
Abstract
The current review describes updated information on the evidence-based assessment of substance use disorder. We offer an overview of the state of the science for substance-related assessment targets, instruments (screening, diagnosis, outcome and treatment monitoring, and psychosocial functioning and wellbeing) and processes (relational and technical) as well as recommendations for each of these three components. We encourage assessors to reflect on their own biases, beliefs, and values, including how those relate to people that use substances, and to view the individual as a whole person. It is important to consider a person’s profile of symptoms and functioning inclusive of strengths, comorbidities, and social and cultural determinants. Collaborating with the patient to select the assessment target that best fits their goals and integration of assessment information in a holistic manner is critical. We conclude by providing recommendations for assessment targets, instruments, and processes as well as recommendations for comprehensive substance use disorder assessment, and describe future directions for research.
What Is Evidence-Based Assessment and Why Does It Matter?
Evidence-based assessment describes an integrated approach that emphasizes the use of research and theory to inform the selection of assessment targets, the methods and measures used to assess such targets, and assessment processes (Hunsley & Mash, 2007). Although sometimes narrowly described as selecting psychometrically sound assessment instruments, evidence-based assessment is much more. More accurately, evidence-based assessment is an approach that recognizes the inherent complexity of assessment, which is itself a decision-making process, and highlights the importance of integrating information across data sources in service of the best clinical outcomes for a given person (Hunsley & Mash, 2007). The current review provides up-to-date information on evidence-based assessment for substance use disorder (SUD). We describe the evidence for the selection of treatment targets, methods and measures to assess such targets, and specific procedures and considerations that clinicians and researchers should follow to integrate information during the evidence-based assessment of SUD. We conclude with a discussion of overall recommendations and future directions.
What Is SUD?
SUD is a heterogeneous condition characterized by the recurrent use of one or more substances that results in harm, distress, or impairment. Heavy and prolonged substance use is associated with a range of consequences, including physical (e.g., death, injury, infection), psychological (e.g., exacerbation of other mental health symptoms), social (e.g., family stress), and economic (e.g., unemployment or underemployment) problems (American Psychiatric Association, 2013; Compton et al., 2007; Schulte & Hser, 2013; Substance Abuse and Mental Health Services Administration, 2013). To reduce and address substance-related risk and impairment, it is imperative to identify evidence-based tools and practices for assessing SUD, especially given the importance of assessment in treatment planning and delivery. Critically, SUD is associated with numerous social determinants, so a multifaceted approach that also considers socioecological factors that are associated with substance use-related problems, such as housing, food insecurity, the criminal legal system, and health inequity is imperative.
Diagnostic Criteria
The predominant diagnostic system in the United States is the Diagnostic and Statistical Manual of Mental Disorders which is currently in its fifth edition (DSM-5; American Psychiatric Association, 2013) and recently underwent a text revision (Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association, 2022). Notably, no significant changes to the SUD diagnoses were made in the text revision (First et al., 2022). The DSM-5 (American Psychiatric Association, 2013) SUD diagnosis includes 10 different drug classes including alcohol, cannabis, caffeine, hallucinogens, inhalants, opioids, stimulants, sedatives, hypnotics, or anxiolytics; tobacco; and other or unknown substances. According to the 2018 U.S.-based National Survey on Drug Use and Health, approximately 1.6% of individuals aged 12 to 17 and 10.1% of individuals aged 18 or older had any DSM-5 SUD in the past year (Substance Abuseand Mental Health Services Administration, 2019).
The DSM-5 outlines 11 specific criteria for SUD that are thought to cover the domains of impaired control, social impairment, risky use, and pharmacological criteria (American Psychiatric Association, 2013). 1 These criteria include: (1) using substances in larger amounts or over a longer period than intended, (2) persistent desire or unsuccessful efforts to quit or cut down on use, (3) spending a significant amount of time obtaining, using, or recovering from substance use, (4) craving or a strong desire to use, (5) a failure to fulfill major role obligations at work, school, or home due to use, (6) continued use despite persistent or recurrent social or interpersonal problems, (7) giving up important social, occupational, or recreational activities because of use, (8) recurrent use in physically hazardous situations, (9) continued use despite having a persistent or recurrent physical or psychological problem caused or exacerbated by use, (10) tolerance, and (11) withdrawal. A SUD diagnosis requires endorsing two or more criteria in the past 12 months. Severity is indicated by the number of criteria endorsed such that endorsing two to three criteria indicates a mild SUD, four to five indicates a moderate SUD, and six or more indicates severe SUD.
Etiology
Due to the various limitations of DSM SUD conceptualization and diagnosis (see Boness et al., 2021, for an overview) including a lack of attention to etiology, there have been calls to shift conceptualizations of SUD away from the traditional clinical-description approach historically taken by the DSM and toward etiologically based mechanisms instead. Recent conceptualizations of SUD, such as the Alcohol and Addiction Research Domain Criteria (AARDoC) and its assessment battery, the Addictions Neuroclinical Assessment (ANA; Kwako et al., 2016, 2017), are compatible with this broad goal. AARDoC is the first addiction-specific mechanistic framework that synthesizes research on its behavioral, neurobiological, and genetic features and integrates them into three higher-order mechanistic domains: reward/incentive salience, negative emotionality, and cognitive control/executive function (Kwako et al., 2016; Litten et al., 2015). There are similar efforts underway to develop a National Institute on Drug Abuse Phenotyping Assessment Battery (PhAB) focused on neurofunctional domains of metacognition, interoception, executive function, incentive salience, negative emotionality, and sleep (Keyser-Marcus et al., 2021) as well as efforts to develop an alcohol use disorder specific mechanistic framework (i.e., the Etiologic, Theory-based, Ontogenetic Hierarchical [ETOH] Framework of Alcohol Use Disorder; Boness et al., 2021). These initiatives have the common goals of formulating more comprehensive risk profiles across individuals to support precision medicine and improve SUD treatment outcomes, but these initiatives are also in their infancy and currently lack well-validated assessment batteries, particularly patient-reported outcome measures. It is important to emphasize that current DSM criteria are largely separate from etiologic and maintenance mechanisms implicated in SUD, and thus, it is important to understand both to inform evidence-based assessment practices.
