
Abstract
The present randomized control trial examined the effectiveness of Gottman Method Couples Therapy (GMCT) over treatment-as-usual (TAU) approaches for couples presenting for therapy following the discovery of infidelity. Forty-nine couples participated in this trial and were randomized to either a GMCT or TAU control group, with 19 completing all pre- and post-treatment assessments. Results showed that GMCT was globally more effective in facilitating affair recovery than TAU approaches, notably in the areas of trust, conflict management, relational satisfaction, and quality of sex. In this article, we (a) outline findings from this study, (b) discuss implications for the field, and (c) offer directions for future research.
Infidelity is a significant source of distress for couples, contributing to enduring and devasting relational consequences, including but not limited to separation or divorce (Vossler & Moller, 2014), increased depression and anxiety (Schneider et al., 2012), and posttraumatic stress disorder (PTSD) symptoms such as hypervigilance and intrusive thoughts (Gottman & Gottman, 2017; Irvine, 2022). Among heterosexual couples, lifetime rates of infidelity in the United States range from roughly 22% for men and 13% for women, with anywhere from 20% to 40% of couples worldwide admitting to having engaged in an affair during their lifetime (General Social Survey, 2017; Irvine & Peluso, 2022; Peluso, 2019). Recently, Gottman et al. (2020) presented the results of assessments from over 40,000 couples seeking couple therapy and completing the Gottman Connect (GC) assessment tool, a battery of online questionnaires (reviewed further below). They found that a large majority of the sample had at least one partner who engaged in an affair at a rate of nearly one-third of heterosexual couples, more than 43% of gay male couples, and one-fourth of lesbian couples. Ultimately, infidelity appears to be a cross-cultural variable, with this betrayal occurring when “self-interest is at the partner's cost” (Gottman, 2011, p. 108).
Practitioners surveyed over the last three decades consistently identify infidelity as one of the most frequent and challenging presenting issues (Glass & Wright, 1992; Irvine & Peluso, 2022; Softas-Nall et al., 2008; Vossler & Moller, 2014; Whisman et al., 1997). In addition, clinicians feel least prepared to address infidelity over all relationship issues presenting for couple therapy (Irvine & Peluso, 2022; Softas-Nall et al., 2008). According to Irvine and Peluso (2022), clinicians’ unpreparedness is attributable to “the lack of specialized training in graduate programs to treat infidelity-related issues such as navigating affair disclosure and managing countertransference reactions” (p. 324). Additionally, in this mixed-methods study, the researchers examined 351 couple therapists’ experiences treating affairs, revealing that roughly 90% of participants denied having ever received an infidelity-specific course in their graduate training program. More concerning, only 48% of respondents had attended an infidelity training during their career, despite actively treating couples for infidelity.
With the rise of couples presenting for affair recovery therapy, a lack of clinical competency in treating infidelity is alarming, further substantiating the need for evidence-based treatments (EBTs) to address this complex issue effectively. Yet, despite this clinical issue's high prevalence and overall challenging nature, the literature is significantly lacking in EBTs for graduate trainees and clinicians to not only broach but also treat infidelity effectively. Therefore, we sought to examine whether Gottman Method Couples Therapy (GMCT) would be more effective than treatment-as-usual (TAU) approaches for couples presenting with infidelity-related issues, intending to validate GMCT as an evidence-driven approach to help promote affair recovery. For the purpose of this study, the following research questions were explored: (a) Will the use of GMCT or TAU approaches significantly improve the relationship quality of couples following an affair? and (b) Will the effects of treatment vary between couples from the experimental group (i.e., GMCT) versus the control group (i.e., TAU)?
Definitions for the Current Study
Infidelity among couples is a highly subjective experience influenced by various intersecting factors such as cultural/ethnic background, gender, sexuality, power dynamics, and social context (Weiser et al., 2023). As a result, the research literature comprises several definitions of an affair (or infidelity), contributing to more than an 84% cause of variance (Moller & Vossler, 2015). For this reason, Weiser et al. (2023) assert that “a universal definition of infidelity is an illusion” (p. 10). Therefore, in an effort to decrease the stigmatization which often circumscribes this topic, we operationally define infidelity as any clandestine emotional/ romantic, physical/sexual, or technology-based liaison with a third party in which one member of the relationship has violated an exclusivity agreement or boundary and considers the interaction(s) as a breach of trust and safety, causing relational harm or distress to the primary romantic partner. Additionally, throughout this manuscript, we refer to the partner who had an affair as the involved partner (IP) and the partner who was hurt or did not have an affair as the uninvolved partner (UP).
Evidence-Based Treatments for Infidelity
Few studies exist specifically validating EBTs for affair recovery (Irvine, 2022). The research literature lacks randomized control trials (RCTs) to support this endeavor, with fewer than 10 efficacy-based studies conducted in the past 15 years (Stamps, 2020). This gap is concerning as RCTs are crucial to validating the effectiveness of treatment interventions and providing generalizable results (Hariton & Locascio, 2018). To date, integrative couple therapy (Gordon et al., 2004; Kröger et al., 2012), behavioral couple therapy (Atkins et al., 2005b; Marín et al., 2014), and emotion-focused couple therapy (Greenberg et al., 2010) are three broad-based couple therapy approaches that have generated RCT studies to validate their methods for affair recovery. However, several limitations exist among these studies, including only sampling married couples, restricting inclusion criteria to couples in the United States, and not exclusively recruiting infidelity couples (Irvine, 2022). Irvine (2022) recently conducted an international RCT validating GMCT for couples seeking infidelity treatment. We sought to further expand on preliminary effectiveness findings by comparing GMCT against TAU approaches for couples seeking affair recovery treatment.
Gottman Method Couples Therapy
For over 30 years, Dr. John Gottman, Dr. Julie Schwartz Gottman, and associates (Gottman et al., 2002; Gottman, 1994, 1999) have studied couples in laboratory settings, obtaining rich information about the workings of successful marriages and relationships. More recently, Gottman and Gottman (2017) have translated this information into a practical clinical approach for helping couples address multiple relationship functioning issues. They have also created several inventories, drawing from decades of empirical work, that tap into critical areas of relationship functioning. Clinicians who become trained in GMCT, referred to as Certified Gottman Therapists (CGTs), are trained to provide a systematic approach to couples therapy that addresses many of the underlying issues of infidelity, such as managing hostile conflict, addressing feelings of betrayal, and rebuilding trust (Gottman & Gottman, 2017). However, until now, scholars have not empirically compared GMCT to broad-based TAU approaches. In this article, we (a) outline findings from this RCT, (b) discuss implications for the field, and (c) offer directions for future research.
Method
In this RCT, we compared an experimental group of CGTs against a control group of similarly licensed couple therapists or TAU clinicians. As part of the recruitment protocol, each CGT was asked to suggest a couple's therapist in their area, controlling for the geographic region between the experimental and control groups; this strategy also provided a homogeneous sample of clients for both groups. We review both couple and therapist participants’ demographic data below.
Participants and Recruitment Procedure
Couple participants
We collected data between March 2017 and August 2022 from a random, voluntary sample of 49 couples seeking couple therapy for infidelity, whether physical/sexual, emotional, or technology/cyber-based. To minimize the potential for confounding data, we defined the term couple as any dyad who identified as being in an exclusively monogamous romantic relationship for a period of at least 6 months or longer at the time of the study (Irvine, 2022). Couples were permitted to participate with the primary inclusion criterion of infidelity as the presenting problem for treatment. In addition, research personnel screened all participants before enrollment, excluding couples from partaking in the study if there was an active addiction, a language barrier (i.e., non-English speaking for observational coding purposes), or characterological intimate partner violence, where offenders use violence to control or hold power over one's partner (Friend et al., 2011). From here, we randomly assigned participants to the CGT or TAU control group.
Forty-five couples participated in the current study. However, after removing couples who were either disqualified from participating or dropped out (n = 33), 19 couples (n = 38 individuals) completed assessments at both pre- and post-treatment and were included in the final data analysis, consisting of 19 males, 18 females, and one non-binary individual. The median age of participants was 43.9 years old, with all individuals identifying as heterosexual. The sample predominantly consisted of Non-Hispanic White or Euro-American participants (n = 35), with the remaining participants identifying as Black or African American (n = 2) and Latinx or Hispanic (n = 1). Approximately 95% of respondents were from North America. Regarding religious affiliation, participants predominately identified as Christian (65.8%) and had an income of less than $50,000 (36.7%). Finally, participants were mainly married at the time of the study (89.5%), with the remaining participants identifying as being in a committed relationship (10.5%).
Therapist participants
Therapist participants included 17 CGTs and 15 TAU couple therapists. TAU clinicians encompassed a wide range of theoretical orientations, including eclectic/integrative (n = 6), emotion-focused therapy (n = 4), psychodynamic therapy (n = 3), systems-based therapy (n = 1), and trauma-informed therapy (n = 1). We recruited therapist participants in several steps. First, research personnel at The Gottman Institute selected CGTs based on (a) having been a CGT for over 5 years and (b) supervising another therapist toward certification. This process ensured that the therapist was accurately utilizing GMCT. Similarly, TAU therapists were invited to participate if they reported having prior experience treating couples for infidelity. Finally, as compensation for participating, TAU therapists were solicited by research personnel and became eligible to receive the Gottman Level 1–3 trainings following the study's completion.
