
Abstract
Emergency medical service (EMS) personnel are subjected to intense and traumatic workplace scenarios, which place workers at risk for developing trauma reactions that lead to mental health conditions such as posttraumatic stress disorder (PTSD), depression, and anxiety. However, little research has explored the impact of EMS workers’ work-related stress on their romantic partners despite evidence supporting the impacts of secondary traumatic stress (STS). This study explored the relationship between EMS workers’ self-reported PTSD symptomology and EMS workers’ romantic partners’ self-reported PTSD symptomology, relationship satisfaction, and social support. The sample consisted of 30 couples, 13 married and 17 unmarried. Findings confirmed that EMS workers with more severe PTSD symptomology were in relationships with partners who also reported higher symptomology. Additionally, increased PTSD severity among EMS workers was associated with partners’ decreased satisfaction with the quality of social support. This study confirms the effect of STS among EMS workers and their partners and highlights practical applications for improving the mental health of EMS workers and their partners. Implications for these findings include assessing partners for dysphoric arousal, psychoeducation, counseling assistance to EMS personnel, and focusing on opportunities for vicarious posttraumatic growth among couples are discussed.
Keywords
Emergency medical service (EMS) personnel face various challenges besides daily physical and mental demands. EMS workers routinely encounter high-stress situations and exposure to death and serious injury, a risk factor for traumatic stress (American Psychiatric Association [APA], 2022; Petrie et al., 2018). Other barriers to worker wellness include financial stress due to low staff pay and limited access to healthcare benefits; the 2021 U.S. median pay for EMS personnel was $36,930 per year (U.S. Bureau of Labor Statistics, 2023). These factors place EMS workers at risk for burnout and departure from the profession (Rudman et al., 2022). The average EMS career spans 5 years (Backberg, 2019). A systematic review indicated that EMS burnout prevalence may range as high as 56% (Reardon et al., 2020). Hutchinson et al. (2021) substantiated that EMS worker burnout scores indicate moderate emotional exhaustion and high depersonalization.
EMS workers are distinct from other first responders in that they are responsible for attending to the public's immediate medical needs, compared to protecting the law, property, or environment (Greinacher et al., 2019). Ambulance workers must care for patients under life-and-death circumstances, in places that they may not be acquainted with, with people surrounding them who could be relatives of the patient or bystanders that could be videoing them, scrutinizing them, or yelling or out of control (Sterud et al., 2006). Alexander and Klein (2001) found that in 6 months, over 80% of paramedics reported experiencing an “extraordinarily disturbing incident.” Further, Regehr (2005) found that paramedics often felt they lacked respect from the public, who simply viewed them as ambulance drivers. However, EMS workers respond to more emergency calls than police and the fire service combined (Clohessy & Ehlers, 1999). EMS workers routinely encounter life-threatening situations and frequent exposure to the death and serious injury of others, engendering consistent risk factors for developing posttraumatic stress (Greinacher et al., 2019).
In addition to direct threats to EMS workers’ wellbeing, an ecological approach may consider potential indirect effects on romantic partners and spouses. Given the increased risk of developing posttraumatic stress and burnout in ambulance work, a family systems perspective recognizes that stressors and mental illness impact the individual and their loved ones. Solomon et al. (1992) likens this to a pebble creating ripples in water, affecting more than simply the original point of entry. A family unit functions as a system where each person plays an independent and interdependent role with each other (Roth & Moore, 2009). From a family systems perspective, the current study investigates the impacts of EMS workers’ self-reported traumatic stress symptomology as an indicator of their romantic partner's self-reported traumatic stress symptomology, relationship satisfaction, and social support.
Literature Review
The Influence of PTSD Symptomology and Secondary Traumatic Stress
Traumatic stress has been conceptualized as “seismic” events that significantly disrupt an individual's worldviews or core beliefs, differentiating traumas from general adverse events (David et al., 2022, p. 400). Trauma occurs in diverse contexts, and responses to traumatic events vary significantly across individuals (Buse et al., 2013; White et al., 2018). Posttraumatic stress disorder (PTSD) describes a prolonged pattern of traumatic stress response involving symptoms of intrusion, avoidance, hyperarousal, and changes in cognitions and moods (American Psychiatric Association, 2022). Ambulance workers have been found to have a higher prevalence of PTSD and traumatic stress than the general population, with men having a greater prevalence of PTSD (23%) than women (15%; Bennett et al., 2004). A systemic review and meta-analysis of 941 articles additionally identified prevalence rates of 15% for depression, 15% for anxiety, and 27% for general psychological distress among ambulance workers (Petrie et al., 2018). In examining the nature of PTSD in first responders, first responders reported more severe levels of depression and greater levels of suppressed anger, emotional numbing, and social detachment (Bryant, 2022). Researchers have also found that one-fourth to one-third of paramedics have a high to severe range of PTSD (Alexander & Klein, 2001). A systematic review of 49 studies investigating the health status of ambulance personnel found that they had a higher standardized mortality rate, a higher level of fatal accidents, and a higher level of accident injuries than the general working population (Sterud et al., 2006).
