
Abstract
Introduction
Ingrown nails are a common debilitating and painful disease caused by the nail plate penetrating the lateral nail fold leading to inflammation and infection. The pain associated with ingrown nails damages quality of life, making it difficult for the patient to wear closed shoes, inhibits walking, and is aesthetically unpleasing. Many treatment options are available, including conservative treatments such as cotton insertion, Gutter treatment, elastic tape, and external devices,1,2 as well as operative treatments5,8 such as wedge resection, phenolization, 6 terminal Symes amputation, 8 and wire techniques3,7 (Sogawa/Machida wire correction). These methods carry the potential disadvantage of leading to cosmetic deformities and have a recurrence rate of 6.2% to 37%.4,5 Here we present a new operative procedure that allows for complete removal of the nailbed without shortening the toe and completely curing the ingrown nail with minimal cosmetic damage.
Technique
Indications
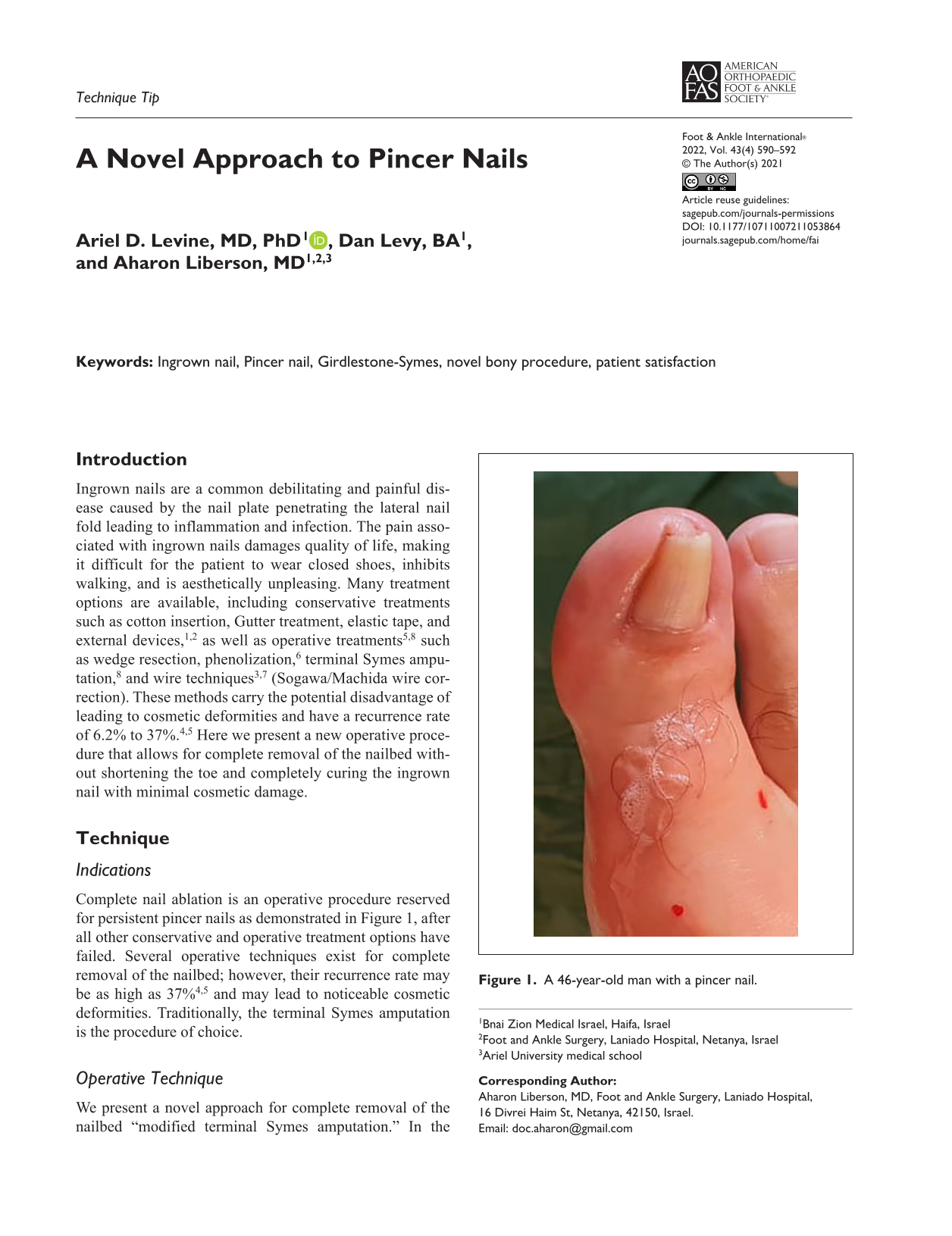
Complete nail ablation is an operative procedure reserved for persistent pincer nails as demonstrated in Figure 1, after all other conservative and operative treatment options have failed. Several operative techniques exist for complete removal of the nailbed; however, their recurrence rate may be as high as 37%4,5 and may lead to noticeable cosmetic deformities. Traditionally, the terminal Symes amputation is the procedure of choice.

