
Abstract
The aim of this study is the relationship between psychological variables and adjustment to the disease in patients and their primary family caregivers to analyze the possible existence of emotional contagion between them. A total of 150 caregiver–patient dyads participated. The results indicate higher levels of anxious-depressive symptomatology in the caregiver than in the patient. The caregiver's presence of anxiety and depression is related to lower scores in quality of life, self-esteem, and a more significant perceived threat of illness. The caregivers’ emotional adjustment is predicted by their own variables (stress, need for approval and hostile conflict resolution) and by those of the patient (self-esteem, threat of illness and quality of life). In the patient's case, their adjustment was mainly explained by their own variables and caregiver's perceived stress. Parents and other primary caregivers provide attention, care, and love and can promote a safe environment for emotional adjustment in patients.
Introduction
The family system is a fundamental source of support and affection for children during childhood and adolescence. The family context is vital in the proper development of adolescents in these early stages, and it is also the setting for fundamental aspects of childcare, such as the management and control of asthma (Crandell et al., 2018). The challenges of controlling asthma can put significant pressure on families because of the introduction of additional responsibilities (to the already complex task of parenting) that it often entails. Besides, this can have a negative impact on the mental health and psychological wellbeing of family caregivers (Bhagat et al., 2019; Sonney et al., 2017). It is important to point out that the level of overload experienced by a family, together with the type of communicative and emotional climate that prevails in family coexistence, is often associated with adherence to children's treatment and their health (Al G Hriwati et al., 2017).
Studies have shown (Barton et al., 2019; Holmbeck, 2018) that family characteristics (such as family cohesion, communication, and organization) are associated with children's mental health. Family routines and functioning dynamics are essential in establishing a suitable adjustment of the adolescent to asthma and help develop better medication adherence, favoring the quality of life of the adolescent (Burg et al., 2018; de Benedictis & Bush, 2017). Like so, adolescents with asthma who participate in family routines often have lower rates of anxiety (Hughes, 2019; Wood et al., 2015).
The demands associated with chronically ill children's regular care can favor the appearance of anxiety-depressive symptoms in parents (Diep et al., 2019; Easter et al., 2015). How parents experience and cope with their children's illness often influences significantly how their children will respond adaptively to their illness (Barton et al., 2019; Wood et al., 2015).
According to studies, in the case of adolescents with chronic diseases, when parents show depressive traits prior to the onset of the disease (Yamamoto & Nagano, 2015), this depressive clinical condition directly influences their parenting style and care patterns (inadequate inhalation techniques, omission of medication doses, and less confidence in the control of the clinical condition) (Oland et al., 2017; Ramratnam et al., 2017), which in turn affects the physical (Weinstein et al., 2019) and psychological state of the adolescent (Kub et al., 2018; Pinquart, 2018).
On the other hand, problems in the adolescent's adjustment to his or her disease are usually associated with increased psychological symptoms in the parent (Chong et al., 2018; Valero-Moreno et al., 2018). Furthermore, the characteristics of the adolescent's health status (such as the severity of the disease and the functional impairment involved) seem to be positively associated with an increase in psychological symptomatology in caregivers (Ramratnam et al., 2017). Literature has found significantly higher rates of symptomatology anxious-depressive in parents of children with severe asthma (Easter et al., 2015; Valero-Moreno et al., 2018).
Therefore, the main aim of this work was to analyze the relationship between psychological variables and adjustment to the disease in pediatric patients with bronchial asthma (BA) and their family caregivers to analyze the possible existence of emotional contagion between them. Based on the objective, the hypotheses posed were H1: It is expected to find a positive association between the presence of anxiety-depressive symptomatology of the primary family caregiver and the adolescent with BA. H2: It is expect to find a positive association between variables related to the emotional wellbeing of the adolescent with BA and the adequate adjustment-adaptation of primary caregivers (emotional contagion).
Methods
Participants
A total of 150 caregiver–patient dyads participated. In adolescents with BA, their ages ranged from 12 to 16 years (M = 13.28; SD = 1.29), with 60.7% being male and 39.3% female. Regarding caregivers, the most common family relationship found was that of the mother of the pediatric patient, with 85% (n = 119), followed by “father” with 15% (n = 21). The primary caregivers’ mean age was 45.43 years (SD = 5.03), the minimum being 27 and the maximum 63.
Design and Procedure
It is a single-pass cross-sectional design. The procedure consisted of identifying all patients with BA who attended pediatric pulmonology consultations at the hospital. Regarding pediatric patients, the inclusion criteria were between 12 and 16 years of age, presenting a bronchial asthma diagnosis at least 6 months ago.
