
Abstract
Nurses face significant physical demands during patient care, leading to high rates of musculoskeletal disorders (MSDs) among nurses in long-term care. Exoskeletons demonstrate promise in supporting nurses and nurse managers with MSDs; however, social contextual factors are crucial to their design and implementation. Through thematic analysis of 17 semi-structured interviews, this paper reveals social contextual factors important to exoskeleton use among nurses and nurse managers in long-term care. Participants expressed concerns about workplace discrimination, co-worker perceptions of their capabilities, and patient confidence. Our findings highlight the need for supportive organizational cultures and open communication channels. Recommendations include in-depth systems analysis to assess exoskeleton feasibility and efficacy, involving input from frontline nurses/managers, management, and patients. These findings can aid human factors and ergonomics (HF/E) experts in balancing social contextual factors and other work system elements to design work system contexts and exoskeletons that promote optimal outcomes in long-term care settings.
Introduction
The nursing profession in the United States (U.S.) confronts formidable challenges stemming from the physical demands inherent in patient care, including tasks such as lifting, handling, and transferring patients. These demands significantly contribute to a high prevalence of chronic and acute pain, discomfort, and potential early retirement among nurses due to the development of musculoskeletal disorders (MSDs; Tang et al., 2022). The growing demand for healthcare services from an aging nursing population compounds this issue (Naserian et al., 2024) and exacerbates the severity of the nationwide shortage of registered nurses (Gatchel, 2018). In response to these challenges, emerging technologies such as exoskeletons have shown promise in assisting individuals with physically strenuous tasks, particularly in controlled laboratory studies (De Bock et al., 2021).
Exoskeletons refer to wearable devices designed to augment or support human physical capabilities, often by providing mechanical assistance to the user’s limbs or torso. While traditionally designed for medical and military applications, exoskeleton technology is now being adapted for occupational use, offering potential relief from physical strain in various sectors including manufacturing (Hussain et al., 2021), construction (Kim et al., 2019), and healthcare (Tröster et al., 2020). In recent years, exoskeletons have been gradually introduced in specific work contexts such as manual material handling and automotive assembly (Bogue, 2018). However, within healthcare, particularly in long-term care facilities, few studies have explored the social implications of implementing exoskeletons.
Moreover, there exists a notable gap in the development of exoskeletons tailored to accommodate the needs of non-able-bodied individuals, such as those with pre-existing MSDs. While many initiatives focus on injury prevention, few efforts are directed towards assisting healthcare providers who are already injured or disabled. Thus, there is a critical need to design exoskeletons that cater to a broader range of workers with different combinations of functional limitations. One approach is to better understand the work system in which the exoskeleton is to be used. Work systems describe the interacting components which shape contextual employee and organizational processes and outcomes. Work system components include people, tasks, tools/technology, organizational factors, physical environment factors, and macro-level external environment factors (Carayon et al., 2006; Holden et al., 2013). This study specifically seeks to examine the social contextual factors influencing the acceptance, adoption, and use of exoskeletons for MSD management among nurses and nurse managers in long-term care settings. Acceptance, adoption, and use are three distinct yet interrelated stages crucial to the successful implementation of exoskeleton technology. Acceptance refers to the initial positive attitude and willingness of potential users to consider using exoskeletons (Bacalso et al., 2023; Peek et al., 2014). Adoption involves the decision to begin using the exoskeleton technology, either at the individual level (end users) or the organizational level (management decisions). Successful adoption often requires support from management, appropriate training, and alignment with organizational goals and workflows (Branko et al., 2023). Use is the sustained and effective utilization of exoskeletons in daily work activities (Karaosmanoglu et al., 2021) and may be shaped by individual factors, organizational factors, and social contextual factors.
