
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder that affects individuals from all life stages, genders, and races/ethnicities. Accurate assessment of ADHD across different populations is essential as undiagnosed ADHD is associated with numerous costly negative public health outcomes and is complicated by high comorbidity and developmental change in symptoms over time. Predictive analysis suggests that best-practice evidence-based assessment of ADHD should include both ADHD-specific and broadband rating scales from multiple informants with consideration of IQ, academic achievement, and executive function when there are concerns about learning. For children under age 12, parent and teacher ratings should be averaged. For adolescents and adults, informant reports should be prioritized when self- and other-report are inconsistent. Future research should provide more stringent evaluation of the sensitivity of measures to treatment response and developmental change over time as well as further validate measures on historically understudied populations (i.e., adults, women, and racial/ethnic minorities).
Attention-deficit/hyperactivity disorder (ADHD) is a chronic neurodevelopmental disorder characterized by developmentally inappropriate symptoms of inattention and hyperactivity/impulsivity (American Psychological Association [APA], 2013). Similar to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), the DSM-5 TR requires (a) six symptoms of inattention and/or six symptoms of hyperactivity/impulsivity, (b) present before the age of 12, (c) impacting functioning in at least two settings, (d) cause impairment, and (e) are not better attributed to another mental disorder (APA, 2022). Diagnosis of ADHD in adults only requires five symptoms per domain instead of six. ADHD has a prevalence rate of roughly 5% of children between the ages of 6 and 18 years worldwide, although prevalence rates in adults are reportedly lower (Faraone & Biederman, 2005; Kessler et al., 2006; Polanczyk et al., 2015). While there is a significant gender-biased prevalence rate of approximately 3:1 favoring males in childhood (Skogli et al., 2013), such differences decrease during adolescence and are lower in adulthood (Das et al., 2012). ADHD is also highly heritable with heritability estimates of about .8, and children with a first-degree relative with ADHD are four to five times more likely to be diagnosed with ADHD (Frazier & Youngstrom, 2006; Gizer et al., 2009; Nikolas & Burt, 2010). ADHD has three presentations: predominantly inattentive, predominantly hyperactive impulsive, and combined presentation, although there is limited stability and evidence of prescriptive utility in specific presentations (Lahey et al., 2005; Pelham, 2001).
Accurate assessment of ADHD is essential as undiagnosed and untreated ADHD has been implicated in numerous important public health outcomes such as increased job instability, obesity, increased mortality due to accidents, and higher incarceration rates and substance use disorders (Cortese & Tessari, 2017; Dalsgaard et al., 2015; Gudjonsson et al., 2009; Hamed et al., 2015; Lichtenstein et al., 2012; Quinn & Madhoo, 2014). Individuals with ADHD also experience increased comorbidity rates compared with those without ADHD. Past epidemiological work has suggested that youth with ADHD are five times more likely to develop disruptive, learning, anxiety, and depressive disorders (Angold et al., 1999). Critically, co-occurrence of depression in those with ADHD has been associated with greater functional impairment, longer and more severe depressive episodes, and higher rates of suicidality and hospitalizations than either disorder in isolation (Biederman et al., 2008; Chronis-Tuscano et al., 2010; Daviss, 2008; Reid et al., 2015).
Evidence-based assessment (EBA) of ADHD is essential for accurate assessment and early intervention, which, in turn, mitigate the substantial negative outcomes associated with undiagnosed and untreated ADHD (Pritchard et al., 2012). Previous studies have demonstrated the accuracy and efficiency of using EBA strategies (Zhou et al., 2018), which keep assessment costs low and reduce lengthy assessment waitlists. However, complicating the use of such measures is the significant degree of heterogeneity in the phenotypic presentation of ADHD, which has resulted in the use of presentations that also show differences in comorbidity profiles (Barkley, 2013; Garner et al., 2013).
