
Abstract
This qualitative study explores the barriers to incorporating portable MRI devices in ambulances, enabling effective patient triage and potentially reducing time to thrombolytic treatment for stroke. Using a digital twin of the patient handling process, semi-structured interviews were conducted with 11 paramedics and 7 neurologists from an emergency medical services system and a tertiary stroke care center. Thematic analysis of interview transcripts, guided by the Systems Engineering Initiative for Patient Safety framework, revealed key barriers: the need for specialized MRI operation skills, complex patient handling procedures, limited space, and the necessity for training and policy development. The study proposes solutions to address these challenges, aiming to facilitate the implementation of ambulance-based MRI systems for expedited stroke care. The findings contribute to understanding the factors influencing the adoption of advanced imaging technology in pre-hospital settings, ultimately improving patient outcomes by minimizing delays in stroke treatment.
Keywords
Introduction
A stroke is a major global health concern, ranking as the second-leading cause of mortality and the third-leading cause of disability worldwide (Johnson et al., 2016). It occurs when the blood supply to part of the brain is blocked, potentially causing irreversible damage. In stroke care, time is critical—every minute lost can lead to further brain tissue deterioration and significantly impact patient outcomes.
An essential metric in stroke care is door-to-needle (DTN) time, which measures the time from a patient’s hospital arrival to the administration of thrombolytic treatment (Brunser et al., 2020). The widely recognized target is 60 min, known as the “golden hour.” However, the treatment window for thrombolysis is narrow, requiring administration within 3.5 hr of symptom onset. This highlights the need for expedited care upon arrival, including immediate axial imaging, typically by computed tomography (CT) scan to exclude hemorrhagic stroke (Cheng & Kim, 2015).
Healthcare systems continually strive to reduce DTN time through rapid response strategies, streamlined protocols, and improved interdisciplinary collaboration. Recent technological advancements, particularly telestroke, have transformed stroke care (Levine & Gorman, 1999). Telestroke uses telecommunication technology to deliver immediate care, addressing expertise and resource shortages. It enables real-time audio-visual communication and medical data sharing, allowing timely and accurate patient assessment in both prehospital and in-hospital settings (Demaerschalk et al., 2017). While telestroke has improved treatment efficiency, patients still require in-hospital brain scans for accurate diagnosis and treatment selection. CT and Magnetic Resonance Imaging (MRI) are the primary imaging techniques used. CT scans quickly identify whether a stroke is due to blood loss or bleeding, while MRI scans, though longer, offer greater accuracy and sensitivity (Chalela et al., 2007). Portable MRI scanners, which are an emerging technology, now offer a flexible option, allowing scans almost anywhere within a facility (Deoni et al., 2022).
A potential solution to further reduce DTN time is to develop methods for performing brain scans during transit to the hospital. Using portable MRI systems in ambulances could enable faster diagnoses and early interventions before arrival. This could allow ambulances to bypass nearby rural hospitals and proceed directly to level 1 stroke centers. A preliminary study conducted by the research team demonstrated the feasibility of a point-of-care portable MRI scanner in a telemedicine-equipped ambulance during active transport, successfully acquiring and transmitting images of acceptable quality (Roberts et al., 2023).
Building on this, the current study focuses on identifying barriers to implementing portable MRI systems in Emergency Medical Services (EMS) ambulances for timely stroke diagnosis and care. The research applies the Systems Engineering Initiative for Patient Safety (SEIPS 2.0) framework to understand human factors considerations, and interactions between people, their work environment, systems, and processes. Specifically, the study examines challenges related to personnel, tools and technology, physical environment, specific tasks, and organizational aspects of the socio-technical work system.
Method
This study employed a qualitative research method to investigate barriers to implementing portable MRI systems in ambulances for stroke diagnosis using the SEIPS 2.0 framework, as illustrated in Figure 1. This approach provided a comprehensive understanding of the integration challenges, considering how each component of the work system affects care processes and ultimately influences patient, employee, and organizational outcomes.
