
Abstract
Ankle instability is an old topic with increasing importance in Orthopaedics’ world, as we start now realising how underdiagnosed this pathology has been. A lot of effort has been made in recent years to better understand the pathomechanics of this injury, with new surgical techniques being tried and even new anatomic structures being described. The objective of this paper is to review and compile the most important and recent literature on this matter, in an academic way, but oriented to clinical practice, so it can help surgeons keep updated in this so important subject.
Introduction
Ankle instability is an old topic with increasing importance in Orthopaedics’ world, as we start now realising how underdiagnosed this pathology has been. A lot of effort has been made in recent years to better understand the pathomechanics of this injury, with new surgical techniques being tried and even new anatomic structures being described.
The objective of this paper is to review and compile the most important and recent literature on this matter, in an academic way, but oriented to clinical practice, so it can help surgeons keep updated in this so important subject.
Epidemiology
Ankle sprains account for 10–30% of all sports injuries. Its incidence peak locates between 15 and 19 years old representing 50% of all lower limb lesions in high school athletes. Inversion-type is by far the most common mechanism of injury happening in 80–90% of cases. Compared with men, women have a slightly higher overall incidence of ankle injuries in similar sports activities. Men, however, have a higher incidence of medial ankle and syndesmotic sprains. Greater mean height and weight, increased body mass index, and certain athletic activities (e.g. basketball, football, rugby) may be risk factors for ankle sprains as well.1,2
Anatomy and mechanism of injury
Bony anatomy
Several bony structures of the ankle are of the utmost importance contributing up to 30% of ankle resistance to rotation. 3 The morphology of the talus, being broader anterior than posterior increases joint stability at neutral position and predisposes for supination-inversion sprains. Posterior position of the fibula and hindfoot malalignment also have been shown to predisposes to ankle instability, 4 and the length of the medial malleoli has been shown to relate with the number and the severity of ankle sprains. 5
Soft-tissue anatomy
The deltoid ligament complex is composed of a superficial layer, a deep layer and the spring (calcaneonavicular) ligament. The spring ligament is often included with the deltoid ligament complex because it assists in stabilising the medial ankle structures of the ankle joint through its connection to the deltoid by the tibiospring ligament.
Laterally, the ligament complex is composed by the anterior talofibular ligament (ATFL) superior and inferior fascicule, the calcanealfibular ligament (CFL) and posterior talofibular ligament (PTFL). The inferior ATFL fascicle and the CFL share the same fibular insertion 6 and are connected by the arciform fibres representing a single functional structure that acts as a ligamentous complex. Thus, the lateral fibulotalocalcaneal ligament complex is a more accurate terminology for this structure. In addition, ATFL's superior fascicle is an intra-articular structure while ATFL's inferior fascicle is extra-articular. 7
Regarding the subtalar joint, increasing interest has been given to the cervical ligament as many authors purpose it can be a source of both pain and instability symptoms.
Mechanism of injury
An inversion ankle sprain is the most frequent cause of acute ankle injury in sports. 8 This typically occurs after a jump, when landing on the lateral border of the foot, but might also occur if the foot gets locked on the ground, while the body continues to turn. This sudden increase in inversion and internal rotation forces, combined with either dorsi- or plantarflexion, produces sufficient strains to rupture the ankle lateral ligaments, causes concomitant osteochondral lesions or aggravates anterior or posterior joint impingement. The ATFL ruptures first and usually is the only ligament injured. 8 This is due to the fact that the ATFL is the weakest component of the lateral collateral ligament complex of the ankle, in particular its superior fascicle.9,10 With higher deforming forces, the injury continues to propagate rupturing the inferior ATFL fascicle and the CFL.1,2 Finally, continuous energy will rupture the PTFL causing the ankle to dislocate laterally. In about 65–80% of cases, an isolated lesion of the ATFL will occur, while combined ruptures of the ATFL and CFL happen in around 20%.8,9 The PTFL is rarely injured during inversion sprain.10,11 In ∼10–15% of all inversion injuries, there is a total rupture of the lateral ankle ligaments. 7
Patients with medial ankle instability may give a history of a pronation-type injury, but more often report having had multiple ankle sprains without clearly remembering the mechanism. Deltoid injuries occur commonly in relation to fractures such as Wb C/pronation external rotation or pronation abduction and less frequently with Wb B/supination external rotation ankle fractures.
