
Abstract
Background:
Syndesmotic complex injuries are supposedly associated with injuries to the deltoid ligament (DL) complex. Several syndesmosis classifications take DL injuries into account when rating the stability of the syndesmotic injury. Still, no study has yet assessed the frequency and severity of DL injuries in unstable syndesmotic injuries. The aim of this retrospective cohort study was to assess both the severity of the syndesmotic and DL injury in patients undergoing surgery for an unstable syndesmotic injury.
Methods:
The integrity of the syndesmotic and DL complex of 37 patients were assessed on MRI by 2 musculoskeletal radiologists. Eligible were adult patients with an acute, isolated, unstable syndesmotic injury (ligamentous or bony avulsions) who underwent surgery. The DL complex was classified as having 3 superficial (TNL/TSL/TCL) and 2 deep (aTTL/pTTL) components. Grade 0 indicated an intact ligament; grade I showed a periligamentous edema; grade II a partial tear presenting as laxity, irregular contour, or partial discontinuity with concomitant hyperintense signaling; grade III a complete tear; or grade IV in case of an avulsion fracture. Frequency and severity of DL injuries were assessed, and possible injury combinations analyzed using an h-cluster analysis and Mann-Whitney U test.
Results:
Mean severity (grade 0-3) was 2.6 ± 0.8 for the syndesmotic complex and 1.6 ± 1.1 for the DL (superficial 1.5 ± 1.1, deep 1.6 ± 1.1). Seven patients (19%) had no (n = 3; 8%) or minor (grade 1: n = 4; 11%) DL injuries. Overall, 2 different patient clusters and 4 separate ligament clusters were identified.
Conclusion:
Unstable syndesmotic injuries can occur isolated or with an accompanying DL injury. There appears to be a great heterogeneity between the severity of syndesmotic and deltoid ligament injuries.
Introduction
The ankle joint is stabilized by bony and ligamentous structures. The syndesmotic and deltoid ligament (DL) complex are 2 of the predominant ligamentous stabilizers. The syndesmotic complex stabilizes the bony ankle mortis, that is, the distal tibiofibular joint. The anterior inferior tibiofibular ligament (AiTFL), the interosseous ligament (IOL), and the posterior inferior tibiofibular ligament (PiTFL) resemble a flexible, 3-point suspension from the fibula to the tibia. 35 The DL complex on the other hand stabilizes the talus on the medial side. It comprises a superficial and a deep layer. The superficial layer is made of 4, and the deep layer of 2, different portions. It is believed to center the talus underneath the tibia and to prevent external talar rotation and valgization.6,25
Therefore, the syndesmotic and DL complex contribute to the ankle joint stability, possibly especially for external rotation, but at different anatomical locations. There is an ongoing debate on whether injuries to either complex should be classified together or separately. The authors are aware of 9 different classifications for syndesmotic injuries5,9,10,14-16,21,22,28 with 5 classifications including injuries to the DL complex.5,9,14,21,28 These 5 classifications vary in almost all aspects and are close to incomparable. Only 1 classification differentiates between different severities of DL injuries 21 and only 1 classification chooses an injury to the DL complex to differentiate a stable (grade IIa) from an unstable (grade IIb) injury. 5
Although 5 of 9 classifications on syndesmotic instability incorporate an injury to the DL into their treatment algorithm, actual data on the frequency of DL injuries in patients suffering a syndesmotic injury is sparse.5,24,28 The authors are not aware of any study explicitly assessing the frequency and severity of injuries to the DL complex in patients with an unstable syndesmotic injury.
Therefore, the aim of the current study was to assess the frequency and severity of DL injuries in patients who underwent surgery for an unstable syndesmotic injury.
Material and Methods
The herein presented study is a retrospective radiographic study.
Diagnostic, Classification, and Treatment Algorithm
At our foot and ankle department, a clearly defined diagnostic, classification, and treatment algorithm for patients with a suspected, isolated, syndesmotic injury is followed (Figure 1). 29 In brief, if the specific clinical examination raises the suspicion for a syndesmotic injury, an MRI including axially oblique imaging planes of the syndesmotic complex is performed. If there is a concomitant ligamentous or bony avulsion injury of the AiTFL and PiTFL, the distal tibiofibular joint (DTFJ) is considered unstable and surgical treatment is recommended. In case the AiTFL is ruptured but the PiTFL is intact, a bilateral external rotation stress test (ERST) under fluoroscopy is performed. Any side-by-side widening of the medial clear space is indicative for an AiTFL and IOL rupture. 30 Because of the subsequent translational and rotational instability of DTFJ, patients are recommended to undergo surgical stabilization. An isolated sprain of the AiTFL, that is, no medial clear space widening in the external rotation stress test, is treated nonoperatively.