SUD etiology is characterized by significant complexity and heterogeneity, and, as such, there exists a rich history of etiologic models that implicate various genetic, biological, psychosocial, and environmental mechanisms (Kendler, 2012). Although the Etiologic, Theory-based, Ontogenetic Hierarchical Framework (Boness et al., 2021) requires validation of its hierarchical and organizational structure, the identification of its core etiologic and maintenance mechanisms was based on a systematic integration of the alcohol use disorder etiology literature. This is in comparison to the Addictions Neuroclinical Assessment, which was developed primarily based on a single etiologic model, the addiction cycle (Koob & Moal, 1997), and Phenotyping Assessment Battery which was developed using the Delphi method and is still in the earlier stages of operationalization (and thus not discussed here further). Although the Etiologic, Theory-based, Ontogenetic Hierarchical Framework was primarily derived from literature on alcohol use disorder, the broad mechanistic domains are likely relevant across substances. Thus, in describing SUD etiology in the following section, we use the Etiologic, Theory-based, Ontogenetic Hierarchical (ETOH) Framework as a guide. We emphasize the Etiologic, Theory-based, Ontogenetic Hierarchical Framework’s overlap with the slightly narrower Addictions Neuroclinical Assessment domains (incentive salience, negative emotionality, and executive function) which now have a growing body of empirical support but may overlook other relevant etiologic mechanisms due to its focus on a single acquired theory of addiction etiology. Taken together, these models suggest the main etiologic domains of relevance to SUD include reward, cognitive control, and negative valence/emotionality as well as environmental factors.
The reward domain describes those etiologic and maintenance mechanisms that are implicated in the transformation of otherwise neutral stimuli or events (e.g., cues) into attractive and wanted stimuli. Reward-related mechanisms implicated in SUD include positive expectancies, reward sensitivity, positive emotionality, incentive salience, reward discounting, and habit (Boness et al., 2021; Kwako et al., 2016). The domain of cognitive control includes mechanisms related to executive functioning and the organization of behavior toward future goals. Cognitive control–related mechanisms include compulsive use, conscientiousness (which includes elements of impulsivity), and response inhibition (Boness et al., 2021; Kwako et al., 2016). The negative valence/emotionality domain includes mechanisms related to both negative emotionality and other negative effects such as physical pain or those resulting from substance use. Negative valence/emotionality mechanisms include punishment sensitivity, coping, negative emotionality, and negative expectancies (Boness et al., 2022; Kwako et al., 2016). Although not consistently included in modern conceptualizations, social and environmental factors, such as racism-related stress (Jordan et al., 2020) and family functioning (Meisel et al., 2022), are also relevant to SUD etiology. However, it remains unclear whether these social and environmental factors are truly mechanisms or whether they might be better described as risk factors or moderators (Boness et al., 2021). That is, social and environmental factors may make someone more vulnerable to developing or maintaining a SUD but may not be core etiological mechanisms. Still, we argue that social and environmental factors are critical to address in the assessment and treatment of SUD.
Developmental Course
There is considerable variability in the developmental life course of SUD across several variables (e.g., age of onset, desistance or aging out, comorbidities, distal outcomes, or consequences). Many substance use trajectories follow an age-prevalence gradient such that use and disorder increase during adolescence, peak between ages 18 and 22, and begin to decrease in prevalence in young adulthood. These reductions tend to continue in later developmental periods over the adult lifespan (Lee et al., 2019). Although these general trends are consistent across various substances, heterogeneity exists by type of SUD (e.g., nicotine disorder has a more stable prevalence rate over the life course compared to other substances; Johnston et al., 2016; Lee et al., 2019) as well as by other contextual and demographic variables (e.g., mortality rates of certain SUDs may impact their developmental life course; Lee et al., 2019).
Lee et al. (2019) highlight three primary pathways to SUD including (a) the deviance proneness pathway, in which individuals with higher levels of impulsivity are more prone to engage in risky behavior including substance use, (b) the stress/negative affect pathway, where individuals who are exposed to early stress or trauma, may cope with negative emotions resulting from these events by using substances, and (c) the pharmacological effects pathway, where individual differences in one’s sensitivity to stimulating or sedating effects of various substances put some people at more risk for addiction and continued use than others. 2 In addition to these pathways, as many as seven developmental trajectories or classes have been identified in the literature and vary depending on the context, substance, and developmental age range (e.g., high users, steady increasers, desisters, adolescent limited users, low/moderate users, late onset, and non-users; Yamada et al., 2016). Common contextual factors that are associated with the risk of developing SUD include early onset of first use (Lee et al., 2010), association with peers who use substances (Connell et al., 2006; Yamada et al., 2016), and family history of substance use (Kirisci et al., 2007). Primary racial/ethnic differences in substance use and disorder include the “crossover effect” in which, relative to their white counterparts, people with minoritized racial and ethnic identities have lower rates of substance use until a certain age or developmental stage (e.g., adolescence or early adulthood) when they are then at higher risk of SUD (Banks & Zapolski, 2018). Furthermore, a growing body of literature has identified that despite lower rates of substance use during certain ages, people with minoritized racial and ethnic backgrounds experience more drinking-related problems (e.g., physical and chronic health conditions, legal problems, dependence symptoms, and comorbidities; Chartier & Caetano, 2010; Hautala et al., 2019; Mulia et al., 2009; Zapolski et al., 2014) than White individuals.
The concept of natural recovery and aging out is important to note. Commonly cited protective factors that are associated with less substance use and disorder include positive parental influence, often defined by a combination of household guidelines and positive parental relationships (Arria et al., 2008; Lippold et al., 2014), prosocial adolescent social supports and relationships (Barnes et al., 2009), and positive bonds to community and school (Barnes et al., 2007). For an extensive review of risk and protective factors see Stone and colleagues (2012). Various pathways to desistance have been identified including maturing personality and role development leading to lower levels of use (Lee, Chassin, & MacKinnon, 2015; Lee, Ellingson, & Sher, 2015), and natural recovery, which is characterized by intentional evaluation of substance use, self-identification of problematic use, and active efforts to change substance use behavior (Sobell et al., 2000). Taken together these risk and protective factors offer insight into how individual and contextual factors might intersect to impact the developmental course of their substance use.
Comorbidity
Extensive diagnostic comorbidity is a well-documented limitation of the DSM diagnostic model (see Krueger et al., 2014; Widiger & Trull, 2007 for reviews). SUDs are observed to be highly comorbid with each other as well as with several other psychiatric symptoms and disorders (e.g., Glass et al., 2014; Sher & Trull, 2002). SUD is most commonly comorbid with externalizing disorders (e.g., Krueger et al., 2009; Slutske et al., 2002), personality psychopathology (e.g., antisocial personality disorder, borderline personality disorder; Fenton et al., 2012; Helle et al., 2020), and internalizing disorders (Kessler et al., 2005; Tully & Iacono, 2016).
