
Abstract
Parents to children with autism spectrum disorder (ASD) experience increased levels of stress compared to other parents. However, it has been difficult to clarify how this parental stress affects the quality of parent partnership, and how stress and partnership quality predict each other longitudinally. Stress and perceived partnership quality of 160 parents to children with ASD who started therapy in an autism therapy center were surveyed at three measurement points. To find out about within-person effects, a random intercept cross-lagged panel model was used. The results showed that a decrease in stress level over the course of therapy led to a decrease in partnership quality. The theory of the parenting alliance can be used to explain these results: coping with demands in parenthood during stressful times seems to tie parents together and strengthen their relationship. Implications for therapeutic practice, such as the use of marriage and family counselors to support the parents’ partnership during their child's autism therapy are presented.
Keywords
Stress of Parents to Children With Autism Spectrum Disorder
Autism spectrum disorder (ASD) leads to limitations in almost all areas of life, which is why parents are permanently challenged to support their children (e.g., Mancil et al., 2009). The majority of persons with ASD are dependent on social and professional support throughout their lives (Müller-Teusler, 2008), although the severity of the impairment varies (Brobst et al., 2009). Hence, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) no longer differentiates between various subtypes of ASD but speaks of a spectrum of disorders (American Psychiatric Association, 2013).
Parents to children with ASD show increased stress levels, as shown in the meta-analysis by Hayes and Watson (2013). They reported that parents to children with ASD experience more stress than parents to children without disabilities. Also, compared with parents to children with learning and attention disorders (Chad-Friedman et al., 2022) or intellectual disability or Down syndrome (Hayes & Watson, 2013), parents to children with ASD report higher stress. It seems, therefore, that the symptoms of ASD are particularly demanding for parents, which in turn is associated with an increased stress level. In general, parental stress occurs when the available parental resources of dealing with the demands of raising their child are insufficient or overused (Tröster, 2011). In his Parenting Stress Model (1995), Abidin explains the separation of stress into three major domains: The parent domain, the child domain, and the domain of situational and demographic life stress. The parent domain includes stress resulting from limitations of parental functioning (e.g., the role restriction of parents) and the child domain includes stress resulting from the characteristics and behavior of the child (e.g., the restricted adaptability of the child). Life stress implies the stress experienced outside the parent-child relationship. These can be stressful situations such as the death of a relative. According to Hoffman et al. (2009), the stress of parents to children with ASD manifests itself primarily in those stress areas of the Parenting Stress Index (PSI; Abidin, 1995) that result from the child's behavior and characteristics. These findings are supported by the results of Sarimski (2016) who found a significantly higher level of stress in the child domain for parents to children with ASD than for parents to children with intelligence impairment.
Perceived Partnership Quality and Stress
Parental stress arises from the fact that, in the parents’ own appraisal, their resources do not adequately meet the demands of parenthood (Tröster, 2011). This mastering of demands can be facilitated by resources. One resource that could reduce the stress of parents to children with ASD is a functioning relationship with their partner. Cooperation with and the support of partners can help to cope with parental demands (e.g., Laux & Schütz, 1996). Studies have found that parents to children with ASD experienced a lower stress level when they were satisfied with their partnership quality (e.g., Siman-Tov & Kaniel, 2011). It can be assumed that a high level of partnership quality is accompanied by a lower parental stress level. This association can have a direct (practical support with the child in everyday life) or an indirect impact (improvement in general well-being) on parenthood (Domsch & Lohaus, 2010). Wiedebusch and Seelhorst (2014) found that parents to children with developmental delays rely on the emotional support and assistance of their partner as a coping response for their stress.
The fact that stress levels are higher in parents to children with behavioral disorders than in parents to typical children has been demonstrated in numerous studies (e.g., Johnston & Mash, 2001), as has the association between childhood behavioral disorders and marital conflict (e.g., Cummings & Davies, 2002). However, the results on partnership quality and ASD are inconsistent. On one hand, there are results showing that the partnership quality is lower among parents to children with ASD than among parents to typically developed children (e.g., Brobst et al., 2009). On the other hand, studies report that parents to children with ASD feel more closely connected due to the challenging task of bringing up a child (Marciano et al., 2015). If we look at the divorce rate as an indicator, the study by Hartley et al. (2010) shows that parents to children with ASD are more likely to get a divorce. However, this was refuted by Freedman et al. (2012) because after controlling for relevant covariates such as symptom severity or mother's mental health there is no longer evidence that parents to children with ASD are more likely to get divorced.