A further complicating factor is a developmental change over time. Namely, research indicates that hyperactivity and impulsivity symptoms are most salient during early childhood but tend to decline throughout middle and late childhood (Olson, 2002). In contrast, during these later childhood periods, inattention symptoms begin to emerge and are more noticeable, particularly as children begin school (Hart et al., 1995; Lahey et al., 2005). These inattentive symptoms (particularly the key symptoms of being easily distracted and having difficulties sustaining attention; see Martel, Eng et al., 2021) tend to persist over time and remain problematic for an individual as they enter adolescence and adulthood, while many adults seem to “outgrow” their childhood symptoms of hyperactivity (Martel, Goh et al., 2021). Ultimately, roughly 50% of childhood ADHD cases continue into adulthood (Faraone & Biederman, 2005; Kessler et al., 2006).
Such heterogeneity impacts how assessments are conducted throughout the lifespan. We briefly present two previously published case studies to emphasize how the assessment procedures for ADHD change across the lifespan and can and should be personalized based on comorbidity considerations. For the sake of brevity, we briefly present the individual’s background and presenting complaints and the authors’ assessment procedures.
Childhood
The case study by Babinski et al. (2018) examined the efficacy of tailoring behavioral parent training and adjunctive social skills for a young girl with ADHD and other concerns. Violet was a 9-year-old girl who was referred to group behavioral treatment related to ADHD and additional interpersonal impairment. Violet had previous diagnoses of ADHD combined type, generalized anxiety disorder, and social anxiety disorder and presented to treatment with significant peer and parental difficulties. Her mother noted that Violet struggled to maintain friends and was frequently rejected, bullied, and excluded by her peers. Violet had difficulty regulating her emotions and presented with a labile mood. At home, she was noncompliant and often required redirection. She also struggled academically and had little ability to initiate her assignments. Prior treatment included the use of selective serotonin reuptake inhibitors and play therapy, the latter of which was terminated because her mother did not find it beneficial.
The diagnostic assessment was conducted using the semi-structured Disruptive Behavior Disorders Interview. Based upon her mother’s report on this interview, Violet met the criteria for ADHD combined presentation but for not oppositional defiant disorder (ODD). She and her mother also completed the mood and anxiety modules of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Aged Children, a broadband semi-structured interview. However, anxiety symptoms were not pervasive enough to warrant a diagnosis of an anxiety disorder. Several additional measures were collected at pre- and post-treatment including the Disruptive Behavior Disorders Rating Scale, the Screen for Child Anxiety and Related Disorders, the Short Mood and Feelings Questionnaire, and the Impairment Rating Scale which are all more specific measures. Therefore, broad and narrow band assessment was conducted. Yet, school difficulties were not evaluated.
Violet’s diagnosis of ADHD combined presentation appeared to be the primary driver of her impairment across settings including school, home, and with peers, contributing to the anxiety she experienced and her oppositionality. Beyond this, Violet presented with several factors that increased her risk of later problems including significant peer rejection, inconsistent disciplining strategies as used by Violet’s parents, and parental psychopathology along with elevated stress at home. Therefore, a comprehensive approach to ADHD (including parent support supplied in a group treatment setting for ADHD with a social skills component) may be most effective for this child and family, highlighting the need for complex assessment of ADHD and related disorders during childhood to mitigate negative outcomes later in life. Yet, it remains unclear whether school functioning needed to be further addressed.
Adulthood
The case study by Puente and Mitchell (2016) examined the efficacy of tailoring group-based CBT for an adult with ADHD. Brian was a 32-year-old Caucasian male who presented to an ADHD program with difficulties in executive functioning skills including concentration, forgetfulness, initiating and completing various tasks, organizing and planning daily activities, and overall time management. These difficulties led to impairments across his life, particularly at home and work.
Assessment procedures, conducted under DSM-IV, included the use of the self- and informant-report versions of the Conners’ Adult ADHD Rating Scale (CAARS) and the Conners’ Adult ADHD Diagnostic Interview for DSM-IV. Across both versions of the rating scales, Brian and his wife endorsed elevations across several domains including Inattention/Memory Problems, DSM Inattention Symptoms, and DSM Total ADHD Symptoms; his wife also endorsed Impulsivity/Emotional Lability, Problems with Self-Concept, DSM Hyperactivity/Impulsivity Symptoms, DSM Inattention Symptoms, and DSM Total ADHD Symptoms. Furthermore, on the structured diagnostic interview, Brian endorsed all nine symptoms of inattention and five of the nine symptoms of hyperactivity/impulsivity.