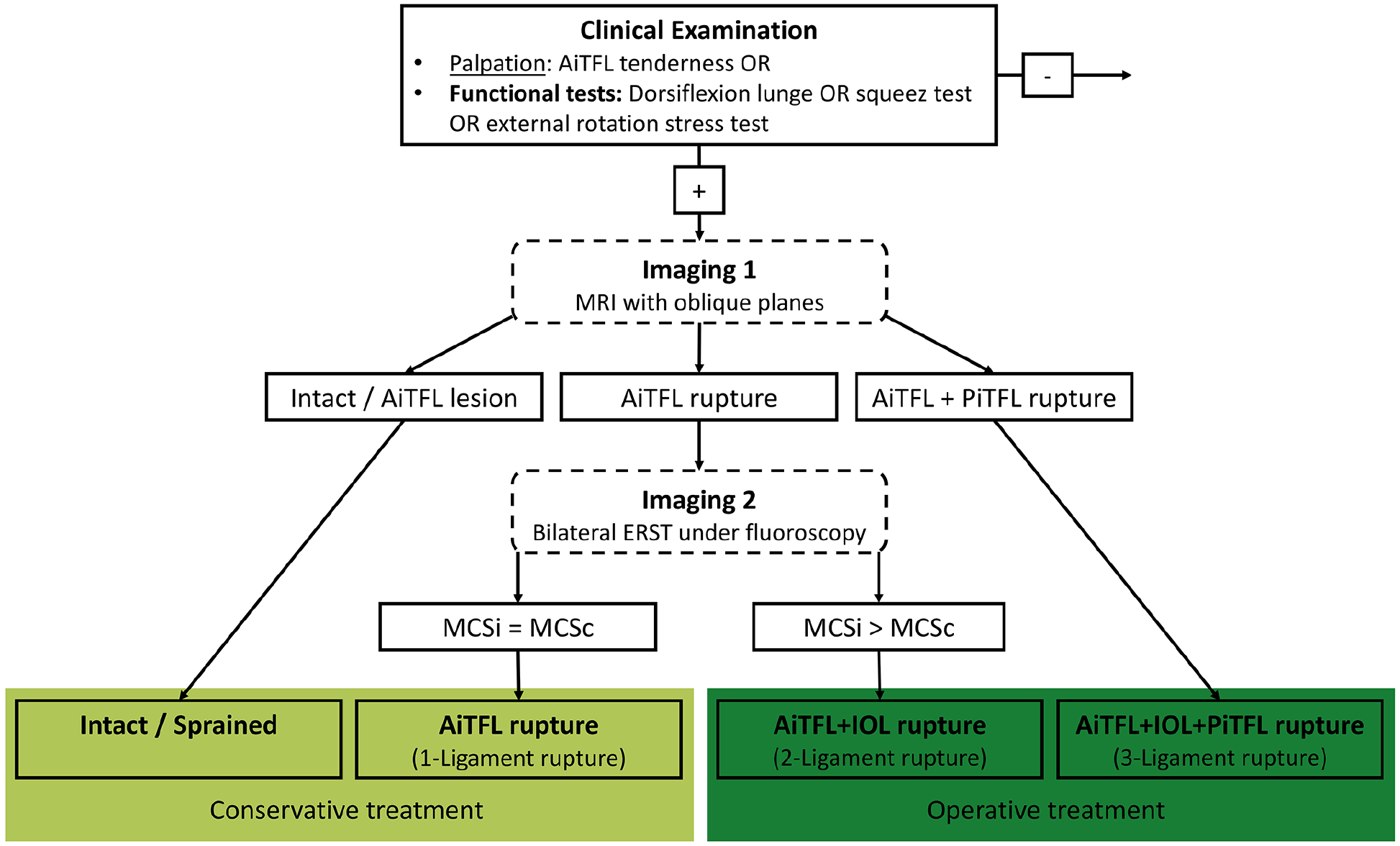
Flowchart illustrating the applied diagnostic algorithm. AiTFL, anterior inferior tibiofibular ligament; ERST, external rotation stress test; MCSc, medial clear space contralateral ankle; MCSi, medial clear space injured ankle; MRI, magnetic resonance imaging; PiTFL, posterior inferior tibiofibular ligament.
