
Abstract
Background:
Capsular shrinkage is an arthroscopic stabilization technique that can be used in patients with chronic ankle instability (CAI), if desired in addition to primary arthroscopic procedures. Despite positive short-term results, long-term follow-up of these patients has not yet been performed. Therefore, our objective was to assess whether capsular shrinkage still provided functional outcome after 12-14 years compared to preoperative scores.
Methods:
This study was a retrospective long-term follow-up of a prospectively conducted longitudinal multicenter trial. The study duration was from February 2002 to September 2016, including a preoperative assessment and short-, mid-, and long-term follow-up. At the time of inclusion, patients were diagnosed with CAI, >18 years old, were unresponsive to conservative treatment, and had confirmed mechanical ankle joint laxity. Patients were excluded if the talar tilt was greater than 15 degrees, if they had received previous operative treatment, or had constitutional hyperlaxity, systemic diseases, or osteoarthritis grade II or III. The primary outcome was the change in functional outcome as assessed by the Karlsson score.
Results:
Twenty-five patients of the initial 39 were available for this follow-up. This group had a mean age of 43.2 years (SD±11.1) and included 15 males. A statistically significant improvement was found in the Karlsson score at 12-14 years (76.6 points; SD±25.5) relative to the preoperative status (56.4 points; SD ±13.3; P < .0005). Although 17 patients (68%) reported recurrent sprains, 23 patients (92%) stated that they were satisfied with the procedure.
Conclusions:
Despite improved functional outcome and good satisfaction in patients with CAI after capsular shrinkage, recurrence rates and residual symptoms were high. For this reason, arthroscopic capsular shrinkage is not recommended as joint stabilization procedure in patients with CAI.
Level of Evidence:
Level IV, case series
Introduction
Lateral ankle sprain is the most prevalent musculoskeletal injury. In the long term, 30% to 40% of patients develop chronic ankle instability (CAI).12,31 In the acute situation, an inversion injury is treated conservatively. Acute surgical stabilization is mainly reserved for professional athletes. With inadequate recovery after conservative therapy and the development of chronic instability, patients may become eligible for surgical stabilization. Multiple techniques can be used. 10
Four general techniques have been described: anatomic repair, anatomic reconstruction, nonanatomic reconstruction, and thermally induced capsular shrinkage. In case of anatomic repair, the original ligaments are preserved and reattached to their origin using sutures and/or bone anchors. This procedure is currently very popular as it can be performed as an arthroscopic procedure whereas the other 2 techniques are primarily performed as an open procedure. 4 Anatomic reconstruction, which can also be performed as an arthroscopic procedure,23-25 uses tendons to restore the stability. Both anatomic repair and reconstruction aim to restore the joint anatomy and to normalize the joint biomechanics. 2 Nonanatomic reconstruction is a third option in surgical joint stabilization and is mainly used as a salvage technique. Often, the peroneal tendons are used to stabilize the ankle joint. As normal anatomy changes, so do joint mechanics. Additionally, nonanatomic reconstruction is associated with higher complication rates. For this reason, it is mainly used as a last resort.3,10
Capsular shrinkage uses heat to induce shrinkage of the joint capsule.8,21 Tightening the capsule aims to reduce laxity and with that reduce ankle instability. A previous study, however, has shown that mechanical joint stability did not improve, but patient-reported outcome measures (PROMs) did show symptom resolution in most patients in the short term. 8 Capsular shrinkage is a minimally invasive technique without the use of implants, like anchors and screws. Long-term outcome after capsular shrinkage, however, has not been reported. Therefore, it is unknown whether patients still experience relief of symptoms in the long term. The objective of this study was to assess the patient-reported outcome at long term follow-up to determine whether patients still experience less symptoms compared to their preoperative assessment. We hypothesized that capsular shrinkage was an effective procedure for patients with CAI showing significantly higher patient-reported outcome 12 to 14 years after surgery compared to the initial preoperative assessment.