All participants and caregivers who met the inclusion criteria and who also completed the informed consent form and agreed to participate were included in the present study.
The exclusion criterion considering for the adolescents was that despite having a diagnosis of asthma, they had a psychological disorder, cognitive impairment, or epilepsy at the time of the assessment. The present study was approved by the UV-INV_ETICA-1226194 ethics committee.
Instruments and Variables
Patient variables
- Anxious-depressive symptomatology: The Hospital Anxiety and Depression Scale (HADS) (Zigmond & Snaith, 1983) was used to assess emotional adjustment, measured through anxiety-depressive symptomatology (Zigmond & Snaith, 1983). For the adolescent population in the corresponding study (Valero-Moreno et al., 2019), the anxiety scale values were .77, and for the depression scale .61.
- Self-esteem: The Rosenberg Self-Esteem Scale was used (Atienza et al., 2000). The scale consists of 10 items, which refer to thoughts or feelings about the adolescent's own perception of self-esteem. In the original study (Atienza et al., 2000), reliability of .92 was obtained.
- Quality of life: To assess health-related quality of life (symptoms such as dyspnea, fatigue, emotional impact, disease control), the Chronic Respiratory Questionnaire (CRQ) was used (Vigil et al., 2011), in its self-administered version translated into Spanish (Vigil et al., 2011). In the present study, a version adapted and validated for adolescents with chronic respiratory disease was used (9–18 years) was used (Valero-Moreno et al., 2019), showing adequate reliability indices .85 for the total scale.
- Threat of illness: To assess it, it was used to The Brief Illness Perception Questionnaire (Broadbent et al., 2006): This scale measures the patient's self-perceived emotional and cognitive representations of their illness In this study, the reduced and adapted version for an adolescent sample is used (Valero-Moreno et al., 2020). The results of the internal consistency analyses performed indicate good-quality indices (Broadbent et al., 2006; Valero-Moreno et al., 2020). In this work, the reliability was .80.
- Psychological control: The subscale of the Parental Styles questionnaire was used (Oliva et al., 2007). It assesses psychological manipulation strategies such as emotional blackmail or guilt induction. Reliability indices were adequate .86 (Oliva et al., 2007). In the present study, the reliability indices were similar: .85.
Caregiver variables
- Anxious-depressive symptomatology: The HADS (Zigmond & Snaith, 1983) was used in the same scale as in adolescents, but in the adult version. Adequate reliability was obtained for the two subscales: .86 for the anxiety dimension and .78 for the depression dimension.
- Perceived stress: The Pediatric Inventory for Parents was used (Casaña-Granell et al., 2018; del Rincón et al., 2007). It assesses the perceived stress levels of parents caring for a chronically ill adolescent. Adequate reliability coefficients were obtained for the two total subdimensions, 0.78 for the Frequency scale and 0.81 for the Effort scale (Casaña-Granell et al., 2018). In these sample, the reliability indices were .79 and .84, respectively.
- Need for approval and hostile conflict resolution: The Adult Attachment Questionnaire was used (Melero & Cantero, 2008). As for reliability indices, the need for approval scale obtained an index of .86, the hostile resolution a scale of .80. In these sample, the former obtained an index of .85 and the latter an index of .76.
Data Analyses
In order to carry out the corresponding analyses, we first calculated the descriptive analyses of the variables included in the study (mean, standard deviation, minimum, maximum, and the corresponding percentiles). Subsequently, the quali-quantitative comparative analysis (QCA) was carried out. This methodology allows, through the Boolean logit, to identify which series of variables (causal conditions) are associated with the presence of a certain result (outcome condition). This type of analysis makes it possible to arrive at the same result through different paths or combinations (produced by the interaction between the different variables) (Eng & Woodside, 2012; Ragin, 2008). On the other hand, to perform the qualitative fuzzy set comparative analysis, the raw data from the participants’ responses were transformed into fuzzy set responses. First, as suggested in the literature (Ragin, 2008), all missing data were removed, and all constructs (variables) were calculated by multiplying their item scores. Before running the analysis, the values of the analysis should be recalibrated between 0 and 1. However, to recalibrate with more than two values, it must consider the following three thresholds: the first (0) considers an observation with this value to be totally out of the set (low agreement); the second (0.5) considers a midpoint, neither in nor out of the set (intermediate level of agreement); and the last value (1) considers the observation to be totally in the set (high level of agreement) (Lacomba-Trejo et al., 2020; Valero-Moreno et al., 2020; Villanueva et al., 2019).
Results
Descriptive Statistics
Of the adolescents with BA, 86% had controlled asthma for at least the past 6 months, compared to 14% with uncontrolled asthma. Regarding the severity of asthma: 60.4% had persistent-moderate asthma, 32.3% had frequent episodic asthma, 6% had occasional episodic asthma, and 1.3% had severe asthma.
