
Abstract
Generalized anxiety disorder (GAD) is a leading mental health concern during pregnancy and the postpartum (perinatal) period. People with GAD engage in problematic behaviors to manage their distress. However, the extent of GAD behaviors during the perinatal period may not be adequately captured by the Worry Behaviors Inventory (WBI), the most comprehensive measure of GAD behaviors to date. We evaluated the structure of the initial WBI item-pool and then evaluated the internal consistency, construct validity, and predictive utility of the Perinatal Revised WBI (WBI-PR) in a sample of 214 perinatal women with and without GAD. A two-factor, 10-item scale was supported, and some of the retained items differed from the original WBI. Internal consistency of the WBI-PR was acceptable, and evidence of construct validity was demonstrated. The WBI-PR predicted GAD diagnostic status both alone and beyond existing generalized anxiety and depression symptoms. Implications of these findings are discussed.
Generalized anxiety disorder (GAD)—characterized by excessive and difficult to control worry about a number of events or activities (American Psychiatric Association [APA], 2013)—is a common mental health concern, with lifetime prevalence of 4.3% (Kessler et al., 2012). GAD is a chronic condition with high likelihood of recurrence and is associated with occupational impairment, health difficulties, life satisfaction, and suicidal tendencies comparable to that of major depressive disorder (MDD; Pelletier et al., 2017; Weisberg, 2009). However, GAD remains one of the most poorly defined and least successfully treated anxiety disorders (Olatunji et al., 2010), as research devoted to understanding its clinical features pales in comparison to other anxiety disorders (Dugas et al., 2010).
Much of the scientific literature on the clinical features of GAD has focused on its cardinal symptom, worry. Prevailing theoretical models emphasize the role of covert processes and avoidance of internal experiences (i.e., thoughts and emotions) as central to the maintenance of GAD (Behar et al., 2009). Worry itself has been conceptualized as a negatively reinforcing avoidance strategy aimed at reducing physiological and emotional arousal (Borkovec, 1994; Borkovec et al., 2004) and is therefore functionally equivalent to the overt behavioral responses observed in other anxiety and related disorders. However, in addition to cognitive avoidance strategies, those with GAD are also thought to engage in overt behaviors to manage their distress. The ‘Metacognitive Model’ (Wells, 1999) suggests that those with GAD engage in meta worry (i.e., worrying about worrying), which leads to the use of ineffective strategies—including overt behaviors (e.g., situational avoidance, checking, reassurance seeking)—aimed at controlling thoughts and emotions (Behar et al., 2009; Wells, 1999). Furthermore, the ‘Intolerance of Uncertainty Model’ suggests that individuals with GAD use various maladaptive behaviors to manage uncertainty (e.g., situational avoidance, excessive information seeking; Hebert & Dugas, 2019). The use of these behaviors is thought to reinforce negative beliefs about uncertainty, as the nonoccurrence of catastrophic outcomes is attributed to the behavioral response. Indeed, those with GAD have been found to engage in problematic avoidance (e.g., avoiding feared situations, procrastination, delayed decision-making) and safety behaviors (e.g., checking, reassurance-seeking, over-preparation, control) in response to their worries (Beesdo-Baum et al., 2012; Coleman et al., 2009; Robichaud, 2013; Robichaud et al., 2019; Schut et al., 2001). Furthermore, greater use of these overt behaviors appears to contribute to poorer long-term prognosis of GAD (Beesdo-Baum et al., 2012). Based on this initial evidence, the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) Anxiety Disorders Workgroup proposed that overt behaviors be added to the diagnostic criteria of GAD (Andrews et al., 2010). Here, endorsement of at least one of four behaviors (i.e., avoidance, procrastination, overpreparation, and reassurance seeking) would be required to receive a diagnosis of GAD. Ultimately, however, behavioral criteria were not implemented due to a lack of evidence to support these changes and an absence of available tools to assess GAD behaviors at that time (Brown & Tung, 2018; Mahoney et al., 2016).
In response to these shortcomings and to facilitate research on the contribution of overt behaviors to GAD pathology, Mahoney and colleagues (2016) developed the first comprehensive self-report measure of GAD behaviors. The Worry Behaviors Inventory (WBI) assesses the tendency to engage in behaviors aimed at preventing, controlling, and avoiding worrying. WBI items were generated based on a review of GAD literature and led to the identification of 26 unique behaviors that were reviewed by six experts and piloted in a sample of treatment seeking patients (Mahoney et al., 2016). Six items were deemed redundant resulting in 20 items, with content covering a range of avoidance (e.g., item 9: “I avoid situations or people that worry me”), reassurance seeking [e.g., item 1: “I seek reassurance from other people (e.g., family, friends, doctors, experts, authorities)”], checking (e.g., item 20: “I repeatedly check that things have been done properly”), controlling [e.g., item 15: “I take control of every aspect of a situation (e.g., try to do everything myself, avoid delegating tasks, control money/finances, keep a close eye on what is happening)”], hypervigilance (e.g., item 8: “I keep a close watch for anything bad that could happen”), and overpreparation behaviors [e.g., item 19: “I over-plan activities (e.g., prepare for all possible bad outcomes, have a plan B, plan every step of an activity)”; see Table 1]. The 20-item pool was administered to 1201 patients seeking treatment for anxiety and depression, and factor analyses led to a two-factor, 10-item scale, which was easily interpretable (assessing avoidance and safety behaviors) and demonstrated good model fit based on the Comparative Fit Index (CFI = .95) and Tucker–Lewis Index (TLI = .97), and mediocre model fit based on Root Mean Square Error of Approximation (RMSEA = .10). The WBI and subscales have since demonstrated acceptable to excellent internal consistency (α’s ranging from .70 to .90), convergence with measures assessing similar constructs (e.g., GAD symptoms and worry), and evidence of discriminant validity (Mahoney et al., 2016; Mahoney, Hobbs, Newby, Williams, & Andrews, 2018; Mahoney, Hobbs, Newby, Williams, Sunderland, & Andrews, 2018; Mahoney, Hobbs, Williams, Andrews, & Newby, 2018). The WBI is also sensitive to change across treatment and has been found to mediate the relation between various cognitive factors (e.g., cognitive avoidance) and GAD symptoms (Mahoney, Hobbs, Newby, Williams, Sunderland, & Andrews, 2018; Mahoney, Hobbs, Williams, Andrews, & Newby, 2018). However, the WBI has not been validated for use during pregnancy and the postpartum (perinatal) period.
