
Abstract
Background:
An understanding of the anatomical development of the fifth metatarsal apophysis is essential for clinical assessment and management of subadult patients presenting with lateral foot pain or oedema that worsens with activity. Despite the common occurrence of subadult lateral foot pain, current understanding of apophyseal development is constrained because of the reliance on plain radiography in the literature, resulting in simplistic descriptions of development. To overcome these limitations, this study aimed to investigate the development of the fifth metatarsal apophysis using 3-dimensional computed tomography analysis, to provide novel morphologic descriptions and normative sex-specific age tables for each developmental stage in a contemporary Australian subadult population.
Methods:
Development and fusion status of the apophysis was scored using a novel 5-stage scoring system on 295 multi-slice computed tomography scans (158 females, 137 males; 0-15 years of age) and 258 lateral, anteroposterior, and oblique radiographs (120 females, 138 males; 0-7 years of age) from the Queensland Children’s Hospital.
Results:
The apophysis commenced ossification as early as 7 years for females and 8 years for males, initially appearing as a thin fleck of bone that elongated to form a crescent shape, with the proximal aspect being wider and extending more medially compared with the distal aspect. Apophyseal fusion demonstrated significant sexual dimorphism with fusion commencing at a mean age of 10.09 years for females and 12 years for males, with the earliest age of complete fusion observed at 9 years for females and 12 years for males.
Conclusion:
This cross-sectional study provides contemporary descriptive reference data for staging development of the fifth metatarsal apophysis and an updated account of its morphology. These observations may assist radiographic interpretation in adolescents; however, the study was not designed to evaluate diagnostic accuracy or clinical outcomes. Further clinical validation is needed before using these data to guide diagnosis or to reduce misclassification of fractures versus apophysitis.
This is a visual representation of the abstract.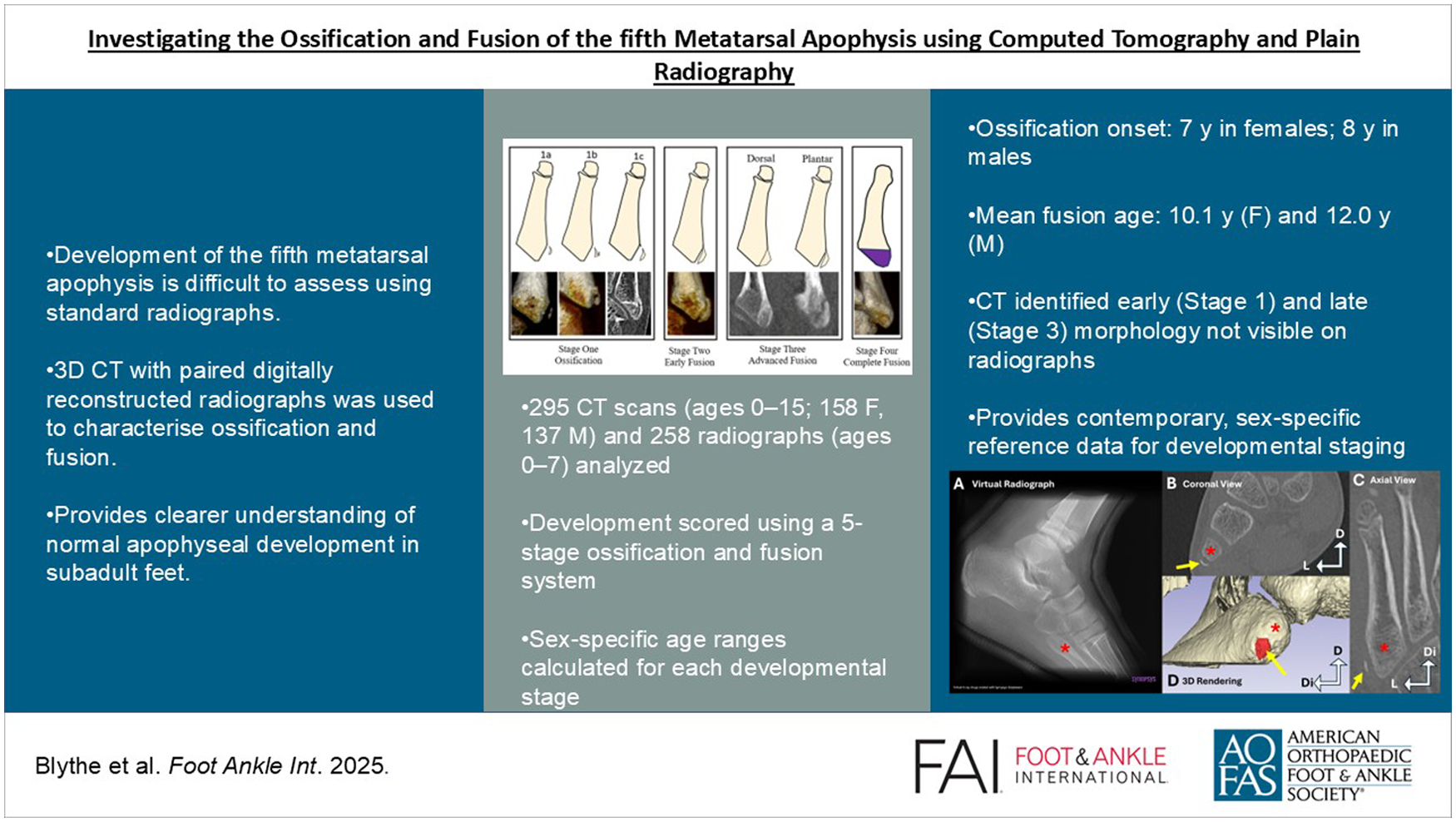
Keywords
Introduction
In Australia, metatarsal fractures are the most common acute or overuse injury of the foot and ankle occurring in approximately 67 per 100 000 individuals annually, with fifth metatarsal avulsion fractures being the main type in 70% of cases.3,10,11,14,16,17 In addition, overuse injuries with corresponding symptomatic pain on the lateral aspect of the foot are commonly seen in clinical assessment of the subadult musculoskeletal system because of the presence of epiphyseal growth plates. 10 Most cases of subadult lateral foot pain are identified as metatarsal apophysitis, which may occur as a result of delayed fusion or fragmentation of the apophysis resulting from increased traction by fibularis brevis and tertius.7,9 Despite the relatively high incidence and diverse range of fifth metatarsal injuries, our understanding of anatomical developmental changes of the apophysis and its anatomical variation is limited. This is echoed by Riccardi et al, 15 who reported an especially high incidence rate of misdiagnosis of fractures of the proximal end of the fifth metatarsal, in which 47% of healthy non-traumatic individuals with apophyses present were misdiagnosed as metatarsal fractures.