Patient Selection
Eligible were adult patients (≥18 years) who were treated surgically for an acute, isolated syndesmotic injury at the foot and ankle department of a single level 1 trauma center between September 1, 2019, and May 15, 2023. Acute was defined as within the first 21 days after injury. Isolated syndesmotic injury was defined as either a purely ligamentous injury or a bony avulsion of the AiTFL or PiTFL. An accompanying DL injury was no exclusion criteria. Excluded were patients with any other additional fractures, including Maisonneuve fractures.
Patients were identified via the hospital’s clinical database per the following OPS: 5-806.3 (suture of the syndesmosis), 5-806.a (ligament repair of the syndesmosis), 5-869.2 (syndesmotic screw / suture-button / augmentation), and 5-806.c (suture of the lateral ligament complex). After removal of duplicates, 2 independent reviewers (F.M., S.F.B.) screened all patients and removed fracture cases, but bony avulsion injuries to the AiTFL (Tubercule de Chaput, Wagstaff fragment) or PiTFL (posterior malleolus fractures affecting the posterolateral corner of the distal tibia). Next, a third reviewer (F.P.G.) excluded chronic cases (≥22 days after trauma) and patients without an MRI available in our radiologic database. The remaining patients were eligible for further analysis.
Clinical Data Collection
The same reviewer (F.P.G.) conducted the further clinical data collection that included general demographics and surgical treatment details.
MRI and Image Analysis
All MRI examinations were performed on a 1.5 (n = 23) or 3-tesla (T) magnet system (n = 15) using a dedicated ankle coil. The quality of the external MR protocols was checked by a board-certified radiologist with 9 years of expertise in musculoskeletal imaging (NH) to meet the in-house standard.
MRI examinations were analyzed by 2 board-certified musculoskeletal radiologists from the same level 1 trauma center (N.H., P.R.) with 9 and 8 years of experience, respectively, in a consensus reading. The following ligaments were assessed on MRI (Figure 2): The syndesmotic complex (AiTFL, IOL, and PiTFL) and the DL complex according to Schneck et al 26 : superficial DL (SDL) layer: the tibionavicular ligament (TNL), the tibiospring ligament (TSL), and the tibiocalcaneal ligament (TCL); deep deltoid (DDL) layer; the deep anterior tibiotalar ligament (aTTL) and posterior tibiotalar ligament (pTTL). Each of these ligaments was graded per the severity of the injury according to Jeong et al 13 : grade 0 indicated an intact ligament, grade I was characterized by periligamentous edema, grade II by a partial tear presenting as laxity, irregular contour, or partial discontinuity with concomitant hyperintense signal of the ligament, and grade III by a complete tear of the ligament. Avulsion fractures represent a grade IV.
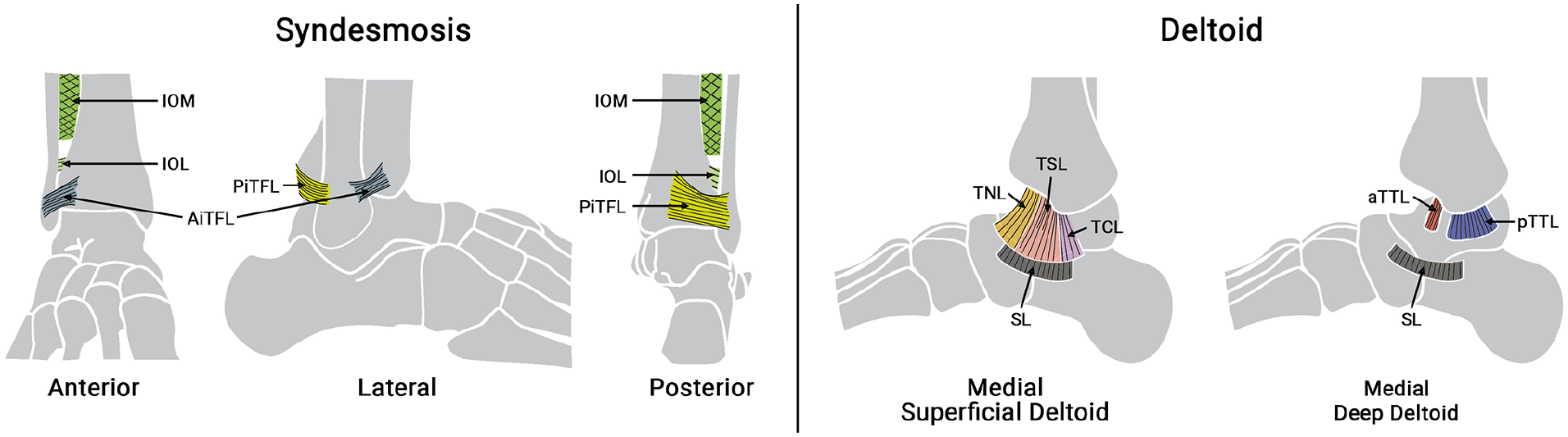
Illustration of the anatomical structures assessed during MRI reading: Syndesmosis and Deltoid ligament complex. AiTFL, anterior inferior tibiofibular ligament; aTTL, deep anterior tibiotalar ligament; IOL, interosseous ligament; IOM, interosseous membrane; PiTFL, posterior inferior tibiofibular ligament; pTTL, deep posterior tibiotalar ligament; SL, spring ligament; TCL, tibiocalcaneal ligament; TNL, tibionavicular ligament; TSL, tibiospring ligament.