Initial Worry Behaviors Inventory Item Pool
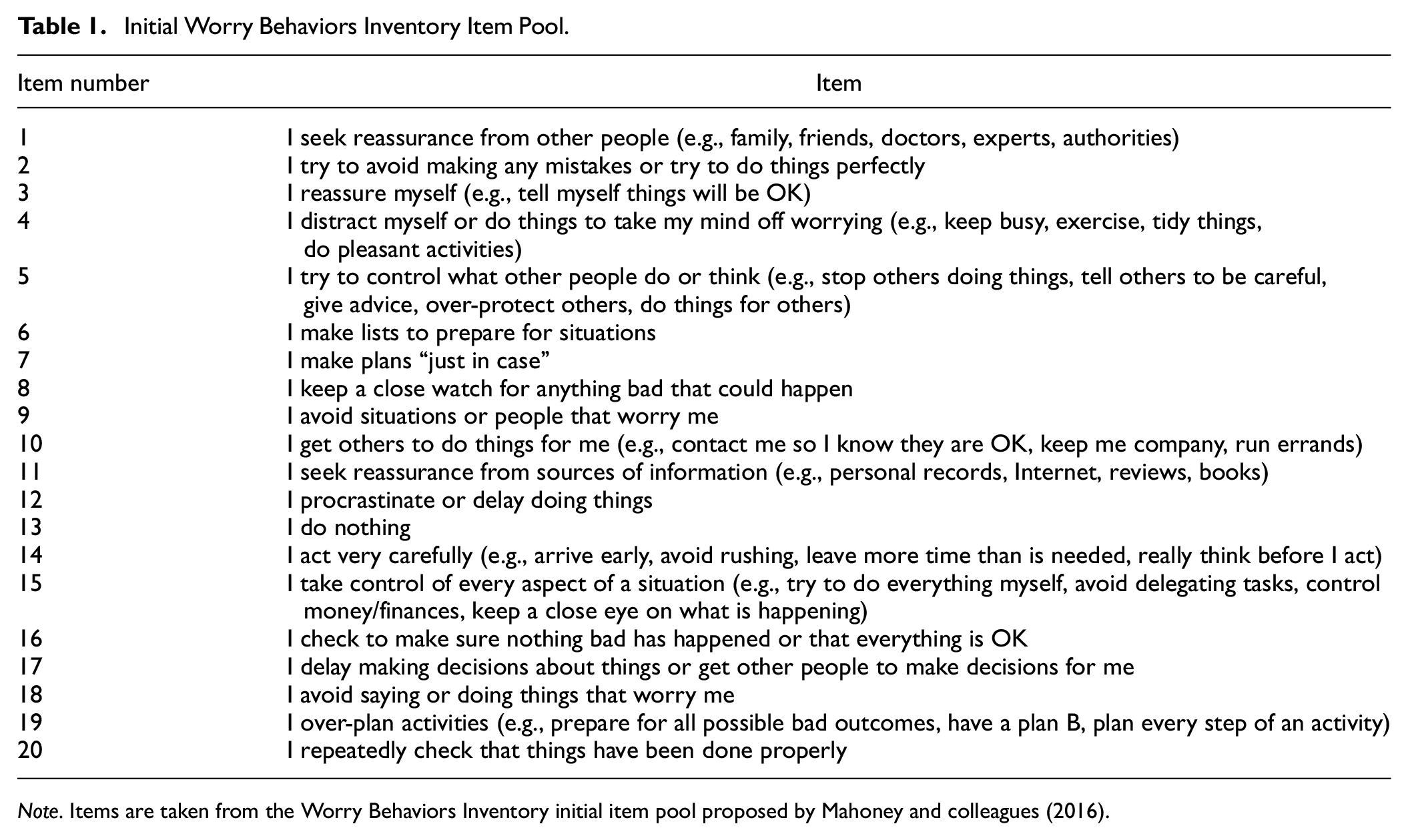
Note. Items are taken from the Worry Behaviors Inventory initial item pool proposed by Mahoney and colleagues (2016).
It is now known that the perinatal period represents a time of increased vulnerability to the onset and exacerbation of psychopathology (Munk-Olsen, & Agerbo, 2015), with up to 13% of perinatal women meeting criteria for depression (O’hara & Swain, 2009; Shorey et al., 2018; Woody et al., 2017) and 20.7% meeting criteria for one or more anxiety disorders (Fawcett et al., 2019). GAD, in particular, is a leading mental health concern during the perinatal period, affecting 4.1% to 5.7% of women (Dennis et al., 2017) and is associated with significant distress and impairment in mothers (Ali, 2018) and impaired social, emotional, and neurological development in offspring (Stein et al., 2012; Uguz et al., 2013). GAD is also highly comorbid with other mental health disorders such as depression (Grigoriadis et al., 2011; Misri et al., 2015), which often results in lower rates of remission, reduced quality of life (Misri & Swift, 2015), and decreased emotional availability in mothers and infants (Aran et al., 2021). While recent efforts have been made to characterize the nature of worry during the perinatal period (Goldfinger et al., 2020), the corresponding behavioral features of GAD have been largely overlooked. In response, Inness and colleagues (2022) conducted a qualitative study to gain insight into the behaviors reported by perinatal women with GAD. They found that perinatal women, like individuals with GAD in the general population, engage in various reassurance seeking, checking, controlling, overpreparation, and avoidance behaviors. However, the extent of these behaviors may not be adequately captured by the 10 retained items of the WBI. For example, items that reflect reassurance-seeking [i.e., item 1: “I seek reassurance from other people (e.g., family, friends, doctors, experts, authorities”)], controlling [i.e., item 15: “I take control of every aspect of a situation (e.g., try to do everything myself, avoid delegating tasks, control money/finances, keep a close eye on what is happening”)], and inflexible behaviors [i.e., item 14: “I act very carefully (e.g., arrive early, avoid rushing, leave more time than is needed, really think before I act”)] were omitted from the WBI (Mahoney et al., 2016). While these items were not representative of GAD behaviors in the general population (Mahoney et al., 2016), reassurance seeking (e.g., confirming baby-related decisions with partner, family, and medical professionals), controlling (e.g., reluctance to delegate baby care tasks), and inflexible behaviors (e.g., rigid parenting practices and routines) are prevalent and may be more relevant during the perinatal period (Inness et al., 2022).