A 46-year-old man with a pincer nail.
Operative Technique
We present a novel approach for complete removal of the nailbed “modified terminal Symes amputation.” In the classical terminal Symes amputation, a deep incision directly through the soft tissues to the level of the distal phalanx is made around the entire nail and nail matrix. This allows for complete removal of entire nail (including bed and matrix), all nail folds (medial lateral and proximal). However, closing such an incision requires removal of the distal part of the phalanx, leading to shortening of the toe and cosmetic deformity. Our modification is to shave off the dorsal part of the phalanx within the incision margin (Figure 2); this allows for mediolateral closure of the operative wound rather than proximodistal as shown in Figure 3. The operative wound is closed with 0/4 nylon sutures, over a drain made from a gastric feeding tube. The wound is dressed in Inadine and gauze pads.
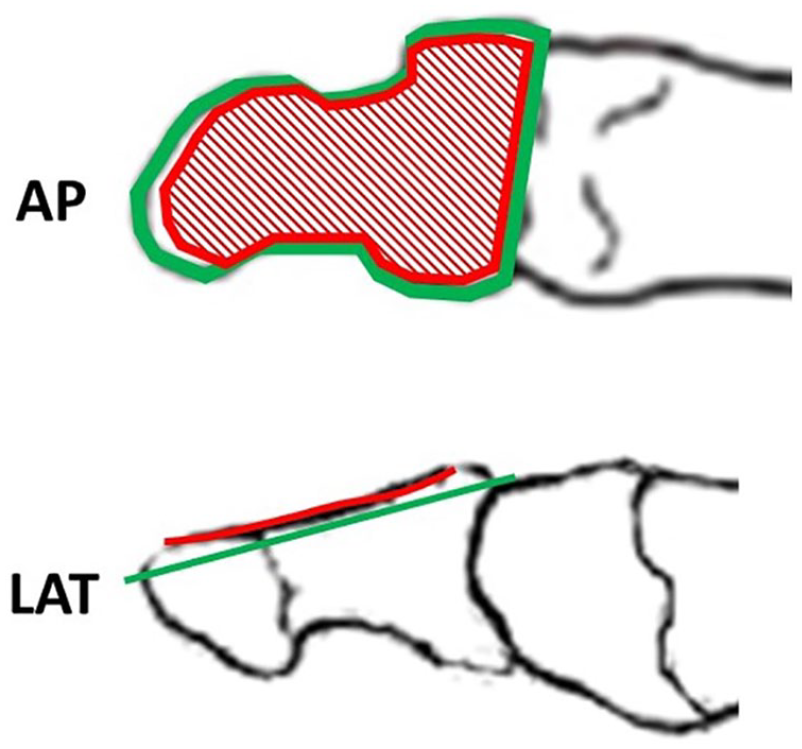
AP: an anterior-posterior representation of the distal phalanx of the big toe. LAT: a lateral representation of the distal phalanx of the big toe. In both cases, the red area represents the nail bed and the green area our operative cut. Such bone resection preserves phalanx length and accomplishes complete nail ablation [See online article for color figure.].
