising from a chair with armrests, walking 3 m at a comfortable pace, crossing a 3-m line, turning around, walking back, and sitting down again (Podsiadlo & Richardson, 1991). This was followed by assessments of two types of TUGdt, respectively: TUG while simultaneously naming different animals (TUGdt-NA) and while reciting months in reverse order, starting with December (TUGdt-MB). The time to complete TUG and TUGdt was registered with a stopwatch, starting with the participant’s back leaving the backrest and stopping when their posterior touched the seat of the chair again. The standardized instructions to the participants were to complete all TUG tests at preferred speed, concerning both mobility and verbal performance, and to complete the mobility sequence even if they did not know what to say. The TUG tests were also recorded by two synchronized high-definition video cameras and thus documented by video recordings of movement and speech.
Data Preparation
For TUGdt-NA and TUGdt-MB, the number of correct words mentioned per 10 seconds during the test performance was calculated and documented as TUGdt-NA or TUGdt-MB words/time: 10*(number of correct words/TUGdt completion time). Quantification of correct words recited during TUGdt-NA and TUGdt-MB was performed by reviewing the video recordings and followed the procedures used in established norms for such tests. For TUGdt-NA, both naming an animal group (e.g., fish) and a specific animal (e.g., salmon) were accepted (Tallberg et al., 2008). For TUGdt-MB, the number of correct months in the correct order was counted. A month was classified as correct when the participant started with December and then recited months in the correct order relative to the month said previously, with permission to repeat but not to omit or transpose the months (Ostberg et al., 2012).
The following segments were compared between adjacent groups for all three TUG conditions (TUG, TUGdt-NA, and TUGdt-MB): forward walk (the walking segment occurring prior to the 180-degree turn), the 180-degree turn, and return walk (the walking segment occurring after the 180-degree turn). For the forward and return walks, the following step parameters were analyzed: step duration, double stance (DS) duration, single stance (SS) duration, step length/body height, and step width. For turn duration, the time (seconds) to complete the 180-degree turn was analyzed.
Data processing for the step parameters was based on the documentation from two synchronized high-definition video cameras using a semi-automatic method aided by a technique for human 2D pose estimation based on a deep learning procedure, described in more detail elsewhere (Åberg et al., 2021) (see Supplementary Material). Based on determined events of contact points of the heel with the ground (i.e., heel strike), steps were quantified during gait, in two segments of straight walking: (a) forward walk during gait toward the 3-m line, starting with the second heel strike and ending with the last heel strike for which no part of the foot had passed the line and (b) return walk during gait back to the chair, starting with the first heel strike for which the whole foot had passed the 3-m line and ending with the last heel strike that did not appear to be preparation for sitting down, as indicated by a foot twist or an atypical short step.
Turn duration (between forward walk and return walk) was measured in seconds from the last heel strike of gait before the 3-m line and ending at the first heel strike of gait back to the chair, as described above.
Quantification of the step parameter outcomes was based on the identified events and positions of the heel points. The 3D positions of the heel points were obtained with the use of a calibration procedure in which known points on the floor were related to image points.
Step duration, SS duration, and DS duration were calculated from the times (in ms) of the identified gait events. Step length was calculated as the distance (cm) between posterior marker points on the heel at heel strike. Since step length is inherently related to body height (Park et al., 2022), we divided each participant’s mean step length with their body height (centimeters) to calculate the body/height ratio (%) (Morio et al., 2019). Step width was determined by the distance (centimeters) between the lateral point of markers of the heels at heel strike.
Data Analysis
Participants’ characteristics were summarized using means and standard deviations or frequencies and percentages by diagnosis groups. The TUG step parameters were not normally distributed and were therefore presented as medians with interquartile ranges and minimum and maximum values. For TUGdt-MB turn duration, time distributions (seconds) were presented as a box plot by diagnosis groups.
For statistical analyses, SAS® version 9.4 (SAS Institute Inc., Cary, NC, USA) was used. TUG step parameters with a Shapiro-Wilks’s test statistic w <0.95 were transformed using natural logarithms. Using logistic regression models, associations were examined between the TUG and TUGdt step parameters and the dichotomous outcome variables dementia disorders versus MCI, MCI versus SCI, and SCI versus healthy controls, respectively. In addition, analyses for dichotomous outcome variables defined as non-adjacent groups (dementia disorders vs. SCI, dementia disorders vs. healthy controls, and MCI vs. healthy controls) were presented as a Supplementary File (Supplemental Table S1). Results were presented as standardized odds ratios (sORs), that is, the increase in odds per 1 SD increase of the TUG step parameter, with 95% confidence intervals (95% CI) and p-values. The logistic regression models were estimated with adjustment for participant age (as a continuous variable), sex, and educational level. Statistical tests were two-tailed, and the nominal significance level was set at p < .05. To account for multiple testing while considering the correlation between tests for each of the three pre-specified dichotomous outcome variables (dementia disorders vs. MCI, MCI vs. SCI, and SCI vs. healthy controls), we estimated the number of effective independent tests (Meff) using the method of Li and Ji (2005), which with the Šidák correction applied to determine the adjusted significance threshold. In contrast to other methods which can substantially reduce power when variables are correlated (e.g., Bonferroni or Holm–Bonferroni), the Li and Ji method maintains control of Type I error while preserving greater statistical power. The number of tests for each of the three dichotomous outcome variables was 27 and Meff = 9, that is, adjusted alpha = 1 − (1 − 0.05)1/Meff = 0.00568.