Methods
This study was a retrospective long-term follow-up based on a prospectively performed longitudinal multicenter trial. A total of 8 centers participated. The surgical procedure was performed by 1 surgeon per center with extensive experience in ankle arthroscopy. The initial study was approved by the Medical Ethical Review Board of all centers and informed consent was provided by all participating patients. The study period was from February 2002 until September 2016. This study included a preoperative assessment, short-term follow-up (9 months), and midterm follow-up (5-7 years). The present study comprised the long-term (12-14 years) follow-up.
In total, 25 patients of the initial 39 were included in this last follow-up. The total initial population consisted of 19 males (48%) and 20 females. Of these, 12 males (48%) and 13 females filled out the long-term follow-up questionnaire (Figure 1). The mean age of the initial population was 43.2 years (SD ±11.1), and the mean age of the long-term follow-up population was 43.4 years (SD ±12.9) (Table 1).
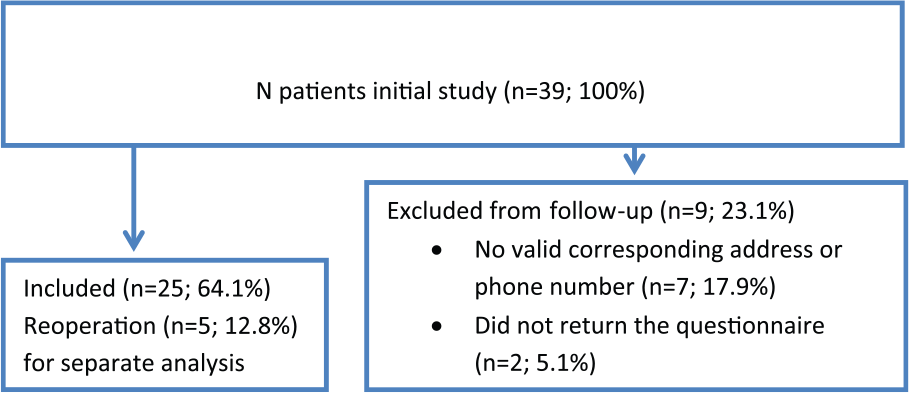
Flow-chart of inclusion.
Abbreviations: FU, mean follow-up; n, number of patients; PROM, patient-reported outcome measure; AOFAS, American Orthopaedic Foot & Ankle Society.
Mean scores and standard deviations and P value for pre- and postoperative outcome measures.
FU in months.
All patients were diagnosed with CAI and were recruited from an outpatient clinic. CAI was defined as recurrent sprains or giving way for more than 6 months after an acute ankle sprain without adequate response to conservative treatment. 18 Furthermore, patients had to be aged 18 years or older, be able to provide informed consent and had increased mechanical laxity. Increased mechanical laxity was defined as a positive anterior talar translation or talar tilt on stress radiographs using the Telos-stress apparatus (150 N), with anterior talar translation ≥4 mm or a difference from the ipsilateral side ≥3 mm and a talar tilt ≥10 and ≤15 degrees or a difference with the ipsilateral side ≥6 degrees. 6 Talar tilt >15 degrees was an exclusion criterion because this indicates that more than just the lateral ligament complex was affected. 8 Additional exclusion criteria were previous operative therapy for CAI, constitutional hyperlaxity, systemic diseases affecting the locomotor system, osteoarthritis grade II or III, or secondary stabilization after failed capsular shrinkage. 28
Surgical procedure
The surgical procedure was performed as a standardized outpatient procedure. The procedure was captured on video and shared with the other participating centers to ensure unity in performance. Standard anteromedial and lateral portals were made. A 4.0-mm arthroscope was introduced through the medial portal and the instruments were introduced through the lateral portal. Additional pathology such as osteophytes, synovitis and loose bodies were treated first. Subsequently intraoperative testing of stability was performed using both the anterior drawer test and the talar tilt test.