Data Analysis and Statistics
Frequency and severity of DL injuries in unstable syndesmotic injuries were assessed using an adapted heat map. To provide a comprehensive overview, standard descriptive statistics were calculated and values were presented as mean ± SD. In order to qualitatively assess a possible injury combination, a hierarchical cluster analysis was conducted using the heatmap function in R. The Ward.D2 linkage method was used with an aim to minimize the total within-cluster variance when merging clusters, resulting in compact and well-separated clusters. Given the ordinal nature of data, Spearman correlation distance was adopted.
To ensure the reliability of the clustering results, several methods were used. First, the Silhouette score plot was included to identify misclassified observations and assess overall clustering quality. Bootstrapping through permutation was then applied to evaluate the significance and stability of the clusters. Consistent outcomes were observed when experimenting with different hierarchical clustering linkage methods. These steps collectively ensured the robustness of the identified clusters.
Finally, the identified patient cohorts were compared using a Mann-Whitney U test and further analyses using a Pearson correlation. Because of multiple testing, a Bonferroni alpha-level correction was conducted, setting the level of significance to .007. Statistics were computed in SPSS, version 29.0.1.0 (IBM Corp) and R, version 4.4.0 (R Foundation for Statistical Computing).
Results
Patient Selection
Of the 593 patients identified per the database query, 62 patients had an acute, isolated syndesmotic injury, and an MRI was available for 37 patients (60%). These patients were included in the further analysis. The patient selection is outlined in Figure 3.
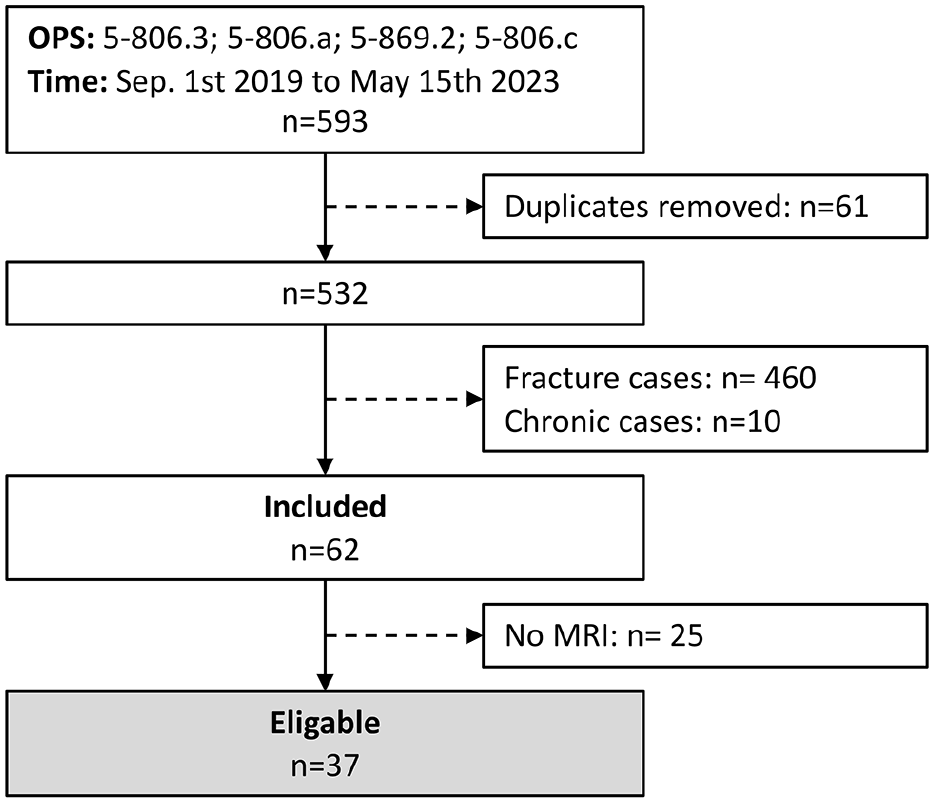
Patient selection flow chart. MRI, magnetic resonance imaging.
