
Abstract
The COVID-19 pandemic accelerated the adoption of telehealth across healthcare systems, permanently transforming the way care is delivered. While telehealth has significantly enhanced healthcare accessibility, this transition has also introduced challenges in maintaining high standards of care. Furthermore, new technological challenges compounded by resource constraints have emerged. Allied healthcare providers, who often face resource limitations themselves, play a crucial role in delivering comprehensive care, including diagnostics, therapy, and support services. To delve deeper into these challenges, we conducted semi-structured online interviews, aiming to uncover the specific ergonomic obstacles that allied healthcare professionals, notably audiologists and speech-language pathologists face during telehealth consultations. By shedding light on their unique experiences, this work aims to pave the way for enhancements in telehealth ergonomics within the allied health sector, providing actionable recommendations that enhance telehealth ergonomics, thereby elevating the quality of remote healthcare services while addressing concerns from both practitioners’ and patients’ perspectives.
Keywords
Introduction
The COVID-19 pandemic catalyzed a rapid and widespread adoption of telehealth across healthcare systems and practices, permanently transforming the way care is delivered (Jagarapu & Savani, 2021). Telehealth has significantly enhanced healthcare accessibility, offering patients the convenience of receiving treatments from their homes (Curfman et al., 2021; Marcin et al., 2016). However, this transition has also introduced new challenges in maintaining the highest standards of care from healthcare providers, alongside new technological challenges exacerbated by resource constraints on both the providers’ and patients’ sides (Blandford et al., 2020; Tazi et al., 2023, 2024). Allied healthcare, encompassing a wide range of services such as audiology and speech-language pathology, plays an indispensable role in modern healthcare systems (Akkunje et al., 2020). Professionals in these fields play vital roles in healthcare delivery by helping individuals of all ages improve their quality of life and functional abilities through devices (e.g., hearing aids, augmentative and alternative communication devices) and rehabilitation interventions (McPherson et al., 2006). Allied healthcare providers often face resource limitations (Foster et al., 2009) and play a crucial role in delivering comprehensive care, including diagnostics, therapy, and support services critical to patient recovery and health maintenance (Saxon et al., 2014). To delve deeper into these challenges, we conducted a semi-structured interview online, aiming to uncover the specific ergonomic obstacles that allied healthcare professionals, notably audiologists and speech-language pathologists (SLPs), face during telehealth consultations. This work aims to shed light on their unique experiences and pave the way for enhancements in telehealth ergonomics within the allied health sector.
In the domain of telehealth, ergonomics is focused on designing systems and processes that optimize human well-being and overall system performance, while ensuring accessibility for users and aiding in their treatment (Jacobs et al., 2012). As telehealth becomes more prevalent, it is essential to identify and address technological challenges to prevent any negative impact on patient and provider experiences or the quality of care delivered (Joseph et al., 2011). Thus, through this study, we had two primary goals: Firstly, to gather insights from audiologists and speech-language pathologists regarding the main technological issues and challenges encountered during telehealth consultations, especially given the allied nature of healthcare where resources are frequently constrained. Secondly, to leverage this data to formulate actionable recommendations that enhance telehealth ergonomics, thereby elevating the quality of remote healthcare services while addressing concerns from both practitioners’ and patients’ perspectives. We aimed to answer the following research questions:
What are the primary resource-constrainted concerns that audiologists and SLPs have identified in telehealth sessions? (This might pertain to the patient’s arrangement, technological elements, environmental conditions, or other components of the virtual appointment.)
How do these challenges affect the patient experience, provider experience, or quality of care?
What strategies, best practices, or solutions have providers tried or considered implementing to address telehealth technological issues?
Methods
To understand the audiologists’ and SLPs’ insights and experiences regarding ergonomic issues within telehealth, we employed a qualitative methodology through semi-structured interviews. We structured a study framework and formulated an interview guide aimed at extracting insights from audiologists and SLPs operating in private practices throughout the United States. We chose online interview given the nature of the study.
Participant Recruitment and Demographics
The target population for this research comprised professionals from the allied healthcare disciplines of audiology and speech-language pathology, specifically those operating in private practice settings within the United States, where access to information technology resources to support privacy and security needs is often limited. Utilizing a stratified purposive sampling approach, we study recruited an equal number of participants from each field—10 audiologists and 10 speech-language pathologists—to facilitate a balanced exploration of professional perspectives. Initial outreach was conducted via professional networks, academic forums, and special interest groups, supplemented by dissemination through specialist social media groups and digital platforms. Furthermore, strategic partnerships were established with relevant professional societies, namely the American Speech-Language-Hearing Association (ASHA) and the Academy of Doctors of Audiology (ADA), which facilitated the distribution of recruitment emails to their extensive membership databases. To broaden the participant base, snowball sampling methods were also employed. The participant pool exhibited considerable demographic and professional diversity, encompassing varying geographical locations, professional roles, years of experience, and familiarity with telehealth technologies (see Table 1 for detailed participant demographics).