When analyzing the results of anxiety-depressive symptomatology in the patient and caregiver, there is a greater presence of anxious symptomatology than depressive symptomatology in both patients and caregivers. In turn, caregivers presented higher percentages of anxious symptomatology than pediatric patients (42.3% vs. 30.1%), and the same was observed for depressive symptomatology (16.2% vs. 6.2%) (Figure 1).
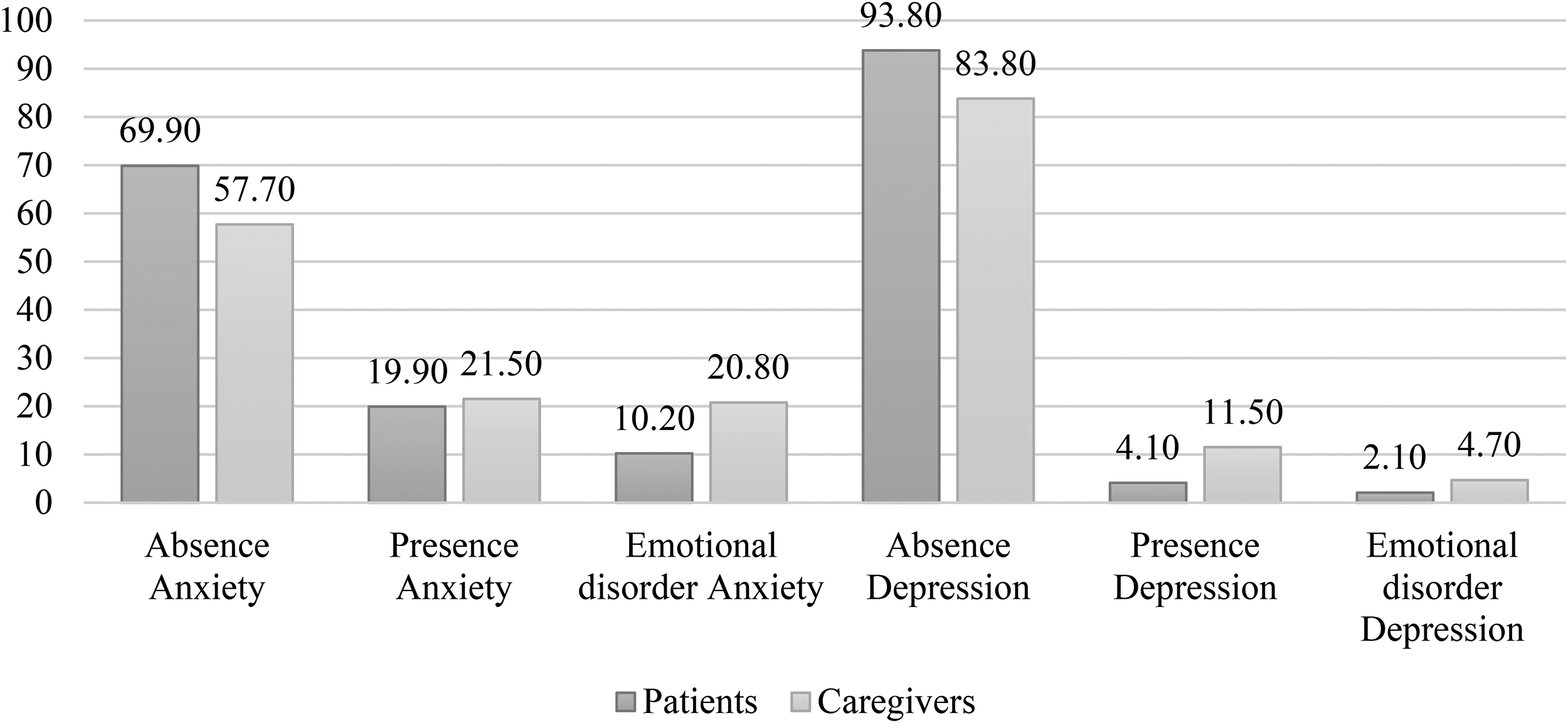
Comparison of percentages of anxiety-depressive symptomatology in the patient and the caregiver.