Exoskeleton research in various domains has begun to articulate how social contextual factors, including workplace relationships, cultural norms, and attitudes toward technology, may play a crucial role in shaping users’ acceptance and adoption of exoskeletons (Turja et al., 2022). Siedl and Mara (2021) conducted a field study among logistics workers and found that perceived physical relief and usefulness significantly influenced acceptance. Workers who felt more strain relief and perceived the exoskeleton as useful were more likely to accept the technology. This study emphasizes the role of perceived benefits in fostering positive attitudes towards exoskeletons, suggesting that demonstrating tangible benefits can enhance acceptance. Gonsalves et al. (2023) explored the impact of social influence on construction workers’ intention to use back-support exoskeletons. Their findings indicate that employer support and requirements played a crucial role in adoption. Contrary to expectations, peer and supervisor attitudes had a minimal impact, while the subjective norm (the perceived social pressure to perform or not perform the behavior) significantly influenced workers’ intention to adopt exoskeletons. This underscores the importance of organizational support and policies in driving adoption at the individual level. Elprama et al. (2020) studied industrial workers and highlighted the role of social processes in shaping the intention to use exoskeletons. Their research points out that workplace relationships, cultural norms, and attitudes towards technology are critical in maintaining the use of exoskeletons over time. Workers’ willingness to continue using the technology was associated with their initial self-efficacy and perceived usefulness, suggesting that continuous training and positive reinforcement can promote long-term use.
Our research aims to identify a range of social contextual factors important to users’ acceptance, adoption, and use of exoskeleton technology in nurses and nurse managers’ daily work and propose strategies to maximize acceptance and effectiveness. By investigating these research questions, this study not only informs the design of exoskeletons tailored to nurses with MSDs in long-term care settings but also contributes to a broader understanding of the social contextual factors pertinent to the design of work systems into which exoskeletons may be integrated. The findings may enable HF/E experts to balance social contextual factors and other elements of the work system and foster the adoption and effective use of exoskeletons that promote optimal outcomes for all individuals in long-term care settings.
Methods
Study Design
We conducted a thematic analysis of 30 semi-structured qualitative interviews to identify themes related to social contextual factors important to exoskeleton design and implementation for nurses with MSDs working in long-term care settings. This study was approved by the University of Virginia’s Institutional Review Board for Social and Behavioral Sciences (Protocol Number 5098). Data was collected from electronic surveys and virtual interviews with eligible participants across the U.S. The electronic surveys inquired about the location and frequency of participants’ acute and/or chronic pain. The surveys were administered via email prior to each interview and the responses guided discussion during the semi-structured interviews. Certified nursing assistants (CNAs), registered nurses (RNs), and nursing managers were recruited via online advertisement or on-site recruitment from nursing homes and long-term care facilities nationwide.
Sampling and Eligibility Criteria
Participants were recruited via online advertisement or through on-site recruitment at nursing homes and long-term care facilities nationwide. Interested individuals contacted the research team via the telephone number and email address listed on recruitment posters and social media posts. Snowball sampling was conducted via participant phone calls and emails. Eligibility requirements dictated that participants were at least 18 years old, employed as a CNA, RN, or nursing manager at a long-term care facility, experience either an acute injury or an injury that has led to chronic pain in one or more part of the body, and reside primarily within the U.S. Eligible individuals were verbally consented over Zoom.
Data Collection
Electronic Surveys
Before conducting interviews, electronic surveys were sent to perspective interviewees via email. These surveys, derived from the Nordic Musculoskeletal Questionnaire, focused on gauging the intensity, frequency, and duration of musculoskeletal discomfort across various body regions. When completed, the responses from these surveys were used to guide the semi-structured interview discussions. In total, 28 responses were collected (two participants declined to complete the survey).
Interviews
We conducted 30 virtual interviews on Zoom spanning from November 2022 to December 2022, each lasting between 45 and 60 min. These interviews utilized a qualitative descriptive approach (Sandelowski, 2000, 2010), aiming to gather a comprehensive overview of the lived experiences, unmet needs, preferences, perceptions, and social contextual factors of nurses and nursing managers working in nursing homes and other long-term care facilities. Interview questions systematically explored all elements of the work system; however, this analysis focuses on the social contextual factors. During interviews, participants viewed a video demonstration of an active, full body exoskeleton during heavy lifting tasks. After, they shared their thoughts and concerns. Interviews were audio-recorded and transcribed verbatim for analysis.
Data Analysis
Descriptive statistics were calculated using the electronic survey data and demographic data captured during the semi-structured interviews (Table 1). Data from the semi-structured interviews were then analyzed according to Braun and Clarke’s (2006) method for thematic analysis. A qualitative codebook was inductively developed from the interview data by a core team of four research assistants trained in qualitative methods with oversight by the senior author. Initial codes were identified through an open coding process across six interview transcripts. Code titles and definitions were iteratively refined until all research assistants agreed that the codebook accurately and completely captured all data relevant to our research question. The codebook was then presented to the senior author for final approval. The finalized codebook guided research assistants in coding all 30 interview transcripts using NVivo® qualitative data analysis software (QSR International PTY LTD. Version 12, 2020). Our team met weekly for consensus building and to ensure data trustworthiness. A transcript was considered reconciled when data was coded in full agreement across all four coders. Discrepancies unresolved during weekly meetings were raised to the senior author.