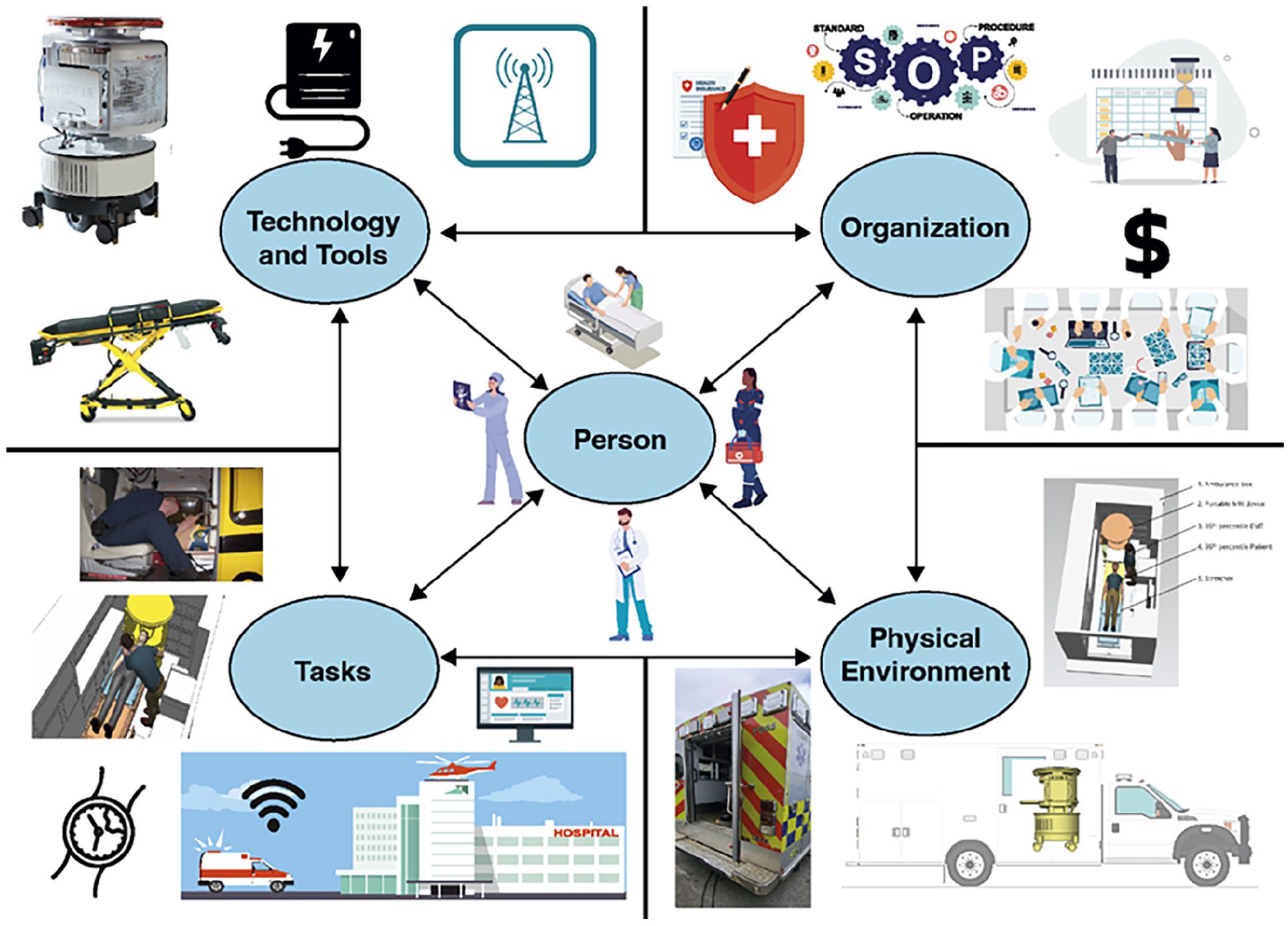
SEIPS 2.0 work system categories.
Participants
The study involved 18 participants: 11 paramedics from Charleston County EMS and 7 neurologists (including three neuroradiologists) from MUSC. Inclusion criteria required at least 1 year of experience with stroke patients for paramedics and at least 1 year of experience in stroke diagnosis for neurologists. Participants were contacted via phone or email.