Beyond these ADHD-specific instruments, as recommended to rule out common comorbid problems, Brian was administered the Structured Clinical Interview for DSM-IV Axis I Disorders, a broadband semi-structured interview. He continued to endorse elevations in inattentive symptoms as well as symptoms consistent with generalized anxiety disorder. Upon further investigation, it was determined that Brian’s anxiety was better explained by his ADHD rather than being its own separate diagnosis. Ultimately, Brian was diagnosed with DSM-IV ADHD, predominantly inattentive presentation, and given this information in the context of his presenting concerns, his treatment might most effectively focus on behavioral strategies for managing executive function and anxiety secondary to ADHD, although the executive function was not formally evaluated.
Choice of Measures
As highlighted in these case examples, there are a multitude of broadband screeners, ADHD-specific rating scales, and interviews that have been validated for the accurate and reliable assessment and diagnosis of ADHD. Due to the high heterogeneity and comorbidity of ADHD with other psychological disorders, broadband measures should be used to screen for co-occurring difficulties as well as alternative explanations for the symptoms being reported by the client and their family. Next, ADHD symptom-specific scales should be administered to both parents and teachers, or, in adults, the client and another informant. Finally, impairment should be assessed, either as a component of another measure or separately, to identify the specific ways a client’s reported symptoms are impacting their day-to-day functioning. These types of measures (summarized in Table 1) should be administered at a minimum.
Recommended Measures.
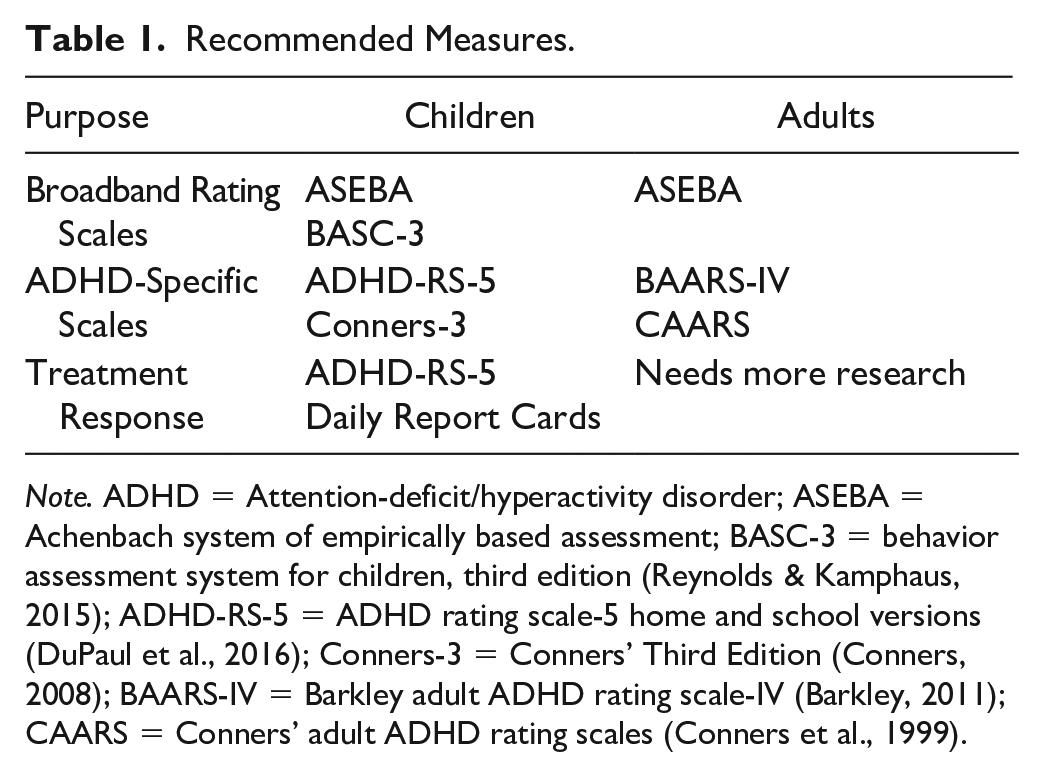
Note. ADHD = Attention-deficit/hyperactivity disorder; ASEBA = Achenbach system of empirically based assessment; BASC-3 = behavior assessment system for children, third edition (Reynolds & Kamphaus, 2015); ADHD-RS-5 = ADHD rating scale-5 home and school versions (DuPaul et al., 2016); Conners-3 = Conners’ Third Edition (Conners, 2008); BAARS-IV = Barkley adult ADHD rating scale-IV (Barkley, 2011); CAARS = Conners’ adult ADHD rating scales (Conners et al., 1999).