The spillover effect might be descriptive for the results of low partnership quality among parents to children with ASD. According to the spillover effect, when the stress level in one area of life (domain) is high, it can be dynamically transferred to other areas of life (e.g., Bolger et al., 1989). In our case, this means that if there is stress in parenthood, it is transferred to the partnership leading to the parents being stressed and therefore less satisfied in this area as well. This could be explained by the possibility that parents are so stressed by the demands of parenting that they no longer have the capacity to handle the demands that a partnership entails. The stress requires so many resources in one domain that there are none left for the other (Buck & Neff, 2012). In everyday practice, a deterioration of the quality of relationships due to a lack of time for hedonistic activities between couples could be a reason (Bodenmann, 2003). Given the high level of care required for a child with ASD, this phenomenon would not be unexpected. Another explanation for an observed spillover effect is the assumption that people develop a coping style so that they repeatedly resort to similar coping strategies in different situations (Aldwin, 2009). For example, if problem situations are approached with a dysfunctional coping strategy such as “avoidance,” as in the area of child education (e.g., an undesirable behavior of the child), it is likely that the parent will also use this strategy in other areas such as conflicts in the partnership. In this example, the situation would probably become worse rather than leading to a solution, which would then be seen in both areas.
However, stress could also work in a positive way, improving the partnership. The findings which argue for a strengthening of the partnership resulting from stress can be explained by the parenting alliance (Cohen & Weissman, 1984). The parenting alliance represents a mutual support system based on partnership, which is seen as central to coping with the challenges of education (Bodenmann, 2000). Gabriel and Bodenmann (2006) explain the strengthening of the relationship of parents to children with behavioral problems with a common perception of the problems in education or child behavior. The shared stressful situation ties both partners closer together as they decide to face the challenges together. In addition to satisfaction with the partnership, it seems to be important for a strong parental alliance of parents to children with disabilities that the partner participates in the caregiving for the child (Abdo & Fischer, 2003). Parents to children with ASD report that while caring for the child is time consuming, they find a relational bond as a couple by caring for the child together (Marciano et al., 2015).
Based on the above contradictory research findings on the relationship between parental stress and partnership quality of parents to children with ASD, the aim was to examine these two constructs longitudinally in order to gain insight into whether there is an inter-relationship between self-reported parental stress and perceived parental partnership quality and whether these two constructs can predict each other longitudinally. In this context, a longitudinal model was used (random intercept cross-lagged panel model; RI-CLPM; Hamaker et al., 2015), which allows a more clearcut interpretation of cross-lagged and autoregressive paths as described below.
Method
Research Design
Data were collected in the research project “ELKASS” (Parents to children with autism spectrum disorders: demands, stress, and resources; Tröster & Lange, 2019). The longitudinal study resulted from a cooperation with therapists from autism therapy centers who perceived a need for research on the topic of stress experienced by parents to children with ASD. All participants were informed about all contents of the project and about anonymity and voluntariness ahead of their participation. The ethical guidelines were officially examined.
Parents to children with ASD who had started an outpatient therapy in one of ten cooperating autism therapy centers throughout Germany during the survey period were assessed with a questionnaire at three points in time. Each therapy center consists of a multi-professional team that works according to the guidelines of the German Autism Association. In accordance with the research question, only those parents who lived in a partnership were selected for the sample. Similarly, parents to children in adolescence and young adulthood were excluded due to better comparability. Therefore, only parents whose children were 12 years old or younger are part of the sample. Only parents who started therapy in one of the cooperating therapy centers were included in the study. The first test was carried out at the beginning of the therapy. One hundred and sixty parents participated in the first testing, 98 parents (61.3%) in the second, and 59 (36.9%) in the third. There were 4 months between each test.