As such, the primary objective of this study was to evaluate the initial 20-item pool proposed by Mahoney and colleagues (2016) to determine whether a divergent factor structure would emerge within a perinatal sample. We hypothesized that the factor structure and items retained within each factor would differ, given previous research to suggest that certain GAD behaviors (i.e., reassurance seeking, controlling, and inflexible behaviors) may be more relevant during the perinatal period (Inness et al., 2022). Given our prediction that the factor structure would differ, our secondary objective was to assess the internal consistency and construct validity of the Perinatal Revised WBI (i.e., WBI-PR), hypothesizing that the WBI-PR would demonstrate good internal consistency, converge with measures assessing similar constructs, and successfully discriminate between those with and without a GAD diagnosis. Finally, given that the implementation of behavioral criteria was suggested for DSM-5 (APA, 2013), our final objective was to evaluate the contribution of GAD behaviors to the prediction of GAD diagnoses, hypothesizing that the WBI-PR would significantly predict GAD diagnostic status both alone, and when controlling for existing GAD and depressive symptoms, which have been shown to explain significant variance in GAD diagnoses.
Methods
Participants
Two-hundred fourteen participants were recruited for this cross-sectional study. Sample size estimates were determined a-priori based on COSMIN guidelines for conducting exploratory factor analyses (EFAs; Mokkink et al., 2010). Participants were included if they were 18 years of age or older, fluent in English, and pregnant (n = 84) or between 0 and 6 months postpartum (n = 130). Participant’s ages ranged from 19 to 44 years (M = 31.95, SD = 4.23). The sample was predominantly married/common-law (94.4%), Caucasian (85.8%), and highly educated (89.2% with a college degree or higher), and roughly half were primiparous (51.8%). One-hundred forty-one participants (65.9%) met criteria for a principal diagnosis of GAD. The remaining participants (n = 73) had principal mood disorders (6.1%), other anxiety and related disorders (6.5%), or no current psychopathology (21.5%). See Table 2 for a breakdown of participant demographics and characteristics between those with and without a principal diagnosis of GAD.
Demographics and Characteristics of Participants with and without a Principal Diagnosis of Generalized Anxiety Disorder
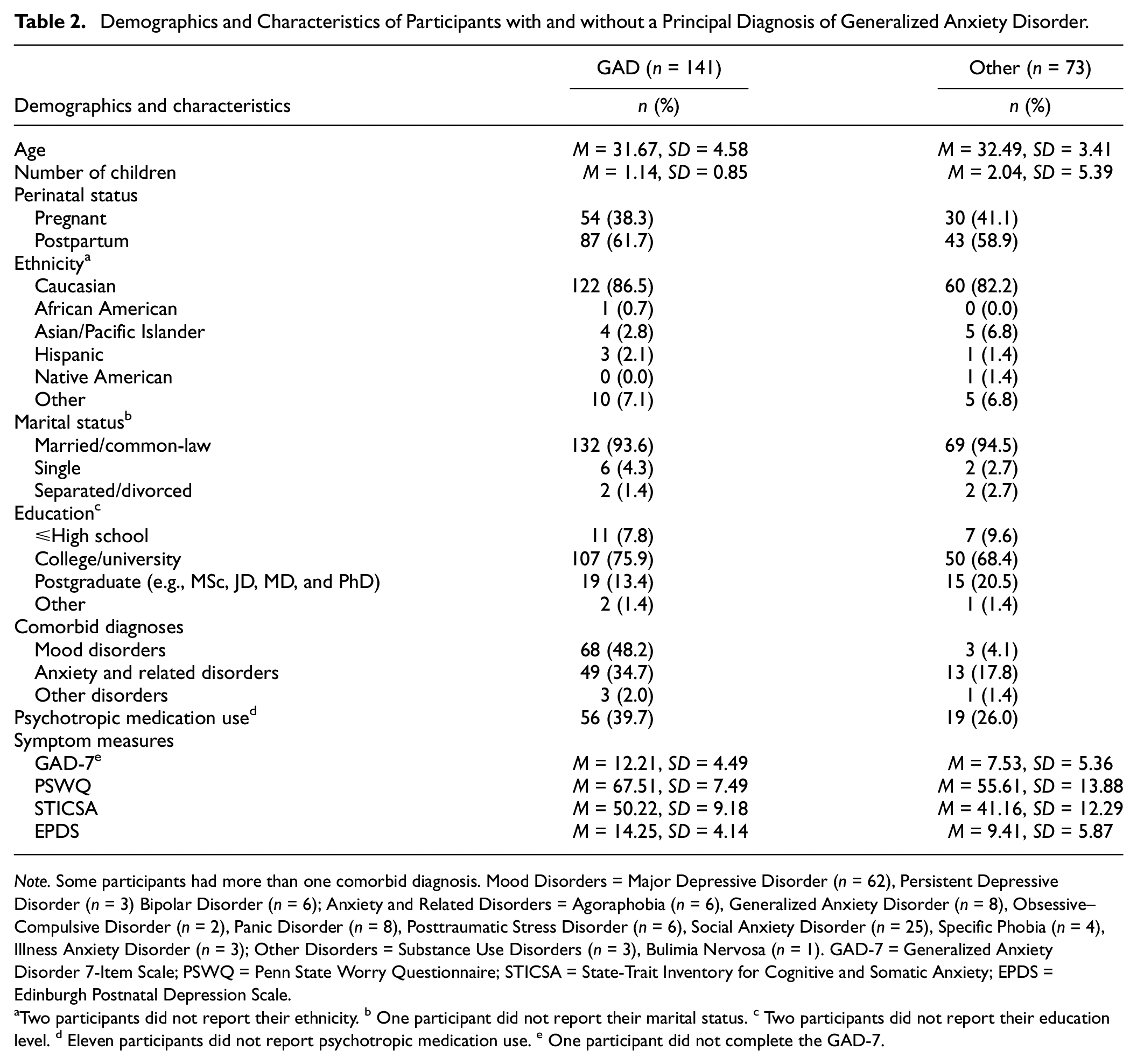
Note. Some participants had more than one comorbid diagnosis. Mood Disorders = Major Depressive Disorder (n = 62), Persistent Depressive Disorder (n = 3) Bipolar Disorder (n = 6); Anxiety and Related Disorders = Agoraphobia (n = 6), Generalized Anxiety Disorder (n = 8), Obsessive–Compulsive Disorder (n = 2), Panic Disorder (n = 8), Posttraumatic Stress Disorder (n = 6), Social Anxiety Disorder (n = 25), Specific Phobia (n = 4), Illness Anxiety Disorder (n = 3); Other Disorders = Substance Use Disorders (n = 3), Bulimia Nervosa (n = 1). GAD-7 = Generalized Anxiety Disorder 7-Item Scale; PSWQ = Penn State Worry Questionnaire; STICSA = State-Trait Inventory for Cognitive and Somatic Anxiety; EPDS = Edinburgh Postnatal Depression Scale.