Study Stimuli Development and Data Collection
A preliminary visit to Charleston County EMS provided detailed images and dimensions of the Ford F550 XLT ambulance’s patient compartment, including patient handling procedures and stretcher specifications. MUSC medical professionals introduced and explained the functionality of the portable MRI scanner. Based on this information, a 1:1 scale digital twin of the patient handling process was developed using PTC Creo and Tecnomatix Process Simulate software. The virtual model was refined through collaboration with experts from MUSC and Charleston County EMS. The digital twin components are illustrated in Figure 2, with virtual model screenshots in Figure 3.
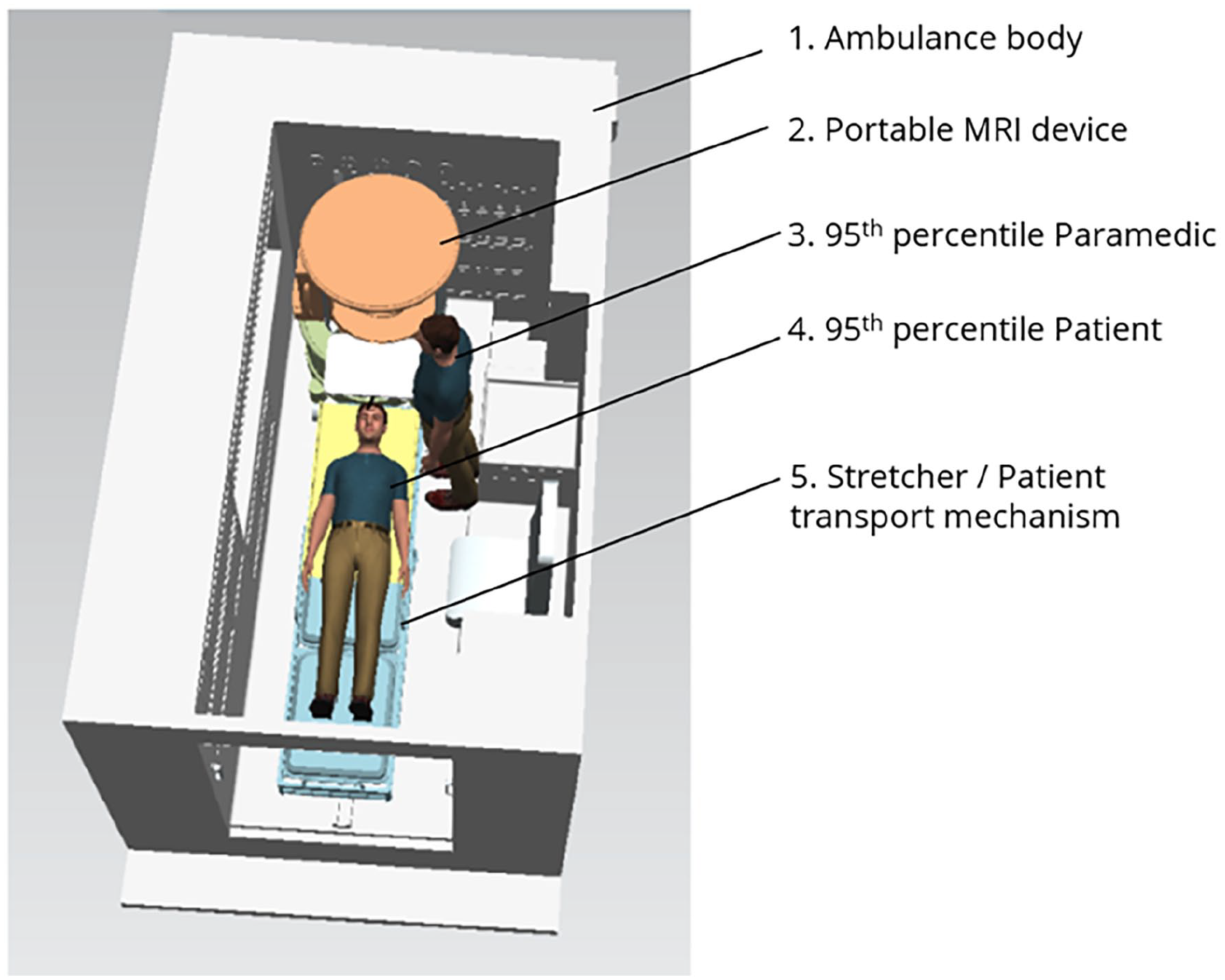
Components of the digital twin.