Participants
Parents to Children With ASD
The following sample information is based on 160 parents (137 mothers). Parents’ age ranged from 24 to 62 years (M = 39.67 years, SD = 6.96 years). German nationality was stated by 85.7% of all participating parents and 13.1% were of other nationalities such as Turkish (3.7%) or Russian (1.9%). Eleven nationalities other than German were mentioned (1.2% missing data). The highest educational degree parents reported was a university or college degree (28%) followed by 27.3% of parents who had obtained their general or subject-related qualification for university entrance, 29.8% reported having a secondary school certificate, 9.9% had passed lower secondary education, and 3.1% had left school without a degree (1.9% missing data).
In addition to supporting the children, the therapists in the therapy centers worked with the parents of almost all families (96.9%) by offering regular parent talks (94.9%) or by supporting the parents through psychoeducation (84.5%). 57% of the parent talks were attended by both parents together (41.9% by the mothers alone). The therapy centers enabled parents to attend the child's therapy session, which 39% of parents took advantage of (78.1% mothers alone, 18.8% both parents together). Other therapy programs that the parents accepted from the therapy center were systemic therapy (26.8%), behavioral therapy (22.7%), crisis intervention (18.6%), and Marte Meo therapy (7.2%), which is a developmental support concept based on video analysis of everyday situations (Baeriswyl-Rouiller, 2008). The autism therapy center also organizes support groups for parents, which were accepted by 7.7% of the parents.
Children With ASD
The ages of the children (138 male) of the parents interviewed ranged from 2 to 12 years (M = 7.68 years, SD = 2.69 years). Information on ICD-10 diagnoses of the children was provided by the therapists at the therapy centers. In addition to the diagnosis ASD, other comorbid disorders were diagnosed. More than half of the children (51.9%) with ASD had at least one or more comorbid disorders. The diagnoses as well as the frequency of comorbid disorders and the four most frequently indicated comorbid disorders are shown in Table 1.
Diagnoses and Comorbid Disorders of Children With ASD According to ICD-10 Codes.
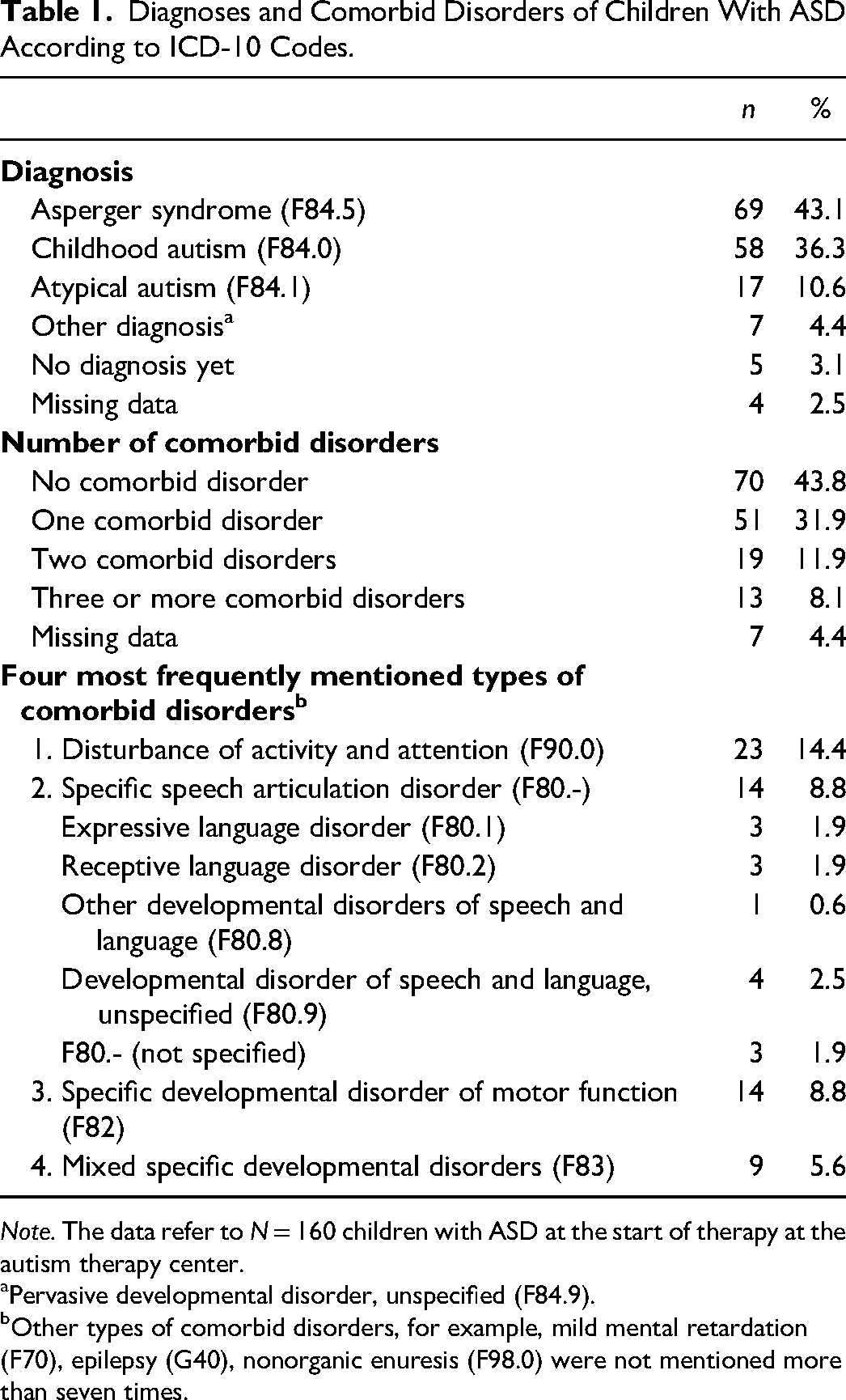
Note. The data refer to N = 160 children with ASD at the start of therapy at the autism therapy center.
Pervasive developmental disorder, unspecified (F84.9).
Other types of comorbid disorders, for example, mild mental retardation (F70), epilepsy (G40), nonorganic enuresis (F98.0) were not mentioned more than seven times.
During the second measurement, the therapists were asked about the therapy offered. Outpatient therapy usually took place once a week (89.8%) with one-to-one sessions (96.5%), which lasted one and a half hours on average (M = 1.47 h, SD = 0.47 h). In most cases, support took place in the therapy center (83.1%). The individualized support of the children was carried out with multi-method therapy approaches tailored to the needs of the clients, namely children with ASD. The three most frequently used therapy methods by the therapists were working through problems via conversations (30%), the TEACCH approach (27.5%; Treatment and Education of Autistic and related Communication Handicapped children; Reichler & Schopler, 1976), and behavioral therapy methods (18.1%).
