
Abstract
Introduction
On March 11, 2020, the World Health Organization declared COVID-19 a global pandemic (WHO, 2020). Since this declaration, public health guidelines in the province of Ontario, Canada varied, including stay-at-home orders, social distancing, masking in indoor public settings, practicing optimal hand hygiene, regularly cleaning public spaces, and staying up to date on COVID-19 vaccines (Government of Ontario, 2022). Although these guidelines were intended to reduce the spread of the disease, there were also unintended consequences for many groups of society. In fact, a Canadian study conducted by Jenkins et al. (2021) nuanced the impact of the COVID-19 pandemic on the mental health of 3,000 adult individuals (Mage = 49.1; SD = 16.2). These authors reported that while there was a deterioration in mental health and optimal coping behaviors among Canadian adults during the early stages of the pandemic (May 2020), those who experienced preexisting additional vulnerabilities (e.g., health, social, structural) on the basis of mental health conditions, disability, income, ethnicity, sexuality, and/or gender were more likely to experience greater deteriorations in mental health and positive coping behaviors than those who did not experience additional vulnerabilities (Jenkins et al., 2021). Although public health guidelines were applied uniformly across the population, it is clear that some individuals were disproportionally affected.
Caregivers of school-aged children represent a cohort who have been impacted greatly by the COVID-19 pandemic (e.g., Dawes et al., 2021). This group of individuals has faced unique stressors, including, but not limited to, balancing childcare (Carroll et al., 2020; Leclerc, 2020), navigating online and in-person schooling for their children (Gallagher-Mackay et al., 2021; Suarez-Lopez et al., 2021), and managing children's behaviors and emotions (Loades et al., 2020; Maunula et al., 2021). Specifically, parents in Ontario had to adapt to four province-wide school closures (totaling almost eight months from March 2020 to January 2022), a three-month period of province-wide closures of childcare/daycare centers (from March to June 2020), and the cancellation of almost all extracurricular activities during periods of high COVID-19 case counts (Gallagher-Mackay et al., 2021). Compared to adults without children, caregivers with children living at home were at an increased risk of experiencing worsened mental health due to the pandemic (e.g., Gadermann et al., 2021). As part of the Ontario Parent Survey (2021) conducted from May to July 2021, 69% of caregivers (total n = 10,778) reported significant depressive symptoms within the last seven days, while almost a quarter reported that their anxiety was making it difficult to complete activities of daily living, including going to work and/or doing household tasks (Ontario Parent Survey, 2021). This points to the reality that facing ongoing psychological challenges limits a caregiver's ability to adapt to adversities, which may inadvertently impact their children's ability to do the same.
Concerns for children during the COVID-19 pandemic has included challenges with social, emotional, cognitive, physical, and behavioral skill development, as well as growing inequalities for children in families with low socioeconomic status (SES; Gallagher-Mackay et al., 2021; Herrenkohl et al., 2021). Despite the many losses children experienced during the pandemic, including learning interruptions and extracurricular cancellations (Subramanian, 2021; Williams, 2021), some researchers have suggested that the mental health of some Canadian children may have improved (e.g., Cost et al., 2021). In a Canadian study on 616 children ages 9 through 15, researchers reported that while many children were worried (27%) and sad (15%), over a quarter of children (26%) felt the pandemic had some positive impacts on their lives, including spending more time with family (37%) and pursuing personal interests (12%; Maximum City, 2020). Given the heightened emotional vulnerabilities of young children (Bagattini, 2019), combined with the long-documented importance of fostering emerging literacy capacities during early childhood (e.g., learning to read and write; Brooks-Gunn & Duncan, 1997; Hardy et al., 1997; Kagan & Kauerz, 2007; Ma et al., 2016), examining how young children coped through the adverse times of the COVID-19 pandemic is of particular importance.
Navigating adverse circumstances, such as those that arise during a pandemic, requires the resilience of children and other family members. Despite the existence of numerous definitions, resilience is often conceptualized as a dynamic process in which psychosocial and environmental factors interact to enable individuals to survive, grow, and thrive during exposure to adversity (Munoz et al., 2017; Prime et al., 2020). Family dynamics, including caregiver flexibility, positive caregiver–child relationships, constructive parenting, and parental strength are considered the foundation for family functioning, which has been identified as a key source of resilience within family units (Black & Lobo, 2008; Daks et al., 2020; Guruge et al., 2021; Torres Fernandez et al., 2012). It is likely that both caregivers and children may have increasingly called upon their resilience to cope during the COVID-19 pandemic, particularly if economic challenges were encountered by the family.