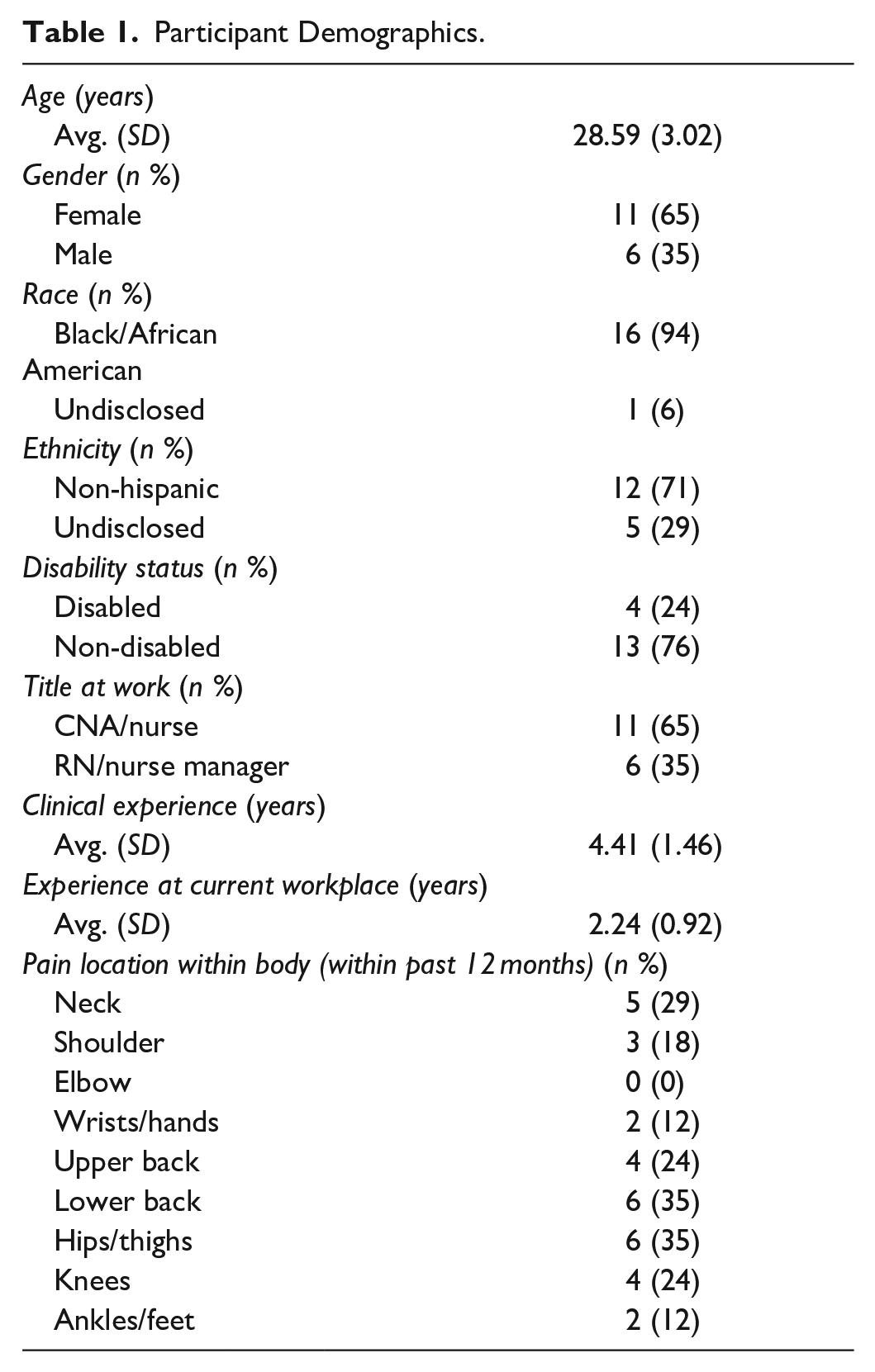
Participant Demographics.