Individuals do not have to experience a traumatic event firsthand to be negatively impacted (APA, 2022); terms such as secondary traumatic stress (STS) describe the impact of being exposed to another person's trauma within a medical or therapeutic setting (Molnar et al., 2017). Nimmo and Huggard (2013) define STS as a stress response that results from the knowledge or witnessing of traumatic experiences by those the individual is close to. Similarly, Cullins (2022) describes STS as the “immediate emotional and psychological effects experienced through vicarious exposure to details” of others’ traumatic experiences. Figley (1999) describes STS as “the stress deriving from helping others who are suffering or who have been traumatized” (p. 10).
In the workplace context, secondary trauma is a symptom of work-related psychological distress, which dovetails into outcomes such as the desire to leave the profession and job dissatisfaction (Dewey & Allwood, 2022). Further, the Diagnostic and Statistical Manual for Mental Disorders (5th ed., text rev.; DSM-5-TR) provides criteria for indirect trauma exposure, aligning with many definitions of secondary trauma in the current literature (APA, 2022; Sprang et al., 2021; Whitt-Woosley et al., 2022). Researchers such as Molnar et al. (2017) and Sprang et al. (2021) have used secondary traumatic stress and vicarious trauma (VT) to refer to the same phenomenon. While STS shares similarities with VT in that another person experiences the original traumatic event, STS differs from VT in that STS represents an acute onset response (Branson, 2019; Cullins, 2022; Singer et al., 2020). STS is more typically conceptualized as symptoms of intrusion, avoidance, and hyperarousal, as opposed to changes in schema (Greinacher et al., 2019).
The Influence of STS on Relationship Satisfaction
Empirical evidence suggests that partners of those with traumatic occupational exposure are indeed at risk for developing STS, supporting the family systems paradigm. Prior research has indicated that partners of peacekeeping soldiers (Dirkzwager et al., 2005), Vietnam veterans (Jordan et al., 1992), and clinical couples (Goff et al., 2006) experience similar levels of distress and trauma as their partners. For instance, one study of emergency service personnel partners found that 20.5% of participants indicated a moderate, high, or severe risk of STS related to their partners’ work (Alrutz et al., 2020). Recent research also suggests that the effects of the COVID-19 pandemic may exacerbate family members’ stress. A qualitative analysis of family members of healthcare workers during the pandemic found that family members worried intensely about the health of their partners and themselves (Tekin et al., 2022). Family members supported healthcare workers in the immediate aftermath of workers’ traumatic exposure, increasing their risk of STS symptoms (Tekin et al., 2022).
STS also deleteriously impacts romantic relationship quality within worker–partner dyads, such as partner coping responses and how they respond to marital tension (King & DeLongis, 2014). A meta-analysis of the effects of workplace traumatic stress symptoms found that workers’ and partners’ PTSD symptoms demonstrated similar effect sizes, suggesting that traumatic stress is transmissible in couples (Wang et al., 2022). The study also found that decreased relationship quality partially explained traumatic stress transmission (Wang et al., 2022). Regehr (2005) found that spouses of paramedics were more likely to report emotional reactivity and withdrawal from their partner following trauma exposure (Regehr et al., 2002). Consequently, paramedics’ work-related burnout has predicted increased withdrawal from their respective partners (King & DeLongis, 2014).
Additionally, in a study of military couples, Riggs et al. (1998) found that 70% of veterans with PTSD and their partners reported significant levels of relationship distress, in contrast with 30% of veterans without PTSD and their partners. Partners of veterans with PTSD endorsed more significant difficulties with intimacy and anxiety (Riggs et al., 1998). Notably, much of the available literature focuses on military and police relationships, identifying a gap regarding the experiences of EMS workers and their partners (Sharp et al., 2022). Many studies have not differentiated between the different types of emergencies and first responders, such as police, fire, and paramedic positions. One such study, a systemic review of 43 studies, found that responders’ work stress often spilled negatively into spousal wellbeing, couple relationships, and domestic violence (Sharp et al., 2022). This study seeks to address this gap by measuring the relationship between the effects of traumatic occupational exposure on EMS workers and their romantic partners.