It is not surprising that the COVID-19 pandemic has been found to exacerbate existing inequities for families (Cusinato et al., 2020; Public Health Agency of Canada, 2020). In fact, economic hardships resulting from the pandemic have been primarily experienced by families with lower income and education levels, as well as those experiencing food insecurity, changes in working conditions, job losses, and heightened financial insecurities (Cusinato et al., 2020; Gallitto, 2020; Prime et al., 2020; SickKids, 2021). Although many COVID-19 guidelines were applied uniformly within distinct geographic regions of Canada, it is apparent that the resultant inequities, particularly those related to health in terms of morbidity and mortality, have impacted neighborhoods with higher ethnic diversities and lower incomes (Abrams & Szefler, 2020; Blair et al., 2022). Inequities in health may stem from disparities in income, education, and employment, with income level being the greatest confounding factor related to COVID-19 illnesses and deaths in Canada (Blair et al., 2022). Together, disparities in these conditions encompass a social hierarchy coined SES (Singu et al., 2020), which can be understood as the social standing of an individual or group (e.g., family), often measured as a combination of income, education, and occupation (American Psychological Association, 2022). Recent evidence has indicated that income alone may be insufficient when measuring financial stability and, as such, researchers suggest also including a measure of financial strain when measuring SES (Hamby et al., 2011). Overall, socioeconomic inequities compound existing health complications on top of financial burdens already impacting disadvantaged portions of the population (Singu et al., 2020). In the Canadian context, families experiencing compounding inequities are referred to as living in hot spots—which are social, systemic, and structural patterns of disadvantage that consider the intersectionality of the social determinants of health (McGrail et al., 2022). During the COVID-19 pandemic, there was a disproportionate rate of COVID-19-related illnesses and deaths in these hot spots, including those areas where the population was nonwhite and of low SES (McGrail et al., 2022).
Given the heightened effects of the COVID-19 pandemic on caregivers’ stress, anxiety, and depression (e.g., Lim et al., 2021; Marzilli et al., 2021; Mikocka-Walus et al., 2021), the impact of these stressful experiences (e.g., the pandemic, financial struggles, etc.) on child or caregiver resilience warrants further investigation. Further, while it is evident that the SES of some caregivers during the pandemic was impacted (e.g., Blair et al., 2022; Cusinato et al., 2020), the nature of the relationship between socioeconomic struggles and caregiver or child resilience remains unknown. This information is of critical importance to understanding the best avenues to take when attempting to bolster resilience among children and caregivers in future waves of the pandemic and/or similar crisis situations. To this end, the purpose of this study was to investigate, in the context of the COVID-19 pandemic, the relationships between (1) caregiver and child resilience; and (2) SES and the resilience of both caregivers and children.
Methods
Study Design
This cross-sectional, quantitative study was a substudy of the larger
Sampling, Eligibility, and Recruitment
Purposive (e.g., targeted ads in online parent groups) and snowball (e.g., caregivers sharing recruitment materials with friends) sampling techniques were used to recruit 27 child–caregiver dyads from locations across Ontario from February to October 2022. This sample size was deemed sufficient to achieve 95% power to detect a large effect size (i.e., f2 = 0.80) at a significance level of a = 0.05 for the planned analyses (Erdfelder et al., 1996).
Eligibility criteria included: (1) being a primary caregiver of a school-aged child (aged 7–10 years); (2) the caregiver–child dyad residing in Ontario; (3) the caregiver–child dyad speaking English; and (4) the caregiver–child dyad having access to an internet connection for audio-based conferencing software (i.e., Zoom). Primary caregivers were defined as any individual (e.g., parent, guardian) who identified as being primarily responsible for the well-being of a child or children) and dyads included each eligible and willing caregiver and child who belonged to the same household. As such, one caregiver could belong to a dyad with more than one of their children who participated. The age range of 7–10 years was selected to capture experiences of both lower- and upper-elementary children in Ontario (i.e., Grades 1–3 and Grades 4–6, respectively) and the existence of previously validated measures of resilience for this age range of children (Naglieri et al., 2013).
Interested participants were directed to email the research team using a secure study inbox, after which eligibility was confirmed. The target sample size for this study was 40 child–caregiver dyads; however, this target was unable to be met due to recruitment challenges encountered, including: (1) ineligible participants expressing their interest in the study and misrepresenting their children's age and/or their geographic location; (2) research bots sending hundreds of nearly identical emails per day, minutes apart, from fake email addresses; and (3) difficulties recruiting eligible caregivers given the already overburdened circumstances many parents were facing during the time of recruitment.
Data Collection
Data collection for this substudy consisted of two online qualtricsXM surveys, one for each member of the dyad, administered from February to October 2022 (Qualtrics, 2022). The data used included participant IDs, demographic responses from both caregivers and children, caregiver resilience scores, as measured by the Brief Resilience Scale (BRS; Smith et al., 2008), and child resilience scores as measured by the True Resilience Scale for Children (RS10; Wagnild, 2009). Each member of the dyad was provided with a $20 honorarium to recognize their contributions.
Demographics
As part of the caregiver survey, demographic questions included caregiver age, gender, marital status, geographic location, education, employment status pre- and during COVID-19, household income pre- and during COVID-19, financial strain, number of children, living situations of children (e.g., full time, part time), and school board of children. For the child survey, self-reported demographics included child(ren)'s age, gender, and school grade.
