
Abstract
To support the ongoing adaptation and implementation of an Emergency Department (ED)-based clinical decision support (CDS) tool to prevent future falls, we interviewed older adults (n = 15) during their ED stay. We elicited their feedback on the written and verbal content of the existing CDS, feelings about the automated risk-screening aspect of the CDS and asked them to identify barriers that would prevent them from following up with the Falls Clinic to which the CDS supports referral placements. Our findings suggest that the older adults interviewed saw the CDS simply as another tool that they trusted their ED physician/APP to interact with. The identified barriers to follow-up reflect common access barriers such as transportation availability and clinic distance. For CDS tools to impact real-life patient outcomes, we must consider patient’s needs and limitations and appropriately match interventions.
Keywords
Introduction
Measuring true patient-centered outcomes from deployed clinical decision support (CDS) is difficult. Often, process metrics are used to ensure that CDS is functioning as intended to drive desired physician behavior, but these process metrics run the risk of ignoring gaps in care systems that can occur downstream. Given the designers of CDS systems are often focused on technical performance of models and changing physician behavior, methods for incorporating patients and their care partners in the design of CDS are underdeveloped. To ensure that CDS is leveraged to its fullest potential for improving patient outcomes, CDS must be designed with patients’ idiosyncratic concerns, needs, and circumstances in mind.
In our work designing and implementing an Emergency Department (ED)-based CDS to refer older adults at risk of future falls to an outpatient fall prevention clinic (Jacobsohn et al., 2022), talking to patients to understand their perceptions of and concerns about the referral and Falls Clinic has been essential. Further, given our CDS uses a machine learning (ML) algorithm to initiate the intervention, we actively sought older adults’ feedback about the automated component of the CDS.
Objective
In this study, we aimed to describe older adults’ perspectives of an ED-based CDS for preventing future falls.
Methods
Parent Study and Setting
This study was conducted as part of a larger parent study aimed at adapting and implementing an existing ED-based CDS tool across a large academic health system in the Midwestern United States. The CDS tool designed by our team leverages an ML model to screen patients for outpatient fall risk and, for the patients at the highest risk, facilitates the placement of a referral to a fall prevention clinic by their emergency medicine physician or advanced practice provider (APP) (Figure 1; Jacobsohn et al., 2022; Patterson et al., 2019).
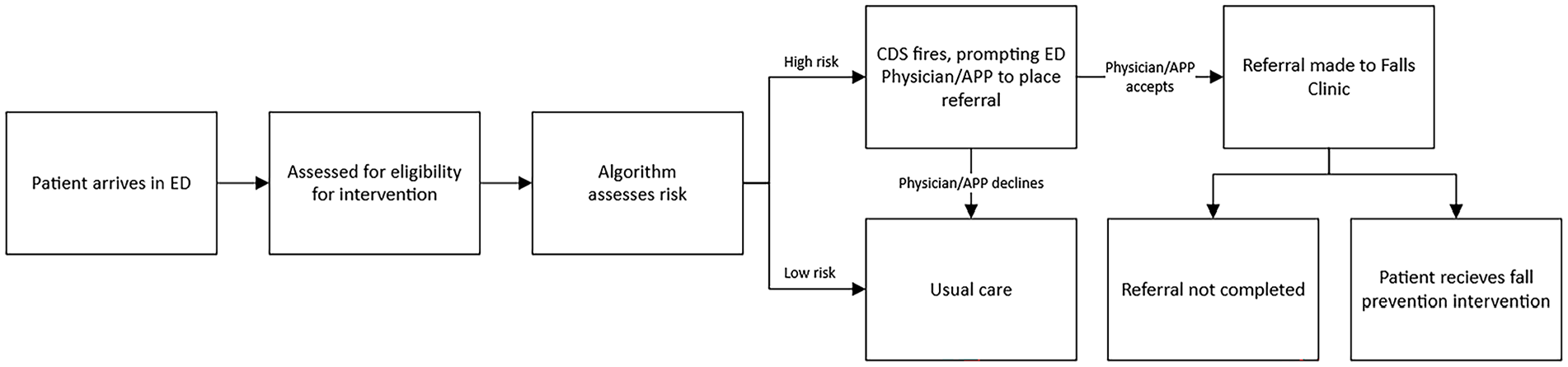
Flow of the ED-based CDS for preventing future falls.