The Influence of STS on Social Support
STS may further influence first responders’ experiences of social support. One meta-analysis found a negative association between social support and symptoms of anxiety, depression, and general psychological distress (Guilaran et al., 2018). A longitudinal study of 135 EMS workers indicated that baseline lower social support (specifically, not having someone to confide in) predicted more significant increases in symptoms of PTSD, anxiety, and depression at a 3-month follow up (Feldman et al., 2021). This result has also been found by Kshtriya et al. (2020), with the addition that social support mediated the relationship between occupational stress and outcomes of PTSD, anxiety, and depression in first responders. Social support has also been found to negatively predict depression and PTSD symptoms in ambulance workers; further, the most beneficial source of support was perceived to be spouses and family members (Reti et al., 2022). Social support is a critical element that must be accounted for when considering STS in EMS workers and their families.
The Current Study
In the present study, the impact of EMS workers’ self-reported PTSD symptomology and severity on their partners’ reporting of PTSD symptomology, relationship satisfaction, and social support was investigated. This study aimed to measure the relationship between the effects of occupational trauma on the romantic partners of paramedics. Based on the review of the literature, the following was hypothesized:
Partners of EMS workers with higher severity PTSD symptoms will report more PTSD symptoms than partners of EMS workers with lower severity PTSD symptoms.
Partners of EMS workers with higher severity PTSD symptoms will appraise the quality of their relationship as less favorable than partners of EMS workers with lower severity PTSD symptoms.
Partners of EMS workers with higher severity PTSD symptoms will report less social support than partners of EMS workers with lower severity PTSD symptoms.
Methods
Participants
Specific EMS workers recruited for this study included individuals who worked on ambulances providing treatment, such as first aid or life support care, to sick or injured patients. This often includes EMS personnel safely preparing and transporting patients to an emergency department, hospital, or other healthcare facility. Inclusion criteria for this study were as follows: (a) either identify as an Emergency Medical Technician (EMT) or paramedic that works for an ambulance service or be a romantic partner or spouse of an EMT or paramedic that works for an ambulance service, (b) currently in a romantic relationship (as defined by the participant), and (c) English speaking. Because we were focused on how EMS workers’ PTSD symptoms, relationship satisfaction, and social support would impact their partners, we only included participants in our study who were in a relationship and whose partners also participated. This left us with a total of 60 usable responses. Thirty-two ambulance worker responses were excluded because their partner or spouse did not consent, complete, or participate in the study. Very little demographic data was collected, and questions asked included: job title, identified gender, age, identified ethnicity/race, sexual orientation, marital status, and length of their relationship.
Ambulance workers
The EMS workers were, on average, 29.1 years old (range = 22–42; years, SD = 5.63). The ethnicity/race of the ambulance workers was 53% (n = 16) Hispanic/Latina(o), 43% (n = 13) non-Hispanic White, and 1% (n = 1) said they were Asian. Of the EMS workers, 83% (n = 25) were male, and 17% (n = 5) were female. Participants in this study reported the following job titles 47% (n = 14) were Paramedics, and 53% (n = 16) were EMTs. Twenty-nine (97%) couples reported being heterosexual and one (3%) identified as being queer. Thirteen (43%) couples were married and 17 (57%) were unmarried.
Partners
The EMS workers’ partners were 80% (n = 24) female and 20% (n = 6) male, with an average age of 28.6 years old (range = 20–47; years, SD = 6.08). The ethnicity/race of the partners was 50% (n = 15) Hispanic/Latina(o), 47% (n = 14) non-Hispanic White, and 1% (n = 1) Asian. As previously reported, of the 30 couples, 13 were married and 17 were not married. The average relationship reported was 4 years and 4 months (range = 2 months–14 years; SD = 3 years and 7 months).
Procedures
Participants were recruited solely through ride-alongs with ambulance crews. Ride-alongs are volunteers that shadow EMS workers during their shifts. This opportunity is a critical element for learners of prehospital emergency care. Following institutional review board ethical committee standards, ambulance workers agreed to digital informed consent before participating in the survey. Those who agreed to participate could continue to the online survey. At the end of the survey, they were asked to provide their partner or spouse's email address. Partners and spouses were then emailed an invitation to participate in the study and were provided a link to the informed consent and survey. Participants were only included in the study if both partners completed the study.
Measures
EMS workers and their partners completed questionnaires on PTSD, couple satisfaction, and social support. EMS workers’ partners were given a code to connect them to their partner's responses.