Ankle instability
Functional instability
A history of insecurity, a feeling of instability, and giving way is far more common in the diagnosis than demonstrable instability on physical examination or stress radiographs. The presence of damaged proprioception nerve receptors located in the ligaments and skin is responsible for this clinical presentation. Delay in muscle reactivity, namely by the peroneal muscles, can also contribute to this type of instability.12,13
Mechanical instability
Mechanical instability is characterised by true insufficiency of the ligamentous stabilisers with objective evidence of ligamentous laxity on the physical exam. Specific tests can be done in order to better understand which structures might be compromised. Those tests will be described later in this text.
Rotatory ankle instability (RAI) is a category that combines lateral and medial instability. Under weight-bearing conditions, ATFL-deficient ankles demonstrate increased anterior translation, internal rotation and superior translation of the talus. 6 These biomechanical changes are associated with the development of degenerative arthritis. CAI may also cause concomitant ankle injuries, leading to a deltoid ligament tear. RAI should be considered when an injury is present in the anterior fibres of the deltoid ligament. It is estimated that 10–40% of all patients affected by CAI have a partial deltoid injury.9,10
Microinstability is an emerging concept within mechanical ankle instability, and the currently proposed pathomechanism is a partial tear of the ATFL affecting only the superior fascicle of the ligament. 11 As recently reported, ATFL's superior fascicle is an intra-articular structure. 7 Because of this anatomic characteristic, proper healing of ATFL's superior fascicle is limited as intra-articular ligaments do not heal by themselves. At an increased risk of ankle sprain recurrence, these patients can go on to develop chronic ankle instability (CAI) or classical ankle instability caused by ligament tear propagation affecting the ATFL's inferior fascicle and calcaneofibular ligament. Therefore, ankle microinstability should be considered as initial and developing ankle instability. 14
Diagnose
The history should address the mechanism of the most recent injury, the ability to bear weight, the frequency of instability episodes and ankle sprains, and previous treatments. The physical examination includes an evaluation of gait and standing alignment, during which the examiner looks for varus hindfoot alignment, which leads to lateral foot overload and can result in ankle instability, peroneal tendon injury and fifth metatarsal stress fracture. Special tests are used to diagnose this pathology include the inversion and eversion test, external rotation test, anterior drawer test and Squeeze test.
Frey et al. 15 found that physical examination was 100% accurate in the diagnosis of grade III ligament injuries but only 25% accurate in the diagnosis of grade II injuries compared with magnetic resonance imaging (MRI) findings. Clinicians most often underestimate the damage with a grade II ligament tear. van Dijk et al. 16 suggested that a more accurate diagnosis is possible if a physical examination is performed 5 days later rather less than 48 h from the injury.
X-ray
Standard plain radiographs should include standing anteroposterior, lateral and mortise views and a comparative Saltzmann view can be useful as well. Dynamic stress X-rays only have diagnostic value if they are positive, with specificity (up to 100%) but low sensitivity (57%).17,18
Magnetic resonance imaging
More powerful and three-dimensional MRI studies have allowed for greater accuracy in the diagnosis of ankle and hindfoot injuries. 19 Axial MRI with a local gradient provides optimal views of the ATFL and PTFL, the deep layers of the medial collateral ligament, and the tibionavicular ligament, whereas MRI coronal imaging allows a complete view of the calcaneofibular, posterior talofibular, tibiocalcaneal and posterior tibiotalar ligaments. In both imaging planes, differentiation of the deep and superficial layers of the medial collateral ligament, as well as between the syndesmotic complex and the lateral collateral ligaments, was possible. MRI has been shown to be effective by several authors in identifying and differentiating lateral ankle ligament injuries; however, many believe that the costs outweigh the benefits. If a peroneal pathologic process is suspected, MRI may be beneficial, but it should not be used routinely to diagnose lateral ligament injury. 2
Ultrasonography