Demographics and Treatment
The patients were on average 35 ± 12 years of age, 43% females. The syndesmotic instability was treated by a single suture button system in 28 patients (74%), by a 2-suture button system in 4 patients (11%) and by a suture button system and deltoid repair in 5 patients (13%).
Ligament Injuries Graded on MRI
The mean severity (grade 0-3; PMF = grade 4) for the syndesmotic complex was 2.8 ± 0.9, for the DL complex 1.5 ± 1.1 (SDL 1.5 ± 1.1, DDL 1.6 ± 1.1). In more detail, all patients (100%) had a complete rupture of the AiTFL, 36 patients (97%) a grade 3 (n = 34; 92%) or grade 2 injury (n = 2; 5%) of the IOL, and 25 patients (68%) a complete (grade 3: n = 4, fracture to the posterior malleolus: n = 14; 49%) or grade 2 injury (n = 6; 16%) of the PiTFL. Per the DL, any injury (grade 1-3) was present to the TNL in 76% (grade 3: 38%), TSL in 76% (grade 3: 19%), TCL in 70% (grade 3: 11%), aTTL in 92% (grade 3: 62%), and pTTL in 68% (grade 3: 0%). Overall, 7 patients (19%) had no (n = 3; 8%) or only minor (grade 1: n = 4; 11%) injuries to the DL complex.
The ligament scoring of each patient is presented as a heat map in Figure 4. The columns represent the individual patients, and the rows the individual ligaments analyzed. The color coding indicates the grade of the ligament injury.
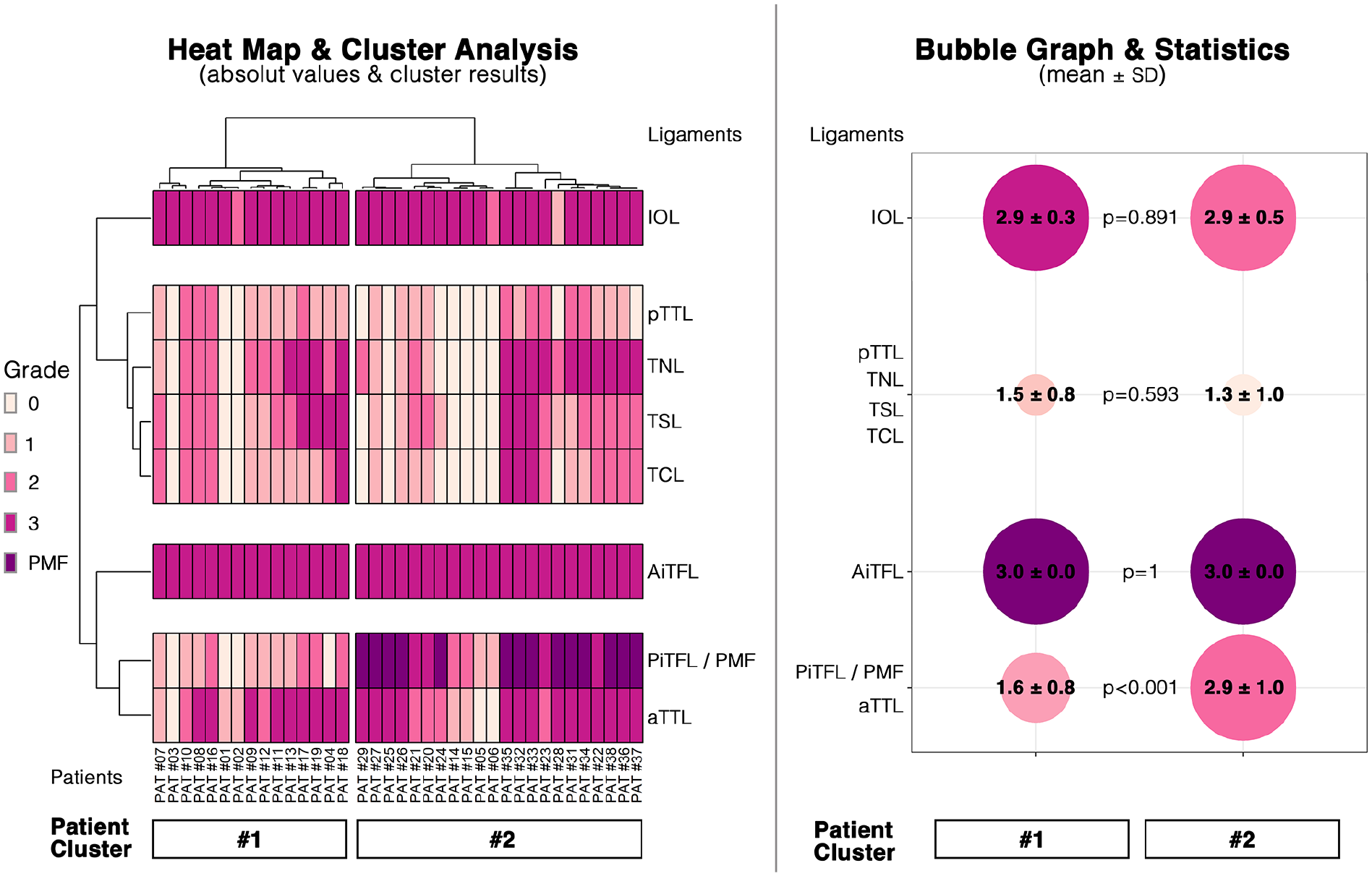
Results of the cluster analysis. Left: Heat map illustrating the grade of ligament injury for each patient. The heat map is divided per the results of the cluster analysis. There are 2 specific patient and 4 specific ligament clusters. Right: Bubble Graph illustrating the cumulative results (mean ± SD injury severity) for each cluster. AiTFL, anterior inferior tibiofibular ligament; aTTL, deep anterior tibiotalar ligament; DL, deltoid ligament; IOL, interosseous ligament; PiTFL, posterior inferior tibiofibular ligament; PMF, posterior malleolar fracture; pTTL, deep posterior tibiotalar ligament; TCL, tibiocalcaneal ligament; TNL, tibionavicular ligament; TSL, tibiospring ligament. [See online article for color figure.]