PTSD
The Self-Rating Inventory for PTSD (SRIP) was used to measure the current PTSD symptom severity of the ambulance worker and their partner (Hovens et al., 1994). The SRIP consists of 22 items that follow the description of PTSD in the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM-IV; American Psychiatric Association, 1994). Sum scores for re-experiencing (6 items), avoidance (9 items), and hyperarousal (7 items) can be derived. Answers are given on a four-point intensity scale ranging from one (not at all) to four (very much). All items were written without reference to a specific trauma (e.g., “I had recurrent unpleasant memories” instead of “I had recurrent unpleasant memories about my job-related tasks.”). The SRIP has proved to be reliable and valid (Hovens et al., 1994, 2000). The test–retest reliability correlation coefficient was .92, and the internal consistency alpha coefficient was .92. The SRIP correlates significantly with the Clinician-Administered PTSD Scale (CAPS), the Mississippi Scale for Combat-Related PTSD, Minnesota Multiphasic Personality Inventory PTSD subscale, and the Impact of Event Scale. The sensitivity and specificity of the SRIP in relationship to the CAPS were found to be very good (sensitivity = 85%; specificity = 70%; Hovens et al., 1994).
In the present study, the total score of the 22 items was used to measure current PTSD symptom severity; Cronbach's alpha coefficient for the scale was .94. PTSD diagnosis was determined according to the DSM-IV guidelines. As previously mentioned, Criteria A, “the person has been exposed to a traumatic event,” was not assessed, meaning no reference was made to a specific traumatic event.
A person had to report a score of “quite a bit” or “a great deal” on at least one item of Criterion B (intrusion), at least three items of Criterion C (avoidance), and at least two items of Criterion D (hyperarousal) to meet diagnosis criteria. It can be assumed, however, that persons not satisfying all criteria for a PTSD diagnosis (i.e., those having partial or subthreshold PTSD) can also experience serious problems (e.g., Stein et al., 1997; Zlotnick et al., 2002). Furthermore, the researcher was interested in the effect of the degree of PTSD symptoms. Total PTSD severity, intrusion symptoms, avoidance symptoms, and hyperarousal symptoms were reported for each ambulance worker and their partner.
Couples’ satisfaction
The Couples Satisfaction Index (CSI-32; Funk & Rogge, 2007) was used to measure the quality of the couple's relationship between the EMS worker and their partner. Thirty-two items reflecting the subjective evaluation of the degree of satisfaction in the relationship were measured. The scale has a variety of items with different response scales and formatting. Most of the answering format consisted of a six-point scale ranging from 0 to 5. A total score was computed, with higher scores indicating a higher degree of satisfaction in the relationship.
Social support
The Social Support Questionnaire (SSQ; Sarason et al., 1983; Heitzmann & Kaplan, 1988) is a 27-item assessment referring to the people in the individual's environment who provide help or support and the satisfaction with the overall support they have. The first part asked them to list up to nine people they could count on that provided them with social support or help, excluding themselves. Respondents could also indicate “no one” if they had no support for a question. The second part of each question asked them to score on a six-point Likert scale (6-very satisfied, 1-very dissatisfied) how satisfied they were with the overall support they received related to that specific question. Scoring for the SSQ was calculated by adding the total number of people listed for all 27 items and dividing it by 27. This provided the participants’ SSQ Number score or SSQN. Total satisfaction was scored by adding the total satisfaction for all 27 items and dividing it by 27. This provided the SSQ Satisfaction score or SSQS. The SSQ is a reliable instrument, showing that social support is (a) more strongly related to positive than negative life changes, (b) more related in a negative direction to physiological discomfort among women than men, and (c) an asset in enabling a person to persist at a task under frustrating conditions (Sarason et al., 1983).
Analytic Plan
To examine differences between partners of ambulance workers with various levels of PTSD symptomology, we divided the partners into four groups. This resulted in the following partner groups: (a) nine partners whose ambulance worker met no criteria for PTSD (level 1), (b) 14 partners whose ambulance worker met one criterion for PTSD (level 2), (c) three partners whose EMS worker met two criteria for PTSD (level 3), and (d) four partners whose EMS worker met three criteria for PTSD (level 4). EMS workers who met PTSD criteria for all three categories (intrusion, avoidance, and hyperarousal) met diagnostic criteria for a PTSD diagnosis (DSM-IV; American Psychiatric Association, 1994). To study overall differences in the outcome measures between partners of ambulance workers with various levels of PTSD, we performed an analysis of variance, with the ambulance workers’ symptom level as the independent variable and the PTSD symptoms, relationship satisfaction, and social support of the partners as the dependent variables. The main effect for the degree of ambulance workers’ PTSD symptoms was also tested.