For the purpose of this study, SES variables included caregiver education levels, employment status, income, and financial strain, all of which were collected as part of the demographic block of the caregiver survey. Questions regarding SES included: (1) What is the highest certificate, diploma, or degree you have completed?; (2) What is the highest certificate, diploma, or degree that your partner has completed?; (3) What was your employment status prior to the COVID-19 pandemic?; (4)What is your current employment status?; (5) What was your average household annual income (after taxes are deducted), including employment, government, government cheques, child support, and other sources of income prior to the COVID-19 pandemic?; (6) What is your current household annual income (after taxes are deducted), including employment, government, government cheques, child support, and other sources of income?; and (7) the 5-item Financial Strain Index (Hamby et al., 2011). The Financial Strain Index was created to assess the ability of caregivers to meet current financial needs and asked participants to indicate whether the following five statements were very true, a little true, or not true about their current financial situation: (1) You do not have enough money to buy the clothes or household items that you or your family need; (2) You are behind one month or more on your rent or mortgage payment; (3) You do not have enough money to pay your regular bills; (4) You do not have enough money to go out to dinner or pay for entertainment or recreational activities; and (5) It would be hard for you to find the money to cover an unexpected expense, such as a medical bill or repair that was $500 or more. This scale has been previously validated to correlate with household income (r = −0.42) and internal consistencies have ranged from 0.73 to 0.83 (Hamby et al., 2011). To score the Financial Strain Index, responses were summed across the five items and provided a score between 5 and 15, with higher scores indicating more financial strain (Hamby et al., 2011).
Resilience Measures
Caregiver resilience was measured via the 6-item Brief Resilience Scale (Smith et al., 2008). This resilience scale was originally developed to assess one's ability to adapt to stress, bounce back, resist illness, and thrive, despite facing adversity (Agnes, 2005; Smith et al., 2008). The six items of the BRS ask caregivers to respond to the following statements using a 5-point Likert scale ranging from strongly disagree to strongly agree: (1) I tend to bounce back quickly after hard times; (2) I have a hard time making it through stressful events; (3) It does not take me long to recover from a stressful event; (4) It is hard for me to snap back when something bad happens; (5) I usually come through difficult times with little trouble; and (6) I tend to take a long time to get over setbacks in my life. In previous research, factor loadings for this scale have ranged from 0.67 to 0.91 with results revealing a one-factor solution that accounted for 55–67% of the variance (Smith et al., 2008). This scale has also been found to be reliable and have good internal consistency with Cronbach's alpha ranging from 0.80 to 0.91 (Smith et al., 2008). To score the BRS, items 2, 4, and 6 were reverse coded and the means of the six items were determined by adding the responses varying from 1 to 5 for each of the six items giving a range from 6 to 30 and dividing the sum by the total number of questions answered (Smith et al., 2008). Item scores ranging from 1.00–2.99 indicate low resilience, 3.00–4.30 indicate “normal” resilience, and 4.31–5.00 indicate high resilience (Smith et al., 2013). Higher scores on the BRS indicate a greater ability to bounce back or recover from stress (Smith et al., 2008).
Child resilience was measured using the 10-item True Resilience Scale for Children (Wagnild, 2009). The RS10 measures a child's ability to respond in a positive way to life events (Wagnild, 2009), with items asking children to determine the extent to which the following statements relates to them: (1) I finish what I begin; (2) When I get upset, I know how to calm down; (3) I like to think about all of the things I want to do; (4) I don’t like to give up, even when something is hard to do; (5) I like to practice hard to get good at what I’m doing; (6) I am excited to learn new things; (7) I am happy with myself; (8) When I do something, I want to do it well; (9) I like to find something to laugh about every day; and (10) I think I’m okay just the way I am right now. Response options include children believing the statement is “Not at all like me,” “Not much like me,” “Somewhat like me,” or “A lot like me.” This scale has been deemed appropriate for children ranging from 7 to 12 years of age based on the Flesch Reading Ease score of 94.8, meaning it should be easily understood for children in the age range (The Resilience Centre, 2021). Further, in previous research that tested the RS10 for validity, Cronbach's alpha was 0.82, meaning that this scale has displayed good internal consistency and is a reliable measure of resilience in this target population (Taber, 2018; The Resilience Centre, 2021). The scores for each of the items on the RS10 can range between 1 and 4, with total scores ranging from 10 to 40. Higher scores suggest greater resilience, although lower scores do not suggest an absence of resilience (The Resilience Centre, 2021).
Data Analysis
Demographics
Measures of central tendency, dispersion, and frequencies were computed for caregivers’ sociodemographic measures of age, gender, marital status, geographic location, education, employment status pre- and during COVID-19, household income pre- and during COVID-19, number of children, living situations of children, and school board of children. The same analyses were run for children's sociodemographic measures of age, gender, and school grade.
Relationship Between Resilience of Caregivers and Children
A Pearson Product–Moment correlation was conducted to examine the relationship between caregiver and child resilience. To determine whether the relationship between caregiver and child resilience was statistically significant, the absolute obtained value of the correlation coefficient was compared to the critical value of the correlation coefficient. The effect size was assessed via the coefficient of determination.
Relationship Between SES and Resilience of Caregivers and Children
A total of eight correlations were conducted to determine the relationship between SES and the resilience of caregivers and children. Four Pearson Product–Moment correlations were conducted to examine the relationship between primary caregivers’ income and financial strain and the resilience of both caregivers and children. For the ordinal-level variables of education and employment, an additional four Spearman's Rho correlations were calculated to examine the relationship between these SES constructs and the resilience of both caregivers and children. Effect size estimates were also calculated for each correlation to determine the magnitude of effect for each SES variable.