The high rate of comorbidity is attributable to several factors, each of which should be considered in the assessment process. Methodological artifacts, due to the use of polythetic criterion sets and shared symptoms, contribute to the observed diagnostic comorbidity. In addition, shared etiology (e.g., childhood trauma), traits, and other transdiagnostic components (e.g., emotion dysregulation, disinhibition, negative emotionality, reward sensitivity; Boness et al., 2021; Kotov et al., 2017) result in high rates of diagnostic comorbidity between SUD and other psychiatric disorders. For instance, Trull and colleagues (2018) found that across mental health settings, comorbidity rates between current diagnoses of SUD and borderline personality disorder ranged from 10% to 72.7% (lifetime rates ranging from 45.5% to 86.2%; the highest rates found for opioid, cocaine, and alcohol use disorders and borderline personality disorder). They attributed this overlap to be, in part, due to shared domains of emotion dysregulation and impulsivity. Clinical symptoms and disorders can also mutually influence each other (e.g., impulsivity during a manic episode could increase the risk for recurrent problematic use of a substance), and thus, an individual may meet diagnostic criteria for several disorders even if primarily driven by mania. Alcohol and substance use may similarly be driven by specific mechanisms (e.g., negative emotionality). In this case, a careful evidence-based assessment may reveal that treating the preexisting psychiatric disorder may indirectly result in reduced substance use (Schuckit, 2006). Acute symptoms of substance intoxication (e.g., substance-induced psychosis) or withdrawal (e.g., depressive or anxiety symptoms) are similarly important, as these symptoms may portray additional psychiatric features which may diminish as the acute symptoms pass; therefore, it is important to first determine whether intoxication or withdrawal symptoms are present.
As illustrated, considering the reason for comorbidity is important as it will likely influence the course of treatment. To parse sources of comorbidity, clinicians and researchers are encouraged to use dimensional, evidence-based models of psychopathology (e.g., Hierarchical Taxonomy of Psychopathology [HiTOP]; Kotov et al., 2017) and other models that focus on etiologic and maintenance mechanisms of use (e.g., Addictions Neuroclinical Assessment; Etiologic, Theory-based, Ontogenetic Hierarchical Framework). This shift in focus could capture what is currently considered “subthreshold” symptoms sooner in the development of a SUD as well as prioritize more specific information about a person’s SUD above and beyond physiological adaptations and psychosocial consequences (Boness et al., 2021; Watts et al., 2023). Such a shift could, in turn, reveal meaningful places for clinical intervention that may be overlooked by DSM-bound assessment approaches.
Components of Evidence-Based Assessment for SUD
Evidence-based assessment requires the use of research and theory to inform the selection of assessment targets, the methods and measures used to assess such targets, and assessment processes (Hunsley & Mash, 2007). In the sections that follow, we describe each of these three components in detail as they correspond to SUD. There is already a vast literature on SUD assessment instruments, yet there is little to no guidance on selecting assessment targets or assessment processes in the SUD literature. Thus, we rely on the larger literature and our clinical expertise in making recommendations for these sections.
Assessment Targets
The identification of SUD-related assessment targets and the selection of a corresponding assessment tool to assess the given target(s) is largely dependent upon the goal of the assessment. That is, is the goal of the assessment to include or exclude participants from a research study, identify the presence or absence of a substance use disorder, understand a person’s unique profile of symptoms, facilitate referral, assist in case conceptualization and/or treatment planning, monitor treatment response and outcomes, predict future behavior, and/or aid in more comprehensive evaluations of fitness, disability, or educational placement, for example. Clarifying the assessment goal is the first step in determining appropriate assessment targets.
The goal of the assessment may also depend upon the setting in which it is taking place. For example, in a primary care setting, the immediate goal may be the assessment of risky patterns of consumption and substance-related harm to determine if there is a need for treatment referral. In an emergency room, the goal of the assessment may be to determine overdose potential, differential diagnosis based on symptom presentation, and withdrawal-related risk. In a comprehensive assessment clinic, the goal may be to determine a person’s unique profile of use and impairment to facilitate their entry into a specific treatment program. It is important to jointly consider the assessment goal within the specific context or setting the assessment is taking place.
Decisions about assessment goal(s) should not be determined solely by the clinician or researcher without input from the client or community of interest. We recommend a parallel process that collaboratively considers the goals of the assessor alongside those of the target individual or group. For example, what does a given individual view as the reason for an assessment and what do they hope to achieve as a result of the assessment? Does this person want to improve their psychosocial functioning? Reduce or eliminate their substance use? Enter diagnostic “remission” from SUD? Does this match the goals of the assessor? Why or why not? How might the final goal reflect these considerations? Although collaborative goal setting may seem to be a more common approach in clinical encounters, particularly during rapport-building processes and treatment planning, we argue that there is a precedent for this approach in assessment and research as well. Indeed, community-driven and community-based participatory research hold at their core collaborative and patient-centered methods that engage community members throughout the research process. This includes involving community members in the determination of research goals, selection of inclusion and exclusion criteria, selection of appropriate assessment approaches, and other components of the research process (Collins et al., 2018; Wallerstein & Duran, 2006). As such, the derivation of assessment goals and the corresponding selection of assessment targets might be best achieved using collaborative approaches. There are also challenges to implementing collaborative assessment approaches, such as organizational requirements and protocols or reimbursement structures which can greatly complicate this portion of the evidence-based assessment (e.g., cases where a patient-preferred target is not sufficient for obtaining reimbursement of services).
Although we do not intend to offer prescriptive guidance about assessment targets that may be relevant in SUD because targets are highly dependent upon the assessment goal, we do highlight several for consideration. These include, for example, frequency, quantity, and duration of use, SUD symptoms, substance-related harm or consequences, psychosocial functioning, and quality of life and wellbeing.
Assessment Instruments
In this section, we provide an overview of evidence-based assessment instruments for SUD separately for adults and adolescents. However, it is first important to note that many of these instruments were based on the traditions of the DSM and the field’s conceptualizations of SUD, more generally. This is partially due to the lack of validated measures available for assessing modern conceptualizations of SUD, such as the Addictions Neuroclinical Assessment and Etiologic, Theory-based, Ontogenetic, Hierarchical Framework. As a result, many instruments focus primarily on physiologic adaptations, including tolerance and withdrawal, and psychosocial consequences, such as a failure to fulfill role obligations, which may neglect other important mechanisms and social and environmental determinants implicated in SUDs (Boness et al., 2021). Focusing on psychosocial consequences in SUD assessment is a particular challenge because consequences may not be unique to SUD (i.e., they may be multiply determined), are contextually and culturally bound, tend to exhibit only modest associations with substance use, and may introduce systematic bias in diagnosis (Boness et al., 2021; Caetano, 2011; Martin et al., 2014; Zapolski et al., 2014). Provider-level factors, such as stigmatizing attitudes and biases toward people who use substances, may similarly result in the misdiagnosis of SUD, especially for marginalized groups, which may contribute to suboptimal quality of care and treatment outcomes (Jordan et al., 2020; Shim, 2021; van Boekel et al., 2013). Thus, when considering the selection of assessment instruments, it is imperative to understand the traditions of a given instrument, what it is intended to assess, and how it may be vulnerable to bias and/or limited in capturing all information relevant to a comprehensive SUD diagnosis.