Bivariate differences were tested employing an analysis of variance with planned comparisons using Helmert contrast coding. Statistical analyses were conducted using R 4.1.0 (R Core Team, 2021). The following contrasts were examined: (1) partners of ambulance workers with no PTSD symptoms versus partners of ambulance workers who met one, two, or all criteria for PTSD, (2) partners of ambulance workers who met one criterion for PTSD versus partners of ambulance workers who met two or three criteria for PTSD, and (3) partners of ambulance workers who met two criteria for PTSD versus partners of ambulance workers who met three, all, criteria for PTSD. Dirkzwager et al. (2005) suggested using planned comparisons because specific a priori hypotheses were formulated regarding the direction of the differences. They stated that using planned comparisons also has advantages over post hoc tests because the test is more powerful. Unlike post hoc tests, not all pairwise comparisons are tested, decreasing the risk of type 1 error (Dirkzwager et al., 2005).
Results
Intercorrelations
Table 1 presents the Pearson correlation between variables for the partners of EMS workers. The total PTSD score and the scores of the three separate clusters of PTSD correlated highly with relationship satisfaction and both subscales of social support.
Intercorrelations Between Variables for Partners of EMS Workers.
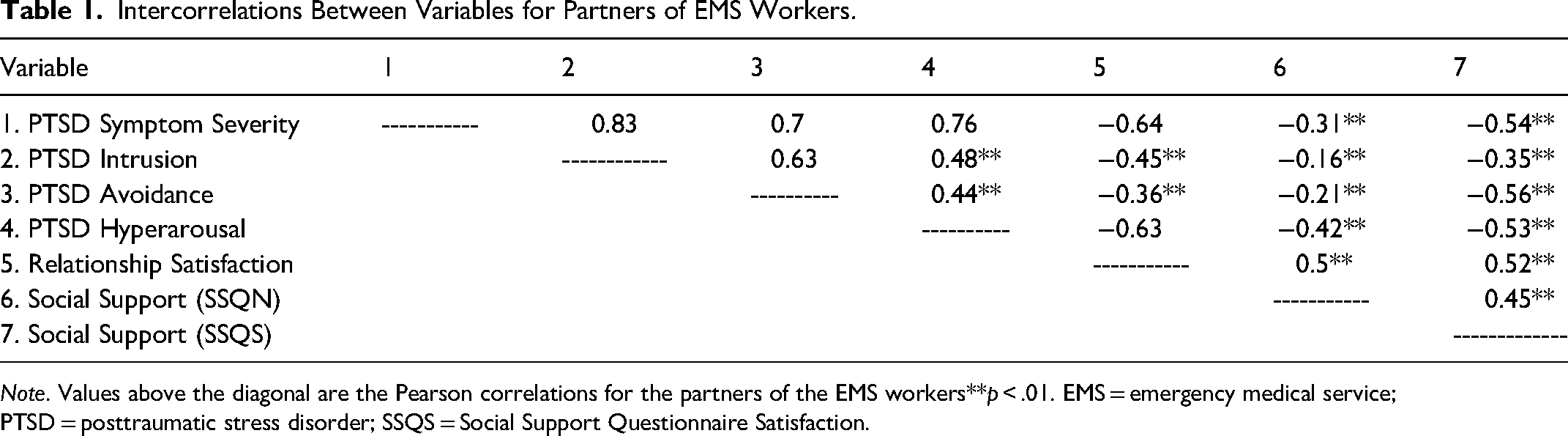
Note. Values above the diagonal are the Pearson correlations for the partners of the EMS workers**p < .01. EMS = emergency medical service; PTSD = posttraumatic stress disorder; SSQS = Social Support Questionnaire Satisfaction.
Partners of EMS Workers
Table 2 shows the mean scores for the PTSD symptoms, relationship satisfaction, and social support of the partners whose ambulance workers reported various levels of PTSD symptomology. Regarding PTSD, the Helmert contrast showed that compared to partners whose EMS workers met one criterion for PTSD, partners of EMS workers meeting two or three criteria for PTSD were more likely to demonstrate higher PTSD severity scores. We also found that partners of EMS workers with the PTSD diagnosis reported significantly higher PTSD severity than partners of EMS workers who met two criteria (F [3, 26] = 9.99, p < .001). Related to specific PTSD criteria, such as intrusion, avoidance, and hyperarousal, we found the following. Partners of EMS workers without PTSD reported significantly fewer intrusion symptoms than partners whose EMS worker met one, two, or all criteria for PTSD. And we found that partners of EMS workers with a PTSD diagnosis were significantly more likely to experience intrusion symptoms than partners of EMS workers who meet two criteria (F [3, 26] = 3.81, p < .01). Concerning avoidance, partners of EMS workers with PTSD symptomology did not report any difference related to their reporting of avoidance symptoms. Lastly, for hyperarousal, compared to partners whose EMS worker met one criterion for PTSD, partners of EMS workers meeting two or three criteria for PTSD were more likely to meet the criteria for hyperarousal (F [3, 26] = 6.56, p < .001).