Comparison of Means
To study how the patient and their family caregiver may influence each other's emotional adjustment, a recording of the HADS scores was performed to analyze whether there were differences in the means of anxiety and depression. For the patient anxiety and depression groups (i.e., the adolescents who presented significant anxious or depressive symptoms), no differences were found in the variables analyzed in the caregiver. On the other hand, for the caregiver anxiety and depression groups, differences were observed in the variables analyzed in the patient. Thus, in caregivers with anxious symptomatology, it was found that their children had worse self-esteem (compared with the children of caregivers with no anxiety). Besides, patients whose caregivers presented a possible psychological disorder due to anxiety showed a greater sense of threat of illness. On the other hand, caregivers with depressive symptomatology were perceived by their children as exercising greater behavioral control (compared to caregivers without depressive symptomatology). If the caregiver's clinical manifestations were of a possible psychological disorder due to depression, this had a very negative impact on their children's quality of life, who showed a poorer quality of life and a significant dyspnea sensation (Table 1).
Difference of Means in Psychological and Family Variables of the Adolescent According to Caregiver Anxiety and Depression Groups.
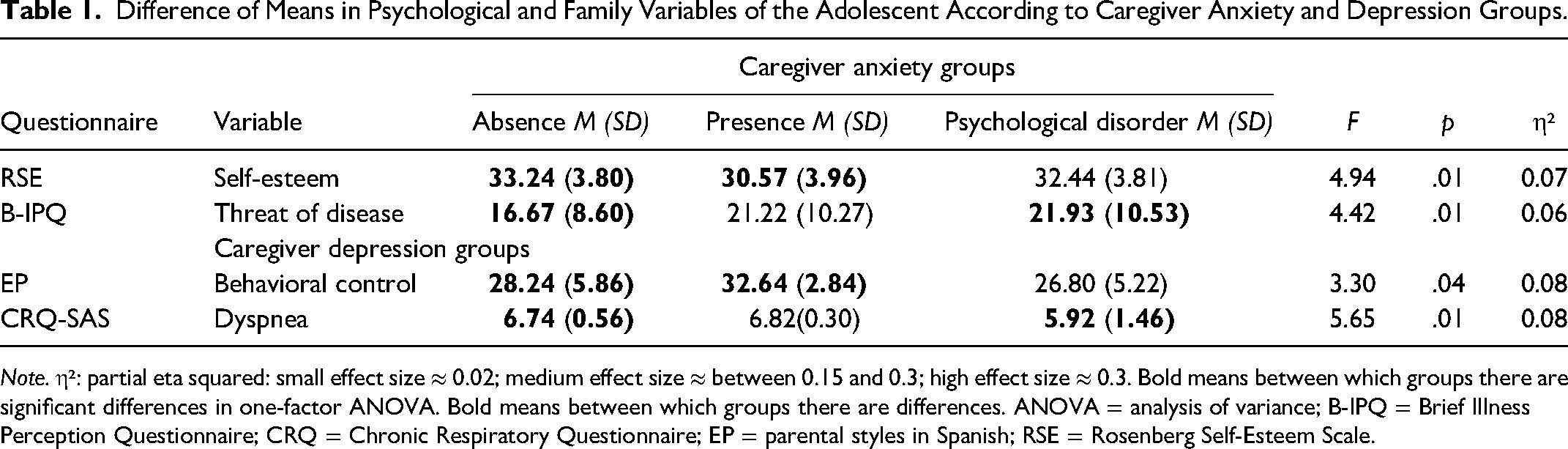
Note. η²: partial eta squared: small effect size ≈ 0.02; medium effect size ≈ between 0.15 and 0.3; high effect size ≈ 0.3. Bold means between which groups there are significant differences in one-factor ANOVA. Bold means between which groups there are differences. ANOVA = analysis of variance; B-IPQ = Brief Illness Perception Questionnaire; CRQ = Chronic Respiratory Questionnaire; EP = parental styles in Spanish; RSE = Rosenberg Self-Esteem Scale.
Correlation Analysis Between Psychological and Family Variables of Patient and Primary Family Caregiver.