After obtaining full agreement across nine consecutive transcripts, the senior author allowed the team to code in pairs of two for the remainder of the analysis. Coding pairs met weekly to build consensus across their assigned transcripts, while continuing to meet weekly with the full coding team to discuss coding applications. Coding partners rotated weekly until all transcripts were analyzed. When complete, codes were grouped into overarching themes identified through iterative discussions with the core research team.
During the analysis our team found inconsistencies in the participants’ survey and interview responses. Due to these discrepancies, we performed an internal quality audit and omitted the data of participants suspected of falsifying information. Participants’ data were excluded if they (1) provided two different responses when asked to state their age in the interview and in the musculoskeletal survey or (2) submitted multiple musculoskeletal surveys with varied responses for their age and/or where they experience pain in the body. As a result, our findings report on themes specific to social contextual factors surrounding exoskeleton use in long-term care across the remaining 17 participants.
Results
Participant Characteristics
All qualified participants (n = 17) were employed as nurses or nurse managers in long term care facilities and experienced chronic or acute musculoskeletal pain. Of these participants, 35% were male, 94% were Black/African American, and 24% identified as disabled. Participants held an average of 4.41 years of clinical experience with an average of 2.24 years at their current long-term care facility. Of the 17 qualified pre-interview survey respondents, 29% experienced neck pain, 24% experienced knee pain, 24% experienced upper back pain, 35% experienced lower back pain, and 35% experienced hip and thigh pain.
Overview of Themes
Themes spanned a range of social contextual factors important to successful exoskeleton design and implementation for nurses with MSDs working in long-term care settings, namely (1) comfortabilities discussing pain- or disability-related needs with managers, (2) coworker perceptions of their capabilities, and (3) patient confidence in their professional abilities.
Discussing Needs with Managers
While some participants reported that they would be comfortable talking to their manager about disclosing pain-related needs or exoskeleton-related concerns to managers, many participants reported feeling uncomfortable disclosing their needs due to fears of being perceived as lazy, experiencing workplace discrimination, or being “pitied.” One participant expressed concerns that managers may incorrectly assume they are lying about their pain to receive lighter duties: “It just feels like something that they’d put at the back of their minds as a con” (P12).
This participant further described that they choose not to discuss pain-related needs with managers out of fear that they might lose their job:
“I feel like disclosing that information would risk my job, because I’m supposed to be here to do strenuous activity, so I can’t be going to management and saying that the strenuous activity, I can’t do. Yeah. It feels like it’s a little bit risky” (P12).
In combination with concerns about workplace discrimination, several participants added that they do not feel comfortable disclosing their needs due to workplace culture or interpersonal relationships with managers. For example, one participant stated:
“I’m this type of person that doesn’t disclose most of everything to people. . .I’m there to work and just to do my job and earn a living and go home. Actually, I will say the managers there are not really, should I say, totally friendly” (P6).
When probed about why they do not feel comfortable disclosing pain-related needs to managers, one participant responded, “Because I feel they pity me so much, or probably try to make me feel sorry for myself. I prefer just being silent” (P23).
Despite their discomfort, several participants disclosed personal information to managers solely out of necessity for receiving workplace accommodations. However, some state this conversation did not occur until after a period of quietly enduring high levels of pain at work. One participant stated, “In the case where I’ve endured enough pain during the course of my duty, I’ll have to report that” (P17).
Coworker Perceptions
When asked how coworkers may react to them wearing an exoskeleton suit, participants expressed concerns regarding negative coworker perceptions. One participant stated:
“I don’t feel it’s quite good because it’s something which I feel I should just go on with my normal work without causing—or rather maybe bringing a lot of my attention—attention from other people. Maybe other times someone would be quite uncomfortable when all people are watching you—‘Okay, what is he wearing?’ or rather something like that or ‘What’s going on?’ or ‘What really happened?’” (P3).
Another participant shared, “I would feel some of them [coworkers] would judge me” (P23).
In contrast, other participants believed coworker perceptions would be predominately positive. For instance, one participant stated, “They [coworkers] are quite understanding. I really appreciate that. I would say this is what has kept me moving” (P3).