Mean (SD) Comparison of Partners of EMS Workers With No, One, Two, and Mets Criteria for PTSD.
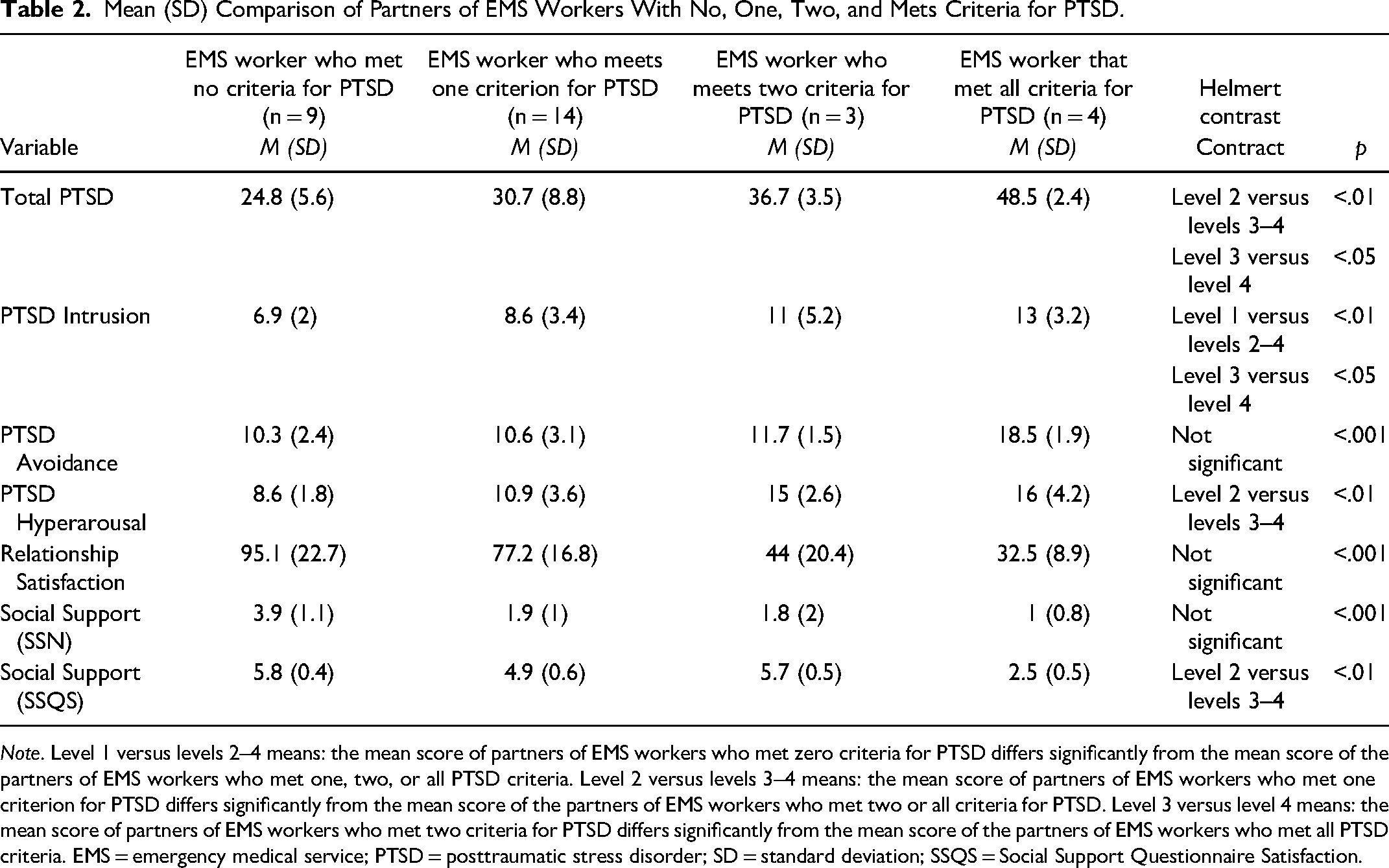
Note. Level 1 versus levels 2–4 means: the mean score of partners of EMS workers who met zero criteria for PTSD differs significantly from the mean score of the partners of EMS workers who met one, two, or all PTSD criteria. Level 2 versus levels 3–4 means: the mean score of partners of EMS workers who met one criterion for PTSD differs significantly from the mean score of the partners of EMS workers who met two or all criteria for PTSD. Level 3 versus level 4 means: the mean score of partners of EMS workers who met two criteria for PTSD differs significantly from the mean score of the partners of EMS workers who met all PTSD criteria. EMS = emergency medical service; PTSD = posttraumatic stress disorder; SD = standard deviation; SSQS = Social Support Questionnaire Satisfaction.