Two participants did not report their ethnicity. b One participant did not report their marital status. c Two participants did not report their education level. d Eleven participants did not report psychotropic medication use. e One participant did not complete the GAD-7.
Procedures
A convenience sample of participants were recruited between June 2021 and January 2022 from the Women’s Health Concerns Clinic, St. Joseph’s Healthcare Hamilton (SJHH), an outpatient mental health facility (Caropreso et al., 2020), and through online (e.g., kijiji, Facebook, SJHH research page) and community (e.g., midwifery clinics) advertisements in the Hamilton and surrounding areas. Eligible and consenting participants were scheduled for a virtual research visit in which the Mini International Neuropsychiatric Interview for the DSM-5 version 7.0.2 (MINI-DSM-5; Sheehan et al., 1998) was administered to assess participants’ current diagnostic status. Diagnostic interviews were administered by PhD-level clinical psychology students, and diagnoses were confirmed by a licensed clinical psychologist. Participants then completed a brief battery of self-report measures (see “Measures” section), via Research Electronic Data Capture (REDCap), a web-based data management and storage system. All study procedures were approved by the Hamilton Integrated Research Ethics Board.
Measures
MINI-DSM-5
The MINI-DSM-5 is a brief, semistructured diagnostic interview used to assess a variety of psychiatric disorders in research and clinical settings, according to DSM-5 (APA, 2013) diagnostic criteria (version 7.0.2.; Sheehan et al., 1998). Participants in this study were assessed using the mood disorders, anxiety and related disorders, substance and alcohol use disorders, eating disorders, psychosis, and suicidality modules of the MINI-DSM-5. The MINI-DSM-5 is a reliable and valid assessment tool (Lecrubier et al., 1997; Sheehan et al., 1997) and has demonstrated good concordance with other diagnostic interviews, such as the Structured Clinical Interview for DSM-5 (APA, 2013; Spitzer et al., 1990).
WBI Item Pool
The initial WBI item pool consists of 20 unique items assessing avoidance and safety behaviors aimed at preventing, controlling, and avoiding worrying (see Table 1; Mahoney et al., 2016). Respondents are provided with the following instructions: “People can worry about everyday things, like their family, finances, work, health, the future, or minor things like being on time. This questionnaire concerns the sorts of things people do to prevent, control, or avoid worrying. Please select the number that best describes what you do generally.”
Items are scored on a 5-point Likert-type scale ranging from 0 (“none of the time”) to 4 (“all of the time”), with higher scores reflecting greater engagement in reported behaviors.
Penn State Worry Questionnaire
The Penn State Worry Questionnaire (PSWQ) is a 16-item self-report measure that assesses the tendency to worry (Meyer et al., 1990). Items are scored on a 5-point scale ranging from 1 (“not at all typical of me”) to 5 (“very typical of me”), with higher scores reflecting greater pathological worry. A cut-off score of 62 or higher has been suggested for determining a probable GAD diagnosis (Behar et al., 2003). The PSWQ has demonstrated excellent internal consistency and validity across various populations (Brown et al., 1992) and has been validated for use in perinatal samples (Voegtline et al., 2021). The internal consistency of the PSWQ in the current sample was α = 0.91.
Generalized Anxiety Disorder 7-Item Scale
The Generalized Anxiety Disorder 7-Item Scale (GAD-7) is a 7-item self-report measure that assesses GAD symptom severity over the previous two weeks (Spitzer et al., 2006). Items are measured on a 4-point scale ranging from 0 (“not at all”) to 3 (“nearly every day”). A cut-off score of 10 or higher with sensitivity of 89% and specificity of 82% has been suggested for detecting a probable diagnosis of GAD (Spitzer et al., 2006). The GAD-7 has also been validated for use in perinatal samples (Simpson et al., 2014). The internal consistency of the GAD-7 in the current sample was α = 0.88.
State-Trait Inventory for Cognitive and Somatic Anxiety
The State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA) is a 21-item self-report scale that assesses cognitive and somatic components of anxiety (Ree et al., 2008). The STICSA is comprised of a state scale that measures individuals’ current anxiety symptoms, and a trait scale that assesses one’s general proneness to anxiety. In this study, only the trait scale of the STICSA was used. Items are scored on a 4-point scale ranging from 1 (“not at all”) to 4 (“very much so”). The STICSA has demonstrated excellent validity and reliability (Grös et al., 2007). A cut-off score of 43 or higher on the STICSA has been suggested for detecting a probable anxiety disorder (Van Dam et al., 2013). The STICSA has been validated for use in clinical samples of adults with anxiety disorders (Grös et al., 2007), although not explicitly in perinatal samples. The internal consistency of the STICSA in this sample was α = 0.89.
Edinburgh Postnatal Depression Scale
The Edinburgh Postnatal Depression Scale (EPDS) is a 10-item self-report measure that assesses symptoms of depression during the perinatal period (Murray & Cox, 1990). Items are scored on a 4-point scale ranging from 0 to 3, with higher scores reflecting greater depressive symptomatology. The EPDS has demonstrated good sensitivity and specificity for a diagnosis of MDD. Cut-off scores of 15 and 13 or higher have been suggested for detecting a probable diagnosis of MDD during pregnancy and the postpartum period, respectively (Matthey et al., 2006). The internal consistency of the EPDS in this sample was α = 0.87.