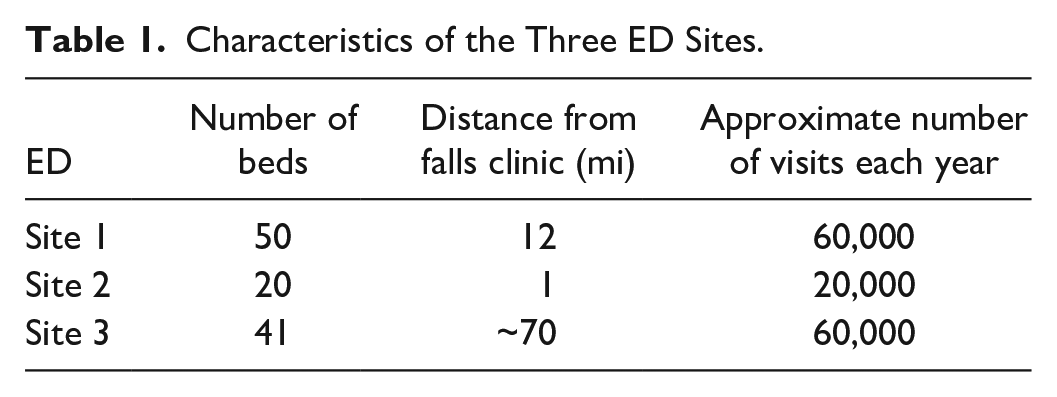
The CDS first went live in the ED associated with the academic medical center (site 1), which sees 60,000 patients per year, in July 2020. It was adapted and went live in an affiliated community ED (site 2), which sees 20,000 patients per year and is staffed by the same physicians and APPs as site 1, in September 2022. Finally, it was adapted again and went live in another affiliated ED (site 3), an urban hospital which sees over 60,000 patients per year, in April 2024. Table 1 provides descriptive data on the three EDs.
Characteristics of the Three ED Sites.
Data collection
We recruited patients 65 years or older from two EDs (sites 2 and 3) to participate in a brief 10- to 20-min interview about the CDS tool before its respective implementation at either site. Interviews at site 2 were conducted in August 2022 (n = 10) and at site 3 in June 2023 (n = 5). Interviews were conducted by one study team member (AM) and took place in the ED. Four older adults were accompanied by a care partner, for example, spouse or (grand)child, who also participated in the interview.
The interview guide was designed to elicit feedback on the verbal and written content of the CDS tool, feelings about the automated screening aspect of the CDS, and barriers to following through with scheduling a Falls Clinic appointment. The interviews were recorded and transcribed for analysis.
Data Analysis
We conducted an inductive content analysis to identify patients’ perceptions of the CDS and Falls Clinic referral intervention (Hsieh & Shannon, 2005). The research team took an iterative approach to discussing and refining codes and resultant themes.
Results
Perceptions of Automated Screening
None of the older adults interviewed expressed concern about the CDS being triggered by an automated screening process. One participant even identified screening as a task that is well-suited for automation: Well, if you have a lot of factors that you need to factor in, it’s awfully hard to do it manually. It makes it a lot easier if you do it with a computer.
All participants agreed that the ultimate decision about their care should be made by their ED physician/APP—suggesting that the older adults viewed the CDS as simply another one of the tools that the clinicians should use to care for them. One participant described their desire for their physician/APP to deliver communication about their fall risk and available interventions: Computers and algorithms are so non-personal. . . the doctor knows your history and knows all of that stuff. The personability of it is what’s important to me.