Results
Participants
Participants in this study consisted of 22 caregivers (Mage = 40.45 years; SD = 4.55) and 27 children (Mage = 8.19 years; SD = 1.14) living in Ontario, Canada. Most caregivers identified as female (n = 20; 90.90%) and reported being married (n = 19; 86.36%) and living in large urban centers (i.e., 100,000+ population; n = 15; 68.18%). Half (50%) of the sample reported achieving a college or university degree, with approximately 45% of participants’ partners reporting the same. Most participants reported being employed full time prior to the COVID-19 pandemic (n = 15; 68.18%) and at the time of survey completion, which was almost two years into the pandemic (n = 13; 59.05%). The average annual household income of families prior to the pandemic was $109,579 CAD and during the pandemic was $105,500 CAD. Out of a possible total score of 15, the average financial strain reported by caregivers was 6.95 (SD = 2.65), indicating low financial strain (Hamby et al., 2011). Full demographic characteristics can be found in Table 1.
Child and Caregiver Demographic Characteristics.
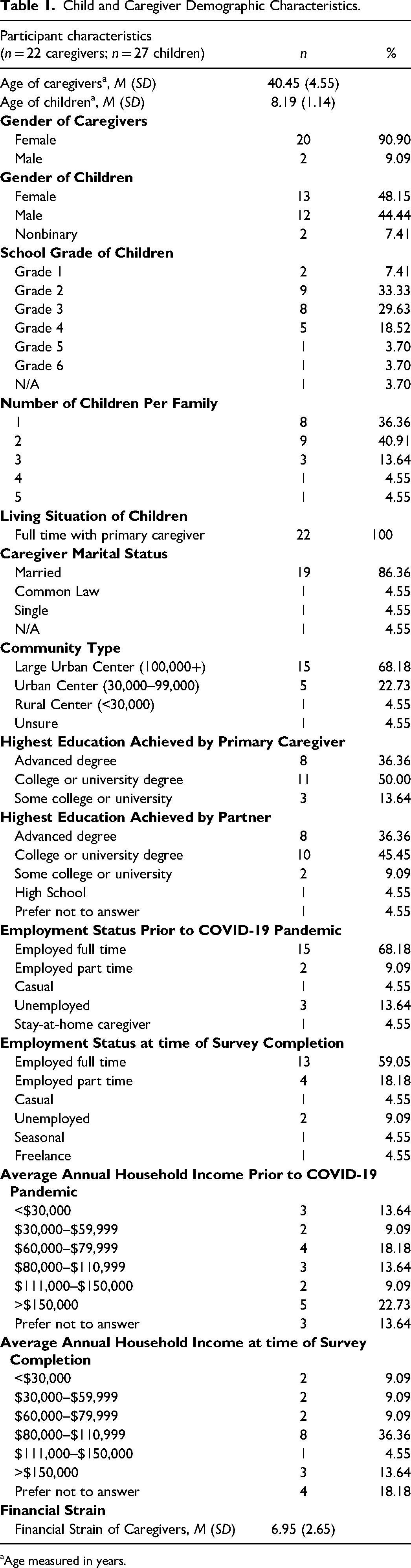
aAge measured in years.
Of the children who participated, 13 identified as female (48.15%), 12 as male (44.44%), and 2 as nonbinary (7.41%). The school grades of children ranged from Grades 1 to 6, with most being in either second (33.33%) or third (29.63%) grade (i.e., 62.96% of children were either 7 or 8 years old). According to caregiver reports, all children lived with their primary caregiver full time, and most lived with either no siblings (36.36%) or one sibling (40.91%). Eleven school boards were represented, with no more than three dyads attending the same school board.
Relationship Between Resilience of Caregivers and Children
Total self-reported BRS scores for caregivers had an average of 19.73 (SD = 4.58) and a mean item score of 3.29 (SD = 0.25; see Table 2), indicating that caregivers in this sample reported “normal” levels of resilience according to the scoring protocol for the BRS. Total self-reported RS10 scores among children had a mean total score of 33.04 (SD = 3.96; see Table 3), which aligns with children developing their resilience as per the scale's scoring guidelines. Results from the Pearson product–moment correlation provided no evidence of a significant relationship between caregivers’ and children's resilience scores, r (28) = −0.21, p = .26 (see Table 4). The children of caregivers who reported low resilience scores (n = 6 caregivers) were found to report varying resilience scores, ranging from 31 to 39 out of a possible 40, which is on average with the rest of the child resilience data.
Descriptive Statistics for Self-Reported Caregiver (n = 22) Resilience as Measured by the Brief Resilience Scale.