Statistical Analyses
Structure
EFAS were used to assess the structure of the initial WBI item pool (Mahoney et al., 2016). Prior to EFA, data were examined for normality and bivariate correlation matrices inspected. Bartlett’s test of sphericity and the Kaiser–Meyer–Olkin measure of sampling adequacy were performed to determine that the data were appropriate for factor analysis. Items with communalities <0.4 were removed prior to factor analysis, as low communalities indicate that the item has little in common with other items and can distort outcomes (Fabrigar et al., 1999). EFAS were then conducted using principal axis factoring with oblique (promax) rotation (Watkins, 2018). Scree plots (Cattell, 1966), Eigenvalue >1 (Braeken & van assen, 2016; Kaiser, 1974) and Revised Velicer’s Minimum Average Partial (MAP) test (Velicer et al., 2000) were used to determine the number of factors to retain. Items with loadings >0.4 were retained and factorially complex items (i.e., items that loaded onto multiple factors) were omitted (Watkins, 2018).
Internal Consistency
Cronbach’s alpha was used to assess the internal consistency of the WBI-PR.
Construct Validity
Correlations between the WBI-PR and PSWQ (worry), GAD-7 (GAD symptoms), STICSA (anxiety), and EPDS (depression) were calculated. The PSWQ and GAD-7 were used as indicators of convergent validity as they are commonly used to assess GAD symptoms (Behar et al., 2003; Fresco et al., 2003; Spitzer et al., 2006). The STICSA and EPDS were used as indicators of discriminant validity, as they measure similar yet distinct constructs. Although cognitive and somatic components of anxiety exist in GAD, worry is generally considered distinct from other cognitive aspects of anxiety (Holaway et al., 2006) and the STICSA is not a measure of GAD per se. The STICSA was chosen as a measure of discriminant validity to assess how specific the WBI-PR is to GAD, as opposed to anxiety symptoms more broadly. Steiger’s z test was used to assess convergent validity by examining whether the WBI-PR was more strongly associated with measures of worry and GAD symptoms than anxiety and depression. To assess discriminant validity, t-tests were performed to determine whether cases of GAD scored significantly higher on the WBI-PR and subscales than noncases.
Criterion Validity
To assess the contribution of GAD behaviors to the prediction of GAD diagnoses, a logistic regression was performed to evaluate how well the WBI-PR, alone, predicted GAD diagnostic status. A hierarchical logistic regression was then conducted to evaluate how well the WBI-PR predicted GAD diagnostic status, after controlling for existing GAD (as measured by the GAD-7) and depression (as measured by the EPDS) symptoms.
Results
Structure
Factorability of the 20 items was examined prior to EFAs. Skew values were between 0.69 to −0.89 and kurtosis values were between 0.22 and −0.90, suggesting that the data were normally distributed. Examination of the bivariate correlation matrix suggested that 15 of 20 items were correlated at 0.3 or greater with at least one other item, indicating reasonable factorability (Watkins, 2018). The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.78, which is greater than the recommended value of 0.7 (Watkins, 2018). Bartlett’s test of sphericity was significant, χ2 (190) = 940.97, p < .001. Nine of 20 items had communalities <0.4 and were removed. Factorability of the remaining 11 items was reassessed. Ten of 11 items were correlated at 0.3 or greater with at least one other item. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.81, and Bartlett’s test of sphericity was significant, χ2 (55) = 598.17, p < .001, suggesting that the remaining 11 items were appropriate for factor analysis.
Rotated factor loadings from the pattern matrix are shown in Table 3. A two-factor structure was preferred based on MAP, Eigenvalue >1, and Scree plot criteria (Eigenvalues: 3.65 and 1.64). The two-factor structure revealed that one item (item 9) did not load onto either factor (item loadings: 0.32 and 0.39). The two-factor solution explained 48.1% of the variance. Factor 1 (Safety Behaviors) included seven items and explained 33.2% of the variance and Factor 2 (Avoidance) included three items and explained 14.9% of the variance. The correlation between the two factors was small and positive, 0.20. Although the factor structure of the scale and number of items indexed by each factor was consistent with the original WBI (Mahoney et al., 2016), some of the retained items within each factor differed and thus, remaining analyses were performed on the WBI-PR.