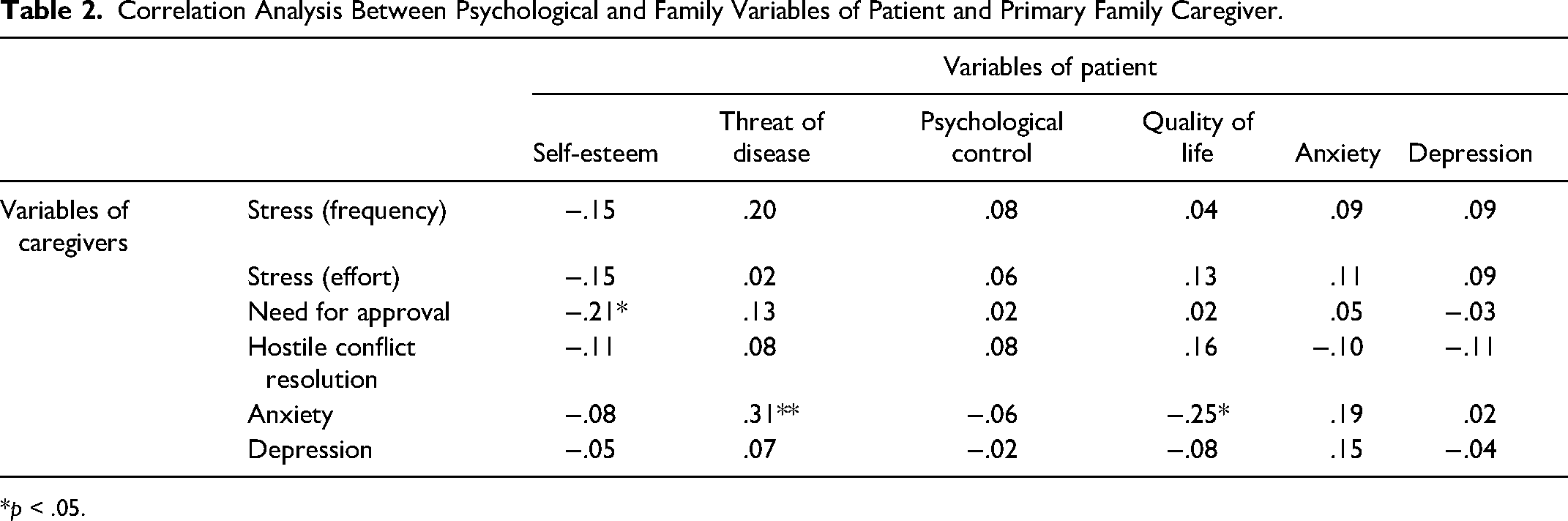
*p < .05.
Relationship Between Patient and Caregiver Variables
Patient anxiety and depression were not related to any of the caregiver variables. Caregiver anxiety was positively related to the patient's perceived threat of illness levels (rx = .30) and negatively related to the patient's quality of life (rx = .25), but caregiver depression was not related to any patient variables (Table 2).
Patient and Caregiver Prediction Models
The variables studied related to the anxiety-depressive symptomatology of the adolescent–family caregiver dyad were used as dependent variables in these analyses.
Analysis of necessity
In the necessity analysis, for both high and low levels of anxiety and depression of the adolescent and the family caregiver, no necessary condition was found because its consistency was less than .90.
Analysis of sufficiency
For predicting high scores in adolescent anxious symptomatology, four pathways were found that explained 49% of all cases (Table 3). The most relevant pathway for predicting these high levels was: the combination of low levels of stress on the caregiver's part and, in the patient, a low quality of life and greater perceived psychological control (consistency = .94; coverage = .36). In the prediction of high scores in caregiver anxious symptomatology, four pathways were found that explained 38% of the cases with high levels in this variable. The most relevant combination for predicting these high levels was: the combination of high hostile conflict resolution and high need for approval on the caregiver's part and, in the patient, low quality of life, low levels of self-esteem, higher perceived psychological control and higher perceived threat of illness (consistency = .94; coverage = .26).
Sufficiency Analysis for High and Low Levels of Anxiety in the Adolescent and Primary Caregiver Dyad.
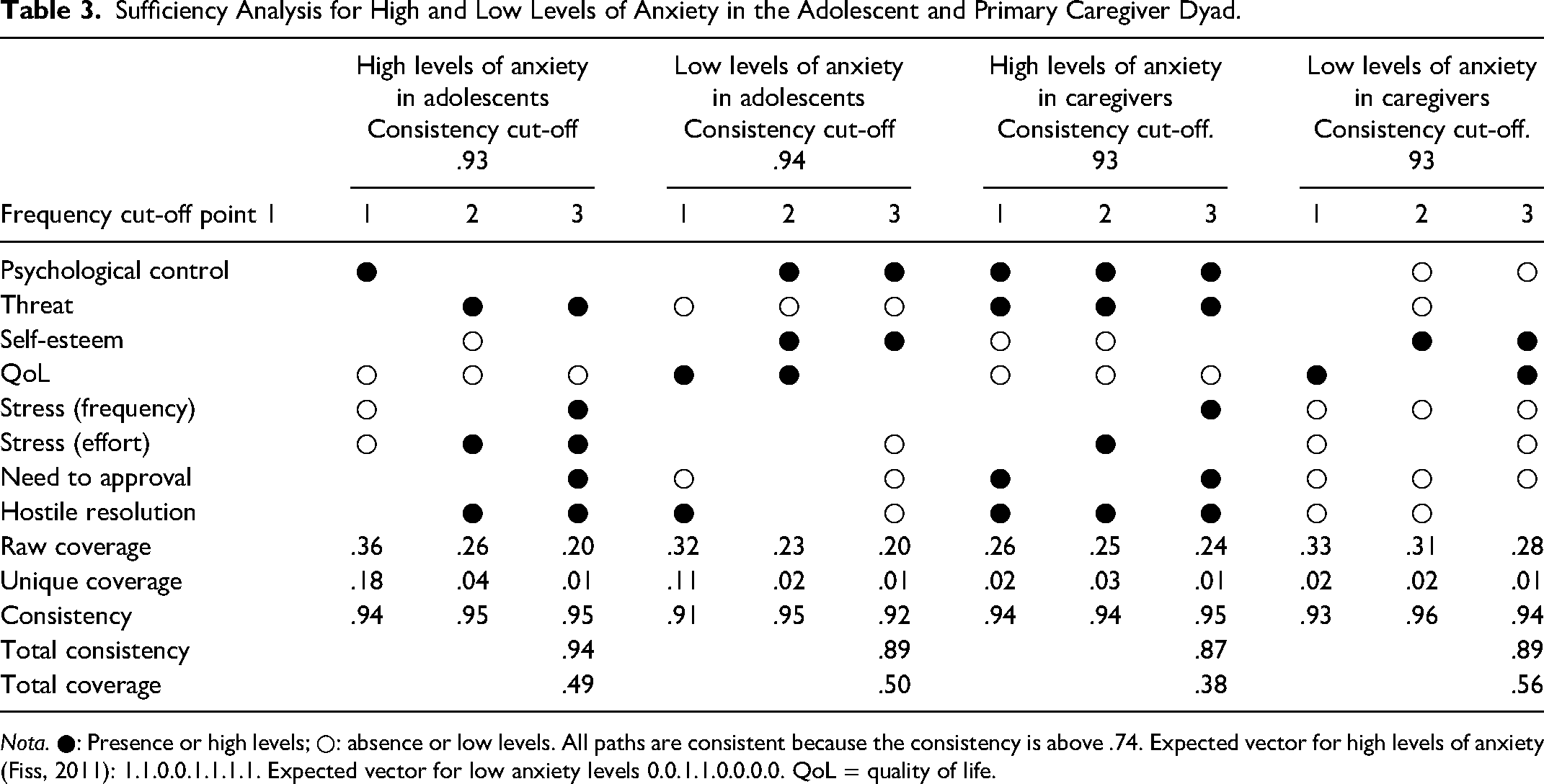