The Receiver Operating Characteristic (ROC) curve and the area under the ROC curve (c-statistics) were presented as a global measure of discrimination between individuals with SCI and controls for turn duration time during TUGdt-MB, where ≥0.7 was considered acceptable (Hosmer, 2000). However, since our findings are exploratory and need to be confirmed in independent studies before any practical thresholds are considered, we refrained from reporting a specific cut-off based on sensitivity and specificity.
Results
Participants
Participants (n = 304) were divided into the following groups based on the diagnosis set by the clinical geriatrician: dementia (n = 57, mean age: 78, 51% women, median MMSE-SR score: 22); MCI (n = 126, mean age: 73, 42% women, median MMSE-SR score: 26); SCI (n = 71, mean age: 67, 45% women, median MMSE-SR score: 29); and controls (n = 50, mean age: 73, 44% women, median MMSE-SR score: 29). The median time to complete TUG in the different groups was: dementia: 15.1 seconds; MCI: 12.6 seconds (IQR = 11.1–14.7); SCI: 10.8 seconds (IQR = 9.8–12.9); and controls: 10.4 seconds (IQR = 9.2–12.1). Table 1 shows full details on participant demographics in the different groups, including performance of the full TUG during the different conditions.
Participant Characteristics: TUG & TUGdt Test Results and Step Parameters by Group.
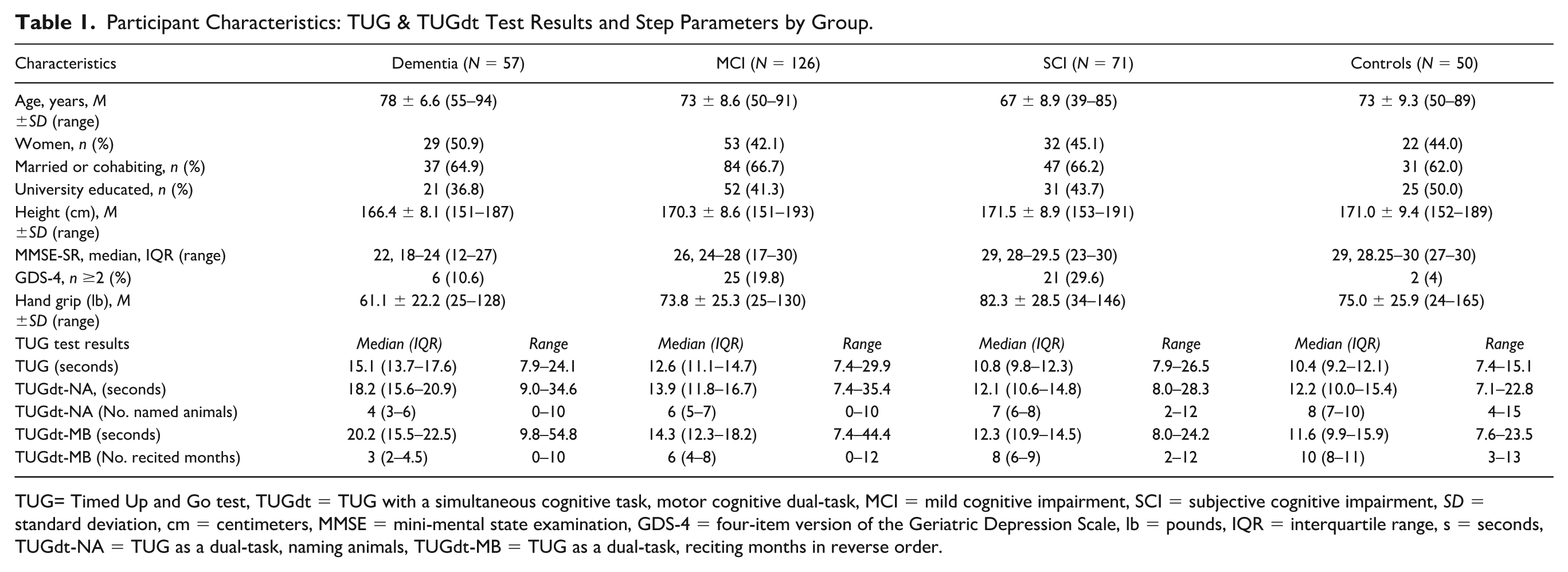
TUG= Timed Up and Go test, TUGdt = TUG with a simultaneous cognitive task, motor cognitive dual-task, MCI = mild cognitive impairment, SCI = subjective cognitive impairment, SD = standard deviation, cm = centimeters, MMSE = mini-mental state examination, GDS-4 = four-item version of the Geriatric Depression Scale, lb = pounds, IQR = interquartile range, s = seconds, TUGdt-NA = TUG as a dual-task, naming animals, TUGdt-MB = TUG as a dual-task, reciting months in reverse order.