Participant Demographics.
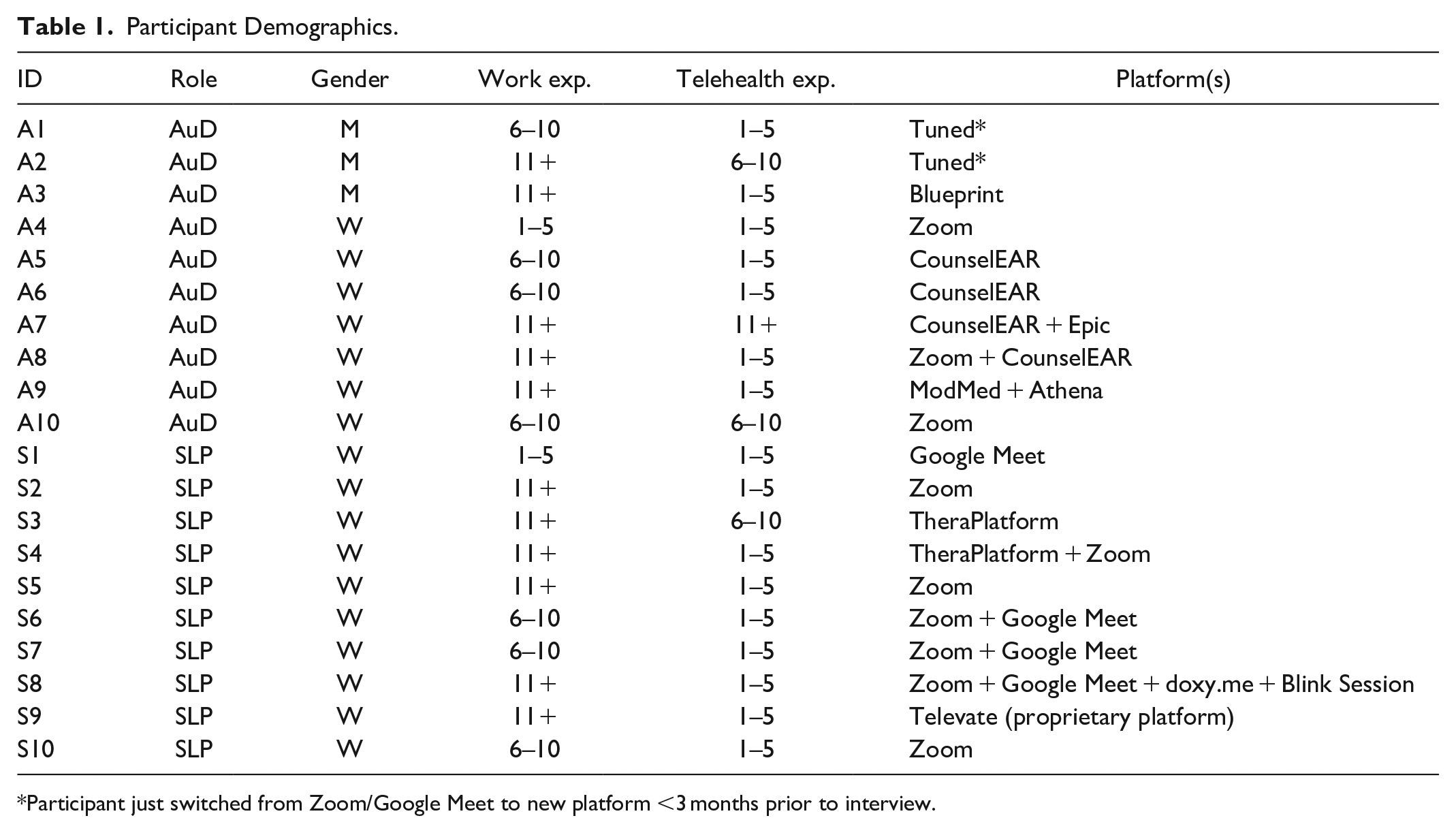
Participant just switched from Zoom/Google Meet to new platform <3 months prior to interview.
Data Collection
We adopted a semi-structured interview format, with open-ended questions carefully crafted to elicit detailed responses from participants. Our approach fostered organic and open conversations, allowing each session to naturally adjust based on the participant’s insights. The interview questions were refined through pilot interviews involving the research team and lab members. Virtual interviews were conducted on the Zoom platform, with an average duration of 46 min, reflecting deep and engaging discussions. Prior to each interview, participants were briefed on the study’s objectives, methodologies, and ethical considerations, and verbal informed consent was obtained, including permission to record the session. Participants were given the option to disable their video if they felt uneasy about visual recording. As a token of appreciation for their contribution, each participant received a $50 USD electronic gift card upon interview completion.