Others believed that coworkers would grow to be accepting of their use of exoskeletons: “I think at first it would spark curiosity, so of course it will raise questions. Even if I was using exoskeletons, I know I’ll be answering so many questions by so many people. Understanding the reason behind it, I think I would have nothing but support.” (P12).
Another participant similarly stated that their coworkers would initially be curious about their exoskeleton, and they would be comfortable responding to their questions: “I guess it’s everyone will be like, ‘How did you get it? How important is it?’ They would want to know how it’s working and all that. I think it will be a very cool thing to introduce to all my fellow coworkers as well.” (P18). This participant continued on and said “. . .it’s important to help your neighbor and also to share knowledge. I would feel okay to be able to be in a position to share all that I know about it [exoskeleton].”
Patient Confidence
Participants noted that patients may feel more or less comfortable receiving care from a nurse wearing an exoskeleton, depending on their personal experiences with MSDs, understandings of exoskeleton devices, and personal comfortabilities with technology. One participant who worked with dementia patients expressed patients “might probably not understand, and they might drift away from me” (P7).
Another participant expressed concern that patients may refuse care from a nurse wearing an exoskeleton:
“Some will be scared to get attendance from you. Maybe they’ll feel like you’re going to break down on them. Somebody may look at it [exoskeleton] as something that hinders them from actually seeking help from you, maybe, if you actually look more worried than them” (P17).
Other participants believed that patient confidence may be shaped by their understandings of exoskeleton devices and comfortabilities with technology. One participant stated:
“. . .Maybe the most educated people might say, ‘This is just a normal equipment for. . . who’s working hospital or maybe in a helping facility like a nursing home.’ Maybe for a person [with less education] might be worried, like what the hell is this!” (P18).
As a recommendation to address these concerns, one nurse noted that patient education of exoskeletons is critical for successful implementation in long-term care—particularly for patients who are less comfortable with technology. They stated, “You just have to explain it. . .They’re [patients] going to have the understanding and the perception of what you’re wearing. [Then] they may not be having some mistrust issues and all that” (P18).
Discussion
This study aimed to identify a range of social contextual factors important to the acceptance, adoption, and use of exoskeleton technology in the daily work of long-term care nurses and nurse managers with MSDs. Our findings highlight three key themes relevant to these nurses’ interactions with managers, coworkers, and patients. Prior exoskeleton research in the robotics literature has predominately investigated person-technology-task interactions of exoskeletons (Bogue, 2018; Gull et al., 2020). Our study extends upon this work by investigating the social contextual factors within long-term care facilities which may shape and be shaped by the design and implementation of exoskeleton technologies. These social contextual factors not only hold direct implications for the adoption and use of exoskeletons for nurses with MSDs but also bidirectionally interact with the person, task, and technology factors of the work system in which the exoskeleton will be embedded (Holden et al., 2013). Therefore, our findings should be applied by HF/E practitioners to balance work system elements and design work system contexts for exoskeletons that optimize outcomes for all individuals in long-term care settings.
This study uncovered actionable recommendations for exoskeleton design and implementation for nurses with MSDs working in long-term care. The participants’ experiences reported in the themes above underscore the importance of cultivating a comfortable social environment for nurses to discuss their pain or exoskeleton use with managers, co-workers, and patients. Fostering this social comfortability is crucial for ensuring that nurses will report issues, concerns, or unexpected pain resultant from exoskeleton use to their managers at work. The creation of a comfortable social environment may also promote patient confidence in receiving care from and asking questions to nurses using an exoskeleton.
To establish this social comfortability for nurses with MSDs, long-term care facilities should maintain supportive organizational cultures and comprehensive education on exoskeleton technology. Practical recommendations include fostering open communication channels and promoting a culture of acceptance and support for nurses with MSDs. HF/E experts may outline policies and procedures for exoskeleton use that both prioritize workplace safety and normalize nurses’ use of assistive devices in long-term care settings. These insights not only inform the effective integration of exoskeletons in healthcare settings but also contribute to broader discussions on the social implications of technology adoption in professional work environments. We underscore the significance of creating inclusive environments that prioritize both physical and social well-being in the workplace.