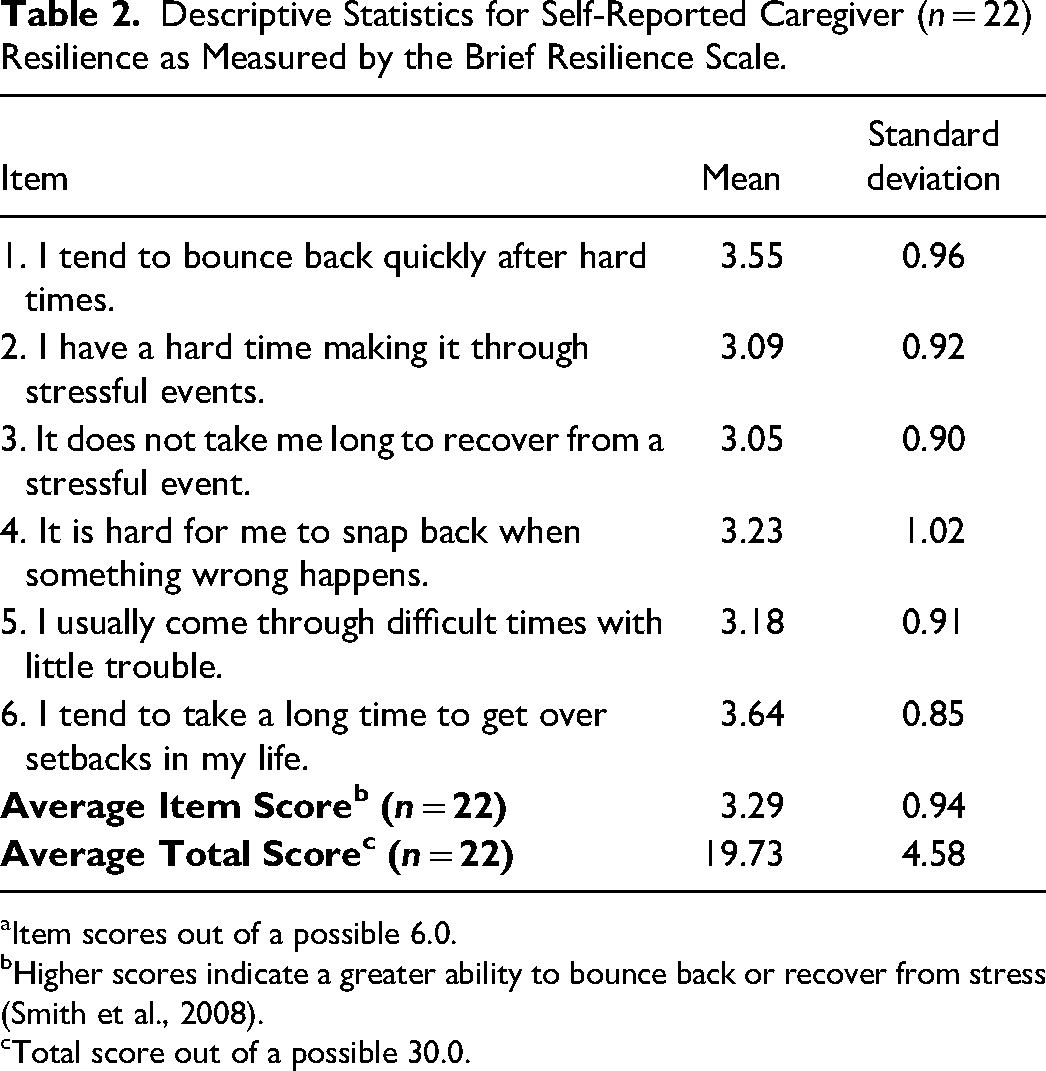
aItem scores out of a possible 6.0.
bHigher scores indicate a greater ability to bounce back or recover from stress (Smith et al., 2008).
cTotal score out of a possible 30.0.
Descriptive Statistics for Self-Reported Child (n = 27) Resilience as Measured by the True Resilience Scale for Children.
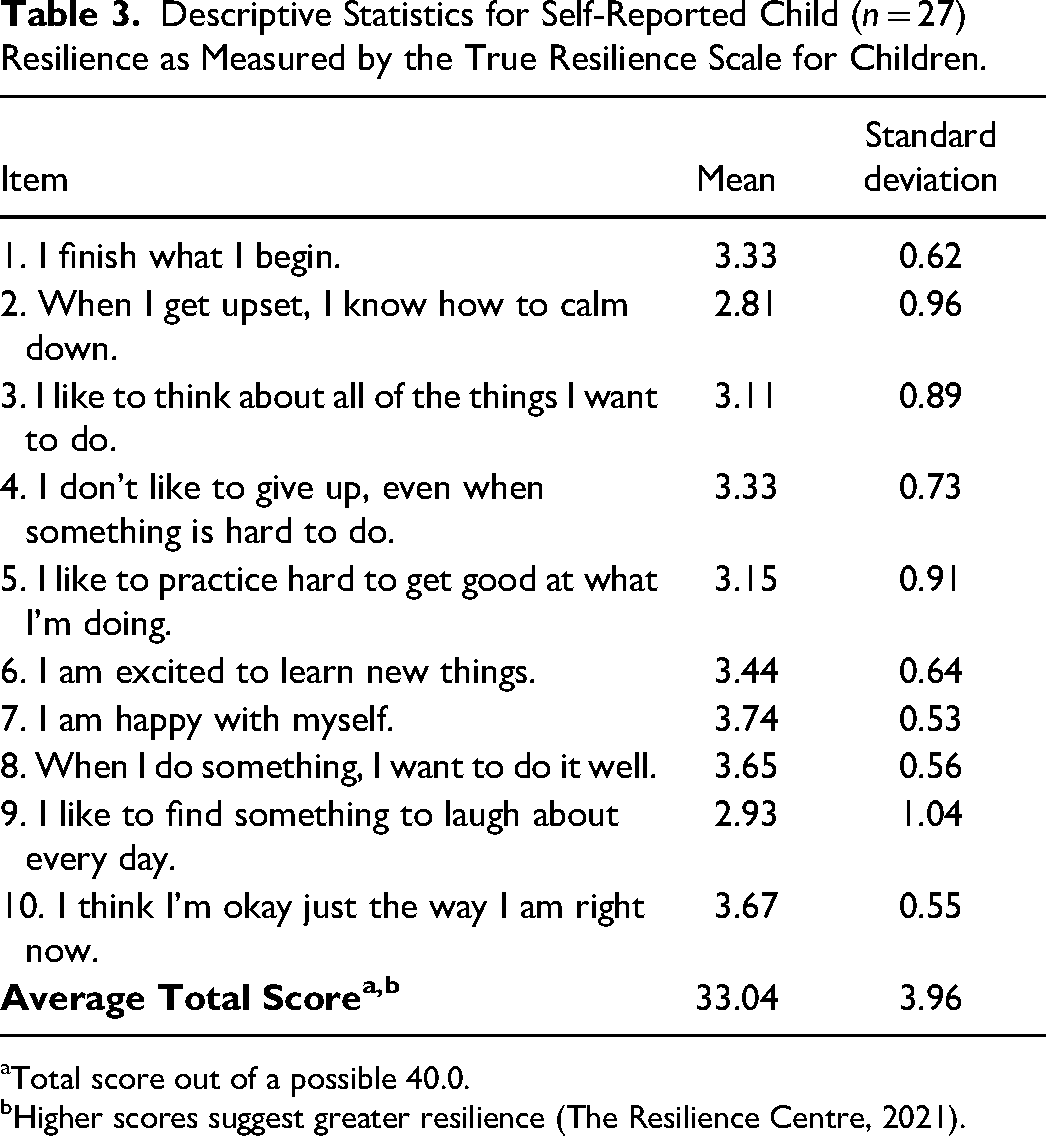
aTotal score out of a possible 40.0.
bHigher scores suggest greater resilience (The Resilience Centre, 2021).