Data Analysis
Following the interviews, the audio recordings were auto-transcribed and verified against the original audio to ensure accuracy. One participant opted out of recording, their input was captured through real-time manual notes. Subsequent to this process, all transcripts and notes were anonymized to remove identifiable details by the first and last authors, after which the original audio recordings were permanently deleted to maintain confidentiality. We then used a thematic analysis approach (Mildner et al., 2023), whereby the first author generated an initial codebook through an inductive review of the interviews. To establish coding consistency, two researchers coded two randomly selected transcripts, and their inter-rater reliability, as measured by Cohen’s kappa ( κ = 0.76), indicated strong coder agreement. Following a discussion to reconcile discrepancies and refine the codebook, the 2 researchers analyzed the remaining 17 transcripts and 1 manually noted interview through an iterative process, regularly convening with the other authors to discuss emerging themes. The qualitative data analysis was facilitated by the use of NVivo and MAXQDA software.
Results
Examination of the interviews showed several recurring ergonomic challenges that audiologists and SLPs faced with patients during telehealth sessions. The main issues reported were connectivity problems, difficulties assessing and troubleshooting technology issues remotely, workflow interruptions, and environmental factors.
Internet Connectivity Challenges
Participants identified internet connectivity issues as a significant barrier to seamless telehealth delivery. Rural patients, in particular, faced challenges due to bandwidth limitations and unreliable internet connections, affecting the quality of audio and visual aspects of telehealth sessions and causing interruptions. As participant A5 noted “The issue that I run into more is a stable Internet connection.” (A5)
This is compounded for patients in remote areas, who may experience more sporadic internet connections: “Some of my patients though are in more remote areas and they could have a bad Internet day.” (A5)
A5 further highlighted the stark digital divide, explaining that many patients in their state lacked home internet access, relying on public spaces like cafes or work internet for connectivity “The issue that I run into more is a stable Internet connection but when you have to look at the demographics of my state much of my state doesn’t have Internet in their home they might go to like a cafeteria for the community and you’d share Internet or maybe they can do it on work hours so for me it’s more of a do they have Internet in their village or in their rural community and if they have Internet are they able to use it for this” (A5)
Similarly, participant S9 reported difficulties working in rural areas with poor internet connectivity, leading to lagging and connection problems. S7 succinctly summarized the issue, “I’m only limited by my Internet connection. . . sometimes my Wi-Fi connection at my current job is not stable, so I might get disconnected sometimes.” (S7)
These connectivity challenges had far-reaching impacts, including disruptions to effective communication between providers and patients, which led to barriers to comprehensive evaluations and high-quality care. Additionally, this has issue the potential to cause privacy confidentiality risks during sensitive discussions, as well as patient frustration and disheartenment.
Technological Literacy and Availability Barriers
Providers faced significant challenges due to patients’ limited technological literacy, making remote troubleshooting during telehealth sessions extremely difficult as A3 notes: “It’s just ease of use I remember a lot of them [patients] are little elderly they don’t know how to turn the camera on they don’t know how to unmute their microphones, if their internet is down what do I do? you know if it freezes what do I do? how do I start this? how do I end this? . . . the technology of the telehealth that tends to intimidate themselves” (A3)
This quote highlights the basic technological hurdles faced by elderly patients, including operating a webcam and microphone. Another participant echoed this concern, stating, “Our patients really don’t have the technology to actually do it unless they have like a daughter or a family member that’s there.” (A6)
This suggests that many patients, particularly older adults, required assistance from younger, more tech-savvy family members to participate in telehealth sessions. Moreover, technological difficulties created communication barriers that impacted quality of care. Participant S7 explained, “If they’re spending a lot of time in the session trying to sign in, that can be frustrating on both ends. . .then if they run into a problem, it takes up half the session, and it feels like that could have been avoided.” (S7)
When patients struggled with basic technological operations, it ate into precious clinical time and disrupted the effectiveness of the appointment. To mitigate this, some providers attempted to be proactive in training patients beforehand, but this placed yet another non-clinical burden on already over-taxed providers, “I’ll show them how to do telehealth before they leave” (A6) “I was explaining to families how to access the platform.” (S5)
Workflow Disruptions
The introduction of telehealth modalities significantly disrupted clinical workflows and processes for healthcare providers. A major issue was the substantial administrative overhead and technical support responsibilities that fell on providers. Participant S7 described the frustration: “If they’re spending a lot of time in the session trying to sign in. . .it feels like that could have been avoided.” (S7)
This quote highlights how providers often spent valuable clinical time getting patients logged in and familiar with the telehealth platform, due to patients’ lack of pre-appointment preparation. Participant S5 echoed this concern, stating, “I do all the troubleshooting myself. . .I pretty much do it all in terms of supporting the families.” (S5)
Providers took on extra administrative burdens like scheduling, confirming appointments, and managing billing/payment processes related to telehealth, without dedicated support staff. This increased multi-tasking demands and cognitive load on providers, making it ”frustrating on both ends” and an inefficient use of time. The quotes suggest that telehealth increased providers’ responsibilities beyond their core clinical duties, blurring the boundaries of their scope of practice. Participant S7 noted, “Basically 100% of the troubleshooting would be on the therapists.” (S7)
Providers were being asked to go above and beyond their core roles, creating extra stress and burnout risk.