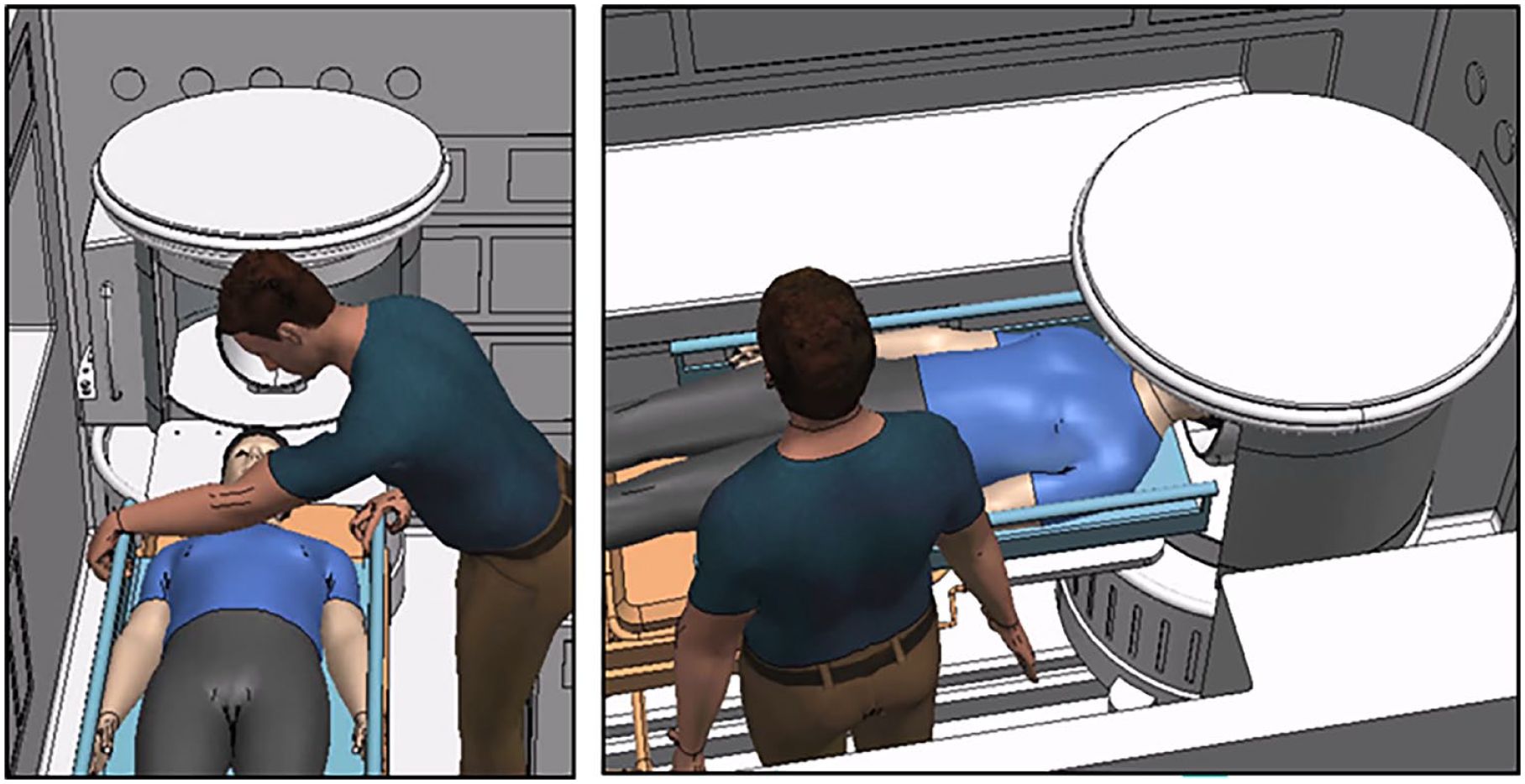
Patient handling process simulation.