Consideration of the psychometric properties of instruments is also an imperative component of evidence-based assessment. Psychometric properties are conditional and thus should always be considered in light of the target sample (e.g., age, gender identity, racial and ethnic identity) and intended assessment purpose (e.g., screening, diagnosis, case conceptualization). Psychometric properties are dependent upon the administration of a particular instrument (i.e., psychometrics are not inherent properties of a measure, but are dependent on conditions during the administration of a particular assessment instrument). Common properties to consider in the selection of assessment instruments include reliability (e.g., internal consistency, interrater reliability, test–retest reliability), validity (e.g., concurrent validity, construct validity, content validity, convergent validity, criterion-related validity, discriminant validity, discriminative validity, incremental validity, face validity, predictive validity, sensitivity and specificity, support for factor or subscale structure, measurement invariance, treatment sensitivity), and clinical utility (i.e., whether the assessment results in improved accuracy, outcomes, or efficiency; Hunsley & Mash, 2007). 3 Evidence of psychometric replication is also important. Although the gold standard is to use instruments that have demonstrated strong psychometric properties across administrations and groups of individuals, it is important to acknowledge that relying solely on psychometric information in assessment selection may be limited. For example, there may be no validated assessment tools for SUD in certain populations (e.g., Deaf people, Indigenous people). In these cases, clinicians and researchers are often forced to use instruments validated in other groups or for other purposes or create/adapt mainstream instruments for their purpose, rendering psychometrics for that specific application of the instrument unknown and necessitating further empirical validation. Adjacent features are also worth considering, including feasibility and acceptability, cost-effectiveness, administration time and resources, and level of training required (Antony & Rowa, 2005). That is, acceptable psychometric properties are ideal but may not be available or sufficient. It is also the case that many assessment instruments that have been used for decades in the field and assumed to have good psychometric properties may not be valid when tested using more rigorous methods for evaluating psychometric properties (Kirouac & Witkiewitz, 2018). Although biological testing is sometimes used in the verification of substance use, self-report is the gold standard for AUD assessments. Thus, we do not review biological measures here but refer interested readers to Haeny and colleagues (2018), Dolan and colleagues (2004), and Hadland and Levy (2016). Despite self-report being the gold standard in SUD assessment, the validity of self-report is often called into question. However, research consistently shows high agreement between self-report and biological measures of substance use (Hjorthøj et al., 2012; Simons et al., 2015). In non-medical clinical and research settings, self-report also tends to be the most accepted by patients, efficient, and affordable. Thus, in the sections that follow, we briefly describe self-report instruments recommended for SUD screening, diagnosis, and treatment monitoring in adults and adolescents. In recommending instruments, we sought to balance psychometric properties 4 with other practical considerations such as ease of accessibility, flexibility and length of administration, and item wording. As such, an instrument with limited but acceptable psychometric information may have still been recommended due to its brevity, availability, and flexible administration format (e.g., Clinical Opiate Withdrawal Scale). We also briefly discuss other key aspects of comprehensive SUD assessment that may not be captured by instruments developed in the tradition of the DSM, including overall psychosocial functioning and wellbeing. Table 1 offers an overview of instruments included in subsequent sections, and Supplemental Table 1 provides detailed information on the advantages and disadvantages of each measure.
Overview of Recommended Substance Use Disorder Assessment Instruments
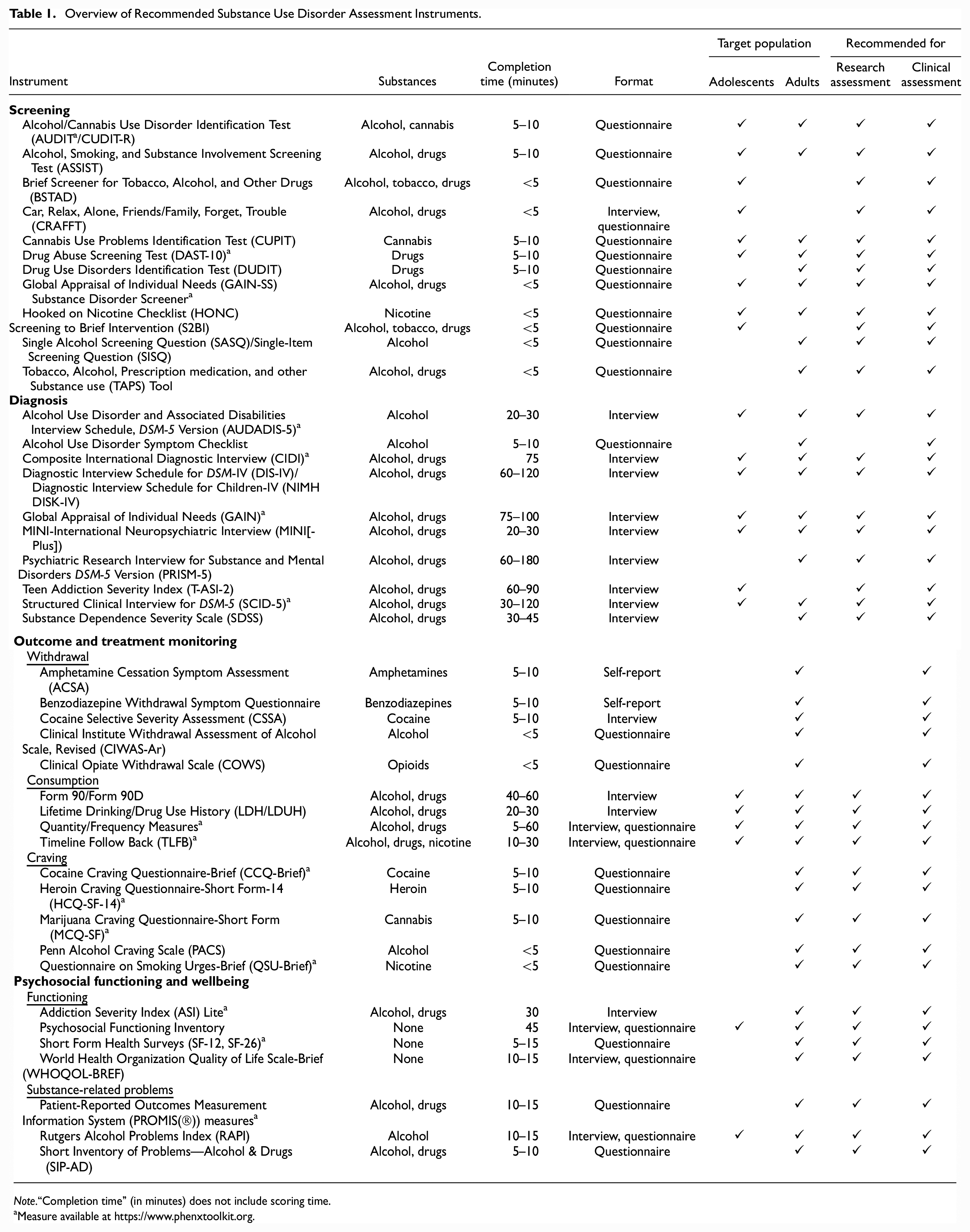
Note.“Completion time” (in minutes) does not include scoring time.