Treatment Procedure
Before recruiting and subsequently randomizing participants, this study was reviewed and subsequently approved by the university's institutional review board. This study incorporated a multimodal assessment strategy, including observational and self-report assessment methods, to analyze couples’ pre- and post-treatment relational dynamics. Treatment took place over an average of 32 sessions, and couples were administered all measures at the first (pre-treatment) and last (post-treatment) therapy sessions. Specifically, couples were asked to complete the GC assessment tool, an online measure consisting of 480 questions to assess couples’ relationship function, averaging 1–2 h to complete per partner. Each sub-scale assessed couples’ relationship distress and symptoms at both pre- and post-treatment. According to Irvine (2022), “Decades of research have validated the efficacy of the GC assessments based on psychometric data and clinical experience,” demonstrating excellent reliability and validity across measures (p. 60). For more detailed information about the GC assessment tool scales, see (Gottman, 1999).
Next, clinicians asked couples in both treatment groups to engage in a 10- to 15-min conflict discussion about an ongoing problem in their relationship without intervention from the therapist; couples were prohibited from discussing the affair as their conflict topic to avoid skewing the findings. These segments were then video recorded, with participant consent, and were repeated at pre- and post-treatment time points of measurement to assess for interactional patterns (see https://www.gottman.com/about/the-gottman-method/ for additional GMCT protocol information). Finally, we utilized Coan and Gottman's (2007) revised Specific Affect Coding System (SPAFF) to code couples’ pre- and post-treatment conflict discussion recordings. We describe this procedure below.
Specific affect coding system (SPAFF) procedure
The SPAFF measures the emotional behavior of a dyad in real-time and can be used in any conversation. In addition, this coding system focuses exclusively on participants’ expressed affect, drawing on facial expressions, vocal tones, and speech content to characterize the emotions displayed (Gottman et al., 1996). According to Gottman et al. (2002), the SPAFF uses 20 codes, ranging on a continuum from positive to negative, to categorize the behavioral affects displayed using seven positive codes (interest, high validation, low validation, affection, humor, surprise/joy, and tense humor), 12 negative affect codes (disgust, contempt, criticism, belligerence, high domineering, low domineering, anger, tension, defensiveness, whining, sadness, stonewalling), and one neutral affect code. See Gottman et al. (1998) for a further breakdown of each code.
Per Gottman et al.'s (1996) protocol, two independent observers trained in this coding scheme coded each conflict discussion in its entirety, computing inter-rater reliability before entering the codes into the dynamic non-linear equations. Next, we analyzed these codes to determine the frequency and percentage of positive, negative, and neutral affect codes. Affect codes (using the modified SPAFF) are summed over a 6-s interval, considered a single data point. For example, with a 15-min conflict discussion, there are 900 s which, when summed over 6-s time blocks, yields 150 data points from each participant. The SPAFF has demonstrated excellent reliability and validity (Gottman et al., 1996; Hayman et al., 2001).
Treatment Approach: The Trust Revival Method
Couples assigned to the CGT group were exposed to Gottman and Gottman's (2017) Trust Revival Method (TRM), an evidence-driven approach created to promote healing and affair recovery (Irvine, 2022). Treatment fidelity was facilitated by having all CGT participants in this study learn the TRM intervention in the GMCT training, Treating Affairs and Trauma (Gottman & Gottman, 2017). Irvine (2022) noted that the TRM is different than other broad-based couple therapy approaches to treat affairs in that “the TRM opts not to down-regulate the UP's feelings; instead, this approach addresses PTSD symptoms that may be present, lending to increased distress and relational dissatisfaction” (p. 45). Specifically, the TRM approach accomplishes these tasks via three central phases: Atone, Attune, and Attach. The initial phase, atonement, focuses on helping the UP get answers to questions about the betrayal, express their hurt feelings, and hear true sorrow from the IP. Next, in the attunement phase, the couple deals with the problems in the relationship that preceded the betrayal and work to rebuild a stronger relationship. Lastly, the third phase, attachment, is designed to help the couple rebuild trust and re-attach in positive, loving ways. We expand on this treatment method in the discussion section of this paper.
Data Analysis
We analyzed and interpreted the data gathered for this validation study in the following manner. First, we analyzed couples’ GC assessment data using multivariate analysis of variance (MANOVA), parametric, and correlational analyses. We also used follow-up univariate analysis of variance procedures to compare the effectiveness of the CGT group versus the comparison (TAU) group. Table 1 shows the means (M) and standard deviations (SD) of the IPs and UPs. In addition, we investigated the data for anomalies (normality, heterogeneity), also examining group-level differences (i.e., gender) and utilizing correlations to determine any patterns of association or relationship among the target variables. Given the directional nature of the hypotheses for this article, correction for familywise error rates was not included. All alpha levels were set to .05. We review these findings in the results section.
Means and Standard Errors for Gottman Connect Scales Involved Partners between CGT and TAU over Time.
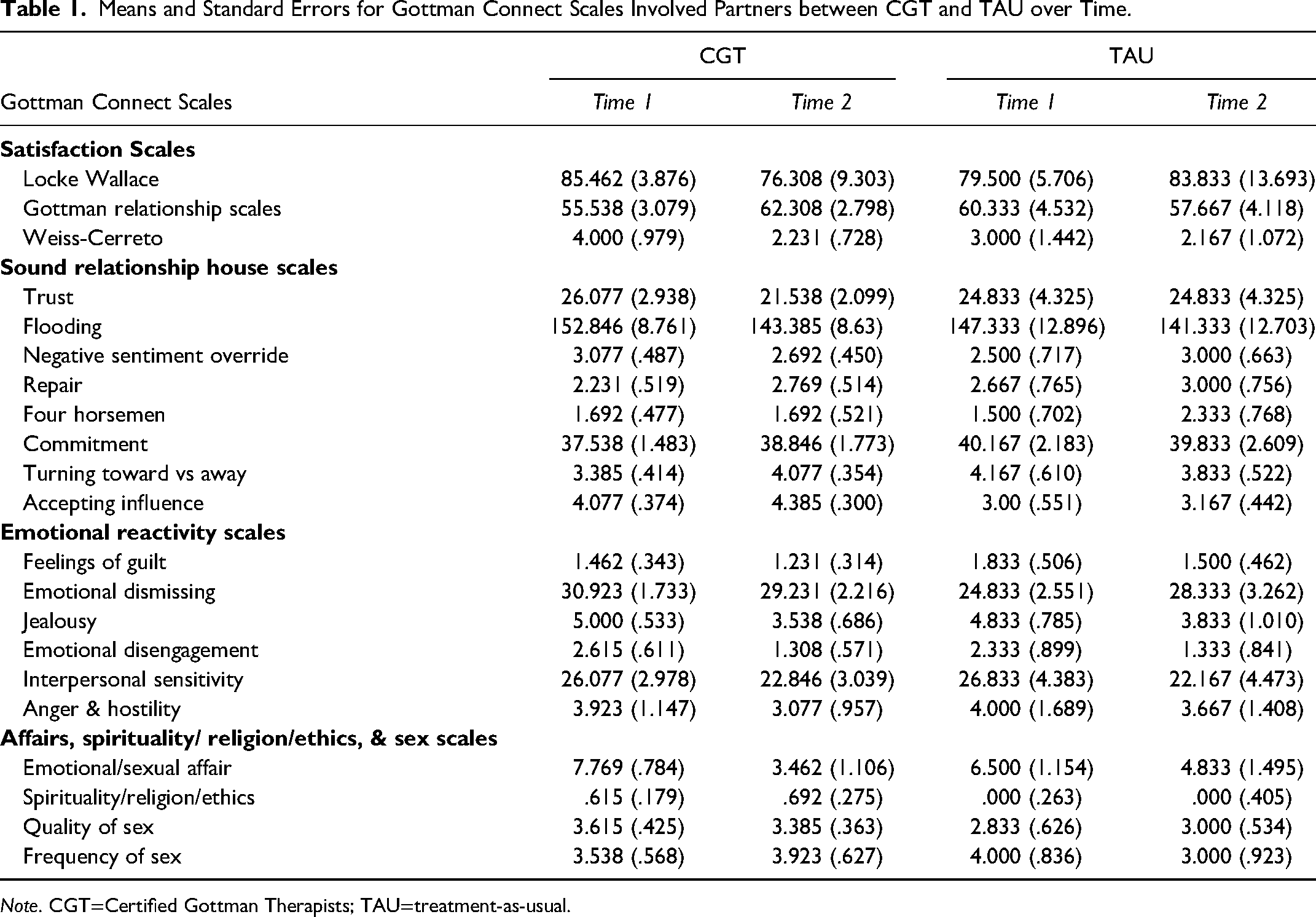
Note. CGT=Certified Gottman Therapists; TAU=treatment-as-usual.
Results
Satisfaction
We used the following three satisfaction measures embedded within the GC assessment tool as the dependent variables in this study: the Lock-Wallace Relationship Adjustment Test (LW), Gottman Relationship Satisfaction Inventory (GRS), and the Weiss-Cerreto Relationship Status Inventory (WC). Next, we assessed for significant group-level differences, using the treatment group (CGT vs. TAU) as the between-subjects variable. Since there were multiple administrations of these scales (pre-treatment and post-treatment), two separate repeated measures MANOVA analyses were employed (one for IPs and one for UPs).