Instrument Selection and Predictive Utility
There are a number of measures available within each category. In a meta-analysis examining parenting interventions for youth with ADHD, Coates and colleagues (2015) identified seven distinct instruments that were used to capture ADHD across 11 (63%) studies. Several reviews have presented evidence suggesting differences between broadband and narrowband instruments (e.g., Angello et al., 2003; Collett et al., 2003; Pelham, Fabiano, & Massetti, 2005), although much of the extant literature has focused on DSM-IV conceptualizations of ADHD. Vaughn et al. (1997) found no differences between the Behavior Assessment System for Children (BASC) and Child Behavior Checklist (CBCL)—using parent and teacher versions for both measures—in diagnosing youth with and without ADHD; the Teacher Report Form (TRF) of the CBCL was better than the other measures at identifying youth without ADHD. Somewhat similar results were found by Angello and colleagues (2003). Their review of six published ADHD rating scales found that the parent and teacher versions of the BASC were able to differentiate between youth with and without ADHD, and between youth with inattentive and combined presentations. In addition, Conners’ Rating Scale-Revised (CRS-R) was uniquely able to differentiate youth with ADHD from youth with mood issues (Angello et al., 2003). More recently, the diagnostic performance of the Attention problems scale on the parent and teacher versions of the CBCL was compared with that of the CRS-R. Ultimately, these measures demonstrated generally similar diagnostic performance (Chang et al., 2016).
In addition to broadband instruments, narrowband rating scales are useful and typically more time efficient in assessing ADHD. The ADHD Rating Scale-5 Home and School Versions (ADHD-RS-5; DuPaul et al., 2016) is a particularly popular narrowband rating scale. Prior work has shown this normative-based rating scale to accurately differentiate between youth with and without ADHD, with rates as high as 68% and 84% for parent report and teacher report, respectively (Angello et al., 2003), as well as differentiating between youth with different subtypes of ADHD (Pelham et al., 2005). The ADHD-RS-5 has also been shown to have a unique predictive ability at the item level. For instance, Martel, Goh, and colleagues (2021) found that a subset of four items on the ADHD-RS-5, as measured at baseline, predicted mental health difficulties 5 years later. The predictive utility of these four items was the same as the predictive utility of all 18 ADHD symptom items. The Conners’ Third Edition is another popular narrowband rating scale (Conners-3; Conners, 2008). Similar to the ADHD-RS-5, prior work has demonstrated the Conners-3 ability to accurately differentiate between youth with and without ADHD, with rates as high as 78% for parent report, 76% for teacher report, and 73% for self-report (Kao & Thomas, 2010). In addition, the Conners-3 and ADHD-RS, along with other instruments including the CBCL and BASC, have shown sensitivity to treatment effects across pharmacological and behavioral treatments (Collett et al., 2003; Pelham et al., 2005) and therefore make them efficient choices of instruments.