Exploratory Factor Analysis: Factor Loadings from the Rotated Pattern Matrix Solution
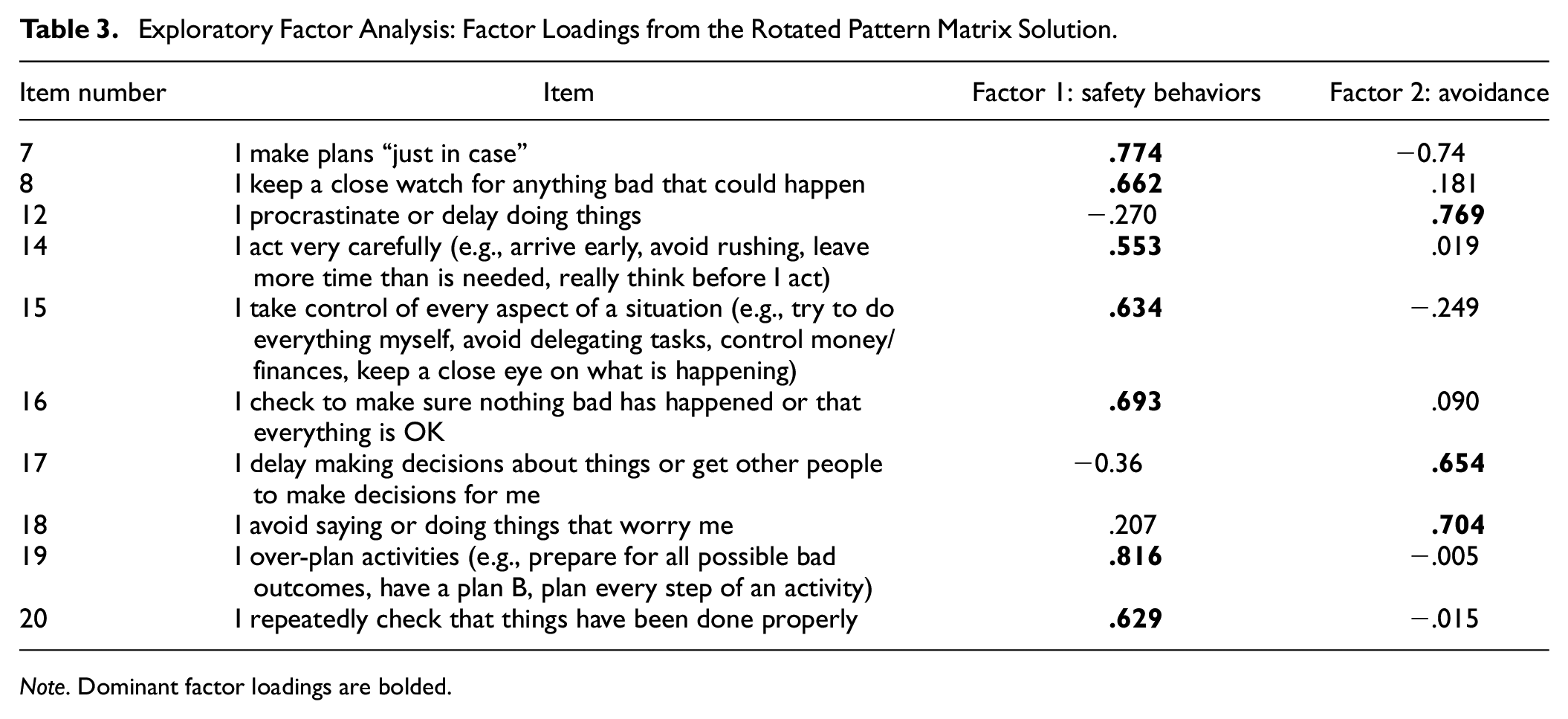
Note. Dominant factor loadings are bolded.
Internal Consistency
Internal consistency of the WBI-PR was α = 0.81 for full scale, and α = 0.86 and α = 0.73 for the Safety Behaviors and Avoidance subscales, respectively, suggesting acceptable internal consistency (Tavakol & Dennick, 2011).
Construct Validity
Participants who completed all convergent and discriminant measures were included in this analysis (n = 213). All correlations were positive and statistically significant (all p values ≤ .013); see Table 4 for correlations between WBI-PR total and subscale scores and measures of convergent and discriminant validity. As hypothesized, the WBI-PR was more strongly associated with measures of GAD symptoms (GAD-7; z = 3.06, p = .001) and worry (PSWQ; z = 3.26, p < .001) than depression (EPDS). However, contrary to hypotheses, the WBI-PR was not more strongly associated with measures of GAD symptoms (z = −1.37, p = .914) and worry (z = −0.04, p = .517) than anxiety (STICSA). The same pattern of results was observed for the Safety Behaviors subscale (GAD-7 vs EPDS z = 3.09, p = .001; PSWQ vs EPDS z = 3.45, p < .001; GAD-7 vs STICSA z = −0.39, p = .654; PSWQ vs STICSA z = 1.06, p = .144). Surprisingly, and in contrast to our hypotheses, the Avoidance subscale was not more strongly associated with measures of GAD symptoms or worry than depression (GAD-7 vs EPDS, z = 0.77, p = .219; PSWQ vs EPDS z = 0.35, p = .363) or anxiety (GAD-7 vs STICSA, z = −2.46, p = .993; PSWQ vs STICSA, z = −2.48, p = .993).
Correlation Matrix between WBI-PR and Subscales and Measures of Convergent and Discriminant Validity
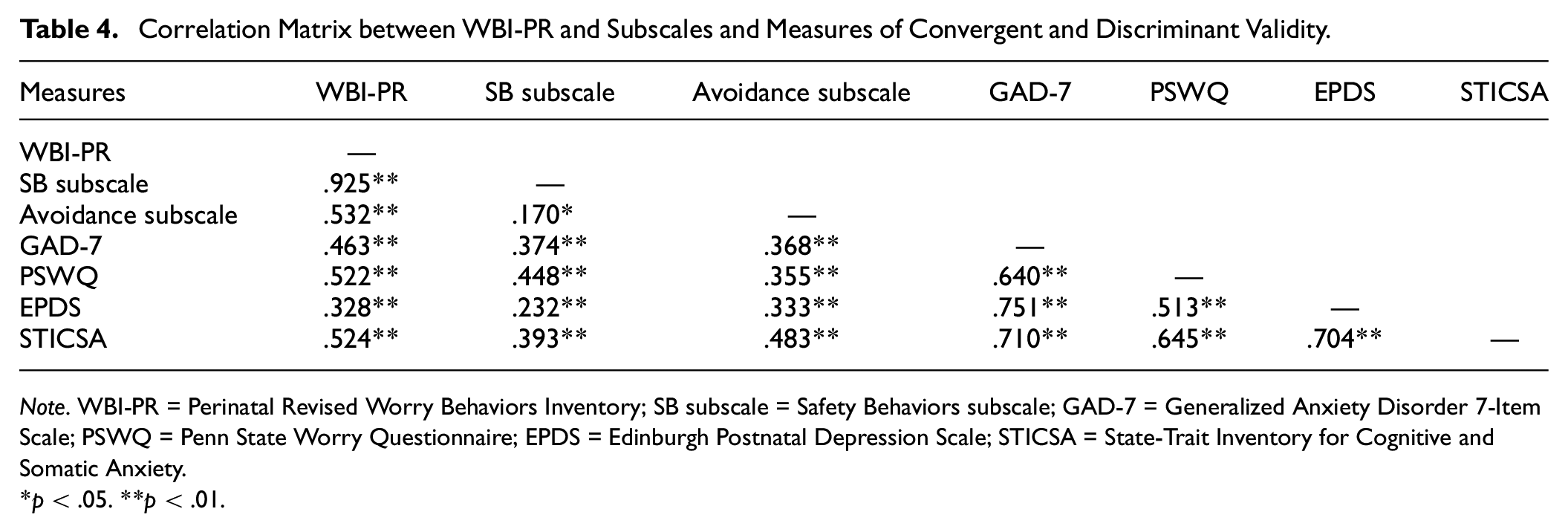
Note. WBI-PR = Perinatal Revised Worry Behaviors Inventory; SB subscale = Safety Behaviors subscale; GAD-7 = Generalized Anxiety Disorder 7-Item Scale; PSWQ = Penn State Worry Questionnaire; EPDS = Edinburgh Postnatal Depression Scale; STICSA = State-Trait Inventory for Cognitive and Somatic Anxiety.
p < .05. **p < .01.