Cluster Analysis of Syndesmotic and DL Injury
Based on the individual values, a cluster analysis was performed. The corresponding dendrogram, separate for the patients and the ligaments, is presented alongside the heat map. Two separate patient clusters were identified (grouped columns). The ligaments clustered into 4 groups, that is, the IOL, the AiTFL, the pTTL/TNL/TSL/TCL, and the PiTFL/PMF/aTTL.
The complete cluster analysis and its robustness testing can be found in Supplemental Material 1.
The mean ± SD values of each patient and ligament cluster were calculated and are presented as a bubble graph (Figure 4). Overall, the 2 patient clusters only differed significantly per the severity of the PiTFL/PMF and aTTL group (P < .001). The injury severity of the PiTFL/PMF is only correlated to the injury severity of the aTTL (r = 0.553; P < .001), but to no other deltoid ligament injury (TNL [r = 0.395, P = .014], TSL [r = 0.229, P = .167], TCL [r = 0.247, P = .135], pTTL [r = 0.154, P = .355]).
In order to account for the misclassification risk given by the low sample size, a silhouette score was used. Silhouette score uses silhouette length, which is a measure of how similar an object is to its own cluster (cohesion) compared with other clusters (separation). Negative values indicate that the object may be assigned to the wrong cluster. It ranges from −1 to 1, where a high value indicates that the object is well matched to its own cluster and poorly matched to neighboring clusters.
The silhouette values for all patients is positive, with a high average silhouette length of 0.6, emphasizing on the confidence in clusters. For ligaments, the silhouette values for AITFL and IOL are zero because there are overall only 3 injuries. The membership of aTTL to cluster 3 could be discussed as it gets a negative silhouette value. This might be because looking at the individual values for each patient, aTTL seems to be correlated with TNL. So aTTL might be closer to TNL and its cluster than to PiTFL/PMF. In general, the misclassification risk can be considered low.