Ultrasonography (US) plays a significant role in evaluating the ankle ligaments. The ligaments are hyperechoic when oriented parallel to the US beam. US is more useful in acute ligamentous injuries, with an accuracy of up to 93.8% sensitivity and a 100% specificity in detecting ATFL tears when compared with MRI. In addition, dynamic US can be performed, assessing for ankle ligament stability and bony impingement in real time using joint stress manoeuvres. However, a skilled and experienced operator is necessary to obtain such results.20,21
Arthroscopy
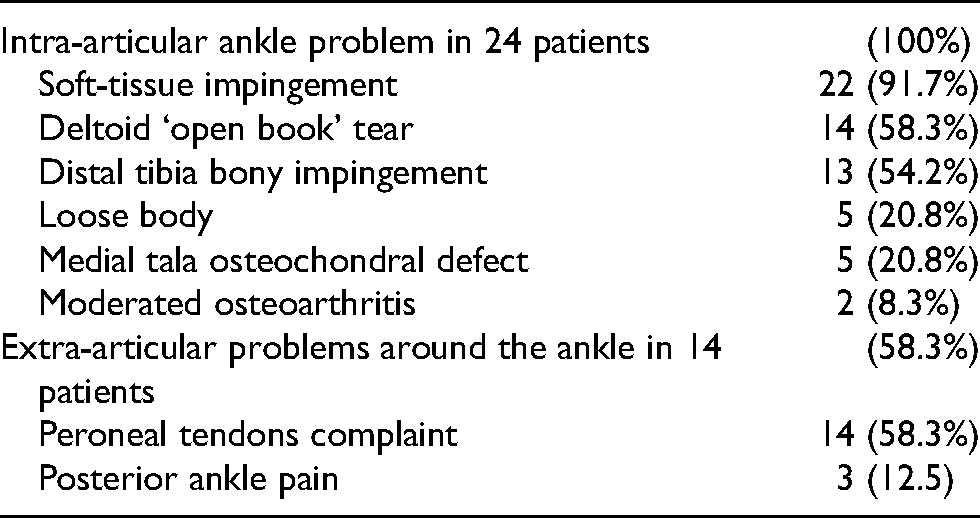
There are several studies highlighting the importance of arthroscopy in the diagnose and treatment of ankle instability due to the amount of concomitant injuries that is possible to find inside the joint that would pass undiagnosed otherwise. Classic studies like Hintermann et al. 9 that was able to find cartilage injury in 66% of patients with lateral ankle instability and in 98% of cases of medial instability enhancing the diagnose from 4% pre op to >50% post op, or Okuda et al. 22 that found 63% chondral lesions undergoing arthroscopy prior to ligament reconstruction, are being continuously supported by more recent papers like Vega et al. 23 where they found intra-articular ankle problems in 100% of the patients (Table 1). Nowadays, arthroscopy evaluation is considered the most important prognostic factor and, because of this, a thorough arthroscopic evaluation, as well as treatment of any intra-articular pathology, prior to ligament surgery, is recommended by most authors.17,24 The treatment of concomitant injuries is beyond the scope of this review.
Concomitant injuries.
Treatment
Although the natural history of ankle sprains is not completely understood, the inherent stability of the ankle mortice and its congruency might contribute to the fact that complete but isolated ATFL ruptures have a good prognosis. Most patients are successfully treated with functional treatment. 25 In some selected cases, especially in elite athletes, it has been proposed that early surgery can be considered as a first-line treatment to achieve a faster return to play.26,27
Non-operative
Optimal management of an ankle sprain is still unclear. Although there is an enormous amount of studies regarding CAI conservative treatment, the heterogenicity of them makes it difficult to make high-quality evidence recommendations.A 2017 meta-analysis 28 failed to clear this topic beyond reaching strong evidence for exercise therapy and bracing in preventing ankle sprain recurrence.
Most experts recommend functional rehabilitation and the use of bracing or taping. Rehabilitative exercises include proprioceptive training and evertor (peroneus brevis) strengthening. Ankle bracing or taping improves mechanical and functional stability in athletes with CAI. Both taping and bracing restrict range of motion, reduce reinjury rates, improve proprioception, have minimal negative effects on other joints, and do not affect athletic performance. Bracing with an ankle stabilising orthosis (a soft brace that provides compression and has straps crossing the ankle joint) limits varus/valgus angulation and provides proprioceptive feedback that helps to improve active stabilisation by the peroneus brevis. Taping is less bulky than bracing and may cater to unusual anatomy; however, bracing has the advantage of being reusable and easily adjustable. Approximately 80% of patients improve with functional rehabilitation and bracing. Nonsteroidal anti-inflammatory drugs, either taken orally or applied topically, may be used to provide short-term (1–3 weeks) pain relief and a reduction in swelling, but they have no long-term effects on the symptoms of CAI. 25 Another important subject withdrawn from the literature is the recommendation of checking whether the non-surgical treatment had been performed properly. If not, it is recommended to restart rehabilitation with most of the surgeons recommending at least 3–6 months of non-surgical treatment. 17
Surgical treatment
Despite adequate conservative treatment, around 20–30% of patients will develop CAI with persistent symptoms (fear of reinjury limiting activity, sense of giving away and recurrent sprains). The operative treatments for CAI include a variety of procedures ranging from simple repairs to complex reconstructions. Repairs consist of either reattaching or imbricating (shortening) the injured native tissues, whereas reconstructions involve replacing the ligaments with either autologous or allograft tissue. Furthermore, reconstructions may be either anatomic or nonanatomic.