Multiple participants described being comforted just hearing that the Falls Clinic exists and that there are people that want to help.
Barriers to Following Through on Recommended Care
When asked what barriers would prevent them from scheduling an appointment, participants most frequently cited access to transportation and distance from the Falls Clinic—distance was especially noted by all five participants from site 3 which is located 70+ miles from the Falls Clinic. Other factors that participants were concerned about included weather, insurance coverage, time investment, and for a participant from the further ED, how they would manage their diabetes while in transit to the Falls Clinic. While most participants agreed that cost would be a factor and they wanted information on it, none spontaneously cited cost as a barrier.
Discussion
Our findings point to a fundamental difference in how we, as CDS designers and researchers, viewed the importance of the automated aspect of the CDS. Participants described no real concerns about an automated screening system, rather, they related to the CDS as another tool in the physician/APP’s toolbox, whom they trusted to apply it appropriately to their unique circumstances. From the patient’s perspective, the automated screening was not separate from the action it triggered, that is, referral to the Falls Clinic.
Consequently, of much more importance to the participants was the recommendation that the CDS put forth. That is, if they were to be referred, patients were concerned with whether the Falls Clinic was worth their time and investment. They wanted to know the details on how it worked (“is it in person?”) so that they could consider how feasible it would be for them to get there.
While the barriers patients identified are not particularly surprising, it is notable that these were not factors we had been initially considering as we designed the CDS (as conceptualized, for example, in Figure 1). As implemented in sites 1 and 2, our falls prevention intervention relies not only on the ED physician/APP referring the patient (accepting the CDS alert) as originally conceptualized, but also on whether the older adult patient will answer the phone to schedule an appointment with the Falls Clinic a few days after being in the ED, their perception of whether going to the Falls Clinic will be good for them, and the availability of transportation to the appointment.
Recognizing the insurmountable barriers there were for patients from site 3 to make it to a Falls Clinic to receive the falls prevention intervention, we chose to adapt the GAPcare (the Geriatric Acute and Post-acute fall prevention intervention) program—a validated ED-based intervention for preventing future falls by providing physical therapy and pharmacy consults within the ED (Goldberg et al., 2019)—for use with our automated screening at site 3. The apparent success of GAPcare may be related to the stark reduction of patient work as compared to what is required of patients to effectively follow-up with the Falls Clinic. Considering that barriers to accessing out-patient follow-up care are inequitably distributed, GAPcare may also prove to be a more equitable intervention—resulting in not only more patients receiving the intervention, but a more diverse population.
An unexpected finding was how often participants reported feeling comforted upon learning that the Falls Clinic exists. One participant was adamant that if their emergency physician/APP suggested they visit the Falls Clinic, they would find a way. It is unclear how such appreciation for this care resource corresponds to personal risk of fall, as reported by the algorithm. It is plausible that patients identified by the algorithm—which includes features such as previous acute care utilization—as high risk are frailer, and thus have more competing care needs making them more skeptical of the clinic’s utility to their specific circumstances. To maximize benefits to patients from a CDS tool, we must broaden our conceptualization of CDS to include the patient’s perception of not only the CDS, but the chain of events initiated by CDS that are required to impact patient outcomes.
Limitations
An important limitation to note is that the older adults interviewed in this study were not necessarily eligible for the intervention, that is, at high risk of falling in the future. Thus, it is possible that the themes described here insufficiently capture the concerns of people who are actively being told they are at risk of a future fall—a potentially upsetting conversation.
Conclusion
For CDS tools to impact real-life patient outcomes, we must go beyond our typical measures of successful implementation, for example, use or acceptance of the tool, to consider how appropriately matched our interventions are to specific patients’ needs and limitations.
Footnotes
Acknowledgements
The authors would like to acknowledge the clinicians who participated in our academic detailing interviews and shared their insights with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality \ Grant # R18HS027735 (Patterson, PI). This work is solely the responsibility of the authors and does not represent the official views of the Agency for Healthcare Research and Quality.