Measure available at https://www.phenxtoolkit.org.
Screening
Although the exact procedures may differ based on the type of setting, screening for SUD typically includes the use of a brief self-report or clinical interview to determine whether someone may be at risk for a SUD or have a probable SUD that warrants further assessment.
Adolescents
Screening tools for adolescent SUD are ideally balanced between efficiency for clinical settings and sensitivity in gathering relevant information to inform the next steps. Two screeners show strong evidence for use among adolescent populations. The Screening to Brief Intervention (S2BI) tool asks about the frequency of use for eight different substances over the past year and has demonstrated high sensitivity and specificity in discriminating among clinically significant risk levels in adolescent substance use (Levy & Williams, 2016). The Screening to Brief Intervention tool can be administered electronically and produces scores that are highly correlated with DSM-5 SUD (Levy et al., 2014; Levy & Shrier, 2015). Equally as efficient in terms of administration is the Brief Screener for Tobacco, Alcohol, and other Drugs (BSTAD; Kelly et al., 2014). The Hooked on Nicotine Checklist (HONC; DiFranza et al., 2002) was included in a recent evidence-based update as a useful screener for adolescent nicotine dependence 5 (Becker-Haimes et al., 2020). As highlighted in a recent research review by Gray and Squeglia (2018), these brief screeners are often paired with additional brief assessments to determine appropriate placement in the correct level of care based on the adolescent severity and specific substance-related problems. Tools used for this purpose include the Car, Relax, Alone, Friends/Family, Forget, Trouble (Knight et al., 1999; S. Levy & Shrier, 2015), and the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST; Gryczynski et al., 2015). Although originally developed for use with adults, the Alcohol Use Disorder Identification Test (AUDIT; Saunders et al., 1993) also has research support for the identification of risky alcohol use among adolescents (Knight et al., 2003). A parallel test was developed for cannabis use, the Cannabis Use Disorder Identification Test-Revised (CUDIT-R; Adamson et al., 2010). Despite this measure showing promise in younger samples (Schultz et al., 2019), a need for continued evaluation among adolescents exists. A similar screener specifically validated among an adolescent population for cannabis use is the Cannabis Use Problems Identification Test (CUPIT; Bashford et al., 2010), which is brief in nature, freely available, and measures both frequency and intensity of cannabis use.
Adults
A commonly used screener in research and clinical settings (e.g., primary care and inpatient settings) is the AUDIT (10 items; Saunders et al., 1993) and its derivative (AUDIT-C, 3 items; Bush et al., 1998). The full-length screener assesses alcohol consumption and alcohol-related problems, whereas the AUDIT-C strictly measures consumption. Both measures have a wealth of empirical support, are well-validated, and are recommended by the National Institute on Alcohol Abuse and Alcoholism; however, it is important to note that some work has found that the AUDIT may be less effective (i.e., low true-positive rate relative to the high false-positive rate) for identifying alcohol use disorder among women and individuals residing in countries with lower rates of alcohol use disorder (Lange et al., 2019). 6 As a companion to the Alcohol Use Disorders Identification Test, researchers developed the Drug Use Disorders Identification Test (DUDIT; Berman et al., 2003) to assess general substance use in clinical and research settings; however, some psychometric concerns have been raised with respect to this measure (e.g., it has yielded an inconsistent factor solution; Berman et al., 2005). The CUDIT-R (Adamson et al., 2010) 7 is an eight-item screen for problematic cannabis use, and it assesses consumption, problems associated with use, dependence, and psychological features. Initial work has supported its reliability and validity; however, there is sparse work examining its psychometric properties among diverse populations (e.g., clinical, community; Adamson et al., 2010). The National Institute on Alcohol Abuse and Alcoholism also recommends the use of the Single Alcohol Screening Question (“How many times in the past year have you had [4 for women, or 5 for men] or more drinks in a day?”), and the National Institute on Drug Abuse Clinical Trials Network recommends that Single Item Screening Question 8 for Drug Use (“How many times in the past year have you used an illegal drug or used a prescription medication for non-medical reasons (for example, because of the experience or feeling it caused)?”) which can both easily be included in brief clinical interviews. Other validated, freely available SUD screeners include the ASSIST (WHO ASSIST Working Group, 2002), 9 the Drug Abuse Screening Test (DAST-10; Skinner, 1982), Global Appraisal of Individual Needs-Short Screener (GAIN-SS; Dennis et al., 2008), and the Tobacco, Alcohol, Prescription medication, and other Substance use (TAPS; Wu et al., 2016).10,11 Of note, the TAPS tool consists of a screening component (TAPS-1) and a secondary brief assessment (TAPS-2) for individuals who screen positive.
Categorical Diagnosis
A formal diagnosis of SUD is important for both treatment and research purposes, and assigning a categorical SUD diagnosis is typically the norm. Diagnostic labels offered by the DSM are useful because they provide a common nomenclature for clinicians (e.g., for treatment planning), researchers (e.g., for predicting related outcomes), and policyholders (e.g., insurance reimbursement, disability determinations; Hyman, 2010). Although categorical SUD diagnoses are limited in many ways (Boness et al., 2021; Hyman, 2010; Widiger & Samuel, 2005), their ability to be assessed reliably with structured and semi-structured clinical interviews is often appealing to clinicians and researchers.
In the sections that follow, we provide recommendations for categorical SUD diagnostic tools. Although we ultimately advocate for dimensional, rather than purely categorical, SUD diagnoses, categorical diagnoses can easily be combined with other assessments described later. If it is not feasible to combine assessments (e.g., due to time), evaluating individual symptom profiles can provide additional information. For example, SUD criteria are presumed to count equally toward a SUD diagnosis, but this assumption does not hold up empirically, and individual symptoms may provide additional information not offered by the overall diagnosis (Boness et al., 2019). Furthermore, there may be distinct clusters of SUD symptoms that offer important information beyond an overall diagnosis and can be used during case conceptualization and treatment planning (Watts et al., 2021, 2023).