Materials
The two constructs of stress and perceived partnership quality were assessed using self-report data from parents to children with ASD who had completed a questionnaire in German.
Parental Stress
The Parent Stress Inventory (“Eltern-Belastungs-Inventar,” EBI; Tröster, 2011), which is based on Abidińs Parenting Stress Model (Abidin, 1995), was used to measure the stress level of parents to children with ASD. Many studies have suggested the EBI's usefulness as a multidimensional screening method for recording parental stress (e.g., Irlbauer-Müller et al., 2017; Sarimski, 2017). The EBI consists of 12 subscales with four items each. Every subscale belongs to either the child or parent domain. The child domain records the sources of stress resulting from the child's characteristics and behavior. Five subscales are defined within the child domain: adaptability (example item: “My child reacts intensely when something happens that it doesn’t like.”), mood (example item: “I sometimes have the feeling that my child constantly places demands on me.”), hyperactivity/distractibility (example item: “I often feel exhausted because my child is so active.”), acceptability (example item: “My child does some things that bother me.”), and demandingness (example item: “My child does some things that challenge me a lot.”). Aspects of stress resulting from the challenges of the parental role are measured by way of the parent domain in the following seven subscales: depression (example item: “It depresses me when I notice that I react irritably to my child.”), role restriction (example item: “To do justice to my child, I have to limit myself more than I had imagined.”), social isolation (example item: “Since I became a mother/father, it has been more difficult for me to make new social contacts.”), health (example item: “I no longer have as much energy to do things I used to enjoy.”), parental competence (example item: “Some aspects connected to raising my child are harder than I expected.”), parental attachment (example item: “In some situations I wish I could better empathize with what is going on in my child.”), and partnership (example item: “Since I had the child, I don’t do as much together with my partner.”). The 48 items in total are answered on a five-point Likert scale (“does not apply at all” to “applies exactly,” high values = high stress). The EBI was normed for mothers aged 20–53 years of infant and preschool-aged children. The gender ratio of children was approximately balanced. In previous German studies, the measurement instrument has been used with parents to children with ASD (Rabsahl, 2016; Sarimski, 2017; Tröster & Lange, 2019). The EBI normative sample achieved a Cronbach's alpha of α = .91 in the child domain and α = .93 in the parent domain. The scaleś reliability calculated in this sample throughout all three measurement points ranged from α = .87 to .95 (see Table 2). The means of the child and parent domains were used for the following calculations.