The data collection process with each participant began with a project overview, followed by a digital twin simulation video demonstrating patient handling and portable MRI capabilities in the ambulance. Semi-structured interviews then gathered feedback on the proposed process. Questions for participants covered barriers, benefits, challenges, and overall impact. All sessions were audio recorded. After the interview, participants completed an online survey capturing demographic and professional information.
Data Analysis
Interviews were conducted from September to November 2023, lasting 45 to 60 min each. The audio recordings were transcribed and anonymized by removing names and locations. Thematic analysis was performed on interview transcriptions. Five researchers independently coded the data. An initial code set was developed from the first three transcripts. A consensus meeting discussed the initial transcripts, achieving an inter-rater reliability of 0.82. In cases of disagreement, each data point was examined thoroughly, and additional evaluators were involved as needed to resolve the disagreement and reach a complete agreement. The remaining transcripts were independently coded. Codes were then grouped into themes and categorized according to work system components.
Results
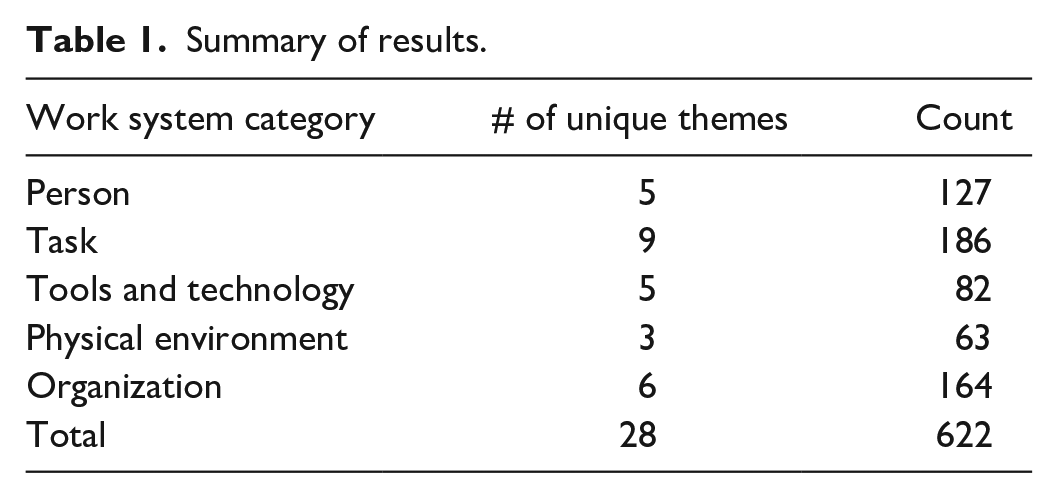
The total number of unique barrier themes and the overall count associated with each work system category are presented in Table 1. Overall, 28 unique barrier themes were identified, with a total of 622 occurrences. The occurrence count represents the number of times the participants discussed a specific theme during interviews.
Summary of results.
Barrier Themes Related to Person (s)
Inadequate training of paramedics in MRI operations is a significant concern, as they lack the specialized knowledge typically possessed by hospital technicians. This gap in expertise could lead to delays, errors, and safety issues. The physical demands on paramedics are also increased, as they must maneuver heavy equipment in confined spaces, potentially risking injury and fatigue. Paramedics also commented about the increased cognitive demands that may lead to additional burdens, including identifying ferromagnetic objects for safety and operating complex systems while performing their usual duties. Patient comfort is another consideration, as the confined space of the MRI may induce anxiety and claustrophobia, potentially compromising scan quality. Safety risks for both patients and paramedics may be increased due to the presence of strong magnetic fields in a mobile environment.
Barrier Themes Related to Tasks
Paramedics and neurologists commented that tasks such as airway management may become difficult due to reconfiguring the ambulance interior by removing the captain seat, potentially compromising patient care. Positioning patients correctly into the MRI device within the confined space of a moving ambulance is perceived to be challenging and risks injury. The scan duration of 10 to 15 min may limit benefits in urban settings with short transit times. Paramedics also commented that emergency patient extraction during scanning may be hindered by the limited space, posing safety risks. Communication barriers between ambulance and hospital teams, along with data transmission issues, may delay critical information sharing. Neurologists and paramedics mentioned the scanner instability in moving vehicles that could produce poor-quality images, necessitating rescans and defeating the purpose of in-transit diagnosis. Equipment disinfection between patients could be challenging and time-consuming, risking cross-contamination. Lastly, paramedics commented that triage decisions could become complex to decide on which patients to scan in transit, requiring specialized training to avoid errors and resource wastage.