The metatarsal apophysis (clinically referred to as Iselin disease) is said to be a small secondary ossification centre shaped as a small fleck of bone located lateral to the base of the fifth metatarsal, appearing at approximately 8-10 years of age in females and 10-15 years of age in males.6,8,12,13,16 Fusion is then described to occur over the next 2 years, with limited reported detail on how fusion occurs, with previous studies restricted to descriptions of “ongoing fusion” and “complete fusion.” The paucity of morphologic descriptions of the ossification and fusion of the apophysis is not surprising given the approach used in previous studies relied entirely on lateral, oblique, and anteroposterior radiographs, resulting in limitations in visualisation of the apophysis because of superimposition and magnification.6,8,16 Although age ranges or mean age in years for each morphologic classification is reported in the above studies, the radiographic limitations mentioned earlier lead to poor or sparse anatomically reported descriptions of ossification and fusion of the apophysis. This underscores the following anatomical gaps in knowledge: (1) does the apophysis ossify from 1 or multiple centres; (2) which direction or orientation does initial and ongoing fusion occur in; and (3) are there any observable anatomical variations in the development of the apophysis that could be misinterpreted as trauma or pathology that should be raised to ensure unnecessary interventions are minimised.
This study uses computed tomography (CT) scans to provide a detailed account of ossification and fusion, overcoming the limitations of radiographic superimposition and magnification allowing for improved visualisation of more complex developmental stages. Analysis of plain radiography scans complements this study to identify the presence of the apophysis in younger age ranges because of limited availability of retrospective CT scans in this age group. This study addresses gaps in the literature on fifth metatarsal apophyseal ossification by improving differential diagnosis in children and adolescents, reducing misdiagnosis through clearer identification, and establishing Queensland-specific assessment standards with updated morphologic descriptions.
Methods
Sample
The study sample consisted of 295 retrospective multi-slice CT (MSCT) scans (158 females; 137 males) and 258 lateral, anteroposterior, and oblique radiographs (120 females; 138 males) of the left or right foot and ankle from separate individuals aged 0-15 years. The upper age limit of 15 years was set using reported ranges of apophyseal development in existing literature, and confirmed through a pilot investigation of individuals aged 15-20 years (60 females, 60 males), with all individuals classified as fused. Of the 553 retrospectively collected MSCT scans and radiographs, 298 individual left feet (149 MSCT; 149 radiographs) and 255 individual right feet (146 MSCT; 109 radiographs) were assessed. Within this sample, plain radiographs were collected from individuals aged 0-7 years (minimum of 17 individuals per age per sex), because of limited availability of MSCT scans in young children. These radiographs therefore supplemented the available CT scans in these younger age categories. From the ages of 8-15 years, only CT scans were used with a minimum of 16 individuals per age per sex.
The scans were collected by a radiologist from the Queensland Health Enterprise PACS database, representing North-Eastern hospitals in Australia. All scans were conducted between 2010 and 2020 on individuals who attended the emergency department for suspected trauma, with the MSCT scans having a maximum slice thickness of 4 mm and slice interval of 0.5 to 2 mm, with a CT scanning parameter range from multiple CT scanners of 80-120 kV, 25-81 mA, and 4-46 table feed per rotation. Scans were excluded from collection if the radiology report described the presence of any metabolic or skeletal disorders that may affect growth or trauma such as fractures to the fifth metatarsal. Sixty individuals within this study were included who had traumatic tibial or fibular fractures. These scans were reviewed and included by a radiologist as the individuals do not have any endocrine, metabolic, or skeletal pathologies that would influence metatarsal bone development (ossification and fusion). To support this, these samples were used in a previous investigation and demonstrated typical calcaneal apophyseal development to individuals without traumatic fractures of the same age and gender. 1 At the Queensland Children’s Hospital, DICOM (digital imaging and communications in medicine) files were imported into OsiriX (Version 4.1, 64 bit; Visage Imaging GmbH) for deidentification with remaining metadata including the patient’s date of scan, age, and sex available to the research team. Ethical approval was granted by The Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee (LNR/19/QCHQ/51243), ratified by the Queensland University of Technology Research Ethics Unit (approval no. 1900000946), and approved by the Queensland Government under the Public Health Act (Section 284) 2020 (RD008018).
Scoring
DICOM data from the 295 (158 females; 137 males) retrospectively collected MSCT scans and 258 plain radiographs (120 females; 138 males) were imported into the software program Horos (version 3.3.6; www.horosproject.org). Using morphologic ossification milestones including ossification centre presence, ongoing fusion, and complete fusion presented by Cunningham et al 4 and existing plain radiographic studies, 5 a novel 5-stage scoring criteria that separates initial and advanced fusion was constructed for application on CT scans (Table 1). The ossification and fusion of the fifth metatarsal apophysis was scored using an MPR view prior to visualising the apophysis using a 3D volume-rendered reconstruction of the CT scans. These 5-stage criteria were also applied to plain radiographs, which were used to substitute the low sample size in the younger age ranges; it should be noted that only stages 0 and 1 were observed in these radiographs, and therefore known limitations of plain radiography were unlikely to have affected ossification scoring in these cases. Digitally reconstructed (virtual) radiographs were generated from selected CT scans to enable comparison of the visualisation and characterisation of the fifth metatarsal apophysis between CT and radiographic modalities, as concurrent radiographs were unavailable because of the retrospective, cross-sectional design of this study.