Descriptive Statistics and Bivariate Correlation (Pearson) Between Perceived Partnership Quality and Parental Stress.
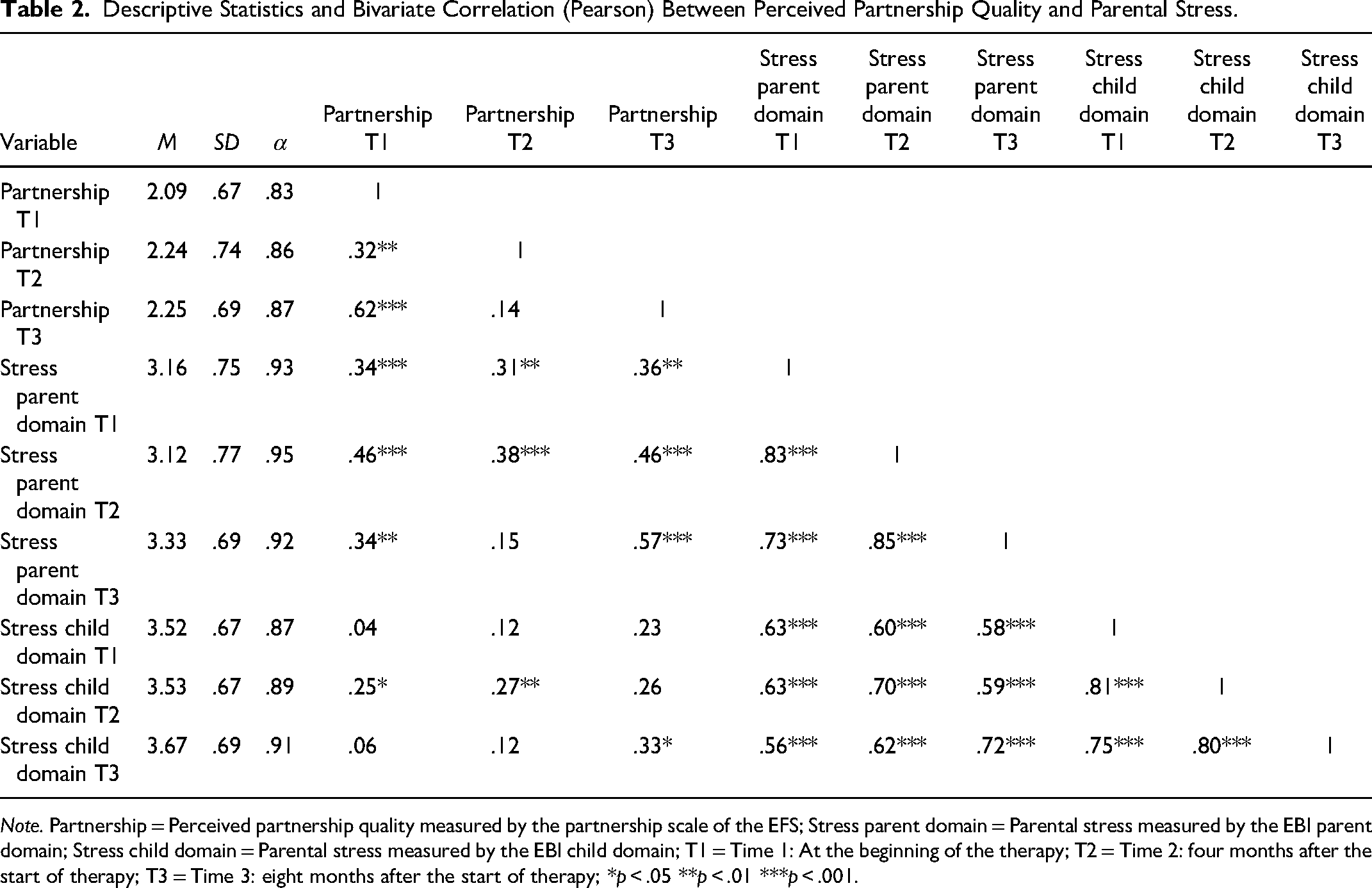
Note. Partnership = Perceived partnership quality measured by the partnership scale of the EFS; Stress parent domain = Parental stress measured by the EBI parent domain; Stress child domain = Parental stress measured by the EBI child domain; T1 = Time 1: At the beginning of the therapy; T2 = Time 2: four months after the start of therapy; T3 = Time 3: eight months after the start of therapy; *p < .05 **p < .01 ***p < .001.