For IPs, there was a significant main effect for the treatment group (Wilks’ λ = .569, F (3, 15) = 3.780, p = 0.033, η2 = .431). Using the guidelines for partial eta squared outlined by Cohen (1988), 0.01 for a small effect size, 0.06 for a medium effect size, and 0.14 for a large effect size, the effect size reported here is considered large. In addition, follow-up pairwise comparisons revealed a significant difference between CGT and TAU on the GRS (MD = 6.769, SE = 2.773, p = .026). As shown in Figure 1, GRS scores for CGT couples increased from 55.5 to 62.3, compared to TAU couples whose GRS scores decreased from 60.3 to 57.6 (see Table 1).
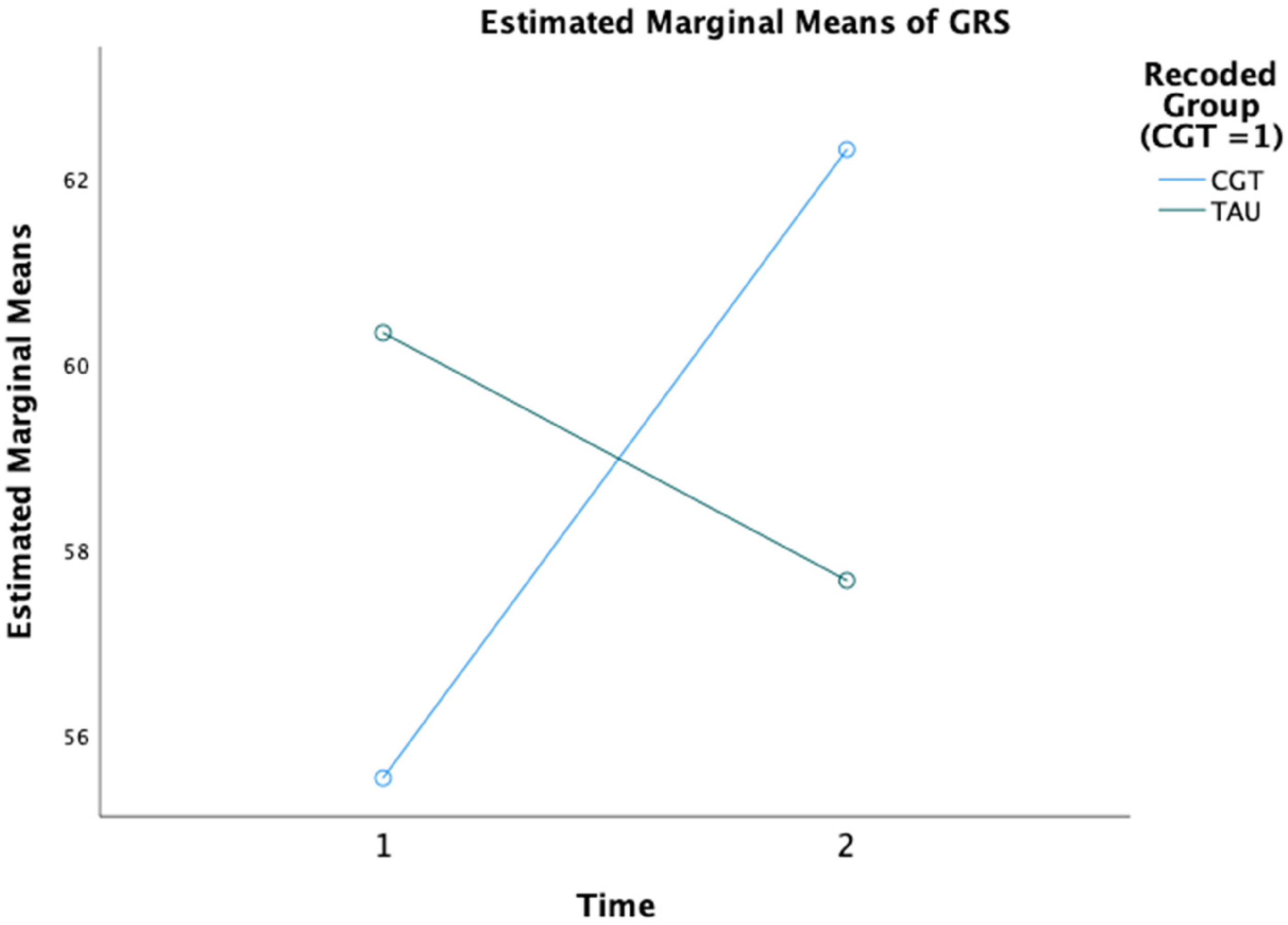
Estimated marginal means of GRS. GRS=Gottman Relationship Satisfaction Inventory.
The analysis for UPs approached significance for the treatment group (Wilks’ λ = .620, F (3, 15) = 3.258, p = 0.061, η2 = .630). While the main effect was not significant, the large effect size suggested a need for additional examination. The follow-up pairwise comparisons revealed a significant difference between CGT and TAU couples on the WC (MD = 2.9, SE = 0.943, p = .006). As shown in Figure 2, the scores on the WC (a measure of separation-proneness) for CGT couples significantly decreased (from 6.2 to 3.3) following treatment compared to TAU couples whose WC scores were not significant, decreasing only from 3.7 to 3.2 (see Table 2).
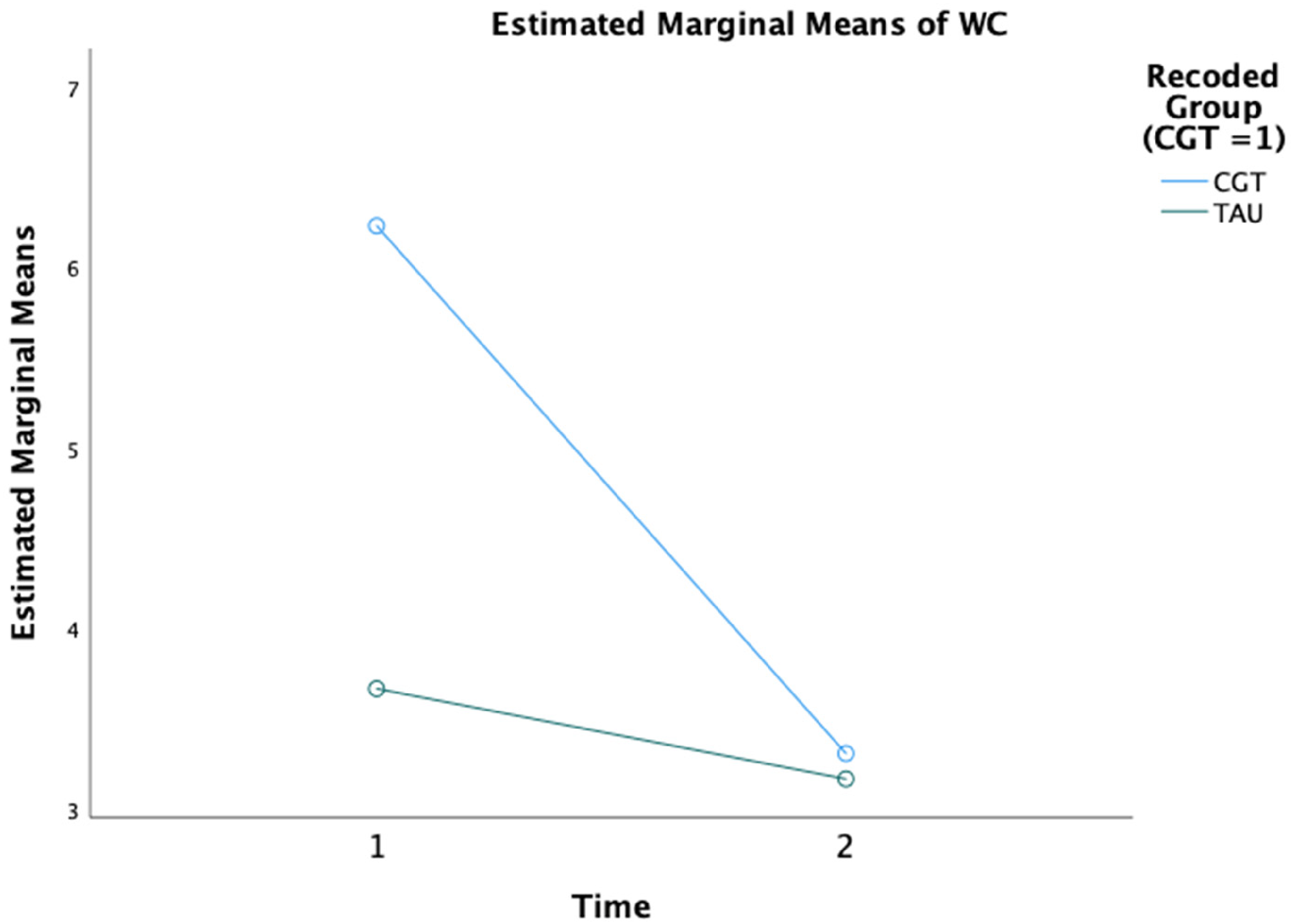
Estimated marginal means of WC. WC=Weiss-Cerreto Relationship Status Inventory
Means and Standard Errors for Gottman Connect Scales of Uninvolved Partners between CGT and TAU over Time.