Adolescents
Numerous well-validated diagnostic interviews for SUD exist, and currently, there is no consensus as to which is best suited for the evidence-based assessment of SUD. Although originally developed for epidemiological purposes, the National Institute of Mental Health Diagnostic Interview Schedule for Children-IV (Shaffer et al., 2000) is appropriate for use in clinical research as well as service settings and includes modules for more than 30 psychiatric diagnoses. The Alcohol Use Disorder and Associated Disabilities Interview Schedule, DSM-5 Version 12 (AUDADIS-5; Grant et al., 2015) and the Composite International Diagnostic Interview (CIDI; Kessler & Üstün, 2004; Merikangas et al., 2009; Robins et al., 1988) are also commonly used in adolescent research studies attempting to estimate prevalence rates of SUD. Notably, each of these diagnostic tools has dedicated questions for a parent/caregiver informant to provide additional collateral information when making a SUD diagnosis. Other interviews appropriate for assessing adolescent SUD include the Mini-International Neuropsychiatric Interview for Children and Adolescents (Sheehan et al., 2010) as well as the Structured Clinical Interview for DSM-5 (SCID; First et al., 2016). In addition, a review of SUD screening and comprehensive measures (Winters & Kaminer, 2008) highlighted the Global Appraisal of Individual Needs (GAIN; Dennis et al., 2003), and the Teen Addiction Severity Index (T-ASI-2; Brodey et al., 2005) as having adequate psychometric properties for the purpose of diagnosis. While an abbreviated version of the GAIN is available as a screener (GAIN-SS), the full GAIN involves a semi-structured interview that measures biopsychosocial functioning over the life course for various subscales including substance use, problems, and internalizing/externalizing symptoms, making it relatively comprehensive. The T-ASI is an additional semi-structured interview that covers seven content areas and produces a five-point severity rating scale for each area with an adequate interrater agreement (Brodey et al., 2005).
Adults
The Structured Clinical Interview for DSM-5 (SCID-5; First et al., 2016) is a semi-structured interview developed as a companion to the DSM-5 and offers versions for research and clinical settings. The SCID-5 has demonstrated excellent reliability, validity, and high specificity for SUD assessment for outpatient or inpatient clinical settings and when using raters with divergent training backgrounds and clinical experience (Osório et al., 2019; Shabani et al., 2021), and research has supported its use in-person and over the phone. 13 The Mini-International Neuropsychiatric Interview (MINI[-Plus]; Sheehan, 2016; Sheehan et al., 1998) is another example of a diagnostic interview developed for clinical and research use; however, much less research is available examining psychometric properties for SUD assessment. The AUDADIS-5 (Grant et al., 2015) similarly assesses an array of SUDs and is primarily used in research settings. It has evinced fair to excellent test–retest reliability (Grant et al., 2015), and it has demonstrated fair to very good concordance with the Psychiatric Research Interview for Substance and Mental Disorders DSM-5 Version [PRISM-5] (Hasin et al., 2011), another well-validated SUD diagnostic interview (Grant et al., 2015; Hasin et al., 2020, 2011). Some caution, however, should be used when interpreting the Alcohol Use Disorder and Associated Disabilities Interview Schedule, as previous work has shown that it likely confounds symptoms of a hangover with withdrawal (Boness et al., 2016). The CIDI 14 (Kessler & Üstün, 2004; Robins et al., 1988) and the Diagnostic Interview Schedule for DSM-IV (Robins et al., 2000) were similarly developed for psychiatric epidemiology research, are well-validated, structured interviews, and can be administered by trained lay raters. The Substance Dependence Severity Scale, a semi-structured interview, has shown good reliability and validity (Miele et al., 2000, 2001), and of note, it was developed to measure changes in diagnostic severity over time. Finally, the Alcohol Use Disorder symptom checklist was developed as a brief self-report instrument that has good reliability for assessment in primary care settings (Hallgren, Matson, Oliver, Caldeiro, et al., 2022; Hallgren, Matson, Oliver, Witkiewitz, et al., 2022). Initial validation on a Substance Use Disorder checklist for primary care was also recently completed (Matson et al., 2023).
Outcome and Treatment Monitoring
The ability to monitor specific outcomes related to SUD as well as treatment response can be useful for many purposes. For example, a person’s main treatment goal may be to reduce alcohol consumption. Thus, the clinician may choose to monitor the person’s consumption at each session as an indicator of progress toward their goal.
Consumption
The ability to capture consumption is often central to the evidence-based assessment of SUD and outcome monitoring more specifically. 15 Instruments recommended for assessing the consumption of substances include Form 90 (alcohol; Mattson et al., 1993; Miller & Del Boca, 1994) and Form 90D (drugs; Westerberg et al., 1998), Lifetime Drinking History (Skinner & Sheu, 1982) 16 and Lifetime Drug Use History (Day et al., 2008), various quantity and frequency measures 17 (see Sobell and Sobell (2004) for a detailed overview), and the Timeline Follow Back (Sobell & Sobell, 1992). Form 90 and Form 90D assess the 90-day interval before a person’s most recent drink, the Lifetime Drinking History, and Lifetime Drug Use History assess lifetime patterns of use including current use, quantity, and frequency measures tend to be past 30 days or past 12 months but are often adapted depending on the goal of the assessment, and the Timeline Follow Back covers the 30 to 365 days prior to the assessment date. Instruments with more recent assessment periods, such as quantity/frequency items, may be best for outcome and treatment monitoring.
Craving
Craving is an especially important outcome to assess, given it is implicated in many models of addiction as an antecedent and consequence of substance use (Boness et al., 2021; Tiffany & Wray, 2012). Craving also exhibits associations with substance use across a range of substances (Serre et al., 2015; Shmulewitz et al., 2023) and may be an important mechanism of behavior change in SUD treatment (Boness & Witkiewitz, 2022; Witkiewitz et al., 2022). Although craving is often measured in treatment research (Tiffany et al., 2012), it can be difficult to assess (Boness et al., 2019; Drobes, 1999; Tiffany & Wray, 2012), and many of the instruments, including some of those described here, would benefit from additional validation efforts (e.g., among adolescents). Instruments recommended for assessing craving are the Cocaine Craving Questionnaire-Brief (Sussner et al., 2006; Tiffany et al., 1993), 18 Heroin Craving Questionnaire-Short Form-14 (Heinz et al., 2006; Singelton, 1998), 19 Marijuana Craving Questionnaire-Short Form (12 item; Heishman et al., 2009), Penn Alcohol Craving Scale (Flannery et al., 1999), and the Questionnaire on Smoking Urges-Brief (Cox et al., 2001; Tiffany & Drobes, 1991).