To evaluate the uncertainty inherent in hierarchical cluster analysis and check the validity of final groups, a permutation method involving multiscale bootstrap resampling was employed using the R package pvclust. This approach calculates P values for each cluster within the hierarchical clustering framework. These P value percentages, ranging between 0 and 100, serve as indicators of the level of support the data provides for each cluster, thereby quantifying the strength of their association.
PVclust offers two distinct types of P values as shown in the plot: AU (approximately unbiased) P value and BP (bootstrap probability) value. The AU P value, derived through multiscale bootstrap resampling, represents a more reliable estimate of an unbiased P value compared to the BP value obtained through standard bootstrap resampling methods.
Here, the AU values for the 4 ligament clusters are 90, 95, 88, and 92, which are high and indicate stronger statistical support for the clusters, suggesting that the observed clustering patterns are unlikely to be a result of random chance alone.
Discussion
The herein presented study focused on accompanying deltoid injuries in unstable syndesmotic injuries. The cluster analysis revealed 2 different patient clusters, which only differed significantly per the injury severity of the PiTFL/aTTL. Overall, there did not appear to be a correlation between the injury severity of the syndesmotic complex and the DL injury.
In various publications, authors state that isolated DL injuries are rare, and usually occur in combination with injuries of the lateral collateral ligament (75%) and much less often with syndesmotic (10%) injuries. 17 In chronic lateral ankle instability, concomitant DL injuries have been reported in 36% to 72% of cases.7,8,11 But when looking at the available primary literature, it becomes obvious that data on DL injuries in patients with syndesmotic injuries is sparse. Based on the data available, DL injuries apparently occur in 8% to 50% of patients with an injury to the syndesmotic complex.5,24,28 Roemer et al 24 reported, that a syndesmotic injury had only a borderline risk increase for a medial side injury (adjusted odds ratio: 2.24). Contrary, the current study found some sort of DL injury in 82% of patients with an unstable syndesmotic injury. A possible explanation for the diverging results could be the way the DL complex was assessed. None of the above-cited studies assessed the different layers of the DL complex or the actual injury severity. Jeong et al 13 facilitated the opposite approach compared to the current study. They analyzed MRIs of 36 patients with an acute DL injury. The medial side injury distribution was as follows: TNL = 83% (grade 3: 50%), TSL = 100% (grade 3: 42%), TCL = 97% (grade 3: 43%), aTTL = 92% (grade 3: 21%), and pTTL = 100% (grade 3: 40%). Overall, the injury distribution for the SDL was similar, for the DDL different, to the herein observed distribution. They did not report the number of accompanying syndesmotic injuries. Overall, concomitant DL injuries occur frequently in unstable syndesmotic injuries.
Several authors have postulated an association between the severity of the syndesmotic injury and severity of the DL injury.5,28 Calder et al 5 reported that a combined injury to the AiTFL and DL was highly predictive for an unstable syndesmotic injury. To the authors’ understanding the correlation is based on the similar injury mechanisms, that is, hyperdorsiflexion and external rotation. 18 In general, both the syndesmotic and DL complex contribute to ankle stability.3,4,27,32 Per the DL complex, the SDL is believed to resist external rotation, and the DDL limits posterior and lateral translation of the talus.6,12,20 Interestingly, this correlation could not be observed in the current study. A higher-grade syndesmotic injury apparently only correlated to a more severe injury to the aTTL. No correlation could be found to the severity of an SDL (TNL, TSL, TCL) or pTTL injury.
For Calder et al, 5 the primary discriminator between a stable and an unstable syndesmotic injury is an accompanying injury of the DL complex. But 18% of the patients presented herein had no relevant injury (grade ≤1) to the SDL or DDL. Still, all these patients had an unstable syndesmotic injury. The European Society for Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) consensus recommendations 33 also focus on the DL. Per their line of argumentation, the DDL is the second structure after the AiTFL to be injured in a syndesmotic injury. The herein presented data only partially supports this line of argumentation. Overall, there appears to be a rather heterogeneous distribution between syndesmotic- and deltoid ligament injuries. This does stress the need for a clear anatomical classification of syndesmotic injuries, independent from an injury of the DL complex. Syndesmotic injuries should therefore not be classified in combination with a medial side injury, but rather separately per the ligaments ruptured, that is, the AiTFL, IOL, and PiTFL.