Segmental Comparison of Extracted Gait and Turn Parameters Between Adjacent Groups
Table 2 presents the median result, IQR, and ranges for the extracted step parameters and turn duration during each TUG condition and TUG segment: step duration (ms), DS duration (ms), SS duration (ms), absolute step length (cm) step length/body height (%) and turn duration (seconds). Figure 1 presents sORs, 95% CIs, and p-value for turn duration (seconds) between each adjacent group during each TUG condition. Variability of turn duration during TUGdt-MB for the groups of individuals with dementia, MCI, SCI, and the control group is illustrated in Figure 2, whereas Figure 3 presents the ROC curve for the comparison of turn duration (seconds) between the SCI and control group during TUGdt-MB. The full results for each analysis between adjacent groups during each TUG segment and condition are found in Table 3. In addition, identical comparisons for non-adjacent groups are presented in Table S1.
Results of the TUG and TUGdt Segments.
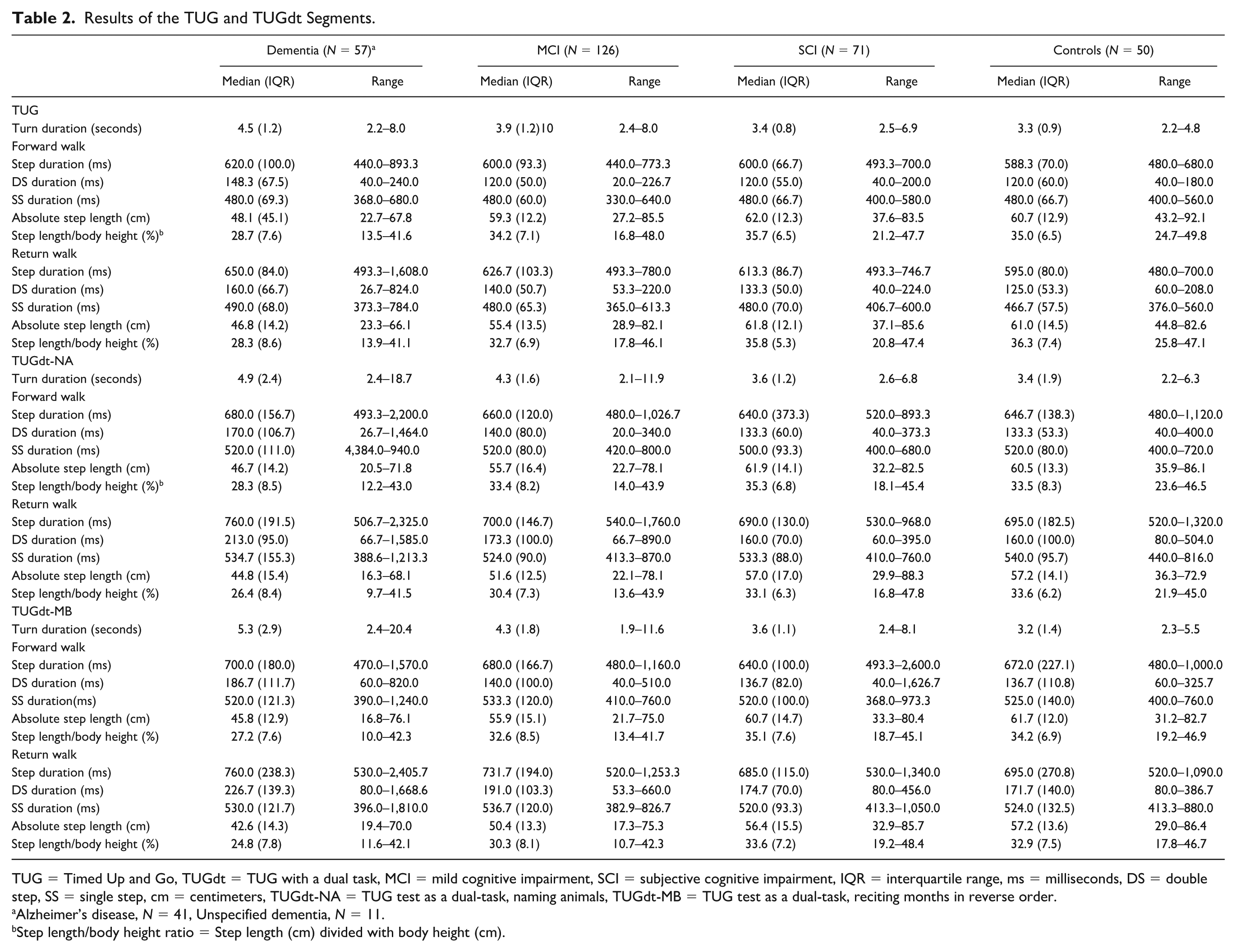
TUG = Timed Up and Go, TUGdt = TUG with a dual task, MCI = mild cognitive impairment, SCI = subjective cognitive impairment, IQR = interquartile range, ms = milliseconds, DS = double step, SS = single step, cm = centimeters, TUGdt-NA = TUG test as a dual-task, naming animals, TUGdt-MB = TUG test as a dual-task, reciting months in reverse order.