Concerning relationship satisfaction, examining the difference between partners whose EMS workers reported various levels of PTSD was not significant, indicating no main effect on the EMS workers’ symptom level. This finding demonstrated that partners of EMS workers with various levels of PTSD did not rate their relationship more or less favorably than partners of EMS workers without PTSD symptoms. Lastly, social support, with respect to the number of individuals, showed no significant difference among the couples. However, compared to partners whose EMS workers met one criterion for PTSD, partners of EMS workers meeting two or three criteria for PTSD were less likely to report satisfaction with their social support (F [2, 26] = 34.72, p < .001).
Discussion
Our results demonstrate that partners of EMS workers who met PTSD diagnosis criteria are at an increased risk for PTSD symptoms compared to partners of EMS workers who met partial or no criteria for PTSD. This confirms hypothesis 1, that as EMS workers report more severe PTSD symptoms, their partners also tend to report more severe PTSD symptoms. These findings are consistent with previous literature (Dirkzwager et al., 2005; Goff et al., 2006; Jordan et al., 1992; Wang et al., 2022). We also found that EMS workers’ PTSD severity most influenced partners’ intrusion and hyperarousal symptoms. Specifically, partners of EMS workers with any PTSD symptoms were more likely to report intrusion symptoms, and partners of EMS workers that met PTSD diagnosis showed significantly more intrusion symptoms than partners of EMS workers that met partial or no criteria for PTSD. Additionally, romantic partners are at an increased risk for hyperarousal at a lower threshold of only meeting two or more PTSD criteria among EMS workers. However, EMS workers’ level of PTSD symptomology does not impact avoidance symptoms among their partners.
Our results indicate that EMS workers’ PTSD symptoms do not significantly impact partners’ reports of relationship satisfaction. This disconfirms the second hypothesis that relationship satisfaction reported by partners decreases as EMS workers’ PTSD symptom severity increases. This finding was inconsistent with prior literature (Regehr, 2005, Regehr et al., 2002; Sharp et al., 2022; Wang et al., 2022). Regarding social support, responses show that EMS workers’ PTSD symptomology does not impact the number of individuals within partners’ social support networks. Instead, increased EMS workers’ PTSD symptomology has a negative effect on partners’ satisfaction with social support networks. This disconfirms the third hypothesis that partners’ number of social supporters is impacted by increasing PTSD symptoms among EMS workers; instead, the quality of social support is reported to decrease as EMS workers’ PTSD symptomology increases which is consistent with existing literature (Sharp et al., 2022; Wang et al., 2022). Level 2 partners were more likely to be satisfied with their social support, whereas levels 3 and 4 partners were less likely to be satisfied with their social support.
PTSD Severity and Partner STS Symptoms
When considering various symptoms after traumatic events, intrusion or re-experiencing symptoms are often seen as a hallmark of PTSD (APA, 2022). According to the DSM-5-TR (APA, 2022), intrusion symptoms include disturbing memories or dreams, dissociative reactions, and physiological or stress reactions to internal or external trauma-related stimuli. If left untreated, intrusion symptoms can become so severe that they are disabling to the individual experiencing them (e.g., veterans who may become incapacitated during flashbacks to combat situations; Jongedijk et al., 2023).
Gross et al. (2023) found that internally cued intrusions produce more dysphoric arousal, but externally cued intrusions create more avoidance. Because no significant impact on partners’ avoidance symptoms was seen, EMS workers’ partners may be more likely to experience internally cued intrusions which include reliving specific, experienced traumatic events or conversations about these events. Gross et al. (2023) also found that internal intrusions were associated with poorer physical functioning and better emotional functioning than external intrusions. Increased emotional functioning associated with internal intrusions might explain why the partners in this study did not report challenges in relationship satisfaction despite increasing PTSD symptomology.
PTSD Severity and Relationship Satisfaction
Although this study did not show any impact of EMS workers’ PTSD severity on their reported relationship satisfaction, prior research highlights partners’ difficulty managing everyday job stress, safety fears, and dealing with their EMS worker's emotional reactivity and withdrawal (Regehr, 2005). Another qualitative study of EMS personnel spouses found that shift work impacts numerous aspects of family life; participants reported challenges such as concern over EMS workers’ physical safety, negotiating role responsibilities, and providing support by listening and helping EMS workers process their reactions to difficult work (Roth & Moore, 2009). Debrot et al. (2018) found that detaching from work stress after the workday increases positive interactions between partners and minimizes the crossover effects of work stress from one partner to another. The respondents of this study may have healthy coping strategies for dealing with challenges associated with EMS work, which might explain why we participants did not report adverse impacts on relationship satisfaction with increasing PTSD symptomology.