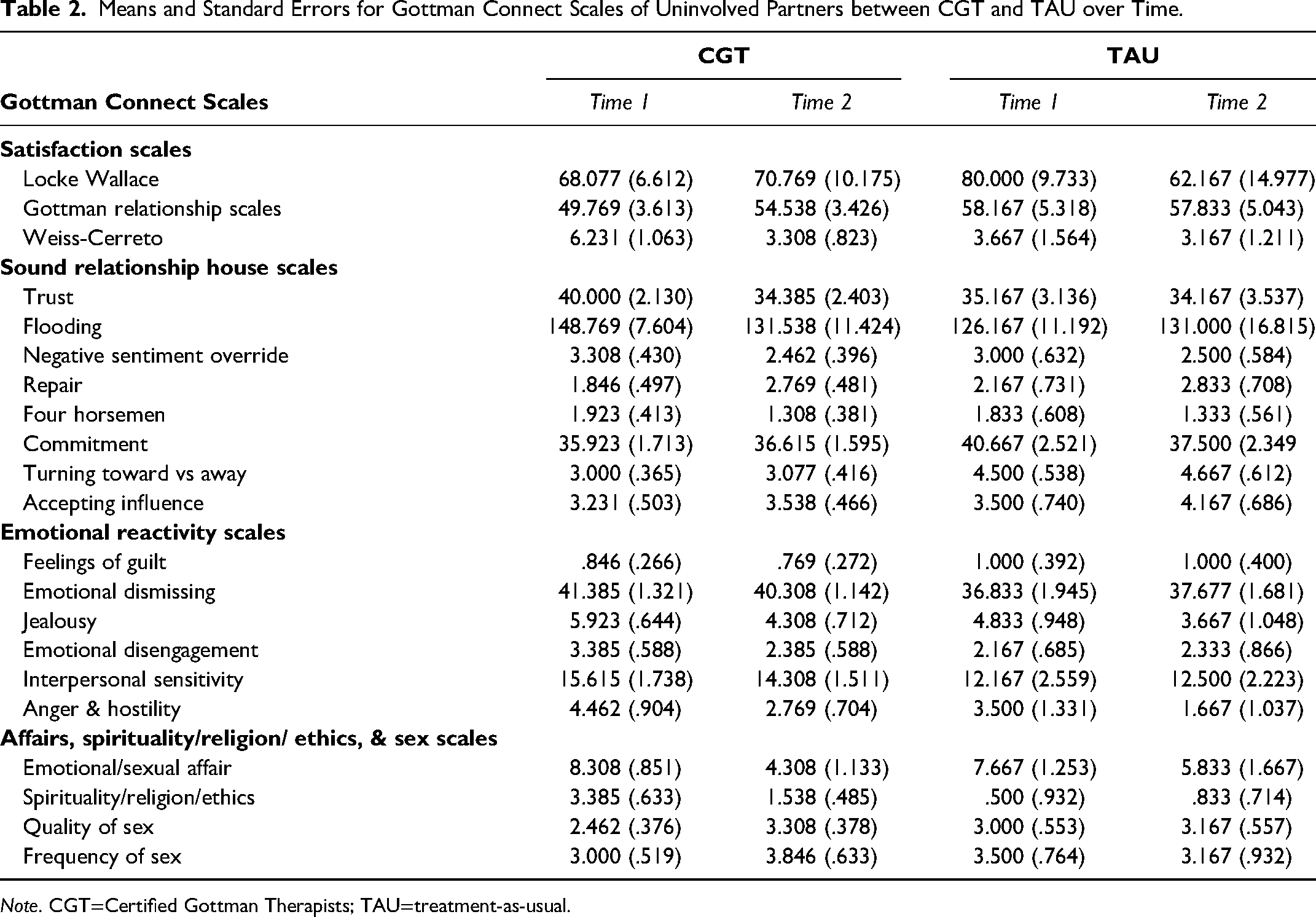
Note. CGT=Certified Gottman Therapists; TAU=treatment-as-usual.
Results of the Gottman Connect Assessment Tool Scales
Next, we investigated responses from other scales embedded within the GC assessment tool. Again, a repeated measures MANOVA was used with time as the repeated measure, scales on the GC assessment tool as the dependent variable, and treatment group (CGT vs. TAU) as the between-subjects variable. Due to the grouping of scales in GC, we conducted four separate analyses for IPs and UPs (see Tables 1 and 2 for the means and standard errors for IPs and UPs, respectively 1 ).
Sound relationship house scales
Emotional reactivity scales
Emotional and sexual affairs, spirituality/religion/ethics, and frequency/quality of sex
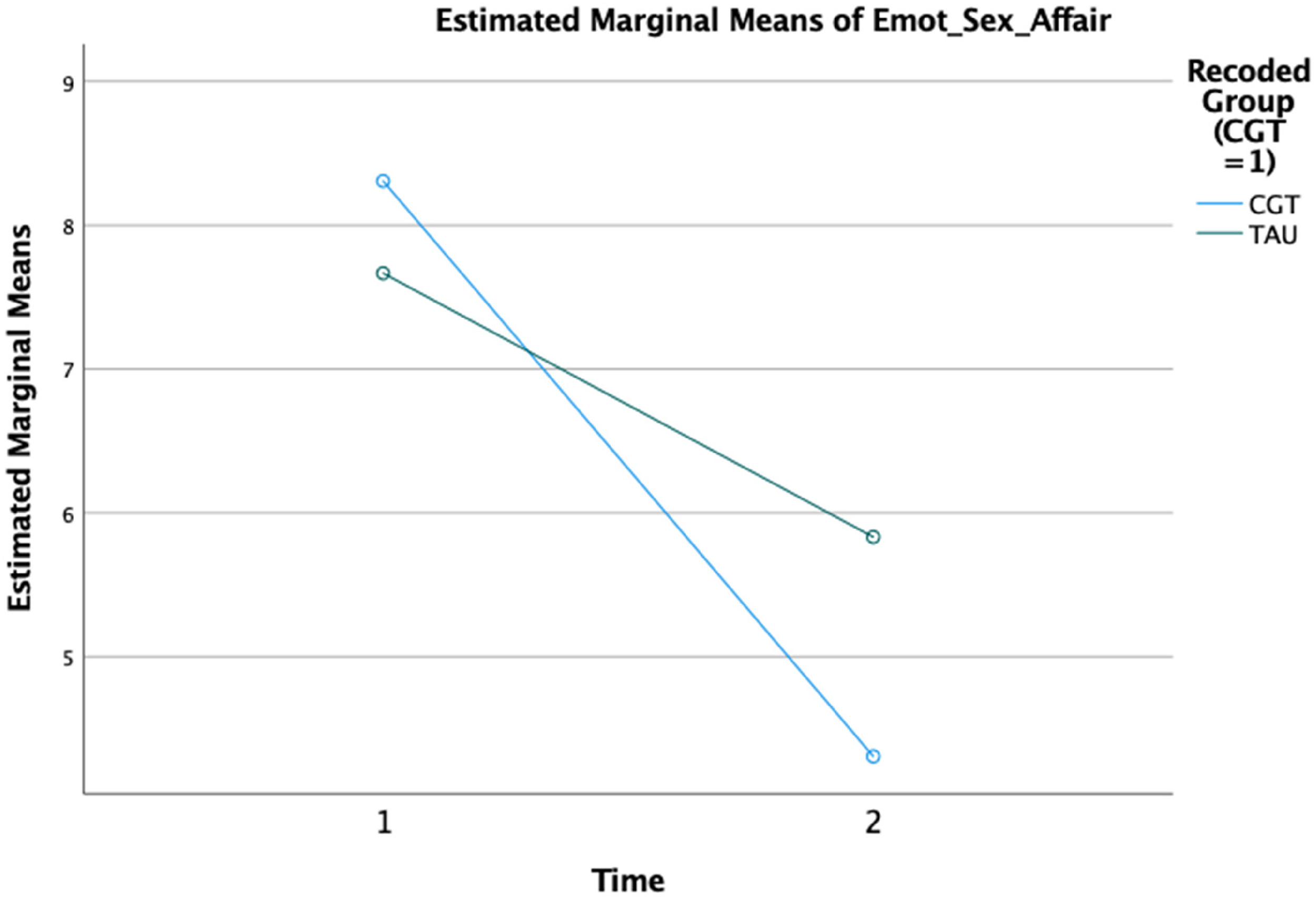
Estimated marginal means of Emot_Sex_Affair.