Five-Stage Morphologic Classification System for the Ossification and Fusion of the Fifth Metatarsal Apophysis Using MSCT Multiplanar Reformatting Views and 3D Volume-Rendered Reconstructions.
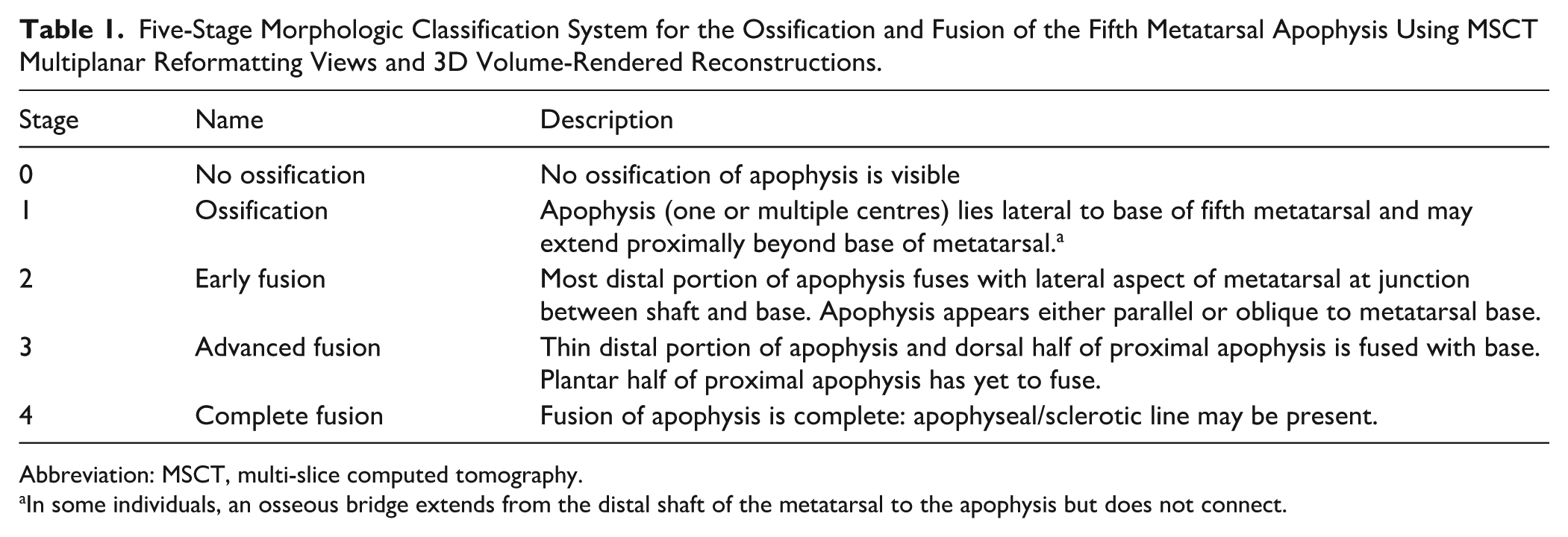
Abbreviation: MSCT, multi-slice computed tomography.
In some individuals, an osseous bridge extends from the distal shaft of the metatarsal to the apophysis but does not connect.
Observer Error
To evaluate intra-observer error and validate the repeatability of the scoring criteria, the first author conducted a repeated assessment of 20 randomly selected MSCT tarsal/foot scans of different ages and sexes on 3 different occasions with a minimum of 24 hours between re-examinations using the novel 5-stage scoring criteria. To quantify inter-observer reliability and validate the application of the scoring criteria, the same 20 MSCT scans were assessed by 2 observers over 1 day. Two observers conducted the radiologic assessments for inter-rater reliability. Both were clinical anatomists with expertise in musculoskeletal development. Observer 1 was a postgraduate anatomy researcher experienced in developing and applying scoring criteria in skeletal imaging studies. Observer 2 was a senior anatomist with extensive experience in musculoskeletal imaging and bone biology. Intra-observer repeatability was measured using a 2-way mixed, single measures intraclass correlation coefficient (ICC) model, with absolute agreement and a consistency-type 95% tolerance interval in SPSS (version 25, 2015; IBM Corporation). Inter-observer reliability was measured using a 2-way random, average measures model with an absolute agreement in SPSS. ICC estimates between 0.75 and 0.9 indicate good agreement and estimates greater than 0.9 indicate excellent measurement reliability.
Statistical Approach
Analyses were performed exploratory rather than hypothesis driven. Descriptive statistics including mean age, SD and minimum and maximum age ranges were calculated for each metatarsal apophyseal stage to compare timing of ossification and fusion using SPSS (version 25; IBM Corporation). A general linear model was used to model the relationship between the independent and dependent variables age (years), sex, and developmental stage of the fifth metatarsal apophysis. Sex, age, and sex × age interactions were tested in the linear model. Sex was found to have a significant effect on the stage of ossification and fusion (P < .001), and therefore male and female samples were split for further analyses. A 1-way analysis of variance with a Tukey post hoc test was also used to determine if mean age (years) was significantly different between stages of apophyseal ossification and fusion.
Results
Analysis of the intra-observer error was undertaken to determine the repeatability of the novel 5-stage scoring criteria over 3 non-consecutive days. An intraclass correlation coefficient of 0.980 (CI: 0.959, 0.991) demonstrated almost perfect agreement over the 3 days. The inter-item correlation matrix demonstrated that scoring accuracy improved over time. Inter-observer reliability demonstrated almost perfect agreement between 2 observers with an intraclass correlation coefficient of 0.973 (CI: 0.930, 0.990), a raw agreement of 83%, and a kappa coefficient of 0.77.