Withdrawal
Substance-related withdrawal is potentially life-threatening, but there exist effective treatments for managing such symptoms. Instruments recommended for assessing substance-related withdrawal are the Amphetamine Cessation Symptom Assessment (McGregor et al., 2008), the Benzodiazepine Withdrawal Symptom Questionnaire (Tyrer et al., 1990) the Cocaine Selective Severity Assessment (Kampman et al., 1998), the Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (Sullivan et al., 1989), 20 and the Clinical Opiate Withdrawal Scale (Wesson & Ling, 2003). 21 These instruments have been primarily validated for use in medical settings, and there is a lack of research on their psychometric properties among adolescents, despite some practice guidelines detailing their use in adolescent populations (e.g., Meltzer & Masry, 2010 [Clinical Opiate Withdrawal Scale]; YouthAOD Toolbox [ Benzodiazepine Withdrawal Symptom Questionnaire, Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised]).
Psychosocial Functioning and Wellbeing
Understanding a person’s level of substance use, or even whether they meet the criteria for a SUD, can provide little information about overall functioning and wellbeing. Indeed, people can drink heavily and still function well in terms of their health, social connections, and quality of life (Pearson et al., 2021; Witkiewitz et al., 2019, 2020; Witkiewitz & Tucker, 2020). It is therefore important to assess psychosocial functioning and wellbeing in addition to other substance-related indicators such as consumption.
Functioning
There exist several comprehensive measures of psychosocial functioning that can be used in the evidence-based assessment of substance use disorders. The Addiction Severity Index (ASI) Lite (Cacciola et al., 2007) assesses functioning in the domains of medical/physical health, employment, alcohol and drug use, legal, family/social, and psychological. 22 The Psychosocial Functioning Inventory (Feragne et al., 1983) is a comprehensive assessment of functioning that includes subjective wellbeing, social roles, unpleasant events, and quality of health care but lacks information on its psychometric properties beyond its initial validation. The Short Form Health Surveys (SF-12 and SF-36; Brazier et al., 1992; Ware et al., 1996) are relatively brief instruments that measure perceived physical and mental health status. The World Health Organization Quality of Life Scale-Brief (The WHOQOL Group, 1998) assesses functioning in the domains of physical, psychological, social relationships, and environment. 23
Substance-Related Problems
One narrow indicator of psychosocial functioning is a lack of, or reduction in, substance-related problems or consequences. It’s important to note that although substance-related problems may be important for providing additional information beyond consumption, the use of problems or consequences as a sole indicator of SUD or wellbeing is also limited (Boness et al., 2021; Martin et al., 2014). Instruments recommended for assessing substance-related problems include the Rutgers Alcohol Problems Index (RAPI; White & Labouvie, 1989), the Short Inventory of Problems—Alcohol and Drugs (SIP-AD; Blanchard et al., 2003), and the Patient-Reported Outcomes Measurement Information System (PROMIS(®)) measures of alcohol consequences (Pilkonis et al., 2013, 2016) and drug use severity (Pilkonis et al., 2015). The RAPI was initially validated among adolescents but has since been extended to young adults (e.g., Martens et al., 2007) as well as other substances (e.g., Shono et al., 2018). The Short Inventory of Problems–Alcohol and Drugs has several variations of varying length with the briefest validated version being 10 items (Hagman et al., 2009). The PROMIS item banks can be delivered in fixed, short form, or computerized adaptive test versions (Pilkonis et al., 2013, 2015, 2016).
Treatment Planning and Level of Care Determination
Although many of the instruments previously discussed can be used for informing decisions about treatment and level of care determination for a given person, it is also important to mention the American Society of Addiction Medicine (ASAM) Criteria. The ASAM Criteria describe a comprehensive set of standards used to determine the level of care, management, and treatment for adults and adolescents seeking alcohol and substance use services. The Criteria assess six biopsychosocial dimensions (i.e., [1] acute intoxication and/or withdrawal potential, [2] biomedical conditions and complications, [3] emotional/behavioral/cognitive conditions and complications, [4] stage of change, [5] relapse, continued use/continued problem potential, and [6] recovery environment) which subsequently inform a level of care designation. There exist several standardized instruments for assessing the criteria including a free self-report questionnaire and paid computer-guided structured interview, although both are quite lengthy and psychometric information is limited. The criteria also include several guiding principles, including taking a holistic and strengths-based approach to assessment and care, individualizing care, providing a universal language across systems, specifying admission criteria for each level of care (e.g., outpatient, residential/inpatient), continued or extended stay, and discharge criteria. Clinicians are encouraged to place individuals in the least restrictive treatment setting with the highest likelihood of change. Early work on the criteria was mixed; however, over time, these guidelines have found considerable support among both clinicians (Padwa et al., 2022) and patients (Mark et al., 2021; Treiman et al., 2021) and have been implemented by various state and federal organizations as well as insurance companies for the purpose of reimbursement (Gastfriend & Mee-Lee, 2022). Despite this, clinical implementation has lagged behind (Gastfriend & Mee-Lee, 2022), perhaps partially due to the length of the assessment (Treiman et al., 2021) or concerns about the level of care recommendations being inconsistent with clinician judgment or patient preference (Padwa et al., 2022). Future efforts are needed to continue to validate the available assessment instruments for the ASAM criteria.
Assessment Processes
The following section covers additional assessment processes beyond the selection of assessment targets and instruments. As acknowledged by Hunsley and Mash (2007), the assessment process is itself a decision-making task. The assessor is required to “iteratively formulate and test hypotheses by integrating data that are often incomplete or inconsistent” (p. 30). Little to no guidance on evidence-based SUD assessment processes is offered in the literature. Here, we describe additional considerations that we view as imperative to a truly evidence-based assessment of SUD. This includes relational processes like establishing rapport and using a patient-centered approach as well as more technical processes such as considering drug classes, comorbidity, social determinants, and informant reports.
Relational Processes
Assessors must be careful to recognize that people who use substances and have a SUD diagnosis are highly stigmatized (van Boekel et al., 2013). This may be especially true for individuals with other marginalized identities (Kulesza et al., 2013). As such, prior to engaging in a formal assessment, assessors should critically self-reflect on biases about people who use substances that they have likely internalized and may have varying levels of awareness about. Such self-reflection should carry through the assessment process including the integration and interpretation of information. Relatedly, we encourage the use of person-centered approaches, such as motivational interviewing (Miller & Rollnick, 2013) which encourages listening to understand and empower, and embraces a spirit of compassion, rather than one of judgment. This can help establish rapport and may communicate the assessment encounter as a safe and supportive setting for the exchange of information about one’s substance use. Relatedly, depending on the setting and how recently a substance was used, engaging in a formal assessment process may be difficult for some individuals. Flexibility is imperative in these cases as people may not feel physically, cognitively, or emotionally able to complete a full assessment protocol at the designated time. We refer interested readers to Treiman and colleagues (2021) for examples of what clients in addiction treatment think SUD intake assessments should look like with respect to several features (e.g., comprehensiveness, logistics and relationship with the assessor).