Shrinkage was induced using an arthroscopic probe with a 3.5-mm side effect tip that applied the radiofrequency energy. The initial energy level was 20 W, but this could be adjusted to a maximum of 50 W. In all patients, shrinkage of the anterior talofibular ligament and adjacent joint capsule was performed.
Postoperatively, patients received a compression bandage for 3-5 days. During this period of time, patients were advised to avoid weight-bearing. After 5 days, an inelastic tape bandage was applied and patients were allowed to mobilize and bear weight on the operated ankle as tolerated. Every 2 weeks over a 6-week period, the tape was replaced. During this period, patients were allowed to resume work as tolerated but were still restricted from participating in activities with a high risk of spraining the ankle. During the last 6 weeks of the 13-week rehabilitation period, patients were allowed to resume sports as tolerated.
Outcome Measures
The primary outcome measure of this long-term follow-up was the change in functional outcome over time comparing preoperative and short-, mid-, and long-term patient-reported outcome measures according to the Karlsson score. 19 The Karlsson score is a score ranging from 0 to 100 points scoring on pain, swelling, instability, stiffness, stair climbing, running, work activities, and required ankle support.
As secondary outcome measures, the SF-36, 1 the Tegner activity score 27 and the score by Good et al. 11 were analyzed. The SF-36 is a questionnaire assessing general quality of life. It consists of a physical and mental component scale. The Tegner scale aims to score activity level from 0 (no activities possible because of ankle complaints) to 10 (performing competitive sports). Finally, the patient was asked to scale themselves according to Good et al. regarding their ankle complaints from grade 1 (Full activity, including strenuous sport; No pain, swelling or giving way) to grade 4 (Recurrent instability and giving way in normal activities, with episodes of pain and swelling). Additional secondary outcome measures were pain, subjective swelling, instability, locking, joint stiffness, difficulty ascending stairs, running, work, and sporting activities using a self-assessment questionnaire. Finally, the scale by Good et al. was used to assess whether there was a correlation between the functional outcome score and reoperation rate.
Statistical analysis
All data were analyzed using SPSS 23.0 (IBM Corp, Armonk, NY). All outcome measures were assessed for normality using the Shapiro-Wilk test in combination with estimation. To evaluate improvement in functional outcome, each patient was assessed individually building a longitudinal database, minimizing missing data. This way individual questionnaire scores were analyzed and compared per time interval using repeated measures analysis of variance (ANOVA) with the Bonferroni correction. Means and standard deviations were provided for all questionnaire scores, and in case of skewed data the median and range were used. The improvement or worsening of complaints was reported as yes/no for experiencing these complaints and assessed using the McNemar test comparing pre- and postoperative reports. The Pearson correlation coefficient was used to assess the correlation between functional outcome score and preoperative severity and the Spearman rho for the correlation between reoperations and preoperative severity. A P value of <.05 was considered statistically significant.
Results
Of the current cohort of 25 patients, 14 patients (56%) reported re-spraining their ankle at least once a year with a maximum of 2 times per month. Of all 25 patients, 92% reported good to excellent treatment satisfaction and 8% low to moderate satisfaction. Seventy-two percent would undergo the surgery again if they had to make that same choice. Five patients (13%) of the original cohort, who responded to the call for follow-up assessment, received a reoperation as capsular shrinkage provided insufficient joint stabilization and were excluded from the initial analysis. For the other 9 patients who reported recurrent sprains, it is unknown whether they had a revision stabilization.