Environmental Factors
The telehealth model introduced significant environmental challenges, impacting patients’ physical surroundings and privacy during virtual sessions. Providers reported that patients’ household environments often posed difficulties, as noted by participant S6, “It depended on their household. . .sometimes they didn’t always have as good of a space as we would have liked.” (S6)
This highlights how home environment and space constraints could make it difficult for patients to find a suitable, quiet, private area for sensitive healthcare discussions. Another provider noted the flexibility of telehealth, but also the risks, “Parents choosing to sign on with their phone in the middle of a parking lot. . .there are privacy risks of being overheard” (S1)
Using a mobile device in a public setting like a parking lot is far from ideal, with distractions, disruptions, and privacy risks. On the other hand, the home environment, while convenient, may lack the boundaries, privacy safeguards, and professionalism of a clinical setting. As noted by some participants, household members could overhear the telehealth sessions, compromising confidentiality and making patients uncomfortable discussing certain topics. This lack of privacy and control over the environment created a suboptimal experience, potentially negatively impacting communication, rapport building, and clinical assessments/evaluations. Moreover, there are legal/ethical implications around privacy violations if sessions are audible or visible to unintended parties in the patient’s environment. Providers may need to explicitly establish privacy/confidentiality practices at the start of telehealth sessions to mitigate these risks. Participant S8 highlighted the challenge of ensuring privacy in telehealth sessions, especially in small living spaces: “In person you have a better sense of who’s right there. . . when kids live in smaller apartments and they have siblings or maybe cousins around, you’re never sure who’s there.” (S8)
This uncertainty raises concerns about confidentiality and HIPAA compliance. A9 echoed this concern, noting that in telehealth sessions, “you don’t have any idea if that’s actually occurring [someone listening in] because they could be sitting right next to the patient listening in and you know I might not even notice that” (A9)
Implication
Our findings have significant implications for the effective delivery of telehealth services. Three key areas require attention: internet connectivity challenges, technological literacy and availability barriers, and environmental factors. Telehealth platforms and services should be optimized for low-bandwidth environments to accommodate users with limited connectivity, ensuring accessible care for all patients, regardless of their location. Furthermore, Policymakers and service providers should prioritize expanding broadband infrastructure and ensuring equitable access to internet services, particularly in rural and underserved areas.
Providers and healthcare organizations should implement patient education programs and provide user-friendly resources to improve technological proficiency and address the technological literacy gap among patients, especially older adults (Lewis, 2003). Additionally, providers should take proactive steps to improve telehealth ergonomics by conducting tech checks before visits, providing instructional resources for optimal device setup, offering IT support for troubleshooting, suggesting alternative visit locations such as local libraries or community centers as alternative visit locations when necessary (Ritchie et al., 2017).
Telehealth implementation necessitates a comprehensive review and redesign of workflows to streamline processes, minimize administrative burdens on providers, ensure efficient service delivery, and include dedicated support staff or resources to assist providers with technical troubleshooting, appointment scheduling, and billing processes related to telehealth, within the workflow of the system, which would allow providers to focus on clinical tasks (Lokken et al., 2020). Addressing these human factors issues will require systems-level solutions accounting for technology infrastructure, design of telehealth platforms, training for providers and patients, and environmental considerations. Reframing telehealth as an ergonomics optimization challenge can help sustain its rapid growth while ensuring visits remain productive, effective, and patient-centered (Winters & Winters, 2004).
Conclusion
The rapid adoption of telehealth has transformed healthcare delivery, enhancing accessibility while introducing new ergonomic challenges. Through interviews with audiologists and speech-language pathologists, this study revealed key obstacles including internet connectivity issues, patients’ limited technological literacy, workflow disruptions, increased administrative burdens on providers, and environmental factors compromising patient privacy and care quality. Addressing these ergonomic challenges is crucial for the long-term success of telehealth.
Footnotes
Acknowledgements
We would like to thank our participants for their time and input and acknowledge the Inclusive Security and Privacy focused Innovative Research in Information Technology (InSPIRIT) Laboratory at the University of Denver.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by CISCO Research Award. Any opinions, findings, conclusions, or recommendations expressed in this material are solely those of the authors and not of the organization or the funding agency.