Levene’s tests suggested that the equality of variances assumption between those with and without a diagnosis of GAD was met for the WBI-PR and subscales (F values = 0.11 to 0.77, all p values > .38). Independent samples t-tests indicated that participants with a principal GAD diagnosis scored significantly higher on the WBI-PR (M = 24.43, SD = 6.37) than participants without a principal GAD diagnosis (M = 19.68, SD = 6.67, t (212) = 5.09, p < .001, g = 0.73). Similarly, participants with principal GAD scored significantly higher on the Safety Behaviors (M = 18.15, SD = 5.55 vs M = 14.64, SD = 5.86, t (212) = −4.29, p <.001, g = 0.62) and Avoidance (M = 6.29, SD = 2.58 vs M = 5.04, SD = 2.58, t (212) = −3.36, p < .001, g = 0.48) subscales than participants without a principal GAD diagnosis.
Criterion Validity
Prior to logistic regressions, normality of the data were inspected. Skew and kurtosis values of the WBI-PR, GAD-7, and EPDS were between ±1, which is considered normal. There were no multivariate outliers according to Mahalanobis distance (all p values > .001). The logistic regression model, with GAD behaviors (i.e., WBI-PR total scores) predicting GAD diagnostic status, was statistically significant χ2(1) = 23.95, p < .001. The model explained 14.6% (Nagelkerke R 2) of the variance in GAD diagnoses and correctly classified 71% of cases, where greater endorsement of GAD behaviors was associated with increased likelihood of a principal GAD diagnosis. Regarding the hierarchical regression, with GAD behaviors (i.e., WBI-PR total scores) predicting GAD diagnostic status after controlling for GAD (i.e., GAD-7 total scores) and depression (i.e., EPDS total scores) symptoms, Model 1 was statistically significant χ2(2) = 48.66, p < .001. The model explained 28.3% (Nagelkerke R 2) of the variance in GAD diagnoses and correctly classified 78.9% of cases, where greater GAD and depression symptomatology was associated with greater likelihood of a principal GAD diagnosis. When GAD behaviors (i.e., WBI-PR total scores) were added in block two, both the overall regression model (χ2(3) = 54.38, p < .001) and block (χ2(1) = 5.72, p = .017) were statistically significant. Model 2 explained 31.2% (Nagelkerke R 2) of the variance in GAD diagnoses, correctly classifying 76.5% of cases. This suggests that GAD behaviors (as measured by the WBI-PR) significantly predict primary GAD diagnostic status over and above existing GAD and depression symptoms; however, the contribution is relatively small, accounting for an additional 2.9% of the variance in GAD diagnoses.
Discussion
Perinatal women with GAD engage in comparable problematic behaviors to those with GAD in the general population (Inness et al., 2022). However, the extent of these behaviors may not be adequately captured by existing GAD behavior measures. This study examined the initial WBI item pool proposed by Mahoney and colleagues (2016) and the psychometric properties of the resulting WBI-PR in a perinatal sample.
EFA led to the emergence of a two-factor solution, indexed by seven Safety Behavior and three Avoidance items. Ten items were omitted from the WBI-PR (items: 1, 2, 3, 4, 5, 6, 9, 10, 11, and 13; see Table 1). Some of the omitted items, such as item 3 (“I reassure myself”), 4 (“I distract myself”), and 13 (“I do nothing”), may reflect more useful attempts to cope with worry, as those with GAD have been found to use less distraction and reappraisal strategies than nonanxious controls (Coles & Heimberg, 2005). Furthermore, behaviors such as distraction, self-reassurance, and doing nothing in response to worries have not been cited in perinatal women with GAD (Inness et al., 2022). Conversely, items that reflect situational avoidance (item 9: “I avoid situations or people that worry me”) and excessive reassurance and information seeking (item 1: “I seek reassurance from other people”; item 11: “I seek reassurance from sources of information”) have been documented in perinatal women with GAD (Inness et al., 2022) but were, nonetheless, omitted from the WBI-PR. It is possible that these omitted items may not be specific to GAD, as we might expect all mothers to seek confirmation of parenting and baby-related decisions, to some extent.
Interestingly, while the factor structure and number of items indexed by each factor was consistent with the WBI, some of the retained items differed between the WBI and WBI-PR. Namely, items 5 (“I try to control what other people do or think”), 9 (“I avoid situations or people that worry me”), and 11 (“I seek reassurance from sources of information”) were replaced by items 15 (“I take control of every aspect of a situation”), 14 (“I act very carefully”), and 12 (“I procrastinate or delay doing things”). While controlling what others do (item 5), researching (item 11), and avoiding anxiety-evoking situations (item 9) have been documented in perinatal women with GAD, so too have behaviors that reflect attempts to “control situations” (item 15; e.g., overseeing and difficulty delegating baby care tasks) and “act carefully” (item 14; e.g., inflexible parenting practices; Inness et al., 2022). Notably, controlling behaviors may be more relevant in maternal populations, as over-protective behaviors have been documented in mothers with GAD outside of the perinatal period as well (Bogels & Melick, 2004; Kalomiris & Kiel, 2016). Procrastination and delayed decision-making have also been cited in GAD (Andrews et al., 2010; Robichaud, 2013; Robichaud et al., 2019). Other retained items such as repeated checking (item 16: “I check to make sure nothing bad has happened or that everything is OK”; item 20: “I repeatedly check that things have been done properly”), over-preparation (item 19: “I over-plan activities”; item 7: “I make plans just in case”) and hypervigilance behaviors (item 8: “I keep a close watch for anything bad that could happen”) have been observed in those with GAD both in the general population (Mahoney et al., 2016) and in perinatal samples (Inness et al., 2022). Perinatal women with GAD in particular, have been found to excessively check their sleeping babies and regularly oversee baby-care to ensure that tasks are completed correctly (Inness et al., 2022). They also report preparing for outings with their babies well in advance, as well as thinking through various worrisome scenarios. Similarly, many perinatal women with GAD report closely watching their infants. As such, the retained items of the WBI-PR were easily interpretable and were consistent with qualitative studies of GAD behaviors during the perinatal period.