ANOVA showed a score improvement for all functional scores used (P = .000-.002). Using the post hoc Bonferroni score, improvements for all PROMs were found, but only the Karlsson (from 56.4 [SD±13.3] to 76.6 [SD±25.5]; P < .0005), Tegner (from 3.0 [SD±2.1] to 4.9 [SD±2.1]; P = .004), and Good score (from 3.9 [SD±0.3] to 2 [SD±1.1]; P < .0005) showed significant improvement comparing the last follow-up to the preoperative assessment (Figures 2 and 3). The Karlsson score showed significant improvement over the full time span and additionally showed that there was no score change comparing the mid- and long-term follow-up (P = 1.000). The SF-36 physical scale score only showed significant improvement at the first (short-term) follow-up. The SF-36 mental scale showed no score change. The Tegner score showed significant improvement over time for both the short- and long-term follow-up. Finally the Good score assessing the severity of the ankle complaints showed improvement as well at each follow-up moment and also showed no change after the midterm follow-up (Figures 2 and 3).
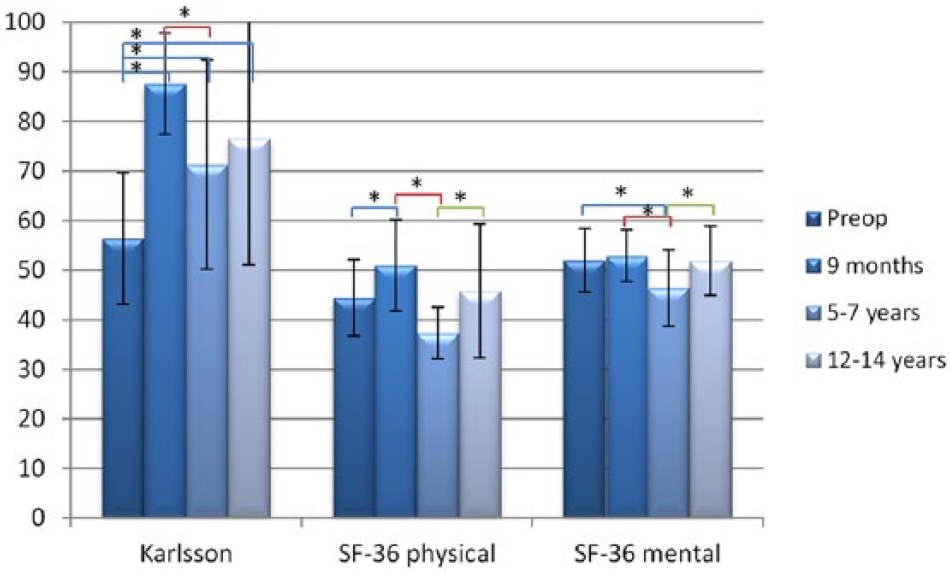
Functional outcome scores (n = 25) and standard deviation of the Karlsson and SF-36 subscores. *Analysis of variance: P < .05.
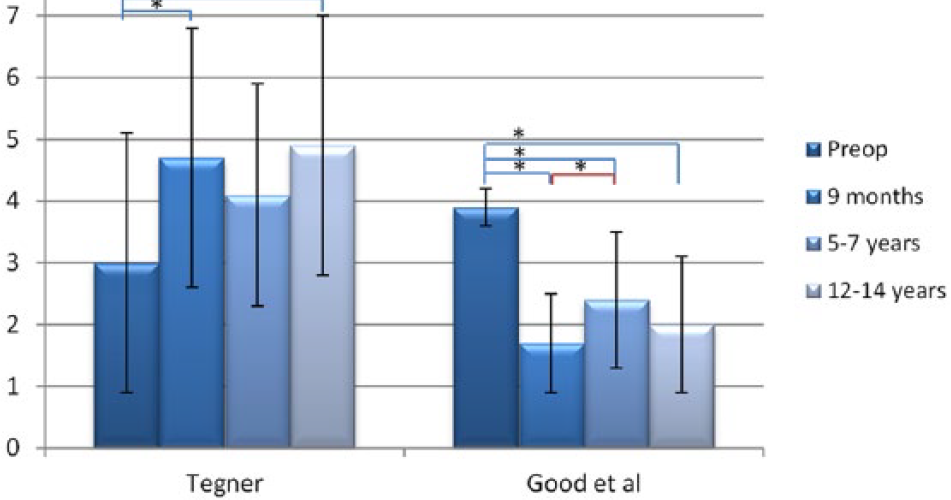
Mean outcome scores (n = 25) and standard deviations of the Tegner and Good scores. *Analysis of variance: P < .05 score difference between follow-up moments.