Of the 18% of patients with no relevant deltoid injury (grade ≤1), all patients had a 2-ligament injury (AiTFL+IOL) of the syndesmotic complex. On the other hand, 16% of patients had a severe injury of both the SDL and DDL (grade ≥2), 50% of which had a 3-ligament (AiTFL+IOL+PiTFL/fracture to the posterior malleolus) syndesmotic injury. This heterogeneity was also revealed by the cluster analysis. One can therefore argue that syndesmotic and deltoid ligament injuries should be assessed separately. But a syndesmotic injury should raise the awareness for an accompanying DL injury.
Several limitations and strengths of the study should be discussed. First, the DL injury has been assessed by MRI, not by direct visualization or arthroscopy. Arthroscopy has the major limitation that it is an invasive diagnostic tool. MRI on the other hand has the limitations that the syndesmotic complex can only be evaluated on oblique views, the IOL is not always clearly visible, and the intra- and interrater reliability has been reported to be moderate to good.2,19,23,30 Still, MRI must still be considered the noninvasive standard of reference. It would have been favorable to correlate the MRI findings with those of the arthroscopy. Second, there is an ongoing discussion on whether MRI imaging should be read by 2 independent reviewers or in consensus. Because of the known limited interrater reliability, the authors decided to perform consensus reading, as done in various recent studies.1,31,34 Third, for the SDL, only 3 ligaments, that is, the TNL, TSL, and TCL were analyzed. The superficial tibiotalar ligament was not rated, as its differentiation to the DDL is not always possible. Finally, the diagnostic algorithm facilitated herein, although evidence-based, 29 might be a selection bias. The bilateral external rotation stress test under fluoroscopy could also be positive in higher degrees of DL injuries. Consequently, it can be hypothesized that patients with an isolated AiTFL injury and higher-degree DL injury have been included in the current analysis.
During the revision process of the article, the applied, advanced statistical analysis was a major point of concern. Presenting data as a heatmap and performing a cluster analysis is far from standard in orthopaedic research, but it was chosen to ensure a comprehensive understanding of our data. Hierarchical clustering allowed to discern underlying patterns within the dataset, whereas silhouette length and robust permutation tests ensured the reliability and generalizability of our findings, even in the face of potential data variability.
Despite these limitations, the present study has several strengths. First, the diagnostic algorithm at our specialized foot and ankle unit is standardized and was the same for all patients. Second, MRI reading was conducted by 2 specialized radiologists. Third, it is the first study to focus on the association between syndesmotic and DL injuries in a larger cohort.
Conclusion
Unstable syndesmotic injuries can occur isolated or with an accompanying DL injury. There appears to be a great heterogeneity between the severity of syndesmotic and deltoid ligament injuries.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241274712 – Supplemental material for Syndesmotic and Deltoid Injuries: Companions or Coincidences
Supplemental material, sj-pdf-1-fai-10.1177_10711007241274712 for Syndesmotic and Deltoid Injuries: Companions or Coincidences by Federico Paolo Gaube, Felix Maßen, Hans Polzer, Wolfgang Böcker, Paul Reidler, Maximilian Michael Saller, Sebastian Felix Baumbach and Nina Hesse in Foot & Ankle International
Supplemental Material
sj-pdf-2-fai-10.1177_10711007241274712 – Supplemental material for Syndesmotic and Deltoid Injuries: Companions or Coincidences
Supplemental material, sj-pdf-2-fai-10.1177_10711007241274712 for Syndesmotic and Deltoid Injuries: Companions or Coincidences by Federico Paolo Gaube, Felix Maßen, Hans Polzer, Wolfgang Böcker, Paul Reidler, Maximilian Michael Saller, Sebastian Felix Baumbach and Nina Hesse in Foot & Ankle International
Footnotes
Acknowledgements
We acknowledge the technical support of Core Facility Statistical Consulting at Helmholtz Munich, Munich, Germany. We thank Dr. Kainat Khowaja and Ronan Le Gleut for help with the advanced cluster analysis.
Ethical Approval
Ethical approval for this study was obtained from the ethics committee of the medical faculty, Ludwig-Maximilians-Universität, Munich (23-0493).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hans Polzer, MD, reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Arthrex GmbH. Sebastian F. Baumbach, MD, reports collaborative research, paid lectures, and support for attending meetings and/or travel from Arthrex. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.