Furthermore, Cleary et al. (2023) highlight that while secondhand trauma can increase the risk of STS, it can also provide an opportunity for vicarious posttraumatic growth (VPTG) and that VPTG increases as STS increases. The duality of distress and opportunity for growth afforded by EMS work among first responder families is another possible explanation for why EMS workers’ PTSD severity does not impact partners’ reported relationship satisfaction. In other words, although EMS workers’ jobs are stressful and increase the risk for PTSD symptoms among their partners, partners may also experience VPTG in which they learn to develop positive psychological changes that lead to more adaptive life philosophies (Cleary et al., 2023). This is consistent with other research supporting co-regulation among couples (Randall et al., 2021). Other researchers suggest that VPTG tends to be more commonly associated with professional identity rather than personal traumatic experiences, common among EMS workers’ family members and first responder culture (Manning-Jones et al., 2015).
PTSD Severity and Social Support
The quantity of social support does not seem to matter; instead, the quality of the social support seems most correlated to EMS workers’ PTSD symptomology. Specifically, partners of EMS workers with increased PTSD symptoms demonstrate lower satisfaction with their social support systems. Because social support predicts the development of PTSD symptoms and mediates PTSD severity (Herr & Buchanan, 2020; Kshtriya et al., 2020), this could mean that partners of EMS workers with increasing PTSD symptomology could be at risk for developing PTSD as well by way of STS and without the protective factor of social support. Possible explanations for the decrease in quality of social support may be that partners are unable or unwilling to engage in social events due to supporting their EMS worker at home or lack of desire to engage with others due to EMS workers’ emotional reactivity and withdrawal upon returning home from traumatic shifts (Regehr, 2005; Regehr et al., 2002; Tekin et al., 2022).
Implications for Practice
This study was motivated by the desire to understand the relationship between how being in close contact with and emotionally connected to someone experiencing trauma may impact dyad relationships. Previous research has found that using personal resources, social support, cognitive strategies, and coping skills predict intimacy and conflict in ambulance workers’ romantic relationships (Shakespeare-Finch et al., 2002). Supporting the efficacy of prevention and interventions that supports EMS workers will support relationships and families (Rojas et al., 2022). In terms of clinical applications, clinicians should assess EMS workers’ partners for dysphoric arousal (e.g., trouble sleeping, difficulty concentrating, and ruminating thoughts) that may elucidate internal intrusions and PTSD symptomology related to STS.
Additionally, promoting access and support for EMS workers and their partners to mental health services includes reducing stigma to seeking resources. Miller (1995) explored how paramedics and other emergency personnel are considered “tough guys” and that their jobs require them to develop certain adaptively defensive toughness of attitude, temperament, and training which are resistant to psychotherapy. Factors that contribute to this include emergency workers’ historical reputation for shunning mental health services, the idea that needing “mental help” implies weakness, cowardice, and lack of ability to do the job, and being perceived by coworkers as “folding under pressure” (Miller, 1995). Stigma related to getting help can be combated by educating EMS workers on mental health impacts. For example, Prioux et al. (2023) found that first responders over 45 years of age who did not know about the psychological effects of traumatic experiences were at a higher risk for developing partial PTSD across 5 years. Education, multicenter screening, early support management, access to institutional support, and psychological and counseling assistance are essential to preventing PTSD (Rybojad et al., 2016).
Limitations
The following limitations should be considered. First, there were limits to the diversity of our sample. Our participants were primarily men that identified as either Hispanic or White. A recent scoping review found that women and nonwhite personnel are underrepresented in the EMS workforce (Rudman et al., 2022). Our results may be influenced by our sample type and size; previous studies have reported a slight increase in stress among female personnel (Blau et al., 2012; Cash et al., 2020). Another limitation related to our study is that all assessments were self-report. Although research on trauma and PTSD typically relies on self-report measures, they can be influenced by recall bias and an individual's subjective interpretation of symptoms. Finally, we only included participants in our study who were currently in a romantic relationship and whose partners could complete the study. It is possible that EMS workers and partners that had less relationship status or higher symptomology would be less likely to complete the study. We also neglected to ask romantic partners if they were first responders or EMS workers.
Conclusion
The current study examined the role of EMS workers’ PTSD symptomology in intimate dyads. The results demonstrated that EMS workers’ exposure to trauma while on the job also impacts their partners. Research has not previously explored the effects of EMS workers’ PTSD symptomology on partners’ relationship satisfaction, social support, and STS. While further investigation is needed, this research sheds light on how EMS workers’ PTSD diagnosis and severity may impact their relationships. The results of this study offer clinical providers, and those affected an understanding of how mental health impacts more than the individual experiencing symptoms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.