Correlations Between Caregiver and Child Resilience.
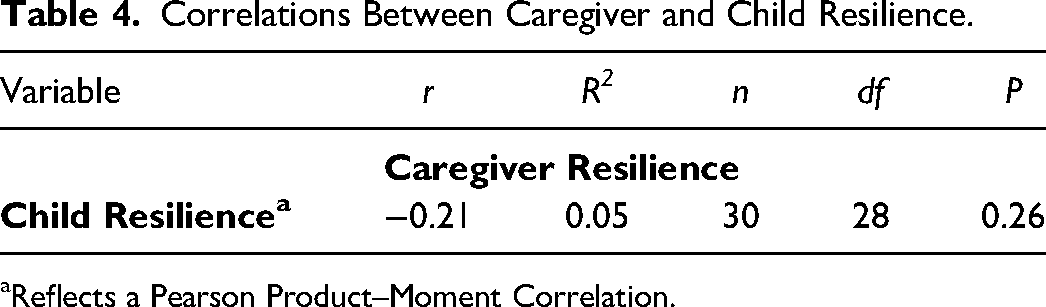
aReflects a Pearson Product–Moment Correlation.
Relationship Between SES and Resilience of Caregivers and Children
None of the correlational analyses investigating relationships between family SES and caregiver/child resilience demonstrated statistically significant interactions (see Table 5).
Correlations Between Caregiver or Child Resilience and Family Socioeconomic Status (SES) Variables.