Lateral chronic instability
Starting with lateral ankle instability, it is important to acknowledge that currently, there is insufficient evidence to support any specific superior surgical intervention in the treatment of lateral CAI. Nevertheless, non-anatomic reconstruction, as the classic Evans, Watson-Jones or Chrisman-Snook procedures, has been shown to significantly alter the normal biomechanics of the ankle complex, particularly the subtalar joint.29,30 Given these concerns, 31 and the favourable outcome of anatomic techniques, the former are currently the first line of surgical treatment.17,24,25 Anatomic open repair was first described in 1966 by Brostrom. 32 This technique respects the original anatomy by tightening the torn ATFL and CFL to the distal fibula. Several modifications were introduced over time, first by Gould et al. 33 that advised to suture the inferior retinaculum extensorum (RE) over the proximal ATFL end to augment the repair, then the modification by Karlsson et al. 34 advised to shorten the ligaments that were often not disrupted but elongated. Nowadays some authors advocate that the augmentation with non-absorbable suture tape may allow for less immobilisation and much earlier and aggressive rehabilitation, although there is still plenty of debate on this issue, with some recent studies failing to find any clinical advantage compared with the standard procedure.35–38 The most recent high-quality study regarding this open technique was a Level I randomised trial published by Ko et al. 39 in 2018 that reinforced the recent trend addressing only the ATFL accomplishing the same results as those who addressed both ATFL and CFL.31,40–42 The functional outcomes of these techniques in their many modifications have been classified as excellent, with success rates of 87–95%.33,34,43 All the anatomic repair techniques depend on the quality of the ligaments’ remnant in order to achieve an effective repair. Karlsson et al. 34 determined risk factors for the worst outcome: hyperlaxity, long-standing injuries and previous surgical treatment.
The current trend on the pursuit of minimally invasive techniques leads to the development of arthroscopically-assisted or all-arthroscopic procedures. In 1987 Hawkins proposed an arthroscopic stapling of the talus tensioning the scared tissue of the ATFL remnant, but due to unsatisfactory results, the technique was abandoned. In the early 2000s, thermal shrinkage with radiofrequency retracting the scared ATFL was presented with good results but only in the short term.44,45 In 2009, it was presented an arthroscopic-assisted Brostrom procedure by Corte-Real and Moreira 46 with the placement of a bony anchor in the distal fibula through the anterolcentral portal and needing an extra portal and a wound no longer than a centimetre to tie the first knot. The outcome of this kind of procedure was similar to the open Brostrom although with greater complications regarding the superficial peroneal nerve. Later, a modification of this technique was developed to avoid the neurologic risk, using an accessory anterolateral portal allowing retrieving of the suture from the medial to the lateral side of the superficial peroneal nerve, avoiding this way its entrapment. To avoid percutaneous steps and their inherent risks, the all-inside arthroscopic technique was later developed and in 2013 by Vega et al. 47 introducing the procedure with knotless suture anchor placed in the distal fibula tying the superior fascicule of the ATFL, and then it was added the biological augmentation using the inferior extensor retinaculum by Cordier et al. 48 In 2019 another paper was published about all-inside technique enhancing the previous procedure targeting also the inferior fascicule of the ATFL and CFL, what was a big change in the technique as being able to address these two extra-articular structures from an intra-articular point of view. 23 Before proceed to any gesture to the ATFL, the surgeon should assess its quality and subjectively categorise it as poor, moderate or excellent 49 in order to decide between a repair or reconstruction procedure. For biomechanical reasons, anatomic repair techniques are preferred over reconstruction procedures.1,9,10,16,23 The native histological characteristics of the injured ligament can only be maintained through its repair and these include the nerve receptors responsible for proprioception. If after arthroscopic assessment of ATFL, the ligament is considered to be of poor quality, which can happen in 20–41%48–51 of patients elected to surgery due to lateral ankle instability, reconstruction with allograft or autograft should be considered. In cases of ligament reconstruction, autologous Gracilis tendon graft seems to be the most consensual graft in the literature due to its biomechanical properties and easy access. 52 However, high cost and immunogenic response associated with allograft use are still a matter of concern, and autograft harvesting can be difficult and cause donor site morbidity. Therefore, techniques that sacrifice a tendon should be reserved for salvage procedures in patients with a failed ligament repair or with long-standing ligamentous insufficiency and absence of ligament remnant. The all-inside arthroscopic ATFL repair augmentation using non-absorbable sutures offers the benefit of maintaining the native ligament while reinforcing the repair, especially in patients with poor remnant ligament-tissue quality that otherwise would necessitate a reconstruction technique. In addition, augmenting the ligament repair with high-resistance sutures allows early rehabilitation without the need of extended protection.53,54 Other potential indications of this technique would include ankle instability with excellent or moderate quality ligament remnant and high demanding patient activity, contra-indications of prolonged ankle immobilisation or patients in need of faster postoperative ankle mobilisation. 49
In cases of microinstability, mimicking the open procedure described by Järvelä et al. 55 in 2002, Vega et al. 50 performed a cadaveric study proposing an arthroscopic transfer of the tibial origin of the ATiFL's distal fascicle onto the talar insertion of ATFL superior fascicle. This study proved that this all-arthroscopic procedure is safe and reliable.