Nota. ●: Presence or high levels; ○: absence or low levels. All paths are consistent because the consistency is above .74. Expected vector for high levels of anxiety (Fiss, 2011): 1.1.0.0.1.1.1.1. Expected vector for low anxiety levels 0.0.1.1.0.0.0.0. QoL = quality of life.
In predicting low scores in adolescent anxious symptomatology, six combinations were observed that explained 50% of the cases. The most relevant combination predicting these low scores was: high hostile conflict resolution and low need for approval, together with high quality of life and high sense of threat of illness in patients (consistency = .91; coverage = .32). In the prediction of low scores in caregiver anxious symptomatology, nine pathways were observed that explained 56% of the cases. The most relevant combination was: low hostile conflict resolution and need for approval together with low levels of perceived stress and, high quality of life (consistency = .93; coverage = .33).
For high scores in adolescent depressive symptomatology, the results found five pathways that explained 40% of variance of the cases. The combination that best predicted these levels was the result of low levels of perceived stress in effort and high in frequency and, low quality of life, low levels of self-esteem, high levels of perceived psychological control and a greater sense of threat of illness (consistency = .94; coverage = .25) (Table 4). In predicting high levels of caregiver depression, six combinations were observed that explained 43% of cases. The most relevant pathway to explain this high depression was the combination of a high need for approval and high scores of perceived stress in effort, and low quality of life, higher perceived psychological control and perceived threat of illness in the patient (consistency = .97; coverage = .26).
Sufficiency Analysis for High and Low Levels of Depression in the Adolescent and Primary Caregiver Dyad.