Barrier Themes Related to Tools and Technology
All participants commented on the size and weight of the portable MRI device (about 1,400 lb or 635 kg) that would require substantial vehicle modifications, complicating the ambulance layout and potentially restricting patient access. Power supply is another concern as noted during the interviews, since MRI devices demand high and consistent power (900 W at 110 V), which could increase the load on ambulance electrical systems and compromise other critical equipment. Electromagnetic interference from the MRI device may disrupt essential electronic devices, posing risks to patient monitoring and communication systems. Maintenance of MRI devices in mobile environments may be problematic due to exposure to vibrations, temperature changes, and contaminants, potentially leading to frequent malfunctions. Issues with stretcher compatibility could complicate patient positioning for MRI scans, as current designs lack the flexibility to align with the MRI device’s transfer bridge. This incompatibility makes it difficult for paramedics to safely and efficiently transfer patients, increasing the risk of musculoskeletal strain.
Barrier Themes Related to Physical Environment
Paramedics and neurologists commented that the confined interior of ambulances, designed for traditional emergency medical equipment and personnel may struggle to accommodate the bulky MRI device. This space constraint can inhibit the ability of healthcare providers to perform critical interventions and obtain clear MRI scans. Accessibility is also compromised, as the presence of the MRI device may limit paramedics’ proximity to patients and access to other essential medical equipment. Another concern reported was the significant weight of MRI device that would necessitate substantial structural reinforcements to the ambulance’s floor and chassis. This modification could be both costly and technically challenging, with only larger vehicle chassis (such as Ford F550, Ford F650, Chevy 5500HD) being suitable for retrofitting.
Barrier Themes Related to Organization
The paramedics commented that developing and implementing new training protocols to operate and maintain MRI-integrated EMS systems requires specialized knowledge beyond traditional emergency medical training. Policy and regulation hurdles may arise from the lack of existing provisions for mobile MRI units, necessitating new or amended regulations to ensure safety and privacy standards. Liability and insurance concerns due to increased risks may lead to higher costs translated to both the healthcare provider and the patient. Establishing robust Standard Operating Procedures (SOP) is critical for safety, efficacy, and compliance, but inadequate or complex SOPs could cause operational delays. Staffing and scheduling challenges emerge from the need for specialized personnel trained in MRI operation and advanced stroke care, potentially increasing shifts or necessitating additional hires. The participants also mentioned the cultural resistance to changing established protocols and skepticism toward portable MRI technology that could slow down the adoption rates.
Discussion
The key findings of the study are summarized, along with potential solutions and strategies to address these barriers. The research concludes by outlining its limitations and suggesting avenues for future investigation.
Person barriers involve the specialized skills required for paramedics to set up the MRI device in moving ambulances and for radiologists to operate them remotely. This complexity adds cognitive burdens as paramedics must integrate new information beyond standard protocols. This is consistent with previous research (Rogers et al., 2020, 2021) which reported that neurologists struggled with task complexity and paramedics faced unclear communication in existing EMS settings. Usability issues with MRI software interfaces complicate scanning and image processing, as noted in various telemedicine studies (Agnisarman et al., 2017; Narasimha et al., 2017). Comprehensive training programs, including simulations and refresher courses, could address these barriers. Appropriate operating protocols and assistive equipment can help reduce physical and cognitive demands during patient setup and scanning.