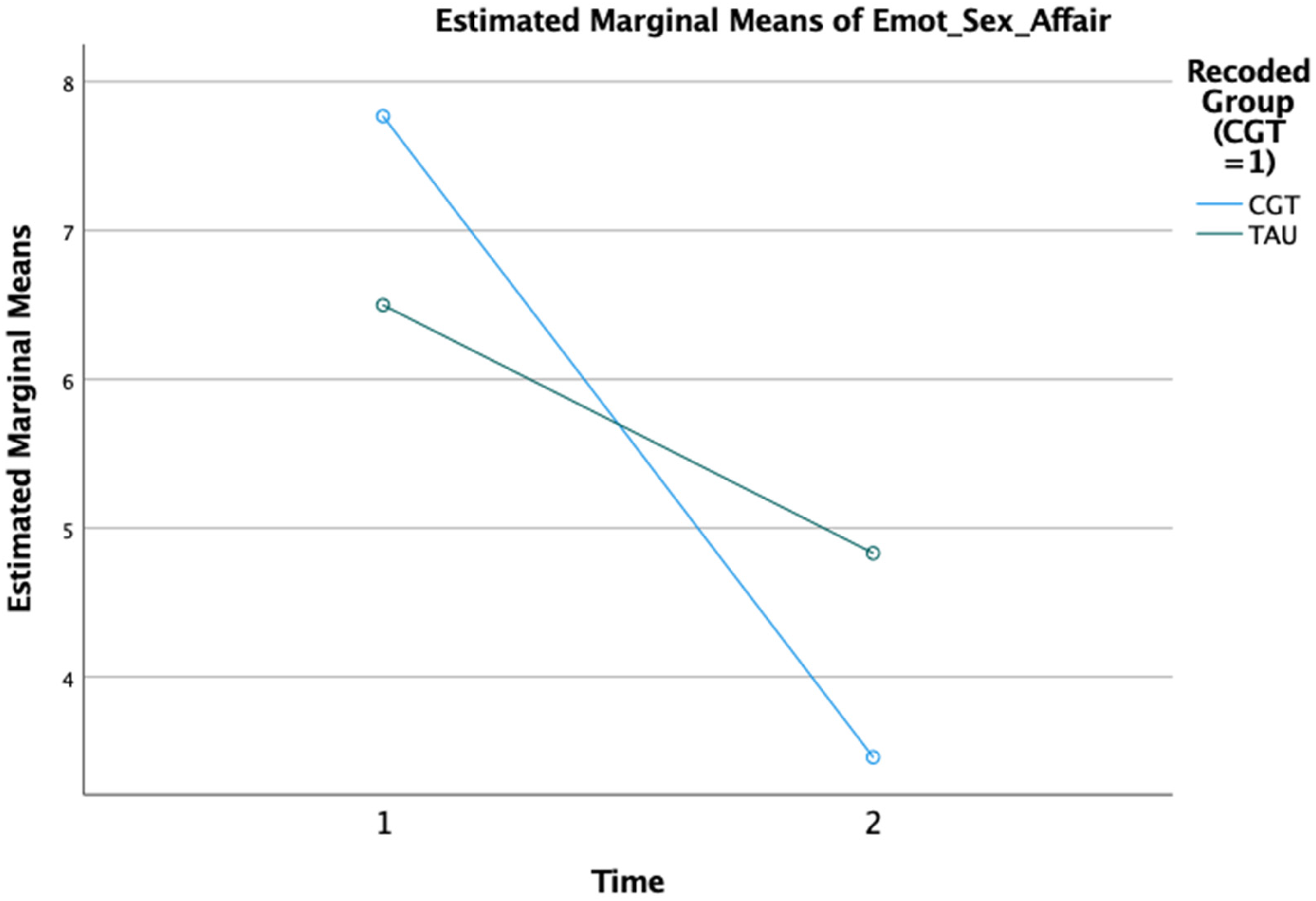
Estimated marginal means of Emot_Sex_Affair.
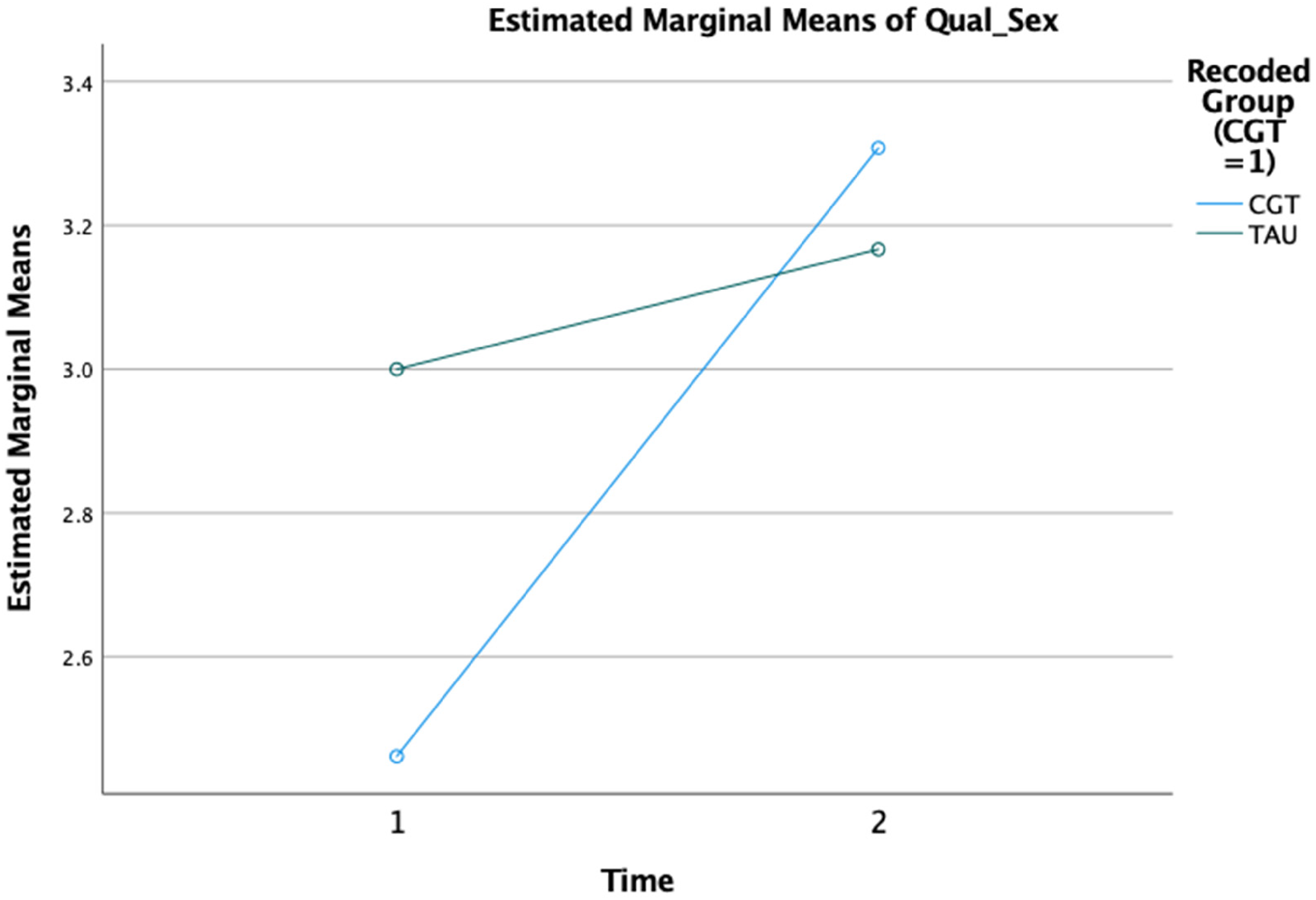
Estimated marginal means of Qual_Sex.
Results of the SPAFF Analysis
Couples’ conflict discussion tapes were analyzed, comparing their pre- and post-treatment conflict discussions. First, we compared the total percentage of time spent in the following codes for IPs and UPs (positive, negative, four horsemen, and neutral), using treatment group as the between-subjects variable. We review these results below.
Involved partners
For IPs, there was a significant overall interaction between time and treatment group (Wilks’ λ = .500, F(3, 12) = 4.00, p = 0.035, η2 = .5000. Follow-up analyses revealed that the total percentage of time in the positive SPAFF codes was significant (F(1, 14) = 4.744, p = 0.047, η2 = .253). Overall, IPs in the CGT group were positive 11.5% of the time compared to 6% for TAU. As shown in Figure 6, CGT IPs were positive 15.8% of the time during the second conflict discussion, while TAU IPs were positive only 4.2% of the time. Furthermore, IPs in the CGT group nearly doubled from the first conflict discussion to the second (7.2% vs. 15.8%), though this result only approached significance (p = 0.063). However, since it did have a large effect size (η2 = .443), we felt it was worth reporting. At the same time, the overall percentage of time IPs in the TAU group spent in positive SPAFF codes decreased from the first conflict discussion to the second conflict discussion (see Table 3).