Table 2 provides the frequency, percentage, mean age, and SD for each developmental classification stage for females and males as well as comparisons between neighbouring/consecutive stages. Overall, there was a significant sex effect (P < .001), with females demonstrating significantly earlier timings of ossification and fusion of the fifth metatarsal apophysis. Males demonstrated significant differences in mean age between neighbouring stages; stage 0 and stage 1, stage 1 and stage 2, and stage 3 and stage 4. Females only demonstrated significant differences between stage 3 and stage 4. It should be noted that the mean ages for stages 0 and 4 are biased based on the selected age range investigated, and interpretation of comparisons between stages 0 and 1, and stages 3 and 4 are cautioned.
Frequency, Percentage, and Mean Age for Each Developmental Stage of the Fifth Metatarsal Apophysis for Females and Males Using the Novel 5-Stage Scoring Criteria.
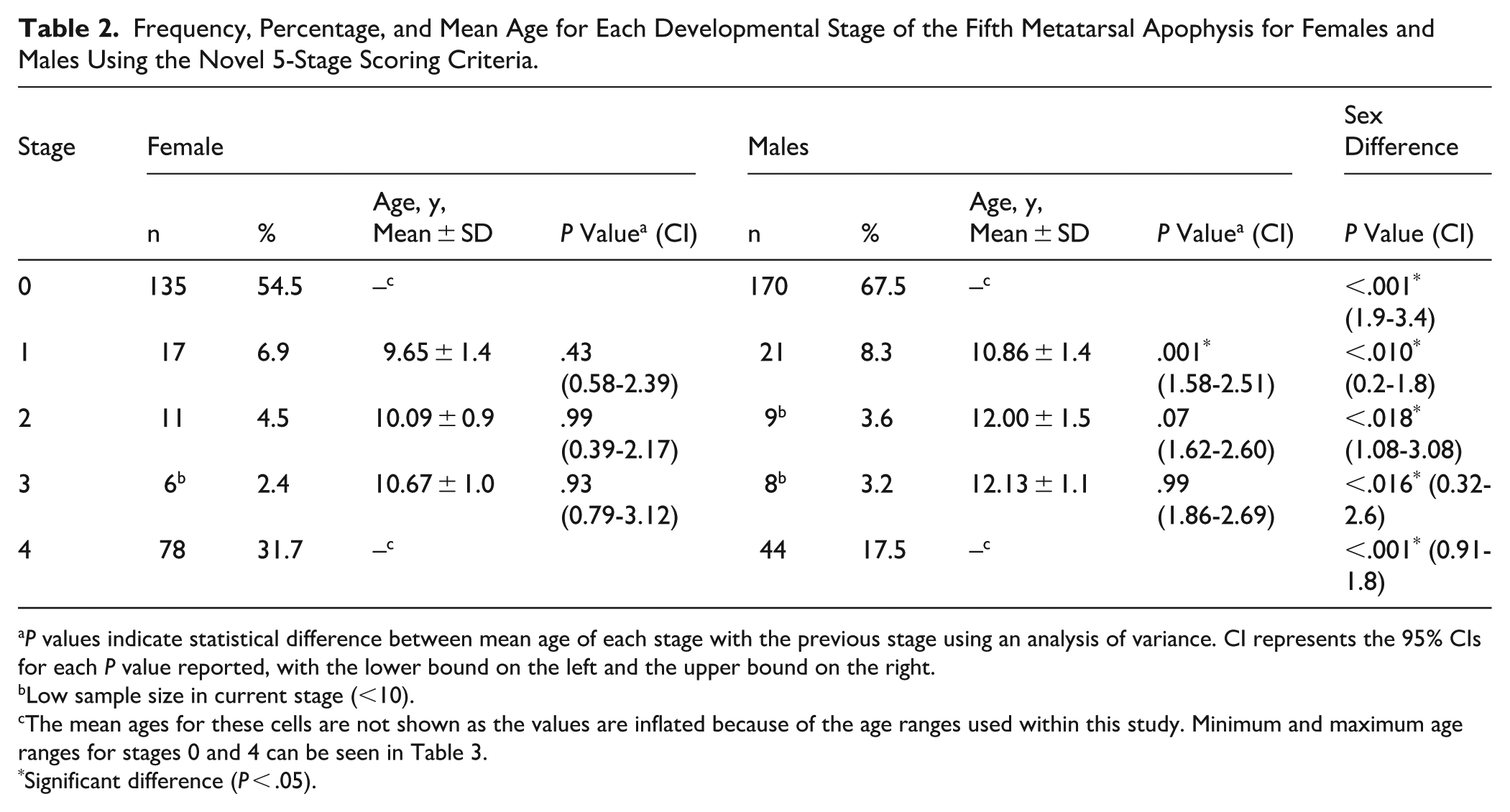
P values indicate statistical difference between mean age of each stage with the previous stage using an analysis of variance. CI represents the 95% CIs for each P value reported, with the lower bound on the left and the upper bound on the right.
Low sample size in current stage (<10).
The mean ages for these cells are not shown as the values are inflated because of the age ranges used within this study. Minimum and maximum age ranges for stages 0 and 4 can be seen in Table 3.
Significant difference (P < .05).
Ossification of the Metatarsal Apophysis
The secondary ossification centre(s) of the base of the fifth metatarsal appeared at a mean age of 9.65 ± 1.4 years for females, and 10.86 ± 1.4 years for males (stage 1) as seen in Table 2, with the earliest age for stage 1 being 7 years for females and 8 years for males. The apophysis appeared as a single small thin platelike secondary ossification centre (n = 33, 68.8%) or as several individual centres simultaneously (n = 15, 31.2%) located lateral along the proximal part of the base of the fifth metatarsal (stage 1) as seen in Figure 1. It should be mentioned that out of the 48 individuals that were scored in stage 1, 39 individuals (81.2%) demonstrated an apophysis located lateral to the proximal aspect of the fifth metatarsal. The remaining 9 individuals (18.8%) demonstrated an anatomical variation in which the proximal aspect of the fifth metatarsal shaft had an osseous extension heading proximally and laterally toward the existing apophysis. The cortical boundaries of the shaft were continuous with this osseous extension with a clear radiolucent gap between it and the apophysis indicating that fusion had not yet commenced. Figure 2 illustrates the differences in visualisation and characterisation of the fifth metatarsal apophysis in a representative case scored as stage 1, comparing the patient’s CT scan with the corresponding digitally reconstructed radiograph, in which the apophysis is not visible.