Alzheimer’s disease, N = 41, Unspecified dementia, N = 11.
Step length/body height ratio = Step length (cm) divided with body height (cm).
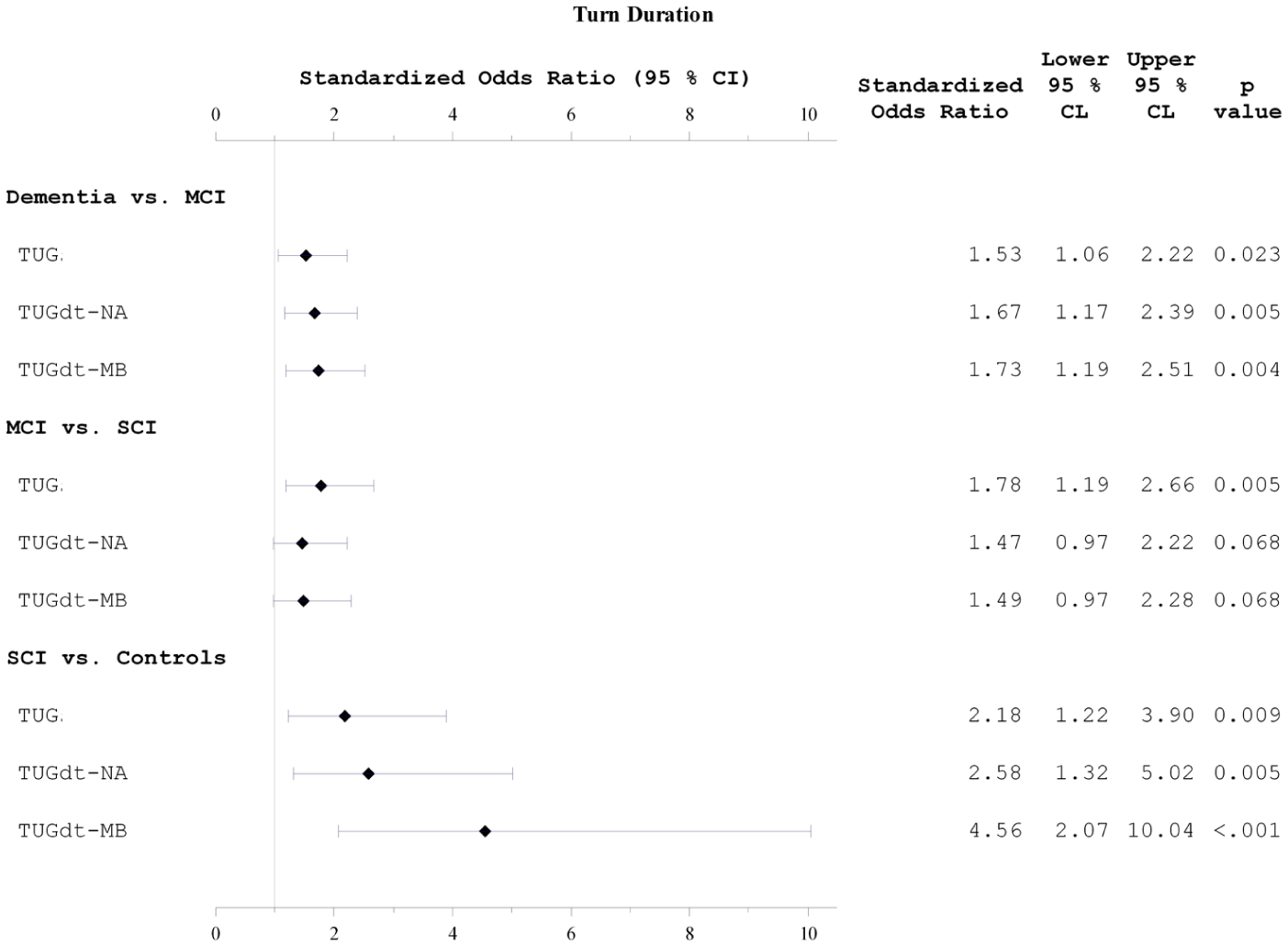
Forest Plot of Logistic Regression Models to Assess Relationship Between Turn Duration During the Different TUG conditions Between: Dementia Disorders Versus MCI, MCI Versus SCI, and SCI Versus Healthy controls.