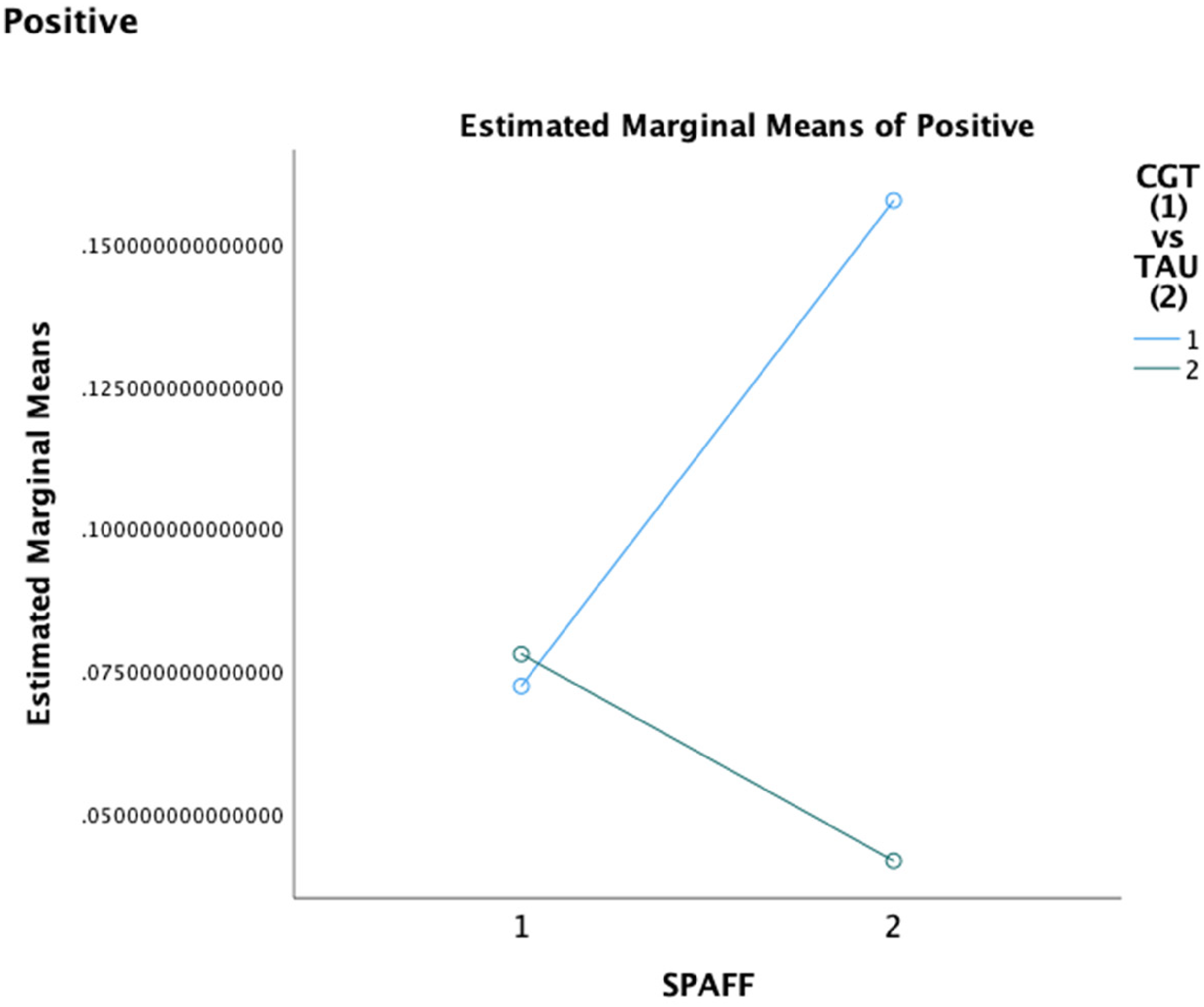
Estimated marginal means of positive.
Means and Standard Errors for SPAFF Codes Involved Partners between CGT and TAU over Time.
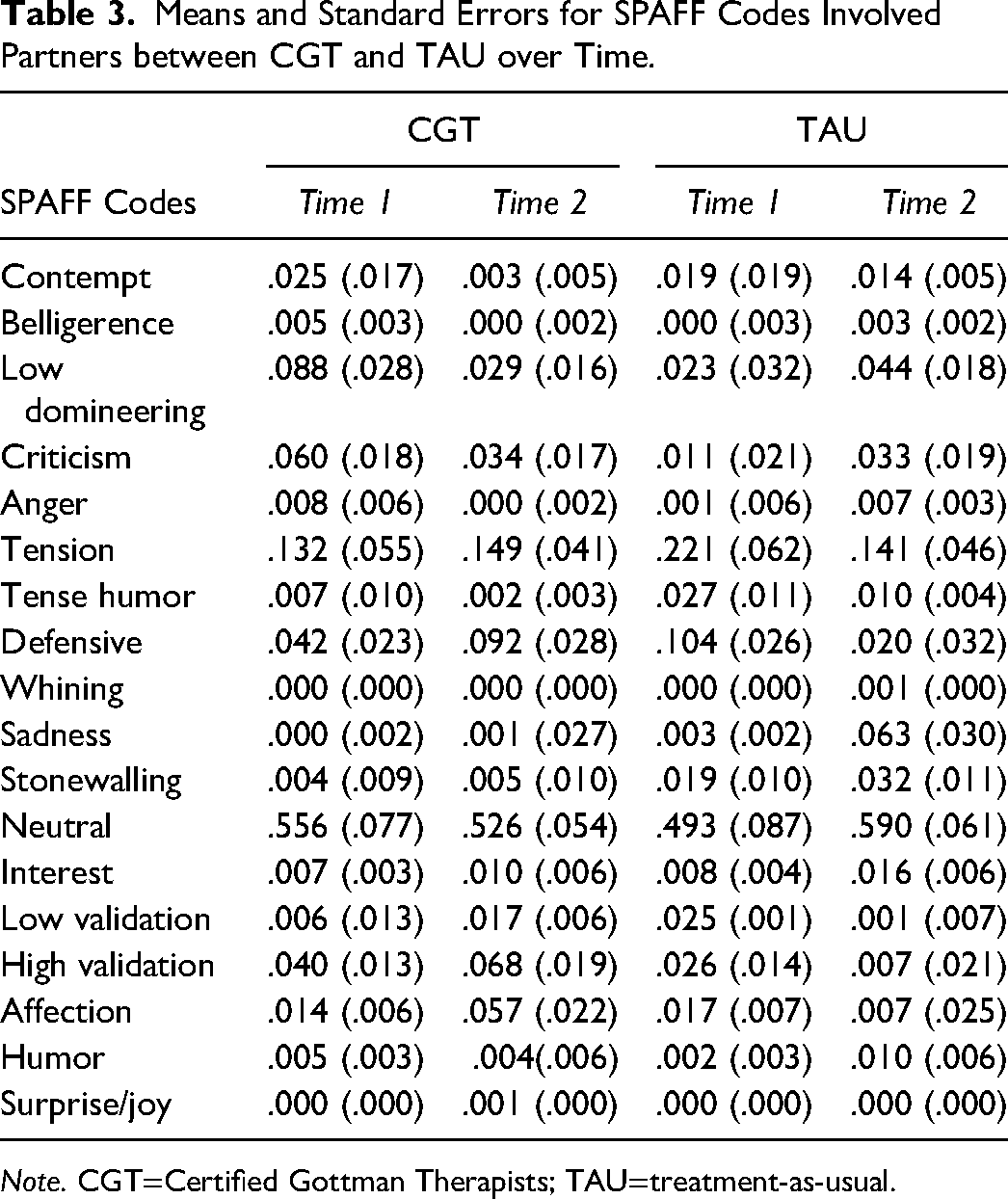
Note. CGT=Certified Gottman Therapists; TAU=treatment-as-usual.
In an analysis of the specific SPAFF codes, there were no significant main effects for either time or treatment group for any of the individual negative SPAFF codes. However, there was a significant interaction of time by treatment group for the negative SPAFF code of defensiveness (F (1, 14) = 5.242, p = .038, η2 = .272). For IPs in the CGT Group, the percentage of time in defensiveness rose from approximately 4% to almost 10%. At the same time, the percentage of time in defensiveness decreased for IPs in the TAU group from almost 10% to approximately 2%.
Just as with the negative individual SPAFF scores, there were no overall main effects for either time of treatment groups. However, high validation approached significance (F (1.14) = 4.273, p = 0.058, η2 = .234) overall by treatment group and was significantly different between the treatment groups during the second conflict discussion (F(1, 14)= 4.572, p < .05, η2 = .246). As shown in Figure 7, IPs in the CGT group showed high validation 7% of the time in the second conflict discussion, while those in the TAU group showed high validation less than 1% of the time.
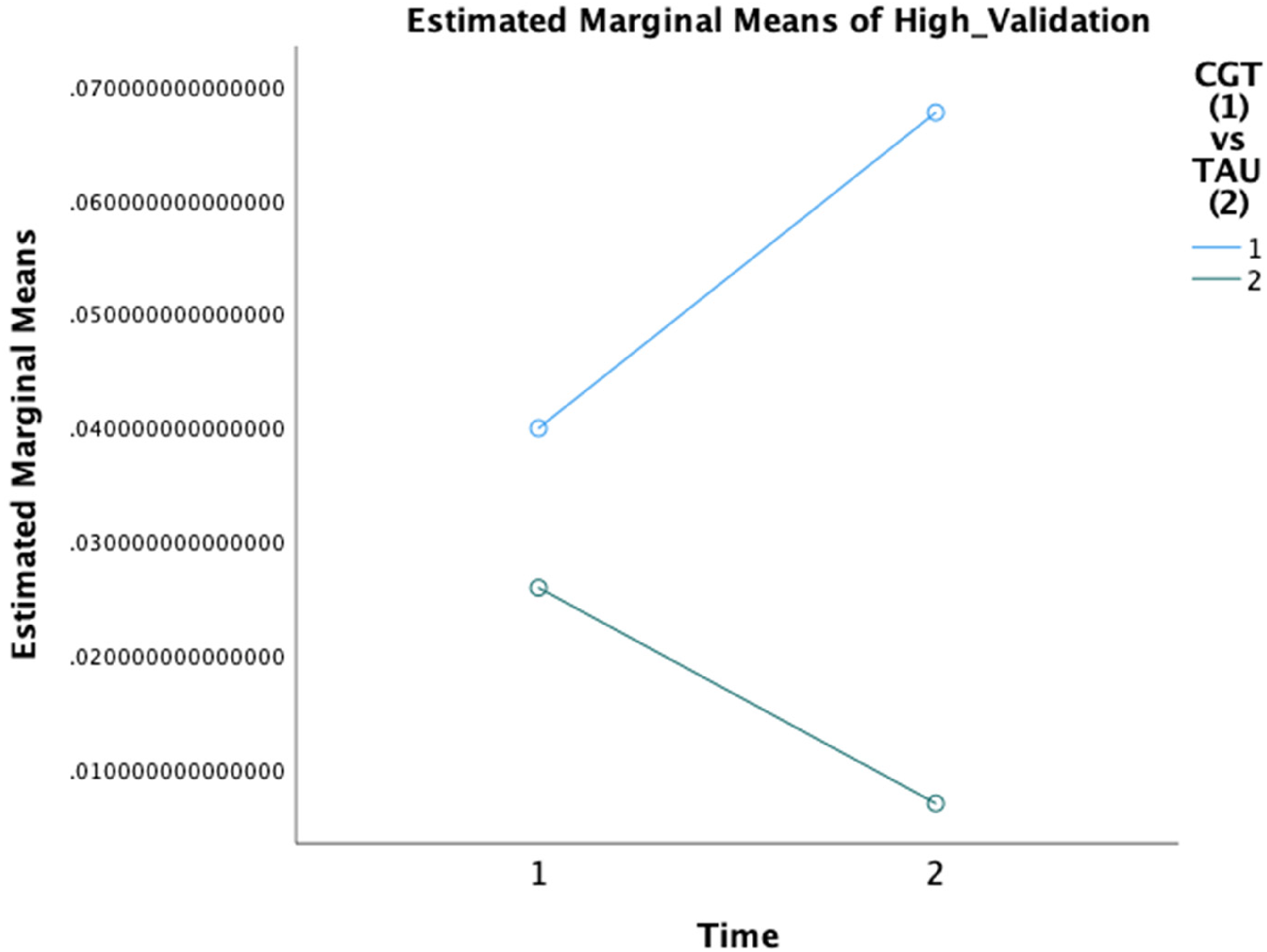
Estimated marginal means of High_Validation.