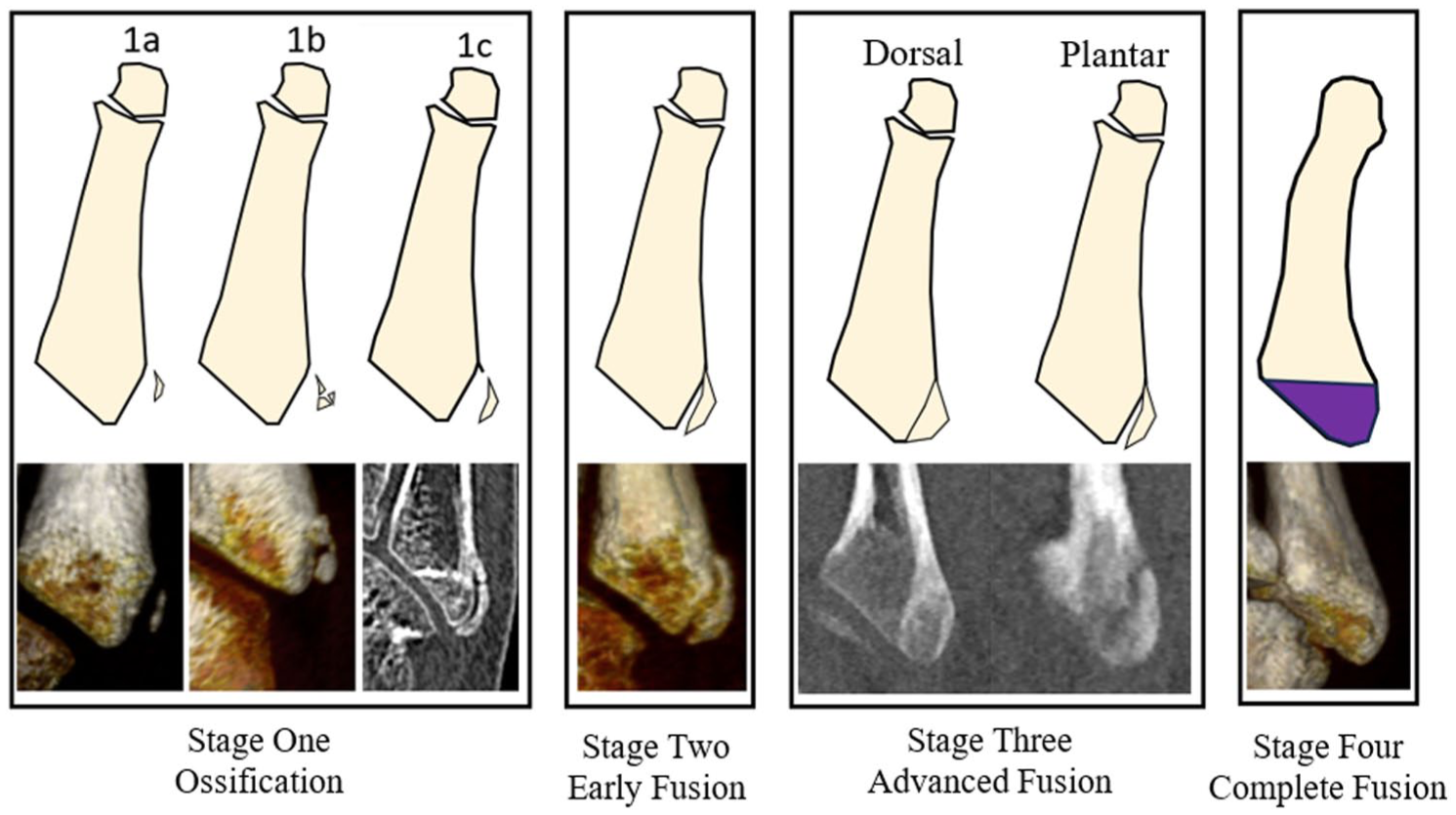
Schematic and example patient computed tomographic (CT) image of each classification stage of metatarsal apophyseal development. Note that the CT images only show the proximal aspect of the metatarsal while the schematic shows the entire metatarsal. Stage zero is not shown because the ossification centre is not present. Stage 1a demonstrates a single ossification centre parallel to the base of the fifth metatarsal observed in 78.8% of the population; stage 1b demonstrates multiple ossification centres (31.2%), and stage 1c demonstrates osseous bridging (18.8%), demonstrating 3 phenotypes of anatomical variation. Stage 2 demonstrates early fusion where the distal aspect of the apophysis is fused to the base of the metatarsal. In stage 3, the fusion is complete dorsally but is incomplete on the plantar surface. Stage 4 shows complete fusion.