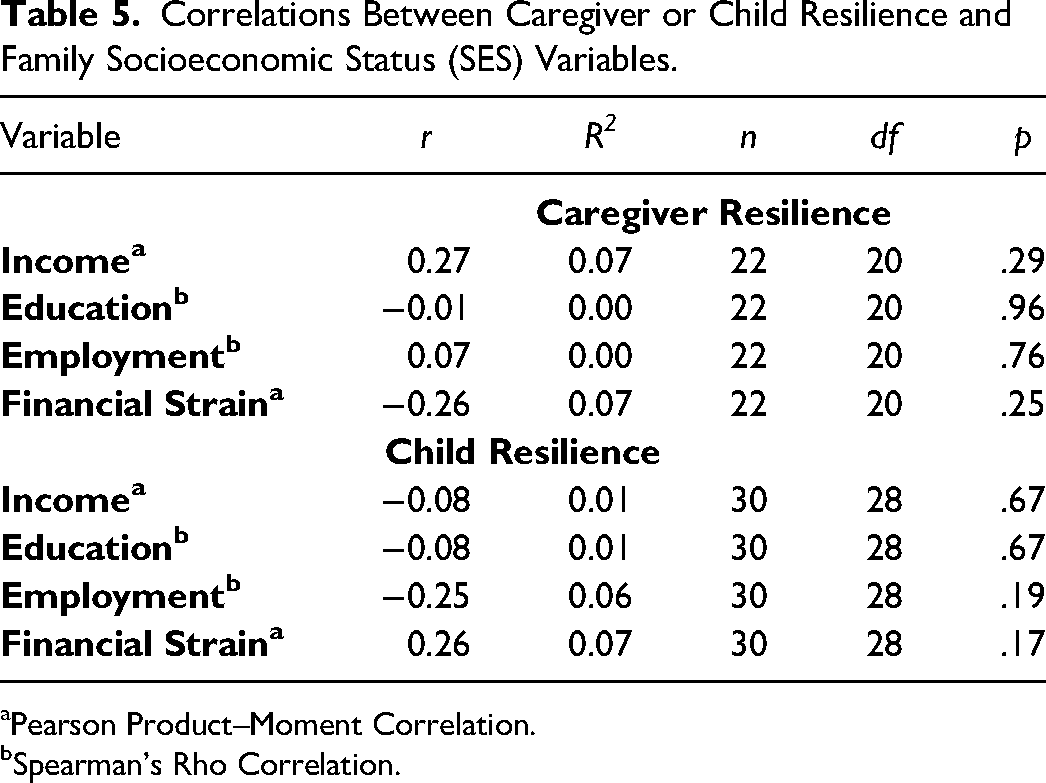
aPearson Product–Moment Correlation.
bSpearman's Rho Correlation.
Due to the limited sample size, the current study was not powered to run subanalyses using the SES and resilience data; however, trends between the constructs were investigated. Despite the lack of significance, the strongest positive correlation was found for the relationship between caregivers’ resilience and their income. According to the BRS scoring protocol, six caregivers had low resilience; the average annual household income was $70,800 CAD among these individuals. Conversely, among those caregivers who reported “normal” levels of resilience, the average income was $118,846 CAD. Contrary to the above, when investigating children's resilience as it related to caregiver's income, those children with the lowest resilience scores (i.e., scale scores between 10 and 30; n = 5 children) had caregivers who reported moderate to high income. In fact, those caregivers who reported the lowest income in our sample had children who scored in the two highest categories of resilience scores (i.e., growing-scale scores of 35–37 and thriving-scale scores of 38–40; n = 10 children). No trends were detected between the resilience of caregivers or children and the remaining SES variables.
Discussion
The purpose of this study was to investigate, in the context of the COVID-19 pandemic, the relationship between: (1) caregiver and child resilience; and (2) SES and the resilience of caregivers and children. Analyses revealed no significant relationship between caregiver and child resilience. Moreover, no significant relationships were found for family SES and the resilience of either caregivers or children during the COVID-19 pandemic. Despite the lack of significant findings, interestingly, the average income between those caregivers with low versus normal resilience scores varied by approximately $48,000 CAD, such that those with “normal” levels of resilience reported having a higher average income.
No significant relationship was detected in the current sample between caregiver and child resilience. This finding adds to an already mixed literature which showcases the ambiguity or indeterminate nature of the relationship between caregiver and child resilience (e.g., Caputi et al., 2021; Mariani Wigley et al., 2021). The average resilience score for caregivers indicated that caregivers in this sample experienced “normal” levels of resilience during the COVID-19 pandemic (Smith et al., 2008). In line with previous research, the “normal” resilience levels found in this study supports the notion that resilience is a common response to adverse experiences (Bonanno et al., 2011; Chen & Bonanno, 2020; PeConga et al., 2020; Zhang et al., 2022). In fact, the many COVID-19-related adversities faced by caregivers (e.g., adjusting to working multiple roles, isolation from supports) likely required caregivers to be resilient in response. Pre-pandemic research by Bonanno et al. (2011) reported a similar phenomenon with a rapid return to “normal” or “baseline” functioning being the most common response following mass experiences of trauma.
Another factor that may have contributed to the resilience scores of caregivers in this study could be the relatively high SES observed relative to the broader Ontario population. It is well-established in research that the COVID-19 pandemic has disproportionately impacted families experiencing multiple disparities (e.g., change in working conditions, reduction in income; Cusinato et al., 2020; Prime et al., 2020; Wu et al., 2021). Specifically, data have indicated that low-income families have been impacted the most by COVID-19 pandemic-related disruptions (Valentino-Devries et al., 2020). To this end, the relatively high SES, and more specifically the relatively high average income (i.e., $105,500 CAD) and lack of job losses reported by participants in the current study could have buffered them from some of the stressors associated with the pandemic (Cusinato et al., 2020; Valentino-Devries et al., 2020). Perhaps not having to grapple with substantial income- or job-related disruptions during the COVID-19 pandemic meant study participants were better positioned to respond to this global crisis, which in turn, could have contributed to their “normal” resilience scores.