Task barriers in using MRI for stroke diagnosis include procedural and operational challenges. Extracting patients during emergencies such as cardiac or respiratory issues, seizures, device failure, or fire can be hindered by tight space and incompatible stretchers. Obtaining comprehensive medical histories in the field, consistent with the findings of a study (Porter et al., 2020), is challenging due to limited access to records, often leading to partial or unclear information. Proper disinfection of MRI equipment between patients is essential but time-consuming due to unfamiliarity with the process and materials. This aligns with the findings of a study which emphasized that regular daily disinfection is critical for controlling microorganisms on medical equipment in a radiology department (Hubble et al., 2016). This highlights the importance of disinfecting contact surfaces between patients for optimal sanitization. Custom-height stretchers can facilitate smoother patient transfers, while assistive tools like roller boards, mega movers, transfer rods, winches, or ceiling lifts can reduce lifting strains and injury risks (Conrad et al., 2008). Quick-release latches, or slide-out mechanisms on the MRI device or ambulance floor can enable rapid emergency extraction. Developing MRI-compatible equipment allows for interventions during scanning. Robust communication links and integrated EMS and hospital IT systems can improve information sharing and decision-making efficiency.
Tools and Technology barriers arise from the large, heavy MRI device requiring significant ambulance modifications. Compatibility with existing stretchers is challenging, requiring design changes for safe patient handling. The 900 W power demand can divert resources from critical equipment, and integrating the MRI without interfering with patient monitoring or communication devices is difficult. Vibration and motion can degrade image quality, necessitating frequent maintenance due to poor road conditions. Potential solutions include a modular MRI design for easier integration, supplementary power sources, radiation shielding, stabilization techniques, and remote monitoring software to resolve technical issues efficiently.
Physical Environment barriers in ambulances include confined spaces unsuitable for large medical devices. Modifying the captain’s seat for an MRI device can hinder paramedics’ access to patients. Significant chassis modifications are needed to support the MRI’s weight, and current ambulances have safety issues during transit. Du et al. (2019) noted that newer EMS ambulances don’t always offer increased crash safety, highligting the limited understanding of movement and impact inside ambulances during collisions. Solutions include designing compact MRI units with reduced weight, using warning systems for ferromagnetic objects, and employing assistive lift devices and reconfigurations to reduce ergonomic strain.
Organizational barriers include the need for extensive training for paramedics and neurologists on in-transit MRI operations, which is currently lacking. Liability and insurance concerns may arise due to the increased risks of operating complex devices in moving vehicles. Detailed protocols for triage decisions and specialized staffing are necessary, impacting costs and workflows. Overcoming cultural resistance and institutional skepticism is also a challenge. Roberts et al. (2023) found the current 80% sensitivity of portable MRI for detecting intracranial hemorrhage may be insufficient for safe thrombolytic treatment, though some neurologists believe low-field MRI is adequate for quick stroke diagnosis. To address these barriers, EMS agencies, MRI manufacturers, and hospitals should collaborate on training programs for paramedics. Engagement with policymakers can help develop standards and regulations for mobile MRI systems. Pilot studies and phased deployment can demonstrate safety and value, aiding acceptance by healthcare providers and insurance companies. Educating patients positively about the process can improve acceptance. Gradual culture shifts may occur as the benefits of mobile stroke diagnosis are proven.
This study has limitations. This preliminary study, based on interviews with paramedics and neurologists and lacking physical experimentation, focused on identifying barriers without quantifying their frequency or severity and was conducted within a specific region and EMS agency.
Future work should develop evidence-based solutions to mitigate the identified barriers and integrate MRI in ambulances. Utilizing the digital twin model can help redesign ambulance interiors, modify patient stretchers, optimize MRI device design, conduct virtual ergonomic assessments, and improve vehicle chassis dynamics and safety. Comprehensive training programs, policies, and prototype validation using human factors and ergonomics principles are critical next steps. A systems approach, emphasizing human-centered design and involving patients, providers, and stakeholders, is essential to ensure the solutions are practical and beneficial.
Conclusion
This study explored the challenges of integrating MRI systems into EMS ambulances for early stroke diagnosis and reducing door-to-needle time. Key issues include safety risks for patients and providers, triage challenges during transit, physical constraints of portable MRI devices, space limitations in ambulances, and the need for standard operating procedures. Other barriers include inadequate paramedic training, scanner instability affecting MRI quality, maintenance difficulties, airway management challenges, and staffing issues. Addressing these challenges through human-centered methods could potentially enhance rapid stroke diagnosis and treatment in prehospital emergency care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Blue Sky Award, and an Academic Matching Grant from the South Carolina Research Authority.