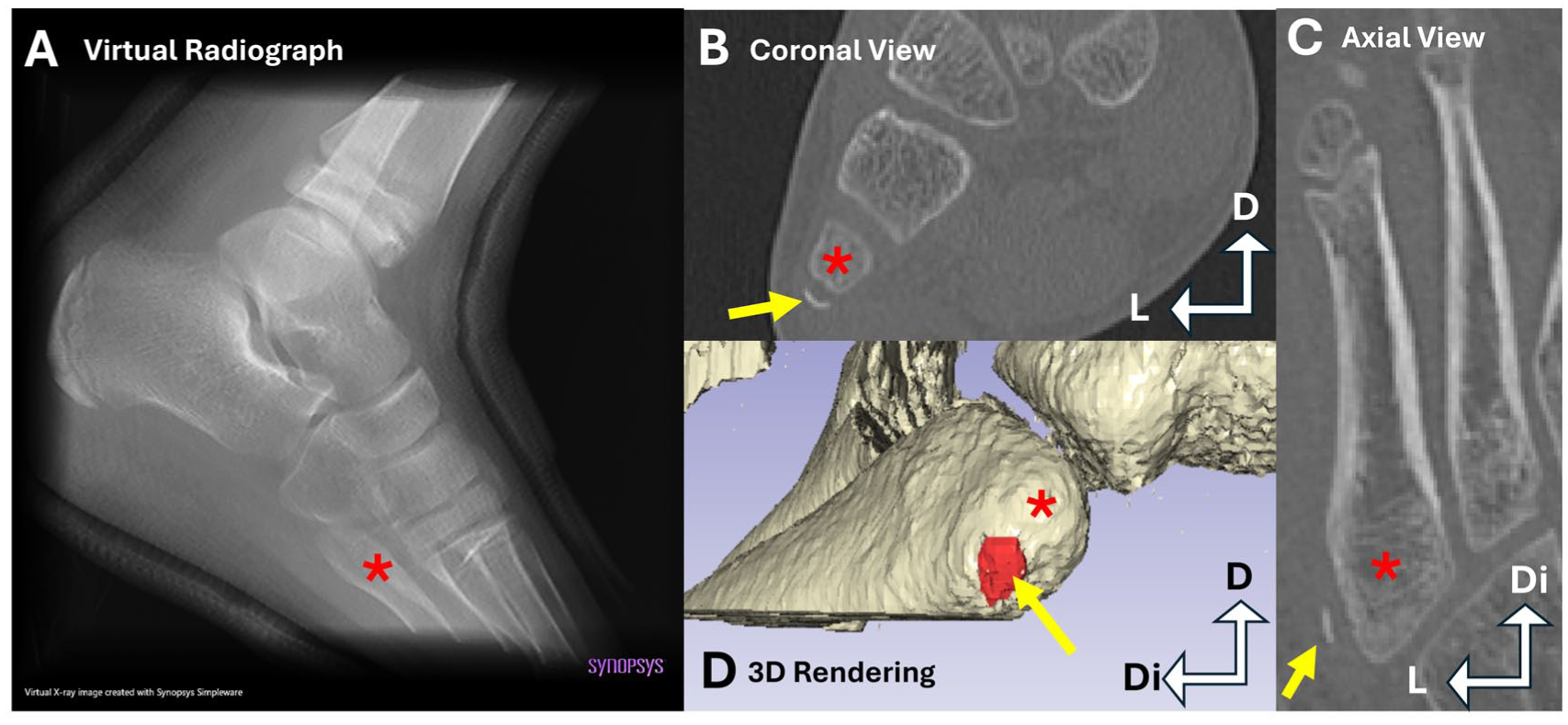
Eight-year-old patient demonstrating stage 1 of fifth metatarsal apophysis ossification visualized using multiplanar reconstructions (MPRs), 3D-MSCT volume rendered reconstruction, and virtual (digitally reconstructed) radiograph. (A) Virtual radiograph created using CT data with no visible ossification center present. (B) Coronal view MPR with apophysis present but not fused (yellow arrow). (C) Anatomical axial MPR with apophysis present but not fused (yellow arrow). (D) 3D reconstruction in a lateral view, with the fifth metatarsal segmented bone color, and the metatarsal apophysis segmented red, indicated by the yellow arrow. Proximal fifth metatarsal (red asterisk), metatarsal apophysis (yellow arrow). D, dorsal; Di, distal; L, lateral; MSCT, multi-slice computed tomography. [See online article for color figure.]
It was inferred that further growth of the apophysis leads the fragmented or thin plate-like multiple secondary centres (if present) to coalesce and elongate and form a baseball bat or crescent-like shape, which extended distal to the base of the fifth metatarsal, with the most distal aspect curving medially. Because the timing and age of ossification is individual dependent, the morphology of the ossifying apophysis varies, ranging from a thin plate-like structure to a large crescent or triangular centre. The proximal aspect of the apophysis elongated superiorly and inferiorly, becoming significantly wider compared to the distal aspect and leading to the apophysis having a triangular shape when viewed laterally.
Fusion of the Fifth Metatarsal Apophysis
Initial fusion of the apophysis (stage 2) commenced with the most distal portion of the apophysis fusing directly to the lateral aspect of the base of the fifth metatarsal. The mean age for initial fusion of the apophysis was 10.09 ± 0.9 years for females and 12.0 ± 1.5 years for males, with a significant sex effect (P < .018; 95% CI 1.08, 3.08). After this, the middle transverse region started to fuse in a distal to proximal fashion, and then progressed in a dorsal to plantar direction, with the plantar aspect being the last to fuse (stage 3), as seen in Figure 3. The mean age for stage 3 was 10.67 ± 1.0 years for females and 12.13 ± 1.1 years for males, with a significant sex effect (P < .016, 95% CI 0.32, 2.6). The mean age for initial fusion and advanced fusion (stage 2 and stage 3, respectively) were not significantly different for either sex. Stages 2 and 3 are easily visualised and characterised using CT; however, when comparing a representative patient’s CT scan at stage 3, the corresponding digitally reconstructed radiograph visualisation is limited, and because of superimposition, the reconstructed apophysis appears separate rather than partially fused, as seen in Figure 3. Complete fusion of the apophysis to the lateral aspect of the base of the fifth metatarsal was observed as early as 9 years for females and 12 years for males as seen in Table 3, with all individuals over 13 years for females and 15 years for males being completely fused.