Best Validated Broadband Measures
Broadband measures are critical for screening for ADHD-specific symptoms as well as other forms of psychopathology. While there are many broadband measures, as described just above, here we will discuss two that have high evidence of predictive utility in identifying children with ADHD. The Achenbach System of Empirically Based Assessment (ASEBA; Achenbach, 2009) has measures to assess both children and adults using multiple informants. Within this system, the CBCL has good reliability as well as convergent and discriminative validity for its DSM-oriented scales (Nakamura et al., 2009). The CBCL and TRF are particularly useful for predicting internalizing and externalizing disorders compared with Youth Self Report (Salbach-Andrae et al., 2009). Parent- and teacher-reported Attention Problems subscales on the CBCL and TRF are better able to identify youth with ADHD than general scales such as Externalizing Problems subscale (Hudziak et al., 2004). This Attention Problems subscale is particularly useful in identifying youth combined presentations but has not demonstrated the same utility in predicting youth with predominantly inattentive presentations (Jarrett et al., 2018).
The Behavior Assessment System for Children, Third Edition (BASC-3; Reynolds & Kamphaus, 2015) also has self, parent, and teacher forms and goes up through age 25. The BASC-3 has high internal consistency and good test–retest reliability and also include age- and sex-specific norms for both general and clinical samples (Reynolds & Kamphaus, 2015). Parent and teacher report on the BASC-3 has also demonstrated clinical utility in that youth with ADHD are rated higher on the Hyperactivity and Attention Problems subscales (Zhou et al., 2018). In addition, high scores on the Executive Functioning and Learning Problems subscales combined with low scores on Functional Communication and Resilience subscales are able to identify youth with ADHD over and above the Attention Problems and Hyperactivity subscales. Overall, the use of broadband rating scales could help to differentiate between individuals with and without ADHD as well as screen for other psychopathology in a cost-effective and efficient manner.
Best Validated ADHD-Specific Measures With Impairment Information
The ADHD-RS-5 and the Conners-3 are both commonly used and empirically supported to assess for ADHD symptoms. The items on the ADHD-RS-5 map directly onto the 18 ADHD symptoms listed in the DSM while the Conners-3 items assess both ADHD symptoms and related problems such as executive functioning, ODD, and conduct disorder. While both measures assess impairment, the ADHD-RS-5 assesses six domains of impairment: familial relations, peer relations, academic functioning, behavioral functioning, homework functioning, and self-esteem. The ADHD-RS-5 has high internal consistency and adequate test–retest reliability, inter-rater reliability, and criterion validity (Acosta-Rodas et al., 2019; Alexandre et al., 2018). The Conners-3 has very good test–retest reliability and internal consistency, and interrater reliability coefficients range from .52 to .94 (Conners, 2008). Therefore, either of these measures would be good option for assessing narrowband ADHD and associated impairment.
The CAARS (Conners et al., 1999) and Barkley Adult ADHD Rating Scale-IV (Barkley, 2011) are similar to the ADHD-RS-5 and Conners-3 but for adults. Although these rating scales have relatively strong psychometrics compared with other measures of adult ADHD, they are vulnerable to malingering, warranting the need for other informant reports (Dvorsky et al., 2016; Silverman, 2012; Taylor et al., 2011).
Developmental Differences and Multiple Informant Integration
ADHD is unique in being one of the only diagnoses that require the use of multiple informants, although the idea has also been considered for personality disorders (Alexander et al., 2017). However, little work has empirically evaluated how information from multiple informants should be integrated, particularly when the informants disagree. Some of the only empirical work that suggests that parent and teacher report should be averaged when assessing children (i.e., ages 6 and 12), as this approach outperformed an OR or AND algorithm approach to integration (Martel et al., 2015; Martel, Markon, & Smith, 2017) in predicting longitudinal outcomes such as social skills and academic performance (Martel, Eng et al., 2021). However, best practices appear to change when assessing ADHD in adolescence or adulthood. In adults, empirical evidence suggests that when there is a disagreement between self- and informant report, other report may be more related to objective forms of impairment such as executive function and should be prioritized (Martel, Nigg, & Schimmack, 2017). Empirical evidence and qualitative suggestions by Sibley and colleagues (2012a, 2012b, 2019) likewise suggest informant report may be more accurate than self-report in adolescents.