The WBI-PR and Safety Behaviors and Avoidance subscales demonstrated acceptable internal consistency (Tavakol & Dennick, 2011) and was comparable to that observed by Mahoney and colleagues (2016) in their initial validation of the WBI.
The WBI-PR was significantly and positively correlated with measures of GAD symptoms, worry, anxiety and depression, supporting convergent validity of the scale. In support of our hypotheses, the WBI-PR was more strongly associated with measures of GAD symptoms and worry than depression. Contrary to our hypotheses, the WBI-PR was not more strongly associated with measures of GAD symptoms and worry than anxiety. However, this finding is perhaps unsurprising when considering that various avoidance (e.g., avoiding feared situations) and safety behaviors (e.g., checking and reassurance seeking) are central to the conceptualization of many anxiety and related disorders (Barlow, 2002; McManus et al., 2008; Salkovskis et al., 1999; Scarella et al., 2019). The same pattern of results was observed for the Safety Behaviors subscale but not for the Avoidance subscale. While the Avoidance subscale was significantly and positively correlated with measures of GAD symptoms and worry, it was more strongly associated with measures of anxiety and depression. Although further research is necessary, it may be that avoidance behaviors are not specific to GAD but common across psychiatric disorders, as avoidance is a core diagnostic criterion of all anxiety and related disorders (APA, 2013) and has been conceptualized as central to the maintenance of depression (Trew, 2011). This finding is also consistent with Mahoney and colleagues (2016) initial validation of the WBI, in which they found that the Avoidance subscale of the WBI was as strongly correlated with symptoms of depression and anxiety (i.e., social anxiety and panic disorder) as it was with measures of GAD. Furthermore, our findings showed that participants with a principal GAD diagnosis scored significantly higher on the WBI-PR and Safety Behaviors and Avoidance subscales than participants without a principal GAD diagnosis, providing preliminary evidence of discriminant validity.
Consistent with our hypotheses, logistic regression analyses suggested that GAD behaviors significantly predicted GAD diagnostic status both alone and over and above GAD and depression symptoms. However, the relative contribution of GAD behaviors to the prediction of GAD diagnostic status when controlling for GAD and depression symptoms was relatively small, accounting for an additional 2.9% of the variance in principal GAD diagnoses. These findings are consistent with research on GAD behaviors in both perinatal samples and in the general population, showing that GAD behaviors are significantly positively correlated with cognitive processes of GAD (e.g., excessive worry, cognitive avoidance; Mahoney, Hobbs, Williams, Andrews, & Newby, 2018; Marcotte-Beaumier et al., 2022) and depressive symptoms (Green et al., 2021; Mahoney et al., 2016) and, while small, contribute unique variance to GAD diagnoses (Brown & Tung, 2018; Marcotte-Beaumier et al., 2022). Item-level analyses of the WBI-PR may lead to the identification of particularly robust items that could be converted into and improve specificity of GAD diagnostic criteria.
Limitations and Future Directions
There are several limitations of this study. First, while our sample size was appropriate for all analyses conducted, our study was not appropriately powered to conduct a confirmatory factor analysis (CFA). While EFA is the preferred method of analysis when relations among the variables are unknown, as is the case in this study, EFA provides weaker evidence of structural validity than CFA (Merenda, 1997; Streiner et al., 2015). As such, no causal inferences can be made about the observed variables and the underlying latent constructs of the WBI-PR until CFAs are conducted. Furthermore, while the WBI-PR demonstrated acceptable internal consistency, relying solely on internal consistency to assess reliability can be problematic, as single administrations of a scale fail to acknowledge other sources of variance that can influence reliability (Streiner et al., 2015). As such, without examining the stability of the WBI-PR between administrations, it is possible that the scores on the WBI-PR are not representative of participant’s true GAD behaviors but due to other testing artifacts (e.g., the environment in which they completed the measure). Thus, future studies should evaluate the test–retest reliability of the WBI-PR. Furthermore, while the STICSA has been validated in clinical samples of adults with anxiety disorders (Grös et al., 2007) and used in perinatal samples (Furtado et al., 2021; Green et al., 2020, 2021), it has not been validated for use in perinatal samples, which may affect the interpretation of results. For example, certain items on the STICSA (e.g., “I have trouble remembering things”; “I feel dizzy”; “My muscles are tense”) may be over-endorsed, as various cognitive and physiological changes occur during the perinatal period (Henry & Sherwin, 2012; Soma-Pillay et al., 2016) that may not be related to anxiety per se. Our study sample also consisted of predominantly highly educated, Caucasian women. As such, our results may not generalize to perinatal women from diverse sociodemographic backgrounds. Finally, while beyond the scope of this study, future research should evaluate the WBI-PR’s responsivity to change throughout treatment, which is crucial to establishing the clinical utility of a measure.
Conclusion
This study evaluated the initial WBI item pool (Mahoney et al., 2016), which led to the emergence of the WBI-PR, a two-factor (Safety Behaviors and Avoidance), 10-item scale. We found initial evidence of reliability, construct validity, and predictive utility of the WBI-PR. Continued use of the WBI-PR by perinatal clinicians and researchers is important for determining the contribution of GAD behaviors to GAD pathology, as well as the significance of GAD behaviors in treatment planning and outcomes. Item-level analyses of the WBI-PR may provide insight into behaviors that are most representative and predictive of GAD diagnoses.
Footnotes
Acknowledgements
The authors would like to extend our sincere gratitude to Hannah Armstrong, research assistant who helped with this project, as well as to the perinatal women who generously volunteered their time to participate in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author (BI) is supported by the Canadian Institutes of Health Research Doctoral Research Award: Canada Graduate Scholarships (funding reference no. 181578).
Methodological Disclosure
The authors report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Availability of Data and Materials
The data set for this study is available from the corresponding author upon reasonable request.