Uninvolved partners
In the initial analysis of total positive scores, there was a significant overall multivariate effect for treatment group (Wilks’ λ = .389, F(3, 12) = 6.289, p = .008, η2 = .611), but not for time. A separate analysis for all the negative SPAFF codes showed a significant overall interaction between time and treatment group (Wilks’ λ = 0.022, F(12, 3) = 11.241, p = 0.35, η2 = .978). Overall, UPs in the CGT group were negative 33.5% of the time, as compared to 46.2% of UPs in the TAU group. In addition, there was a significant difference in stonewalling from the first conflict discussion to the second conflict discussion for UPs in the CGT group only. Specifically, their stonewalling percentages decreased from 4.5% to 0.1%. By comparison, UPs in the TAU group did not show any stonewalling in either conflict discussion tape (see Table 4).
Means and Standard Errors for SPAFF Codes of Uninvolved Partners between CGT and TAU over Time.
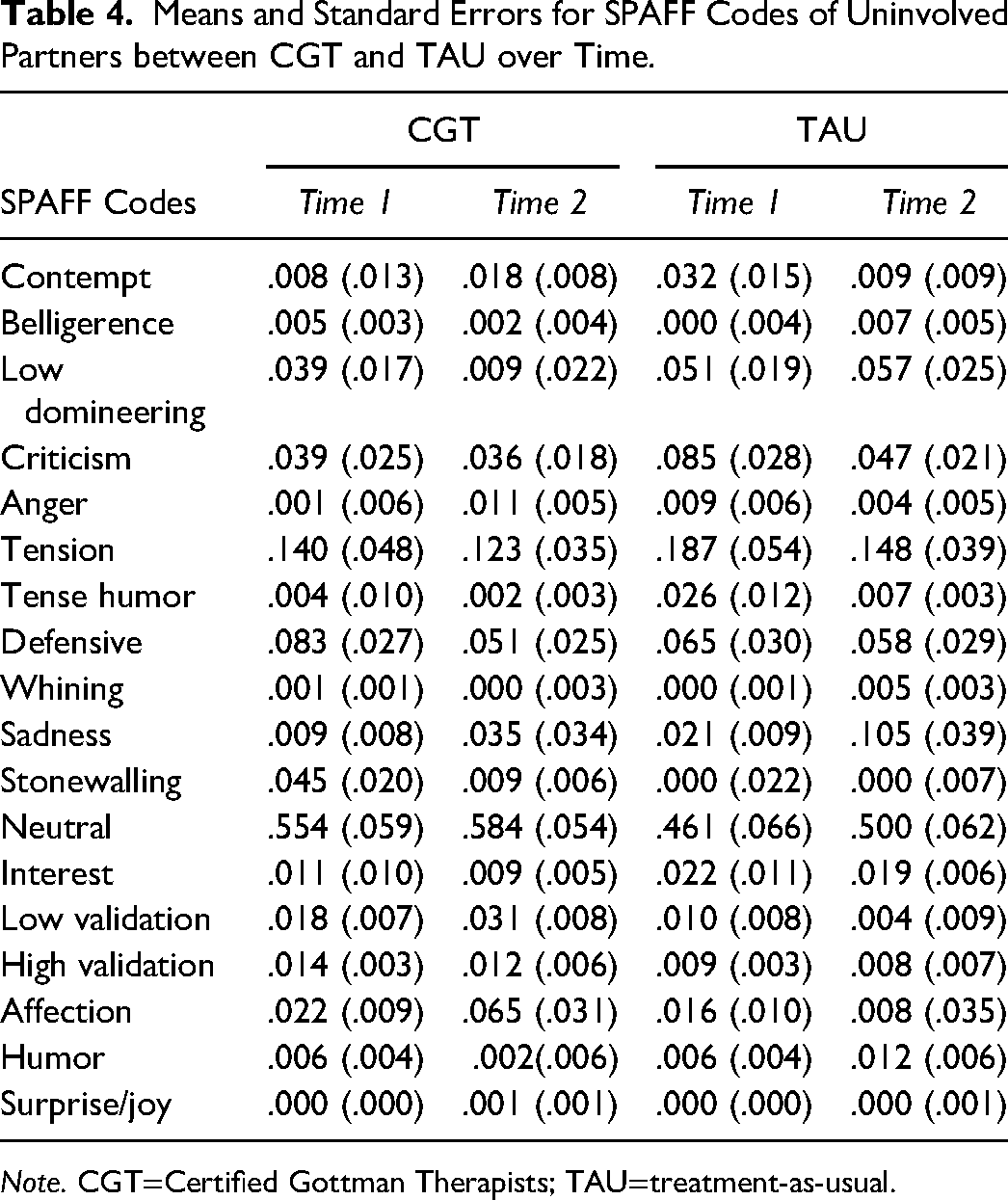
Note. CGT=Certified Gottman Therapists; TAU=treatment-as-usual.
Finally, in investigating the individual positive SPAFF scores, low validation was significantly different between the treatment groups (F(1, 14) = 6.552, p = 0.23, η2 = .319), with UPs in the CGT group expressing low validation 2.4% of the time compared to 0.7% of the time for TAU, overall. Furthermore, in the second conflict discussion, UPs in the CGT group showed low validation 3.1% of the time, while in the TAU group, the scores decreased from 1.0% to 0.4%.
Discussion
Infidelity is a common and distressing issue in couple therapy, with considerable negative consequences for relationships and individuals. However, according to Irvine and Peluso (2022), a significant number of couple therapists do not feel equipped to handle cases of infidelity because their graduate training coursework did not cover this topic, and even though they work with couples who have experienced infidelity, many therapists do not seek out additional specialized training. Additionally, inadequate efficacy and effectiveness research on treating infidelity in couples therapy highlights the necessity for effective interventions to train therapists and support couples seeking to recover from this relational trauma (Irvine & Peluso, 2022; Softas-Nall et al., 2008).
The current study examined the effectiveness of GMCT versus broad-based, TAU approaches in improving couples’ relationships in the aftermath of infidelity. Although the results of this study provide evidence that TAU approaches show some efficacy in helping couples to heal from infidelity, GMCT demonstrated more statistically significant outcomes, suggesting that this is a more effective approach. In addition, our findings showed that GMCT significantly improved relationship satisfaction for both the IP and the UP. Specifically, the GMCT group showed a significant improvement in GRS scores for the IPs, while the UPs showed a significant reduction in separation-proneness (as measured by the WC), compared to the TAU group. These results are consistent with previous research that has demonstrated the effectiveness of couple therapy in improving relationship satisfaction and reducing separation-proneness (Atkins et al., 2005b; Gordon et al., 2004; Greenberg et al., 2010; Marín et al., 2014).
In addition to the above results, our study also examined the effect of treatment on various dimensions of a couple's relationship. The Sound Relationship House scales were used to assess dimensions of relationships, such as trust, repair attempts, four horsemen, etc. The GMCT group had significant improvements in trust for both the IPs and UPs, indicating effective trust revival using Gottman and Gottman's (2017) TRM, otherwise known as the Atone-Attune-Attach protocol (Gottman & Silver, 2013). The Atone-Attune-Attach protocol guides the couple's therapist in supporting healing in three stages. A pilot study on the TRM concluded that this protocol had statistically significant effects on trust, commitment, turning towards, and accepting influence in the aftermath of infidelity, as evidenced by the comparison of pre- and post-treatment GC assessments and enhanced SPAFF coding affect scores for couples who completed treatment (Irvine, 2022). This paper adds more evidence to the effectiveness of the TRM approach and a specific protocol in treating infidelity.