All patients reported 1 or more complaints (pain, swelling, instability, or locking) before surgery, and 15 patients (56%) reported 1 or more of these complaints at final follow-up. Comparing the preoperative reports with the final follow-up showed a significant decrease over time for pain, instability, ascending the stairs, running and work (P = .000-.006). The preoperative Good score was not correlated with any of the functional outcome scores or the reinterventions.
Discussion
Capsular shrinkage seems to be a relatively effective treatment with regard to outcome scores for patients with CAI confirming our hypothesis. Patients still show improvement after 12 to 14 years in functional outcome compared with the preoperative PROM scores. Even though improvement was shown, a little more than half of the patients postoperatively still had 1 or more complaints such as pain, swelling, locking, stiffness, difficulty ascending stairs or running. Additionally 68% experienced recurrent sprains. Five patients even had a revision surgery. The preoperative severity of the ankle instability as measured by the Good scale, however, was not correlated to treatment outcome on the long term. Between the short- and midterm follow-up, the Karlsson and SF-36 scores decreased, possibly indicating a diminishing effect of the shrinkage procedure over time. Whether recurrence rates, persistent complaints, and a diminishing effectiveness over time are more or similar compared with other arthroscopic stabilization techniques is unknown as these outcomes seem to be underreported. 30 In contrast to the initial PROM score, decrease between short- and midterm follow-up is followed by a subsequent score improvement from mid- to long-term follow-up. This may be due to habituation to the complaints or adjustment of expectations and activities (Figures 2 and 3).
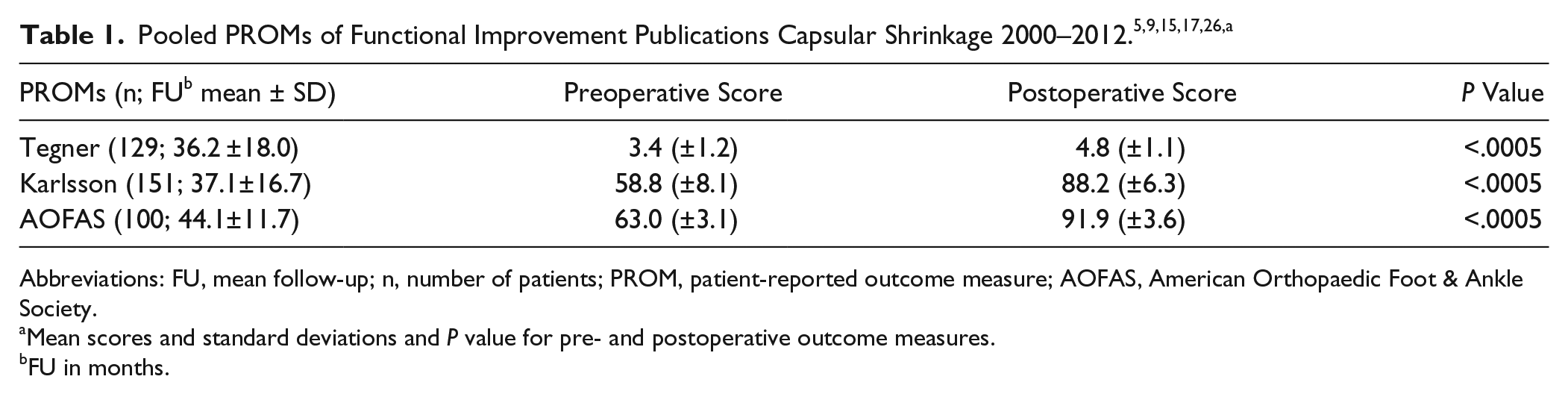
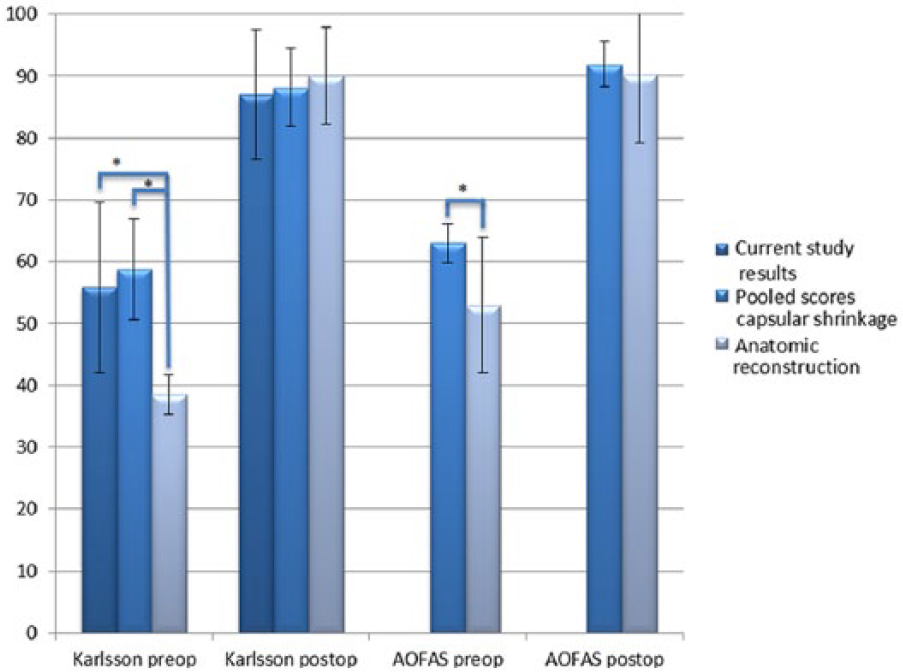
In the literature, we identified 5 studies reporting on outcomes after capsular shrinkage therapy for CAI.8,16,22,26,29 These studies include 165 patients with a mean of 33 patients per study, a mean age of 33 (SD ±9) years, and a mean follow-up period of 35 (SD ±17) months. Functional outcome was assessed using the Tegner score (in 2 studies), the Karlsson score (3 studies), the Good score (1 study), the SF-36 (1 study) and the AOFAS (2 studies), the short-AOFAS (1 study), all showing postoperative improvement compared to the preoperative assessment (Table 1, Figure 4). Complications reported by these studies included altered sensation (3%), reoperation (2%), ROM restriction (2%), tape allergy (1%), persistent postoperative pain (0.6%), and persistent instability (0.3%). Long-term follow-up results have not yet been reported.