Technical Processes
When assessing for SUD, we encourage assessment within specific drug classes (e.g., depressants, hallucinogens, and stimulants) given substances tend to differ with respect to their physiological effects, behavioral effects, and associated consequences (Advokat et al., 2018). It is important to understand the unique patterns of use for each substance as well as associated antecedents and consequences.
Relatedly, it is valuable to consider comorbidity, especially given the high co-occurrence of SUD with several other forms of psychopathology. This may be easily achieved with structured and semi-structured diagnostic interviews which often include modules on other forms of psychopathology. If a full diagnostic interview is not feasible, other options exist including the use of brief symptom checklists or screeners for other symptoms such as depression or anxiety. Regardless of the specific approach, at minimum, it can be useful for case conceptualization and treatment planning purposes to assess transdiagnostic features that are known to be implicated in SUD and other co-occurring disorders, such as negative affect (Watts et al., 2023).
Although we have explicitly considered age and developmental stage in the current review, there are other additional sociodemographic considerations that should be considered in a truly evidence-based assessment. Beyond consideration of whether an instrument has been appropriately validated for the individual being assessed, assessors must also consider how the individuals’ identities are relevant in choosing assessment targets and integrating assessment information. Assessors could consider the use of a formal instrument, such as the DSM-5 Cultural Formulation Interview (available at https://www.psychiatry.org/psychiatrists/practice/ dsm/educational-resources/assessment-measures) which can be administered to a patient and/or informant to elucidate potential differences such as cultural understandings of etiology and manifestation of, natural history, and treatment or healing paths for SUD. Assessors might choose to informally inquire about processes such as how their symptoms are viewed in their community, what degree of social support they have, and so on. Many minoritized groups embrace a holistic understanding of wellbeing that includes spirituality and social factors in addition to biological and psychological factors (Conner et al., 2009; Galanter et al., 2007). In addition, it is imperative to consider what social determinants (e.g., housing, health care, education, neighborhood, income, discrimination) are at play for a person, especially as they relate to the causes and maintenance of their SUD and what next steps may be best for the person. We refer readers to Paquette and colleagues (2019) for a more thorough discussion.
There may be instances, such as when working with youth or someone who is currently intoxicated, where informant reports may be included as part of the assessment process. Informant reports of substance use are limited in some ways. For example, mothers tend to underreport substance use relative to adolescent self-report (Winters et al., 2000). Despite this, informant reports may still improve the validity of SUD assessments by (a) providing additional details the patient is either not aware of (e.g., due to lack of insight) or unable to report on (e.g., due to substance-related disinhibition or impairment such as altered mental status), and (b) providing additional insight into overall functioning beyond substance use, for example. Given that discrepancies between adolescent and parent reports may indicate higher levels of adolescent risk (Kerr et al., 2010), careful consideration of when to include informant reports and how to frame them in the service of positive treatment outcomes is warranted. We encourage consideration of all available data in the course of an evidence-based assessment with a clear indication of discrepancies across informants should they arise.
Overall Recommendations
Our overall recommendations for the evidence-based assessment of SUD are as follows. First, we encourage assessors to reflect on their own biases, beliefs, and values, including how those relate to people that use substances or have a SUD (Frank & Nagel, 2017; Treiman et al., 2021; van Boekel et al., 2013). Second, viewing the patient as a whole person, consider their profile of symptoms and functioning inclusive of strengths, comorbidities, and social and cultural determinants (Conner et al., 2009; Galanter et al., 2007; Paquette et al., 2019; Treiman et al., 2021). Next, collaborate with the patient (and even their family or other providers) to select the assessment target that best fits their goals (while understanding some targets may also be required by the clinician or organization; Pincus et al., 2007; Tauscher et al., 2021). This will guide the selection of the best instrument(s) for the given target, which can be further selected based on whether the psychometric properties support the instrument’s use for that person. Here, we encourage dimensional over purely categorical diagnostic approaches and encourage direct assessment of strengths and wellbeing (Tauscher et al., 2021; Watts et al., 2023). Finally, assessment information and data should be integrated in a holistic manner, considering informant reports or collateral information when indicated and explicitly noting any limitations of the conclusions (e.g., using an assessment instrument that may not have sufficient psychometric information to determine its appropriateness for use with that specific patient).
Future Directions
Future directions worth considering in the evidence-based assessment of SUD are numerous. Importantly, assessment instruments must continue to be validated among diverse groups of individuals, with issues like measurement equivalence considered as part of such validation efforts to ensure precision in capturing SUD. When measurement invariance is not evidenced or a cultural group finds assessment instruments unacceptable (e.g., certain important constructs are missing), then cultural adaptations of instruments or the development of new instruments may be warranted which then need to undergo psychometric evaluation. We also advocate for assessors to move beyond categorical SUD assessment and instead toward dimensional assessment practices, especially those that focus on etiologic, maintenance, and socioecological processes over psychosocial consequences (Boness et al., 2021; Martin et al., 2014). Dimensional assessment, in comparison to categorical assessment, can provide a clearer picture of individual profiles of functioning. Dimensional assessments that focus on etiologic and maintenance mechanisms alongside socio-ecological processes have the potential to clarify targets for precision medicine efforts which may ensure that people are getting the best SUD treatments for them (Boness & Witkiewitz, 2022). Last, we call for a more systematic consideration of assessment utility (i.e., the degree to which assessment itself impacts relevant treatment targets; see Epstein and colleagues, 2005 for an example).
Supplemental Material
sj-docx-1-asm-10.1177_10731911231177252 – Supplemental material for Evidence-Based Assessment of Substance Use Disorder
Supplemental material, sj-docx-1-asm-10.1177_10731911231177252 for Evidence-Based Assessment of Substance Use Disorder by Cassandra L. Boness, Juan Carlos Gonzalez, Chelsea Sleep, Kamilla L. Venner and Katie Witkiewitz in Assessment
Footnotes
Acknowledgements
We wish to explicitly acknowledge that our entire authorship team was trained as clinical psychologists, which may influence the information and recommendations presented in the current manuscript. We would also like to thank the reviewers who provided constructive comments on earlier versions of this manuscript.
Authors’ Note
The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Investigator effort partially supported by NIAAA K08AA030301 (PI: C.L.B.) and R25AA028464 (PI: Flanagan).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.