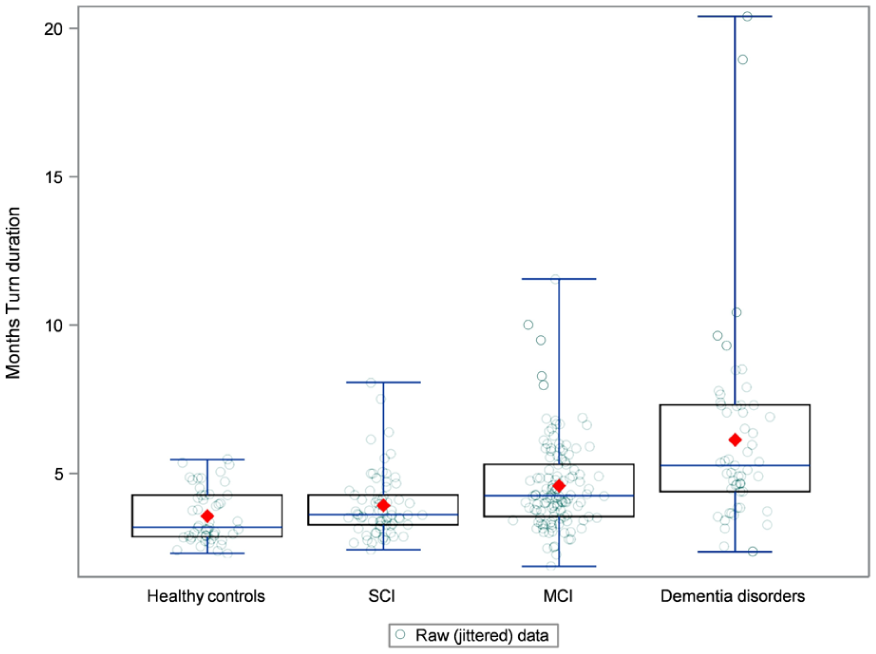
Boxplot Illustrating the Distribution of Results for Turn Duration during TUGdt-MB.
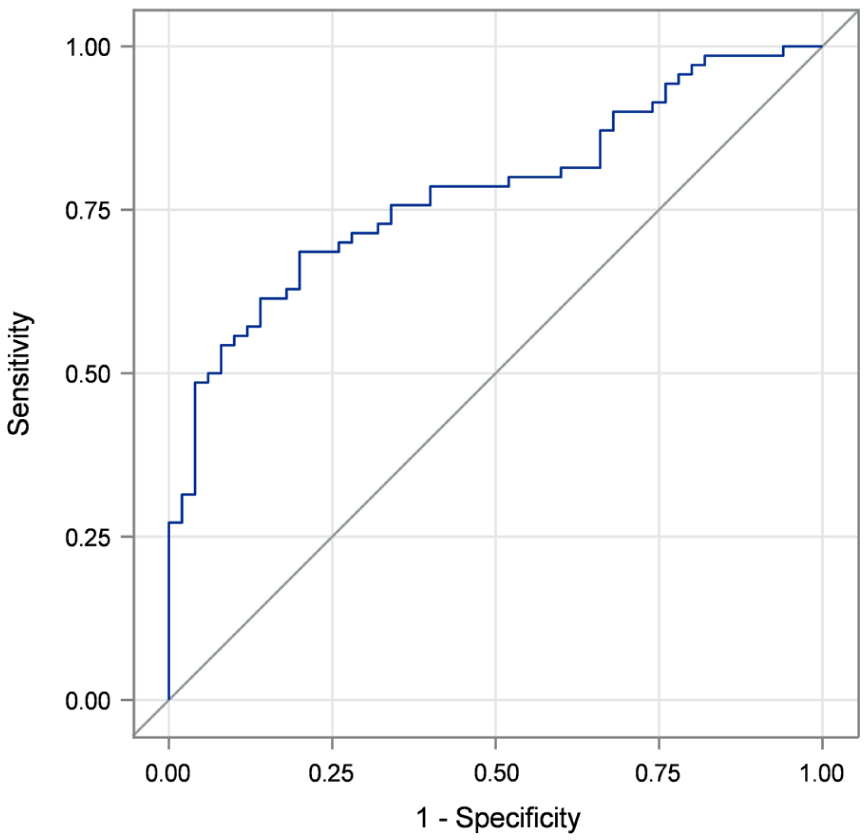
Receiver Operating Characteristic Curve for Classification Between SCI (Subjective Cognitive Impairment) and Healthy Controls Based on Turn Duration during TUGdt-MB (C-Statistics = 0.778) and Covariates Age, Gender, and Education.
Standardized Odds Ratios a for Association Between TUG/TUGdt Parameters and Dementia Versus MCI, MCI Versus SCI, and SCI Versus Controls.