To summarize, current limited empirical evidence suggests that parent and teacher ratings should be averaged when assessing children aged 12 and below, but informant ratings should be prioritized in adolescents and adults when ratings from multiple informants are inconsistent. However, self-report rating scales may be useful for identifying potential internalizing symptoms and areas of risk that parents may not be aware of (e.g., covert delinquency, substance use, and sexual behaviors). Self-reports may also be useful for planning interventions that target specific symptoms and areas of impairment, even for individuals who do not meet full criteria for ADHD. Many of the above measures, including the BASC-3, ASEBA, and Conners-3, offer self-report forms for some ages (BASC-3 self-report begins at age 6).
Executive Functioning and Neuropsychological Assessment is Not Diagnostic
Although ADHD has historically been conceptualized as a disorder of executive function (EF; Nigg, 2001), recent meta-analyses have suggested that EF deficits have poor sensitivity and specificity with respect to predicting ADHD diagnosis (see review by Willcutt et al., 2005). Furthermore, children with anxiety, ODD, autism spectrum disorder (ASD), and other forms of psychopathology also exhibit EF deficits (see review by Pennington & Ozonoff, 1996). Even attention tasks like the Conners’ Continuous Performance Test (CPT) only inconsistently predict ADHD cases (Jarrett et al., 2018).
Because not all children with ADHD have EF deficits, an EF subtype of ADHD was examined in preparation for DSM-5. Yet, the number of subtypes found seemed to depend on how many tasks were included (Fair et al., 2012; Roberts et al., 2017), and some work suggests that EF does not clearly delineate various subgroups within ADHD, being more useful at predicting nondichotomous continuous outcomes such as academic and other external impairment indices (Goh et al., 2020; Samuels et al., 2016; Willoughby et al., 2012). Therefore, support is lacking for EF as a diagnostic criterion of ADHD or even an EF subtype within ADHD (Frick & Nigg, 2012). Yet, EF deficits in children with ADHD do clearly predict academic difficulties and, thus, may be useful in comprehensive psychoeducational evaluations to aid in personalized interventions (Martel, 2020; Willoughby et al., 2017). Likewise, although classroom observations can be helpful in a challenging case of differential diagnosis, they are often not practical due to cost-effectiveness and/or protecting client confidentiality.
Assessment for Comorbid Learning Problems
ADHD is often comorbid with learning disabilities (LD), with children with ADHD being three to four times more likely to have LDs than their typically developing peers (reviewed in DuPaul & Volpe, 2009). Prior research indicates that the association between ADHD and LD is driven by inattentive symptoms, deficits in working memory and processing speed, and by multiple genes that are implicated in both disorders (Paloyelis et al., 2010; Rabiner et al., 2000; Rapport et al., 2008; Shanahan et al., 2006). Due to this high comorbidity, the presence of LDs should be ruled out using achievement and intelligence testing, parent- and teacher-report, and/or academic records. Although ADHD and LD share similar IQ profiles with deficits in working memory and processing speed, these scores are not diagnostic, and completing intelligence and achievement tests is often costly and time-consuming. Therefore, this additional testing should only be completed if there is a specific concern about learning or the caregiver or school requests such testing. IQ profiles should be combined with other information from rating scales, observations, and clinical interviews to identify strengths and weaknesses to better inform treatment goals and interventions (reviewed in Calderon & Ruben, 2008; Martel, 2020).
Measure Sensitivity to Developmental Change in Symptoms
A final area where differences across measures may exist is in their sensitivity to developmental change in ADHD symptom trajectories. There is a bounty of work examining trajectories of ADHD symptoms across the lifespan. Franke et al. (2018) presented a theoretical framework for several distinct ADHD symptom trajectories from childhood to adulthood, ranging from typical developing controls and subthreshold patterns to onset post-brain injury and persistent ADHD trajectories. A review of the empirical literature highlights that the majority of studies examining ADHD symptom trajectories have often used diagnostic interviews or, to a lesser extent, broadband scales; few have used narrowband measures to capture repeated measures of ADHD symptoms.