Reported concerns about workplace discrimination, perceived capability, and patient perceptions build upon the findings of prior work in the ergonomics literature. In a previous study examining geriatric nurses’ intended uses for exoskeletons, researchers began to articulate potential social impacts of exoskeletons in healthcare work settings (Katila & Turja, 2021). A study by Turja et al. (2022) described social impacts of exoskeleton use as described by seven nurses in Finland. In this study, participants reported realized and anticipated changes in their relationships and interactions with managers, other nurses, and patients because of exoskeleton use. In alignment with our findings, authors detailed nurses’ discomfort surrounding the unwanted attention brought by the exoskeleton (Turja et al., 2022). Our paper extends upon this work by taking a deeper dive into the underlying factors stimulating nurses’ social discomfort in the context of long-term care in the U.S. Our study, however, does diverge from prior findings in this work reported that nurses believed that the exoskeleton would not draw patients’ attention.
Finally, healthcare organizations should partner with HF/E experts and implementation scientists to perform full, in-depth sociotechnical systems analyses. These analyses may assess vital interactions between and among exoskeletons, nurses with MSDs, social contextual factors, and all other work system elements before, during, and after exoskeletons are piloted in long-term care settings. Understanding multi-level, micro-, and macroergonomic systems interactions may promote feasibility, efficacy, and eventual effectiveness of exoskeleton integration. Iterative improvements and adjustments should be made based on feedback from frontline staff, managers, and patients.
Future work should focus on longitudinal studies that track the long-term impacts of exoskeleton use on nurses’ health and job performance (Vallée, 2024). Additionally, research should investigate the scalability of exoskeleton implementation across different healthcare settings, examining the adaptability of recommendations to diverse organizational cultures and workflows. Future studies should also explore how exoskeleton use impacts team interactions in healthcare. This includes investigating effects on coordination, communication, and workflow efficiency, as well as task distribution, role assignments, and collaboration. Understanding these dynamics can help develop guidelines for optimizing team performance and effectively integrating exoskeletons into healthcare environments (Atweh et al., 2022). Exploring the economic implications, including cost-benefit analyses and funding strategies for widespread adoption, will be crucial. Finally, interdisciplinary collaborations between engineers, healthcare professionals, and social scientists can further refine exoskeleton designs to enhance user experience and acceptance.
Strengths and Limitations
One strength of our study is the racial composition of our sample; 94% of participants identified as Black/African American, which is uncommon in research. This is important since, in long term care settings, members of minority groups comprise nearly 50% of the workforce (Bates et al., 2018). We were able to recruit this sample via snowball sampling which allowed participants to help recruit other participants.
Our study should be considered with several limitations in mind. Interviews took place virtually on Zoom with the intentions to engage a broad sample of nurses and nurse managers across the U.S. However, online recruitment may have biased the sample as our recruitment posts on social media were more likely to reach individuals with a higher technological proficiency. As such, our findings may not be representative of nurses who are less comfortable using modern technology. Future exoskeleton research should explicitly explore the perspectives of nurses with differing levels of technological proficiencies and comfortabilities. Further, there is a possibility that social desirability bias may have shaped participants’ responses during semi-structured interviews. Our team worked to minimize this bias by using techniques recommended by Bergen and Labonté (2020) such as ensuring participants that there are no right or wrong answers to our questions, building rapport, and probing for additional information. Moreover, this study centralized perspectives of nurses working in long-term care facilities. Thus, our findings may or may not be transferrable to the work systems of patients with MSDs or nurses with MSDs working in other professional healthcare settings.
Conclusion
Despite these limitations, this study uniquely uncovers a range of social contextual factors critical to the successful design and implementation of exoskeleton technology for nurses with MSDs working in long-term care facilities. Our thematic analysis uncovered nurses’ (1) discomfort discussing pain- or disability-related needs with managers, (2) concerns for co-workers’ perceptions of their need/preference to use an exoskeleton, and (3) concerns that patients may be uncomfortable receiving care from nurses wearing exoskeletons. The findings presented in this study can guide HF/E experts in balancing social contextual factors and other work system elements to design work system contexts and exoskeletons that promote optimal outcomes for all individuals in long-term care settings. Future work should focus on longitudinal studies to assess the long-term impacts of exoskeleton use on nurses’ health and job performance, as well as the scalability and economic implications of exoskeleton implementation in diverse healthcare settings. Additionally, investigating the effects of exoskeleton use on team interactions, coordination, and workflow efficiency will be essential to optimize team performance and enhance user acceptance in healthcare environments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the National Science Foundation (NSF) under Grant Number 1839946.