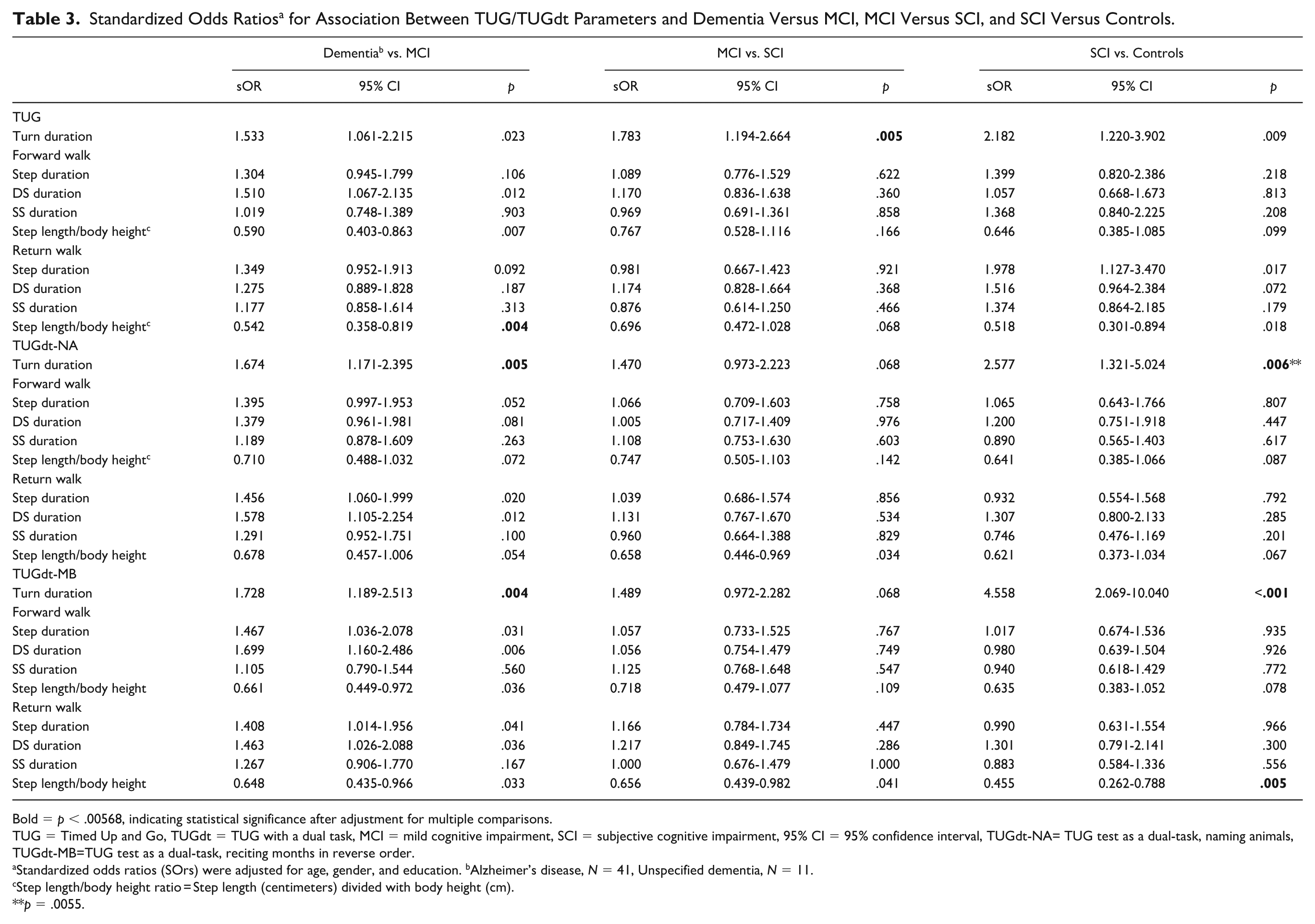
Bold = p < .00568, indicating statistical significance after adjustment for multiple comparisons.
TUG = Timed Up and Go, TUGdt = TUG with a dual task, MCI = mild cognitive impairment, SCI = subjective cognitive impairment, 95% CI = 95% confidence interval, TUGdt-NA= TUG test as a dual-task, naming animals, TUGdt-MB=TUG test as a dual-task, reciting months in reverse order.
Standardized odds ratios (SOrs) were adjusted for age, gender, and education. bAlzheimer’s disease, N = 41, Unspecified dementia, N = 11.
Step length/body height ratio = Step length (centimeters) divided with body height (cm).
p = .0055.
Turn duration segment
During TUG, the median time for turn duration in the different groups was: controls: 3.3 seconds; SCI: 3.4 seconds; MCI: 3.9 seconds; and dementia: 4.5 seconds. As presented in Table 3 and Figure 1, sORs were high between all adjacent groups (sOR = ≥1.53, 95% CI = [≥1.06, ≤3.90]). However, the Šidák correction revealed a significant difference to occur only between MCI and SCI (sOR = 1.783, 95% CI = [1.194, 2.664], p = .005).