Regarding RAI, Buchhorn et al. 56 proposed an open repair of both lateral and medial structures after a diagnostic arthroscopy. Vega et al. 10 described an ‘all-inside’ technique for the same pathology using a knotless suture anchor addressing both the lateral complex and the anterior deep fascicule of the deltoid ligament. In both studies, excellent clinical and radiographic outcomes were achieved. It is difficult to ascertain if patients would have had similar outcomes if they were treated only for the lateral ligamentous injury. It was from the authors’ experience that some patients treated with isolated lateral ligamentous repair developed postoperative medial ankle symptoms and residual pain. It was only in recognising the rotational instability injury pattern could we identify those patients who might have benefited from an additional deltoid repair. A cautious look for deltoid ligamentous injury is advised in every patient undergoing arthroscopic ankle ligamentous repair and the authors believe that any identified injury must be anatomically treated to allow for the best results.
Chronic medial instability
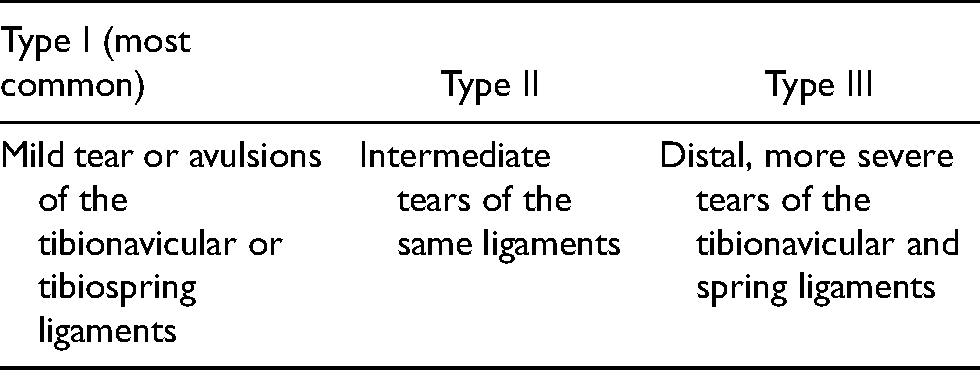
Because chronic medial instability often does not cause severe disability that cannot be treated conservatively and because the reconstructive options have had less success than those laterally, there is little information concerning the best treatment options for this difficult problem. The treatment options depend on the level of ligament injury and local soft tissue status (Table 2). 21 The primary option is to tension the deltoid from distal to proximal and attach it to the medial malleolus by transosseous sutures or anchors, provided that the deltoid tissue quality is sufficient. If the soft tissues are inadequate for a stable direct repair, reconstruction options are the alternative.
Types of medial-sided ankle sprains.
Reconstruction of
Reconstruction of the affected ligaments alone has been successful in inherently well-aligned feet; however, this is not the same in cases with longstanding hindfoot valgus and forefoot abduction. With these deformities, the achieved ligament repair tends to fail once the patients resume full physical and sports activity. These cases require either a lateral calcaneal lengthening OT or a medial sliding calcaneal OT to correct hindfoot valgus and forefoot abduction or hindfoot valgus only, respectively. 21
Conclusion
Ankle instability is an underdiagnosed but still very prevalent pathology. Understanding the anatomy and the biomechanics of the ankle is essential for both diagnosis and treatment. Non-surgical treatment is indicated for all cases, both acute and chronic, as the first line of treatment, leaving surgery for refractory cases or selected cases like professional athletes.
Nowadays, although diagnostic arthroscopy is considered mandatory, the open Brostrom-Gould procedure is still considered the gold standard of treatment of lateral ankle instability. On the other hand, with the existing trend for minimally invasive surgery and the development of newer devices, arthroscopic-assisted or all-arthroscopic procedures are expected to increase as well as procedures addressing the deltoid ligament.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.