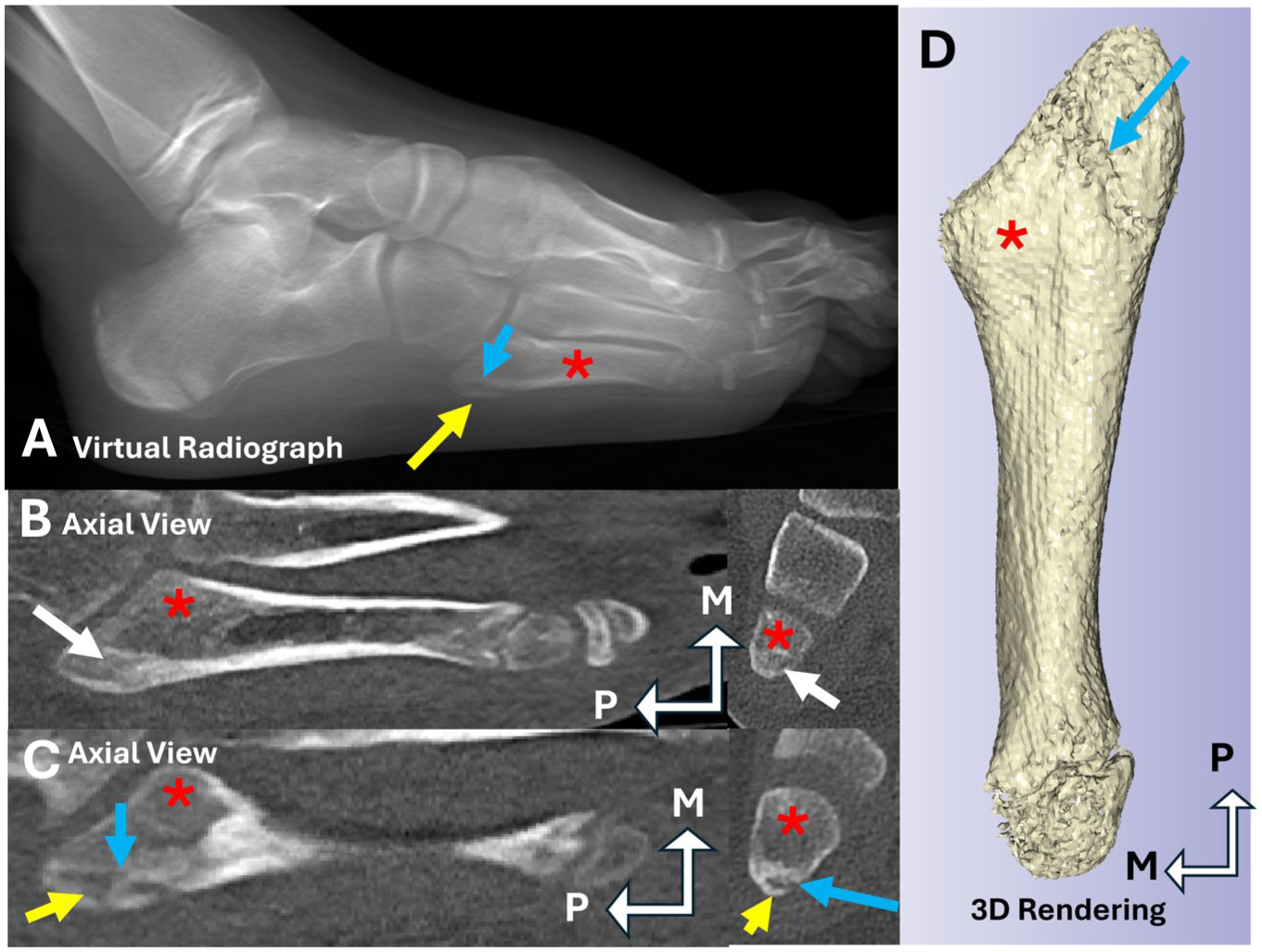
Thirteen-year-old patient demonstrating stage 3 of fifth metatarsal apophysis development visualized using multiplanar reconstructions (MPR), 3D-MSCT volume rendered reconstruction, and virtual (digitally reconstructed) radiograph. (A) Virtual radiograph created using CT data with apophysis present (yellow arrow), with radiolucent space located between the apophysis and the proximal end of the fifth metatarsal (blue arrow). (B) Anatomical axial view MPR of the dorsal aspect of the apophysis and metatarsal, demonstrating complete fusion of the dorsal aspect (white arrow). (C) Anatomical axial view MPR of the plantar aspect of the apophysis and metatarsal, with the apophysis still unfused, indicated by the radiolucent gap (blue arrow). (D) Inferior/plantar view of a 3D reconstruction with the fifth metatarsal segmented bone color, with a gap in the segmentation indicating non-union of the most plantar aspect of the apophysis to the metatarsal (blue arrow). Proximal fifth metatarsal (red asterisk), unfused metatarsal apophysis (yellow arrow), fused aspect of metatarsal apophysis (white arrow), non-union of apophysis to metatarsal (blue arrow). CT, computed tomography; M, medial; MSCT, multi-slice computed tomography; P, proximal. [See online article for color figure.]
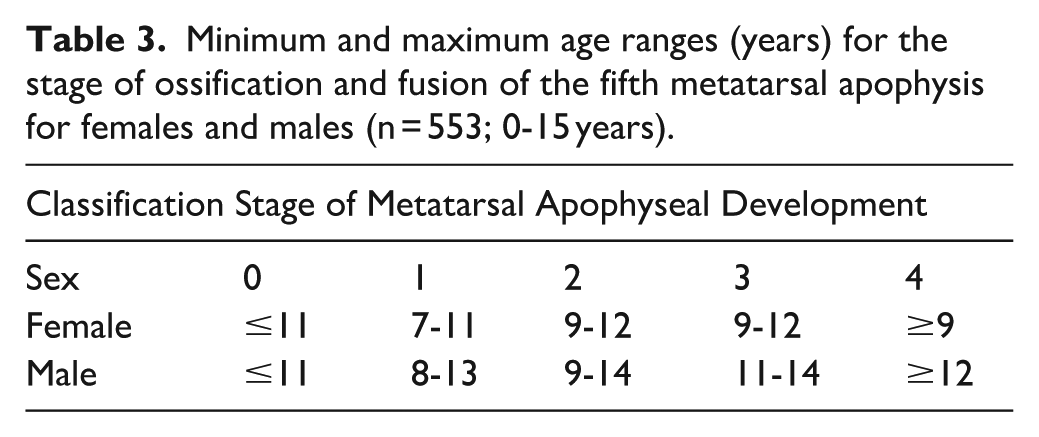
Minimum and maximum age ranges (years) for the stage of ossification and fusion of the fifth metatarsal apophysis for females and males (n = 553; 0-15 years).