Children in this study reported mid-to-high levels of resilience. This finding is contrary to the early pandemic hypotheses advanced by leading children's researchers, suggesting that children would experience psychological struggles, including low resilience, during the pandemic (e.g., Cost et al., 2021; SickKids, 2020, 2021). Notably, Chung et al. (2021) found that among a Chinese sample of school-aged children (n = 186, Mage = 10.4 years, SD = 2.5 years), average resilience scores fell into the lowest quartile during the COVID-19 pandemic. Comparatively, children in the current study reported higher levels of resilience through the pandemic than their age-similar peers in the Chinese sample. This could point to the timing of data collection between these studies. While Chung et al. (2021) collected data early in the pandemic (i.e., March–December 2020), data collection in the current study took place almost two years into the pandemic (i.e., February–October 2022). The higher self-reported resilience scores among children in the current sample may point to a stabilization in resilience as the pandemic progressed. This distinction could also be due to variations in pandemic-related adversities faced by the two samples, including the length and severity of lockdown measures. More specifically, children in Ontario could have been afforded more opportunities to support their resilience than children in China, due to the less stringent COVID-19 measures in place.
There was also no significant relationship between the self-reported resilience of either caregivers or children and the family SES variables reported by caregivers. While the study was not powered to compute subanalyses, there was a trend observed between the income and resilience of caregivers. COVID-19-specific research is clear that there is a disproportionate burden on low SES families, such that they are less likely to have economic buffers in place to cope with sudden adversities (Cusinato et al., 2020; Prime et al., 2020; Valentino-Devries et al., 2020; Wu et al., 2021). Among a nationally representative sample of adults in Canada (n = 3,000), financial concerns were among the highest reported stressors early in the COVID-19 pandemic (Jenkins et al., 2021). Moreover, of those surveyed, those who reported a low household income were more likely than their higher income counterparts to identify COVID-related coping challenges. Based on these findings, it is probable that challenges coping during COVID-19 may be a rationale for the low levels of resilience seen among the current sample of caregivers with lower income. A study conducted by Bates et al. (2021) on caregivers of children (n = 245) in the United States further supports this as the authors reported that COVID-19-related stress was significantly higher among participants with a low family income, and this stress was significantly negatively related to family resilience during the early pandemic (i.e., May 2020). These results are similar with the trend found in the current study regarding caregivers with low resilience reporting a lower average annual household income than caregivers who reported “normal” levels of resilience. This suggests that household income may play a role in caregivers’ resilience in the context of the COVID-19 pandemic.
Interestingly, the same trend between caregiver income and resilience levels was not found among children in this sample. Children with caregivers who reported low income reported mid-to-high resilience scores, which may suggest that children were protected from socioeconomic hardships experiences by families during the pandemic. In fact, children with the lowest self-reported resilience scores had caregivers who reported a higher-than-average income. In a study by Luthar and Latendresse (2005) on 614 American sixth-grade students, differences between affluent and low-income families were investigated. Notably, this study reported that compared to parents with higher self-reported incomes, parents who reported having a low income were no more emotionally distant, and their children did not differ in average levels of perceived closeness to caregivers or in the frequency with which they ate dinner with at least one parent (Luthar and Latendresse, 2005). Together with the lack of trends in the current study, it is clear that one cannot assume that the demands of low SES will result in less adequate care for children by caregivers; instead, findings could lend to the idea of parents sheltering their children from those adversities (e.g., financial strain).
Limitations
Findings from this study should be considered within the context of the limitations. First, the sample was not entirely representative of the broader population in Ontario, Canada. The gender representation among caregivers in this study was not representative of the larger population; however, the ratio of female to male caregivers who participated in this study (10:1) is what was expected based on past research studies on this population (Davison et al., 2017; Phares et al., 2005). Research with caregivers typically solely involves mothers, with only 26% of studies on child development including perspectives from fathers (Phares et al., 2005). Moreover, the average caregiver-reported household income of this sample after taxes surpassed that of the average Ontario household ($105,500 versus $80,322, respectively; Statistics Canada, 2011). Knowing that the pandemic may have had vastly different impacts on those of low SES or those of a broader gender representation, it is important to strive to include these populations in future research. Second, the small sample size of 22 caregivers and 27 children may have limited the detection of significant relationships between constructs. Although the study was powered to complete the planned analyses, no powered subanalyses could be conducted, which limited the ability to interpret meaningful differences between the constructs of interest. Finally, although validated measurement tools were employed to maximize the rigor of this study, data collection relied on self-report which is prone to biases (Bauhoff, 2011).
Conclusion
Caregivers and school-aged children in Ontario have experienced unique challenges throughout the COVID-19 pandemic. Based on previous research conducted during adverse times, many experts believed that pandemic-related challenges would negatively impact the resilience of these individuals; however, the results from this study do not suggest that resilience was hindered. In fact, neither the resilience of caregivers nor children in this study was considered low. This suggests that approximately two years into the pandemic, families were resilient through the ongoing adversities. Although no significant relationships were found between self-reported resilience and SES among participants, there was a clear trend found for the income and resilience of caregivers, in that those with lower income seemed to experience lower resilience. Children of low-income households, however, seemed to be protected from these hardships, as the resilience of children from low-income families was not found to be low. Future research should examine possible environmental factors that contribute to the resilience of caregivers and children through adversities. It is critical to identify risk and protective factors that contribute to helping families survive, and even thrive, through crises to ensure a proactive and effective public health response in future iterations of the pandemic or pandemic-similar situations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Social Sciences and Humanities Research Council (SSHRC) Insight Development Grant.