For both TUGdt conditions, significant differences occurred between individuals with dementia and MCI (sOR = ≥1.67, 95% CI = [≥1.17, ≤2.51], p ≤ .005) and SCI and controls (sOR = ≥2.58, 95% CI = [≥1.32, ≤10.04], p ≤ .006), whereas the differences between individuals with MCI and SCI were non-significant (sOR = ≥1.47, 95% CI = [≥0.97, ≤2.28], p =.068). As illustrated in Figure 2, during TUGdt-MB, the variability of turn duration results increased with the severity of cognitive impairment. Notably, the highest sOR (4.56, 95% CI = [2.07, 10.04], p ˂ .001) between adjacent groups occurred between individuals with SCI and controls. This result was further analyzed with ROC curves, where the results supported the test’s ability to distinguish between the groups (C-statistics= 0.778) (see Figure 3).
Forward and Return Walk Segments
For step parameters during the forward walk segment, the largest sOR (1.70; 95% CI = [1.16, 2.49]) occurred for the step parameter DS duration during the TUGdt-MB condition between the dementia and MCI groups. However, no step parameter significantly discriminated between adjacent groups (p ≥ .006).
During the return walk segment, the results for the TUG condition showed that individuals with dementia walked with a significantly shorter step length/body height ratio compared with individuals with MCI (sOR = 0.54, 95% CI = [0.36, 0.82], p =.004). A similar finding occurred during TUGdt-MB, where individuals with SCI walked with significantly shorter step length/body height than controls (sOR = 0.46, 95% CI = [0.26, 0.79], p = .005).
Discussion
This is the first study to explore if the performance of turn duration and specific step parameters during different segments of TUG and TUGdt can discriminate between individuals with different levels of cognitive ability. Although preliminary due to the exploratory nature of this study, the results may suggest that the duration of the turn has the potential to discriminate between adjacent groups during TUG conditions and indicate longer turn times among individuals with lower levels of cognitive ability. In particular, the results show a similar trend during both TUGdt conditions, with generally high SORs (1.7–4.6) where the only non-significant differences occurred between individuals with MCI and SCI. For the forward walk segment (prior to the 180-degree turn), no step parameters discriminated significantly between adjacent groups during any TUG condition. In contrast, during the return walk segment, a tendency occurred for the step length/body height parameter.
In recent years, increased research interest has been directed toward exploring if the performance of specific segments of TUG may reveal subtle but important information of clinical relevance. Due to the multifaceted characteristics of TUG, this test increases demands on different cognitive and functional domains as the different TUG segments occur (Sunderaraman et al., 2019). Particularly turning, primarily due to its association with falling and physical disability (Leach et al., 2018), has long been an area of concern in numerous populations. In recent years, an association between turning and cognition has also become apparent. Indeed, turning is a complex motor sequence, requiring a subset of motor skills and is associated with executive functioning, processing speed, and visuo-spatial processing (Mirelman et al., 2014; Sunderaraman et al., 2019). While turning has most commonly been investigated as an isolated task, during TUG the turning sequence is embedded in a complex mobility task. As turning in everyday life tends to be conducted in direct relation to other movement sequences, the possibility of assessing turning during TUG increases the ecological validity of this outcome. This may support the importance of our findings that turn duration significantly discriminated between adjacent groups during all TUG conditions, and most evidently during the TUGdt conditions. Interestingly and somewhat surprising, across all TUG conditions, the highest sOR between adjacent groups occurred for turn duration between individuals with SCI and controls during TUGdt-MB. This result was also further supported by the result of ROC analyses. Although speculative, this result may be related to varying task prioritization (Yogev-Seligmann et al., 2012) in the different groups during turning, possible somatization in the SCI group (i.e., overly cautious turning), or may be due to chance. Therefore, the robustness needs to be confirmed by future studies. Nevertheless, this result may suggest the potential of turn duration to detect subtle changes in cognitive ability and may therefore be an important outcome for the early detection of cognitive impairment.
Previous studies have investigated walking segments of TUG with regard to completion times but not specific step parameters. In addition, the forward walk and return walk segments have been found to discriminate between individuals with different functional capabilities (Dibilio et al., 2017). However, it has not been investigated if the performance of these segments can discriminate between groups of individuals with different cognitive functions. Although the results of step parameters during the forward walk segment in our study did not exhibit any discriminatory potential, during the return walk segment, we found tendencies that the parameter step length/body height may entail discriminatory capacity. These results may be argued to align with previous findings, where tendencies of discrepancies have been found between the forward walk and return walk segments (Y. Cedervall, Stenberg, et al., 2020; Ishikawa et al., 2019). In addition, it has previously been found that reduced step length/body height may identify individuals with subtle levels of cognitive impairment during the full TUG and TUGdt (Löfgren et al., 2025). Although somewhat speculative, since cognitive fatigue has been found to affect the gait pattern during dual-task conditions (Behrens et al., 2018), the finding that individuals with SCI walked with significantly shorter step length than controls during TUGdt-MB may indicate that they experienced some extent of cognitive fatigue during the return walk segment. Indeed, as TUG is a complex mobility task that includes the resource-demanding 180-degree turn, the prolonged performance of a simultaneous cognitive task that requires continuous activation in cortical areas may therefore challenge cognitive robustness during the latter part of this mobility sequence. Since more research on this topic is needed, future studies should be designed to specifically investigate if step length/body height during cognitively demanding conditions can detect subtle impairment of cognitive function.