Döpfner et al. (2015), Sasser et al. (2016), and Walton et al. (2017) identified three distinct developmental trajectories of ADHD, characterized by low, medium, and high symptom trajectories. Importantly, measures of ADHD symptoms varied across studies, with Döpfner et al. (2015) using the German-based ADHD Symptom Checklist from childhood to adulthood, Sasser et al. (2016) using the Diagnostic Schedule Interview for Children, and Walton et al. (2017) using the Development and Well-Being Assessment Interview; the latter two studies examined trajectories from childhood into adolescence.
Not all studies have observed these same three trajectories, however, as some studies have found different results when modeling hyperactivity/impulsivity symptoms separate from inattention symptoms and when considering gender. It should be noted that no studies have examined race/ethnicity. Differences across these studies are undoubtedly due, in part, to methodological variation including sample types and sizes, assessment points, predictors of trajectories, and diagnostic procedures. Further work is needed to evaluate normative symptom trajectories across development, gender, and race/ethnicity. Furthermore, empirical evaluation of developmental sensitivity to normative changes in ADHD symptoms is desperately needed with one of the few studies to date suggesting decreasing importance of hyperactive/impulsive symptoms in adulthood (vs. childhood; Martel et al., 2012).
Evaluation of Treatment Efficacy
As a related point, work on the sensitivity of measures to symptom change from treatment is sorely needed because assessment of ADHD symptoms and impairment should not end once an ADHD diagnosis is given. As recommended for other disorders, continued assessment of ADHD symptoms is essential to ensure that treatment is effective and that functioning improves. For children with clinically significant ADHD symptoms, reliable change in symptoms and impairment can be tracked using the ADHD-RS (Szomlaiski et al., 2009). However, for children without clinically significant ADHD symptoms (including those whose symptoms have improved so that they are no longer clinically significant), symptom change is less reliable, and tracking general functioning (vs. ADHD) is a more reliable way to assess improvement (Karpenko et al., 2009). However, that is outside the scope of this article and will not be discussed herein.
In addition to the use of the ADHD-RS-5, during the initial assessment, clinicians should collaborate with caregivers to identify the behaviors that are creating the most impairment. After target behaviors have been identified, functional assessment tracking is an additional useful way to track personalized treatment goals of the individual or family. Several different methods for tracking these types of behavior can be useful. The most well-studied is daily report cards (DRC), which is a time-efficient way for teachers to communicate treatment progress in children with caregivers and clinicians by indicating the frequency that specific behaviors occurred at school (Evans & Youngstrom, 2006). Research on DRCs has indicated they are sensitive to both medication and psychosocial treatment effects (Pelham et al., 2002). There are numerous other methods for assessing personalized treatment goals in adults such as frequency of target behaviors, but these methods are less well-standardized and well-studied. Some research suggests that wearable technology and daily mobile surveys of symptoms might be more accurate than in-visit measures of treatment monitoring (Surman et al., 2022; I. C. Wong et al., 2019). As such, they are an important direction for future work.
Future Directions
Although there is much that is known about ADHD and its EBA, more research is needed to better assess certain populations. For example, many clinicians report lacking confidence in their ability to accurately diagnose ADHD in adults (Schneider et al., 2019). Adults only need five (instead of six) symptoms per domain to be diagnosed with ADHD, and many DSM-5 symptoms include additional language to better describe symptom expression in adulthood. However, more research is needed to determine if different sets of symptoms should be used to diagnose adults. For example, “runs about” and “often has difficulty playing or engaging in leisure activities quietly” appear less relevant for adults with ADHD (Martel et al., 2015). Symptoms such as restlessness and emotion dysregulation might be more developmentally appropriate and still allow for the differentiation between ADHD and neurotypical adults, an idea that is still being evaluated (Hirsch et al., 2018; Wender et al., 2001). Little work thus far has provided a rigorous evaluation of developmental differences and changes in symptom expression from preschool to adulthood.