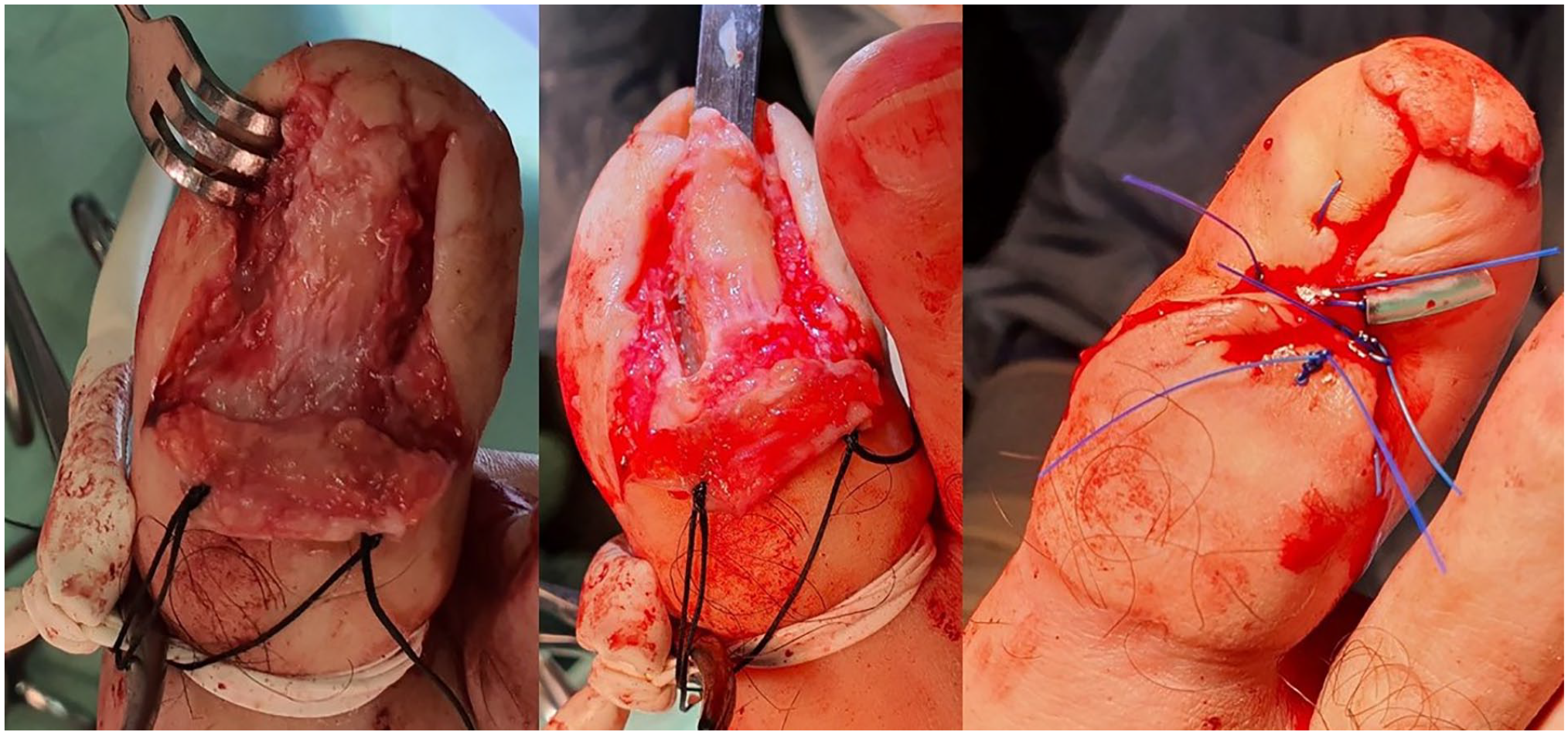
Left: Distal phalanx following nail removal. Middle: Distal phalanx during modified terminal Symes amputation. Right: Big toe after suture (with drain).
Postoperative Follow-up
Patients were discharged the following day without any weightbearing restrictions and were examined during outpatient follow-up 10-14 days later, at which time the sutures were removed. To date, we have seen only 1 postoperative complication, which was an operative site infection with positive MSSA culture from the operative wound. The patient was admitted to our department for a short course of intravenous antibiotics followed by 3 weeks of oral antibiotics on an outpatient basis. At the 1-year follow-up, all patients demonstrate good healing of the operative site without recurrence of the ingrown nail or shortening of the great toe as shown in Figure 4.

A sample of our results over a year postsurgery.
Discussion
Many treatment options for ingrown toenail are available. Although most complete nail and nailbed removal procedures demonstrate good results, these treatments are last resorts and carry with them the risk of recurrence and cosmetic deformities. Here we presented a novel approach to complete nail and nailbed removal that should allow for a lower recurrence rate, minimal cosmetic deformity, and a low postoperative complication rate. We achieved this by shaving the dorsal part of the distal phalanx, removing only the nailbed without shortening the phalanx; thus, we preserve the length of the toe. Thus far we have performed our operative method on 10 patients between 30 and 80 years old, suffering from persistent pincer nails, who had failed both conservative and operative treatments. All patients demonstrated good operative site healing without recurrence of the ingrown nail or major cosmetic deformities. With such results, we believe that widespread application of our technique will lead to better operative results with greater patient satisfaction.
Footnotes
Author Note
The article was written as part of the requirements of the School of Medicine in the Galilee, Bar-Ilan University, Israel, for Dan Lavi’s M.D. degree.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.