Despite good short-term results, long-term results raise some doubt whether arthroscopic capsular shrinkage is an adequate technique to treat patients with CAI. It does not decrease mechanical ligament laxity, 8 and the number of reported recurrent ankle sprains is high. Capsular shrinkage is a technique that was introduced about 15 years ago to resolve complaints of ankle instability. Other techniques that were performed at that time were tenodesis and anatomic reconstruction, of which long-term results are reported7,20 (Table 2). Comparing the outcomes of the current capsular shrinkage studies to the long-term outcomes of tenodesis and anatomic reconstruction, as published by Krips et al 20 and de Vries et al, 7 minimal differences are observed between the techniques (Table 2). For the Karlsson score, the score of Good et al, the severity of postoperative arthrosis, subjective joint stiffness, and the number of reoperations, better outcomes were achieved by anatomic reconstruction compared with both tenodesis reconstruction and capsular shrinkage. Considering satisfaction, ROM restriction, reoperations (capsular shrinkage vs tenodesis), and subjective instability, all techniques seem to score equally. For postoperative pain and swelling, capsular shrinkage seems to score best and for postoperative work and sport restriction worst. Recurrent sprains were only assessed by this study. The reported high satisfaction may have resulted from addressing the additional pathology encountered during surgery, particularly as it is not in line with the other outcomes such as recurrent sprains and postoperative work and sports restrictions. Prior to the present report, all studies that reported the results of capsular shrinkage for treating CAI concluded that it is a suitable arthroscopic treatment for moderate chronic ankle joint laxity, even in patients with complete ATFL lesions.8,16,22,26,29
Long-Term Results After Capsular Shrinkage, Tenodesis, and Anatomic Reconstruction. a
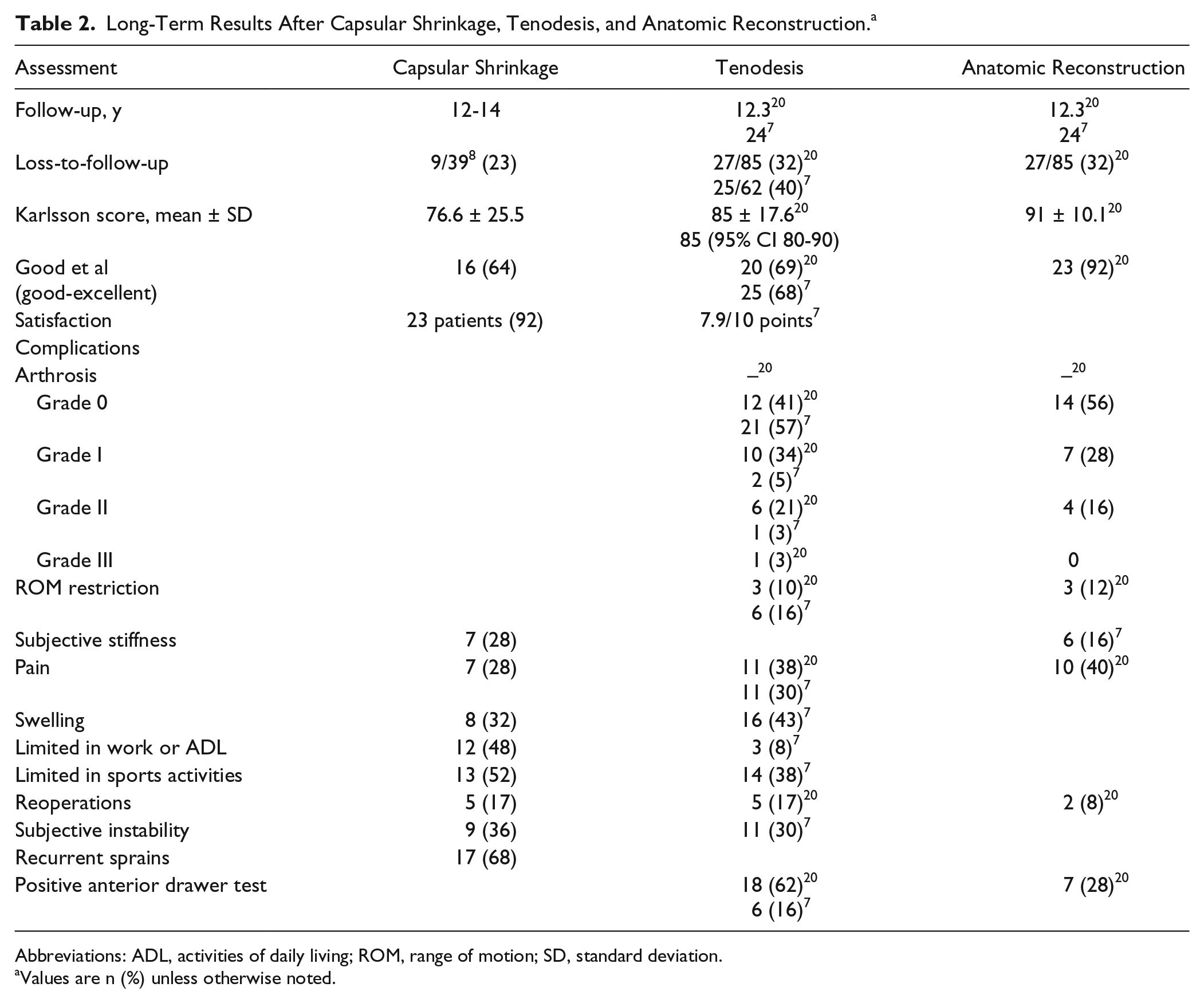
Abbreviations: ADL, activities of daily living; ROM, range of motion; SD, standard deviation.