This study has several limitations. The investigation of step parameters and turn duration during the segmented TUG during three conditions inevitably resulted in multiple analyses, which increases the risk of type I error. However, in exploratory research, where Type II error is generally considered a larger problem, it has been advised against correcting for multiple analyses (Bender & Lange, 2001; Ranstam, 2019). To balance this, we estimated the number of effective independent tests (Meff) using the method of Li and Ji (2005) with the Šidák correction to determine the adjusted significance threshold. In addition, these analyses were corrected for age, gender, and education. However, education was a dichotomous variable, which weakens its predictive validity. Therefore, future studies should strive to include education as a continuous variable to minimize the risk of residual confounding. Regarding assessments, the inclusion of a higher number of steps would have been preferable due to the largely variable nature of step parameters, not least during TUGdt conditions. However, the UDDGait project was designed to enable implementation into clinical practice. Accordingly, the inclusion of patients with dementia, MCI, and SCI was conducted in close collaboration with specialist memory clinics, where individuals undergoing memory assessment were included, thus increasing the study’s ecological validity. With this in mind, the sample size was comparable to similar studies (McArdle et al., 2017; Montero-Odasso et al., 2017). In addition, the assessments entailed performing TUG and each TUGdt condition once, and without a practice session—the latter of which was originally recommended (Podsiadlo & Richardson, 1991). This differs from the majority of studies included in a recent scoping review (Bottinger et al., 2024) on studies investigating TUG segments. However, since the recruitment procedure was conducted in clinical practice, whereby time efficiency and minimized patient burden are crucial factors (Wang et al., 2023), some trade-offs may be inevitable. Indeed, clinical research has been criticized for commonly excluding potential participants with higher degrees of disability (DeCormier Plosky, 2022). Nevertheless, the exploratory nature of this study, motivated by the urgent need of detecting risk of cognitive decline at the earliest possible stages, emphasizes that these results should be interpreted with caution and confirmed by future research. In addition, to facilitate implementation into clinical practice, future research needs to focus on developing user-friendly and valid technical solutions to capture potentially important outcomes of the segmental TUG and TUGdt.
Conclusion
This was the first study to explore if the performance of turn duration and specific step parameters during different segments of TUG can discriminate between individuals with different levels of cognitive ability. The results indicate that longer turning duration occurred for groups of individuals with lower levels of cognitive ability, particularly during TUGdt conditions. This finding may be particularly important, as turning during TUG is clinically relevant, and embedded in a mobility sequence, it assimilates activities of everyday life. In addition, step length/body height also showed a small tendency of discriminatory capacity during the return walk segment. Although these results need to be confirmed by future research, they may highlight the potential of assessing turning and the return walk segment of TUG, particularly under TUGdt conditions, to enable early identification of individuals at risk of cognitive impairment.
Supplemental Material
sj-docx-1-asm-10.1177_10731911251410337 – Supplemental material for Can Turn Duration and Step Parameters During the Timed Up and Go Test With and Without a Dual-Task Discriminate Between Individuals With Different Cognitive Abilities? An Explorative Study
Supplemental material, sj-docx-1-asm-10.1177_10731911251410337 for Can Turn Duration and Step Parameters During the Timed Up and Go Test With and Without a Dual-Task Discriminate Between Individuals With Different Cognitive Abilities? An Explorative Study by Niklas Löfgren, Lars Berglund, Vilmantas Giedraitis, Erik Rosendahl and Anna Cristina Åberg in Assessment
Footnotes
Acknowledgements
We thank all participants for contributing to this research.
Author Contributions
NL: conceptualization and main responsibility of writing the original draft.
LB: conceptualization and responsible for data analyses.
VG: data preparation
ER: critical review of the manuscript.
ACÅ: conceptualization, methodology, data collection, writing parts of original draft, project administration, and funding acquisition.
All authors participated in data interpretation and manuscript preparation.
Data Availability Statement
The material analyzed during the current study is not publicly available due to its content of sensitive personal data. Datasets generated can be available from the principal investigator, ACÅ, on reasonable request, after ethical considerations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open access funding was provided by Dalarna University. This work was supported by grants from the Swedish Research Council (2017-1259 and 2020-01056), the Promobilia Foundation, the Dementia Foundation, Sweden, and Konung Gustaf V:s och Drottning Victorias frimurarestiftelse. The funding bodies had no role in the design, methods, data collection, analysis, or preparation of the manuscript.
Ethical Considerations
The Regional Ethical Review Board in Uppsala and the Swedish Ethical Review Authority approved this study.
Consent to Participate
Written and verbal informed consent to participate in this study was obtained from all participants prior to study commencement.
Consent for Publication
This study does not entail data on the individual level.
Supplemental Material
Supplemental material for this article is available online.