In addition, further research is needed on ratings and diagnoses of ADHD in adolescent girls and women in general. Girls and women with ADHD may be underidentified, given they have lower rates of comorbid disruptive behavior disorders and higher rates of internalizing problems (Chronis-Tuscano et al. 2010; Hinshaw et al., 2022). Preliminary research suggests ADHD symptoms begin to fluctuate on a cyclical basis in concordance with the menstrual cycle beginning around puberty (Roberts et al., 2018). Adolescent girls with ADHD likewise appear to begin to experience increased depression and impairment (Eng et al., In Press). Assessments therefore not only need to be sensitive to these effects but potentially may need to take into account reproductive and menstrual cycle phases in girls and women.
Another heavily understudied area in the assessment of ADHD is the impact of race and ethnicity. Despite race and ethnicity being social constructs with little, if any, biological meaning (Mersha & Beck, 2020), group differences across socially defined race groups are likely related to social and systemic factors (e.g., racism, differential access to health care, SES, etc.; see Flanagin et al., 2021). Such differences have relevance for ADHD. Racial and ethnic minorities may be at higher risk of exposure to risk markers of ADHD, including lower birth weight, maternal education, and household income (Cénat et al., 2021). Yet, the limited research assessing racial and ethnic differences in ADHD’s prevalence has yielded equivocal results.
For instance, some studies have suggested that Black children exhibit a higher prevalence of ADHD compared with White children (Cuffe et al., 2005; Danielson et al., 2018). In contrast, other research has found no such differences (A. W. Wong & Landes, 2022), or reversed effects (i.e., higher rates in White versus Black adolescents; Shi et al., 2021). Reasons for any differences also remain unclear; it has been proposed that ADHD may be underdiagnosed in Black children (Coker et al., 2016), despite Black mothers tending to rate children as higher on ADHD symptoms compared with White mothers (Barrett & DuPaul, 2018). One review has also suggested that Black children tend to exhibit more ADHD symptoms than White children but are diagnosed less often, possibly related to parental effects and accessibility of treatment (Miller et al., 2009). Furthermore, other races/ethnicities show differences as well but have been less studied (but see Chung et al., 2019; Collins & Cleary, 2016; Getahun et al., 2013; Kapke et al., 2019; Shi et al., 2021; A. W. Wong & Landes, 2022).
In general, causes of racial and ethnic disparities in ADHD are likely numerous and involve factors related to problem recognition, cultural stereotypes and biases in raters and clinicians, and care-seeking tendencies (Coker et al., 2016). Furthermore, it is likely that fear of stigma and racial discrimination continue to underlie differences in referral and diagnosis, yet these effects remain understudied. Clarification and resolution of these issues will likely demand a multipronged approach that involves several interested/affected groups and partners. In particular, the deployment of culturally sensitive and appropriately normed assessment protocols that both address gaps in knowledge about ADHD and help facilitate strong and trusting relations remains a vital goal. Similarly, it will also be worthwhile to determine whether ADHD criteria identify children to the same degree across race and ethnicity, or whether they need to be modified depending on cultural context. There is also a need for professionals to develop a wider understanding of cultural variations in ADHD, particularly in racial and ethnic minority groups, in addition to cultural competence pertaining to various models of illness, behavior, bias, family dynamics, and developmental issues (Kagitcibasi, 2005).
Summary
In sum, current evidence-based procedures for ADHD clearly suggest the need for narrow- and broadband ratings to assess ADHD and common comorbidity, with consideration of academic achievement, IQ, and executive function assessment in cases with concerns about learning problems. Furthermore, the developmental phase is an important consideration that impacts how multiple informant data should be integrated. Limited current data suggest parent and teacher reports should be averaged during childhood, but other informants should be prioritized over self-ratings of ADHD in adulthood with consideration of self-report of comorbid internalizing problems. A particularly important direction for future work is the sensitivity of symptom ratings to developmental change over time and treatment response. In addition, the validity of measures to populations such as adults/adolescents, girls/women, and non-Caucasian races/ethnicities desperately needs additional empirical examination.
Footnotes
Authors’ Note
NIAAA and NIH had no role in the writing of the manuscript or the decision to submit the paper for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Alcohol Abuse and Alcoholism training grant T32 AA027488 and the National Institute of Mental Health R01-MH119119.