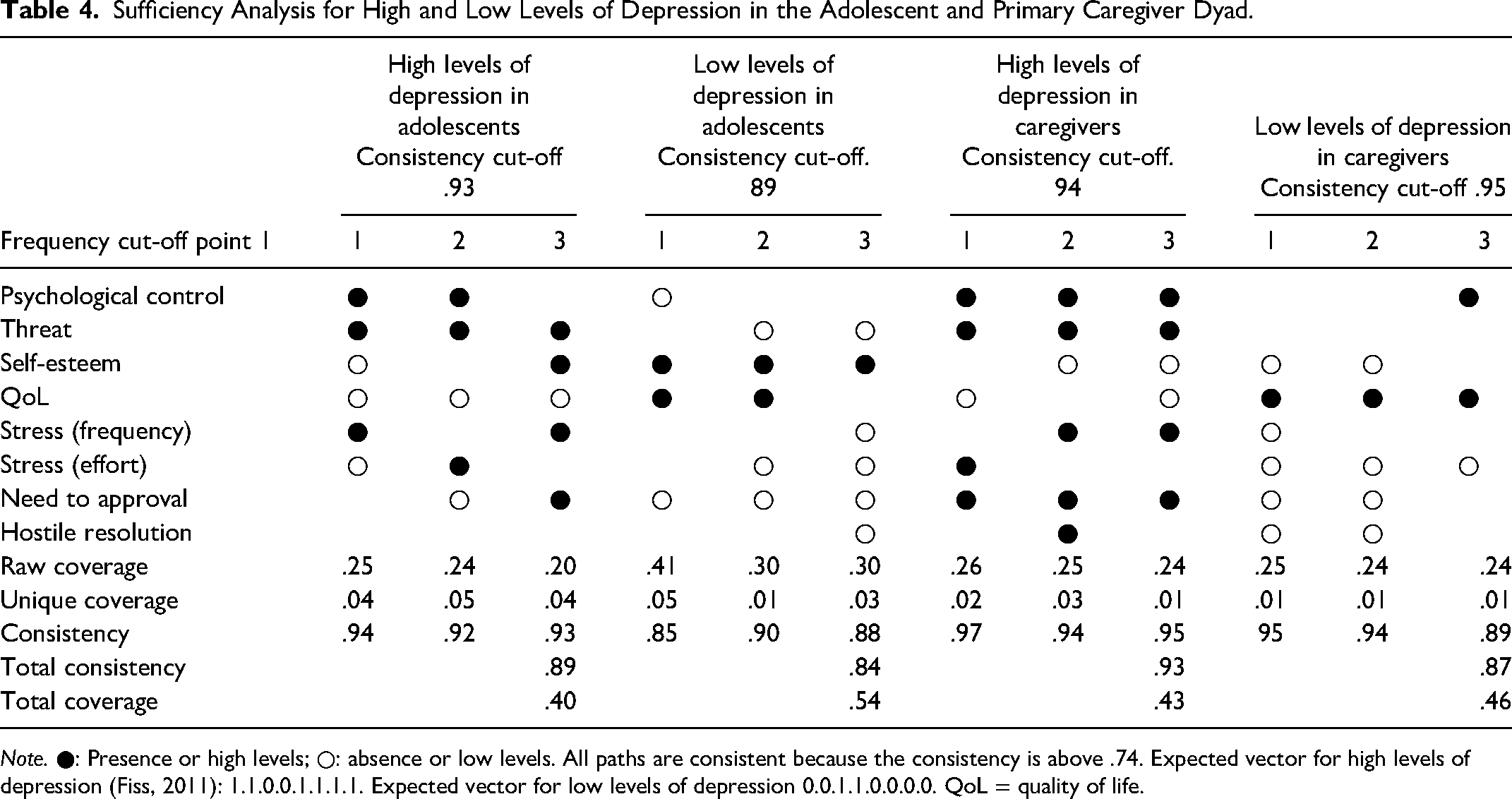
Note. ●: Presence or high levels; ○: absence or low levels. All paths are consistent because the consistency is above .74. Expected vector for high levels of depression (Fiss, 2011): 1.1.0.0.1.1.1.1. Expected vector for low levels of depression 0.0.1.1.0.0.0.0. QoL = quality of life.
In the prediction of low scores in adolescent depressive symptomatology, eight pathways were observed that explained 54% of low levels. The most relevant combination was the interaction of a low need for approval in the caregiver, and high quality of life, high levels of self-esteem and low perceived psychological control in the patient (consistency = .85; coverage = .41). In predicting low scores in caregiver depressive symptomatology, five pathways were observed that explained 46% of variance with low scores. The most important combination was the result of combining: low hostile conflict resolution and need for approval together with low scores of perceived stress in the caregiver, and, in the patient, high quality of life and low levels of self-esteem (consistency = .95; coverage = .25).
Discussion
This work has aimed to study, the relationship between psychological variables and adjustment to the disease in patients and their primary family caregivers, to analyze the possible existence of emotional contagion between them.