Discussion
This is the first study to describe age-associated morphologic appearances of the fifth metatarsal apophysis using CT, overcoming the previous limitations of dry bone and radiographic studies. It is the first to report the timings of apophyseal appearance and fusion in an Australian contemporary population. The intended use of the outcomes reported in this study are primarily research based, to improve the reader’s anatomical understanding on the ossification and fusion of the metatarsal apophysis. However, the contemporary sex-specific mean ages (years) and lower and upper age (years) bounds for each developmental stage could be applied within a clinical or forensic setting.
In this study, we observed that the apophysis initially appears as a single secondary ossification centre or as several centres clustered lateral to the proximal surface of the base of the fifth metatarsal. To our knowledge, this is the first study to report that the apophysis can develop from multiple secondary ossification centres, and under-representation of this observation may be due to superimposition and limited visualisation of 3-dimensional centres using lateral and oblique radiographs in earlier studies. 15 Previous studies have reported fragmentation and widening of the apophysis in cases of fifth-metatarsal traction apophysitis2,7; however, this fragmentation may simply be the presence of multiple ossification centres before they coalesce, as seen in our CT population.
In our study, females demonstrated significantly earlier ossification of the apophysis compared with males, at 9.81 ± 1.2 and 10.86 ± 1.4 years, respectively, with the earliest appearance being 7 years for females and 8 years for males. The appearance of the apophysis for females in our study ranged from 7 to 11 years, with the upper range being supported by lateral radiographic studies by Dameron 5 in a North American population and Davies et al 6 in a UK population, who identified apophyseal appearance to be 8-11 years and 8-13 years, respectively, for females. The earlier age of appearance for the females in our study may be due to improved visualisation in CT compared with earlier radiographic studies. Apophyseal appearance for males in our study ranged from 8 to 13 years, with the upper age limit supported by Dameron 5 and Davies et al, 6 who reported the most common age range of appearance as 8-14 years and 10-14 years, respectively, for males. Rather than an age range, the North American study by Hoerr et al 12 reported the mean age of ossification to be 9.7 ± 1.2 years for females and 12 ± 1.3 years for males.
Our study is the first to describe variation in the initial fusion of the apophysis to the proximal base via an osseous extension, likely due to limitations in visualisation of the apophysis in plain radiography. Initial fusion for females ranged from 9 to 12 years (mean age 10.09 ± 0.9 years) and for males ranged from 9 to 14 years (mean age 12.0 ± 1.5 years), with fusion occurring as early as 9 years for both sexes. The female results are similar to those reported by Davies et al 6 at 8-12 years. For males, Davies et al 6 reported fusion between 11 and 14 years, supporting the upper age range found in our study. Davies et al 6 classified fusion as “fusion ongoing,” which could include apophyses that are starting to fuse, undergoing active fusion, or complete fusion without obliteration of the apophyseal line, resulting in age ranges that are broad and nonspecific.
Using multiplanar reconstructions, we were able to visualise an advanced fusion category that has not been previously described, with the middle transverse portion of the apophysis fusing in a distal to proximal plane. Continued fusion occurred in a dorsal to plantar direction, with the plantar-proximal aspect of the apophysis being the last to fuse (stage 3). Although the mean ages between initial fusion and advanced fusion (stages 2 and 3) were not statistically different, understanding the morphologic changes may help interpret clinical symptoms leading to lateral foot pain in individuals. Complete fusion was first observed as early as 9 years in females and 12 years in males, supported by Davies et al 6 who measured complete fusion as the apophyseal line being obliterated. In our sample, all individuals over the age of 13 years for females and over the age of 15 years for males were completely fused. To avoid age bias when investigating a wide age range, the minimum and maximum age ranges for each developmental stage in our study are reported in Table 3.
Limitations
Because of the retrospective nature of this study, the frequency of individuals seen in each developmental stage is uneven, specifically in stages 0 and 4. The frequency for these stages is biased based on the selected age range investigated (0-15 years), and comparisons between neighbouring stages are cautioned. To minimise the use of mean ages for these stages, the earliest and latest age observed for each developmental stage have also been reported (Table 2).
Although the primary purpose of this study was to improve anatomical understanding around the development of the fifth metatarsal apophysis, the scoring system created and implemented has only been validated within our cohort, and it is recommended that it be prospectively validated in future studies using symptomatic and asymptomatic patient cohorts to correlate with patient outcomes.
Conclusion
We provide contemporary, sex-specific reference data and morphologic descriptors for fifth-metatarsal apophyseal development, derived from CT with paired digitally reconstructed radiographs. Early ossification (stage 1) and advanced fusion (stage 3) are often not reliably visualized on radiographs alone, which can invite misinterpretation. Although CT is not routine in pediatric foot imaging, CT-informed age ranges and morphology can support more cautious radiographic interpretation and help distinguish normal variation from apophysitis or fracture, reducing overdiagnosis without claiming diagnostic accuracy.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251398523 – Supplemental material for Investigating the Ossification and Fusion of the Fifth Metatarsal Apophysis Using Computed Tomography and Plain Radiography
Supplemental material, sj-pdf-1-fai-10.1177_10711007251398523 for Investigating the Ossification and Fusion of the Fifth Metatarsal Apophysis Using Computed Tomography and Plain Radiography by Connor S. Blythe, Aaron P. Robertson and Laura S. Gregory in Foot & Ankle International
Footnotes
Acknowledgements
We appreciate the continued support provided by the radiology team in the Department of Medical Imaging and Nuclear Medicine at the Queensland Children’s Hospital, in particular, Dr Gillian Long for their time in collecting the MSCT data.
Ethical Considerations
Ethical approval was granted by The Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee (LNR/19/QCHQ/51243), ratifed by the Queensland University of Technology Research Ethics Unit (Approval No. 1900000946) and approved by the Queensland Government under the Public Health Act (Section 284) 2020 (RD008018).
Informed Consent
Informed consent is impossible to obtain due to the anonymised nature of this retrospective study, and therefore consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are not publicly available because of privacy or ethical restrictions but are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.