Atonement
The first stage of the TRM model is atonement. During the atonement phase, the IP atones for the betrayal and hurt the UP has experienced by confessing the betrayal, demonstrating transparency by answering questions posed by the UP about the betrayal, offering (initially) verification behaviors, and apologizing/expressing deep remorse to the UP. The significant decrease in anger and hostility from time 1 to time 2 for UPs in the CGT group indicates an effective atonement phase, signaling that IPs validated UPs’ hurt by the betrayal. This finding may be further enhanced by a significant increase in the repair attempt scores for the IP, suggesting more effective repairs and apologies for the relationship. The WC and SPAFF coding findings add to this evidence, showcasing a significant decrease in separating thoughts and stonewalling behavior from the IP for the CGT group. In addition, Gottman and Silver (2013) state that stonewalling is harmful in relationship conflict because it shuts down hope of repair and correlates with increased thoughts of separation. These results demonstrate that atonement phase interventions in the CGT group were effective in processing the betrayal and starting the process of rebuilding trust.
Attunement
During the attunement phase, partners explore current and prior challenges in their relationship by continuing to learn communication skills that support rebuilding the relationship (Gottman & Gottman, 2017). Findings showed that attunement interventions used by CGT clinicians yielded significant increases in accepting influence for the IP, a decrease in the Gottman's (1994) Four Horsemen behaviors (i.e., contempt, stonewalling, defensiveness, and criticism) for the UP, and an increase of defensiveness for the IP. This outcome may indicate attempts to assert oneself rather than be silent about relational challenges.
Another component of the attunement phase, accepting influence, was not statistically significant for couples in the CGT group; conversely, this domain was statistically significant in the TAU group but for UPs only. Despite the nonsignificant results in the GC assessment score, UPs in the CGT group still exhibited accepting influence, as evidenced by a significant decrease in the Four Horsemen behaviors, notably stonewalling, as well as a significant increase in low validation; among the CGT group, this result indicates improvement in UPs’ conflict management, which requires the ability to accept influence, repair, and negotiate compromises (Gottman & Gottman, 2017).
It was also interesting that turning towards versus away scale was significantly higher for UPs in the TAU group compared to the CGT group at both the first and second administrations. This outcome may be explained as some models, such as emotion-focused therapy, focuses on having couples turn toward one another using enactments (Johnson, 2019). For this domain, the small sample size may have also contributed to the lack of significant findings for CGT couples since UPs in the CGT group still turned towards the IP, as evident in the decreased stonewalling and increased low validation behaviors. The GC and SPAFF codes reported above highlight the efficacy of the attunement phase.
Attachment
The attachment phase aims to strengthen intimate trust and loyalty between partners by intentionally cherishing each other, developing rituals of connection, deepening shared meaning, and renewing or strengthening the sexual relationship, to foster lasting commitment (Gottman & Gottman, 2017). The consequences of further betrayals are also outlined to increase commitment. Evidence of the effectiveness of the attachment phase can be seen in the significant decrease in the emotional and sexual affair scores for both the IP's and UP's assessment scores for the CGT group. The emotional disengagement of IPs also decreased, indicating a greater emotional connection in the relationship. Further, the decreased emotional engagement and jealousy scores for IPs in the CGT group indicate a reduced attraction to alternative romantic or sexual partners and insecurity.
Renewing the sexual relationship is a key and effective part of this phase, as demonstrated by the significant increase in the quality of sex for the UP in the CGT group. Additionally, there was a significant decrease in spiritual, religious, and ethical conflicts in the GC scores for UPs in the CGT group, highlighting how exploring shared meaning can enhance a couple's spiritual and ethical connection, deepening commitment and loyalty. Finally, the positive SPAFF ratings for IPs in the CGT group doubled from time 1 to time 2. Increased displays of positive affect codes among couples serve as a preventive measure in protecting the relationship from future betrayals (Gottman, 1994). In addition, positive codes indicate cherishing one's partner, which is crucial in safeguarding the relationship from the cascade toward betrayal (Gottman & Silver, 2013). This study's results demonstrate that the attachment phase of the TRM positively changes aspects of the relationship so that commitment and connection can become buffers from considering alternative partners or relationships.
Contributions of the study
While the broad-based TAU group helped support a couple in repairing the relationship in the aftermath of an affair, the CGT group, using the TRM, proved more effective in significantly improving key variables in couples’ relationships such as trust, repair, emotional connection, quality of sex, and positive affect; these components are necessary for repairing and rebuilding a relationship following a traumatic betrayal such as infidelity (Gottman & Gottman, 2017). This study contributes to the infidelity literature by adding another infidelity-focused RCT and validating GMCT as a framework for clinicians to support couples in affair recovery.
Implications for Counseling, Training, and Research
This study highlights specific needs for specialized couples counseling, therapist training, and research. Couples who present in therapy with infidelity are often in crisis and therefore have a unique set of presenting problems that need to be addressed. Infidelity has been cited as one of the most frequent and challenging presenting issues among couple practitioners (Glass & Wright, 1992; Irvine & Peluso, 2022; Softas-Nall et al., 2008; Vossler & Moller, 2014; Whisman et al., 1997), and yet therapists who treat couples often have not had any specialized training in its treatment. The results indicate that the therapists who had specialized training to treat infidelity had a significant impact on the couples’ recovery. The results also offer some insight into what may go wrong in couples therapy. Traditional couples therapy may not address all of the phases required in the recovery process of infidelity. For example, some therapists may not ask the couple to have an atonement conversation. Other therapists may not recognize that the betrayal has created PTSD symptoms within the betrayed partner. Therefore, therapists who intend to work with couples should seek advanced and empirically validated treatment modalities beyond their training program to learn how to treat infidelity as well as other couple comorbidities.
Another implication of this study is to call for therapist training programs to expand their curriculum to include effective treatment modalities for infidelity in couple relationships since therapists who treat couples often do not feel educationally equipped to address the specific challenges of infidelity (Irvine & Peluso, 2022). The couples who made significant improvements were those who worked with therapists trained in the TRM. Training programs that focus on infidelity should address the couple's need to appropriately atone for the betrayal, manage PTSD symptoms, help the couple emotionally attune to one another, develop communication skills to effectively manage conflict, and rebuild their relationship. These components help rebuild intimate trust and attachment to one another (Gottman & Gottman, 2017).
The third implication of the current study calls for more robust research studies on infidelity. The number of RCT studies available on the treatment of infidelity was limited. The fact that there are so few studies highlight the challenge of recruiting couples to participate in RCT research. Couples tend to be reluctant to share sensitive information about intimate parts of their relationships, especially when there has been infidelity; this also contributed to a less diverse group sample. Specifically, the participants recruited in the current study were a homogeneous group (i.e., they were mostly heterosexual, Non-Hispanic White, and married). Future studies on the treatment of infidelity could be more inclusive of race/ethnicity, sexual diversity, and relationship status.
Another implication for research would be to be more inclusive of therapists who use other treatment modalities. Seventeen of the therapists in the current study were trained in GMCT. The TAU therapists used a wide variety of treatment methods but were compared as a single method. However, the TAU therapists used different approaches, including eclectic/ integrative therapy, emotionally focused therapy, psychodynamic therapy, systems-based therapy, and trauma-informed therapy. Some of these treatment methods may be more effective in treating infidelity than others. Additional studies could include an equal number of therapists per treatment method to determine if other methods are equally effective.
Limitations and directions for future research
Limitations
One notable limitation of this study is the small sample size, which may have limited our statistical power and generalizability of the findings. A larger sample size and a more diverse participant pool, including non-English speaking couples and lower socioeconomic couples, would increase the validity of GMCT's TRM approach. Additionally, the lack of a control group that received no treatment makes it difficult to rule out placebo effects or other extraneous factors that may have influenced the results (Irvine, 2022). Future studies should include a larger and more diverse sample, as well as a control group, to address these limitations.
Furthermore, this study was constrained by the limited number of available CGT clinicians. Specifically, due to the extensive requirements for certification in GMCT, there were currently fewer than 400 fully trained CGTs during the study period; further, only about 90 of the 400 had completed the necessary training required to carry out the TRM affair recovery intervention in this study. Consequently, the available sample size of CGTs was considerably limited. In addition, these therapists also have extensive training in couples therapy, which may not reflect the quality and specific training of other therapists who treat couples experiencing infidelity. Finally, the GC assessment tool and SPAFF coding procedure may have lent to more favorable results for the CGT group, given that the GMCT framework was informed by early SPAFF research, and the GC assessment tool comprises measures that are in line with this model (e.g., the Sound Relationship House measures such as trust and the Four Horsemen).
Directions for Future Research
Some suggestions about future research can be offered based on the results of the current study. Considering the limitations described earlier, this study could be replicated to include a larger sample size of participants, a more diverse population, and a larger pool of therapists. A major difficulty in research is finding participants. Couples who struggle with infidelity are often reluctant to expose their relationships to scrutiny, so expanding the sample size can be a challenge. However, the generalizability of the effectiveness of treatment relies on the inclusion of more participants. The participants in the current study were mostly Non-Hispanic White, heterosexual, married couples. Therefore, a more diverse sample, including more diversity in ethnicity/race, relationship status, and sexual orientation, is needed in future research. Likewise, a larger pool of therapists would be important for future research. Recruiting therapists from different theoretical orientations would also help understand the effectiveness of different treatment modalities for infidelity. However, like couples, therapists are also reluctant to have their work scrutinized, so therapist recruitment may also present a challenge in research.
Conclusion
In conclusion, our findings provide promising evidence that GMCT is an effective intervention for improving the relationship in the aftermath of infidelity. The results of this study highlight the importance of addressing communication skills in the context of infidelity and the potential benefits of using GMCT to achieve this goal. Further research is needed to replicate these findings in larger and more diverse samples, exploring the long-term effects of GMCT on relationship outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.