Values are n (%) unless otherwise noted.
A total of 13% of the original cohort (n = 5) required reoperation. This raises the question whether these patients should not have been directly treated using anatomic reconstruction, instead of capsular shrinkage. For this reason, an additional analysis was performed comparing the results of this study and the pooled capsular shrinkage results with primary anatomic reconstruction in patients that are consistent with our inclusion criteria (Figure 4).5,9,15,17 Comparing capsular shrinkage with anatomic reconstruction showed an overall lower preoperative Karlsson and AOFAS score for patients who received primary anatomic reconstruction, whereas the postoperative scores were equal to both capsular shrinkage cohorts. Overall, anatomic reconstruction seems to be used in patients with more severe complaints, leading to equivalent results postoperatively as in patients with less severe complaints undergoing capsular shrinkage. This might indicate better results are achieved by anatomic reconstruction compared with capsular shrinkage. However, based on our results, the severity of ankle instability does not seem to be associated with a better or worse outcome after capsular shrinkage or with reoperation. Therefore, this study cannot support the hypothesis that capsular shrinkage is mainly suited for the less severe cases of ankle instability.16,22,26,29
Capsular shrinkage does not decrease laxity of the ankle ligaments as tested by the anterior drawer test or the talar tilt test. 8 This might be the reason this procedure is thought to be less fit for patients with severe joint laxity. 13 Self-reported instability was assessed by the scale of Good et al 11 scoring ankle function over 4 degrees of severity, ranging from full activity to recurrent ankle instability. As this scale only contains 4 degrees of severity and grade 3 does not include spraining the ankle, patients almost always scored themselves a 4 in case of instability—possibly making this scale not specific enough to assess the degree of subjective instability.
The main limitation of this study is the number of patients. Only 25 of the initial 39 responded to the call for follow-up or fit the inclusion criteria. No conclusions can be drawn concerning the preoperative severity of complaints and reoperations as there were only 5 reported reoperations and a total of 39 patients, resulting in a lack of power. Additionally, the Good score only has 4 grades of severity and therefore is biased by a floor and ceiling effect. The use of another outcome measure, like the Cumberland ankle instability tool, scoring severity of complaints as well, might provide more details on severity of ankle instability and therefore provide a more reliable answer on possible correlations. 14
In conclusion, despite the improved functional outcome and good overall satisfaction reported by the patients in the short and long term, arthroscopically applied capsular shrinkage is a minimally invasive technique that is technically not effective in the long term, with high rates of recurrence and revisions and persisting complaints. Based on current results, this technique is not recommended as a stabilization technique for patients with CAI. Anatomic reconstruction may be preferred as it provides superior results in the long term and is currently also performed arthroscopically.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Editor’s Note
The authors are to be commended for reporting longer-term follow-up on this interesting patient population. I would certainly agree with their conclusion that thermal capsular shrinkage should not be used for chronic ankle instability. Although the technique was met with great enthusiasm when it was introduced for shoulder instability, the long-term outcomes there also were poor. It was no real surprise when such a nonbiologic method, that is, heating tissue beyond the point of cell viability, resulted in eventual stretching of the tissues that had undergone thermal shrinkage.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.