Regarding H1, previous research indicates that there is a two-way relationship between the emotional state of adolescents and their family caregivers. When there is a poor adjustment to the illness by the patient, this is associated with increased emotional difficulties in the caregiver (Chong et al., 2018). In addition, previous studies indicate that the evolution of bronchial asthma, its control and severity, may influence the caregiver's emotional state, increasing the presence of psychological disorders in caregivers (Weinstein et al., 2019). Moreover, the studies highlight how parental depression negatively affects their children's adherence to medication and can make it difficult to control asthma (Kub et al., 2018; Oland et al., 2017; Pinquart, 2018). Based on the studies and the hypothesis formulated, the results found no relationship between caregiver and patient anxiety and depression, contrary to expectations. The patient's emotional state did not influence the caregiver's psychological and family variables, but the caregiver's emotional state influenced the patient's psychological variables. The fact that caregiver and patient discomfort does not appear to be related could be understood by some additional variables, which have not been addressed in the present study. These variables could include explaining the existing relationship of the dyad's emotional adjustment (e.g., the inclusion of moderating variables such as family type, as well as the degree of control and severity of asthma). It would be interesting to analyze this aspect in-depth in future research to determine if it influences this relationship.
On the other hand, regarding H2, results indicate that the anxiety-depressive symptomatology of the adolescent was not related to the variables of the primary caregiver, but parental anxiety and depression were associated with patient variables. The primary caregivers who presented anxious symptoms were associated with a higher perception of threat of illness and poorer quality of life for adolescents with BA. The findings are consistent with previous research (Chong et al., 2018; Yamamoto & Nagano, 2015), which indicates that emotional management by parents directly influences children, since caregivers are their main models. In general, studies emphasize the importance of adequate psychological functioning by parents, because of its repercussions on the management of the disease. Research shows that a greater presence of anxiety-depressive symptoms in the caregiver is associated with lower rates of adherence, increased visits to the emergency department, and affects the progression of the disease and misuse of medication (Oland et al., 2017; Weinstein et al., 2019).
In addition, research indicates that family styles and the way parents and children bond (attachment) can affect the latter's psychological wellbeing (Mónaco et al., 2019). Results show that the caregiver's high self-esteem scores, without requiring constant approval by others, are associated with fewer emotional problems in the patient and a better relationship of trust and bonding with their children. Results of the associations and the QCA models for emotional adjustment of the patient–caregiver dyad are in line with those mentioned above, but in this case, it is the patient's variables that seem more relevant for predicting the emotional adjustment of the dyad. For anxiety levels, the psychological control perceived by adolescents was a variable that appeared in the different paths for both the patient and the caregiver, and the perceived threat of illness also explained the anxiety levels of both. Meanwhile, as previously mentioned, the patient's self-esteem is a protective variable in parental anxiety and patients themselves. Furthermore, to a lesser extent, parental stress influences the caregiver's and the patient's anxiety levels and the need for approval or hostile conflict resolution in caregivers.
This methodology has shown how risk and protective factors in the dyad can affect a better or worse adjustment depending on their presence or absence. As a result, our hypothesis can be accepted, as there is a certain degree of emotional contagion between the patient–caregiver dyad. Likewise, the variables that are protective factors for the adolescent are also protective for the caregiver, and vice versa.
For depression levels, results were very similar to those for anxious symptomatology. Again, the patient's psychological control, self-esteem and threat of illness are relevant variables in the emotional adjustment of the dyad. Furthermore, in the case of depression, the patient's quality of life levels influences their emotional state and that of their caregivers. In other words, high levels of quality of life are associated with lower levels of depression in both. All the above, combined with perceived stress levels, can increase or reduce the presence of depressive symptoms in both.
This study's main contributions lie in the fact that it combines variables related to the BA and its impact on the dyad's emotional adjustment. Besides, the patient's experience and that of the caregiver have been addressed, favoring a complete view of the emotional adjustment to BA. On the other hand, the study has analyzed the combination of variables to predict the dyad's emotional adjustment in a collaborative manner (QCA models) and not in a linear manner as in previous studies. However, this study is not without limitations, and it would be advisable to extend the sample to a larger number of participants (patients and caregivers) to make the results more generalizable.
Conclusions
The family is a fundamental pillar in the physical and emotional health of adolescents with chronic conditions. Parents and other primary caregivers provide attention, care, and love and can promote a safe environment for exploration and growth. Positive childhood role models associated with healthy parental parenting styles exert a strong influence on the physical and mental health-related behaviors of pediatric patients.
Footnotes
Author's Contributions
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Ethics Approval
The present study was approved by the UV-INV_ETICA-1226194 ethics committee.
Availability of Data and Material
To consult the database contact the corresponding author.
Consent to Participate
All participants and their legal guardians signed the informed consent for participation and for the publication of data for scientific purposes.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Conselleria de Innovación, Universidades, Ciencia y Sociedad Digital, Generalitat Valenciana (grant number ACIF17/389).