Perceived Partnership Quality
The partnership scale of the parental stress questionnaire of Domsch and Lohaus (“Elternstressfragebogen,” EFS; 2010) was used to survey three areas of partnership: (a) the satisfaction with the partnership (example item: “There are some aspects of the partnership I would like to change”), (b) the support by the partner (example item: “My partner relieves me of the task of raising the child”), and (c) the agreement on educational issues (example item: “Regarding issues of education, my partner and I are in complete agreement”). The three areas are understood as “perceived partnership quality” because they only describe the subjective perception of a partner. In what follows, the construct will be referred to as “partnership quality” for convenience. The seven items were measured on a four-point Likert scale (from “applies exactly” to “does not apply,” high values = high quality). The ESF was normed with parents of children attending kindergarten (M = 35.8 years, SD = 5.3 years) as well as grades one through six in school (M = 39.9 years, SD = 5.2 years). The questionnaire was predominantly completed by the parent who was the primary caregiver of the child, which was the mother 91.4% of the time in the kindergarten sample and 92.2% of the time in the school sample. The internal consistency of the partnership scale was α = .84 in the kindergarten sample and α = .83 in the school sample. The ESF has been used in other studies for parents to children with ASD (e.g., Niemczyk et al., 2019). In our sample Cronbach's Alpha proved to be good with α = .83 to .87 in the different measurements (see Table 2). The mean of the seven items was used for the model calculations.
Statistical Analysis
To answer the research question, we used an RI-CLPM, which estimates between- and within-person effects separately. Numerous comparisons between the conventional CLPM and the RI-CLPM (e.g., Hamaker et al., 2015) show that controlling for stable between-person differences is important because estimated cross-lagged effects and autoregressive effects change in significance and magnitude when moving from CLPM to RI-CLPM. The CLPM assumes that the level of the two variables considered is the same in the population. However, it is implausible to assume that all parents have the same stress level and perceive their partnership quality to be equally high. Therefore, two random intercepts are used in the RI-CLPM in order to eliminate the between-person effects and, thus, to be able to clearly interpret the within-person effects.
A CLPM serves to analyze the interaction between different variables over time. This involves two or more different variables measured at two or more points in time. However, the results of the CLPM in some studies show biased estimates in the analysis of mutual effects of longitudinal data due to the confounding of interindividual and intraindividual effects (e.g., Bailey et al. 2020; Hamaker et al., 2015). In order to allow not only for temporal stability but also for interpersonal stability overall survey periods, random intercepts have to be included (Hamaker et al., 2015). In this way, time-stable, unobserved third-party variables can be controlled (Kühnel & Mays, 2019). In longitudinal data, the results must be considered separately at two different levels: the within-person level and the between-person level. In several studies comparing a CLPM and an RI-CLPM, the results show that especially the autoregressive effects (see Figure 1: α and δ) in the RI-CLPM are often insignificant and rather small, compared to the classic CLPM (e.g., Bailey et al., 2020; Kühnel & Mays, 2019). The RI-CLPM considers estimates for both within-person and between-person differences, although the following section will focus primarily on within-person effects to answer the underlying research question.
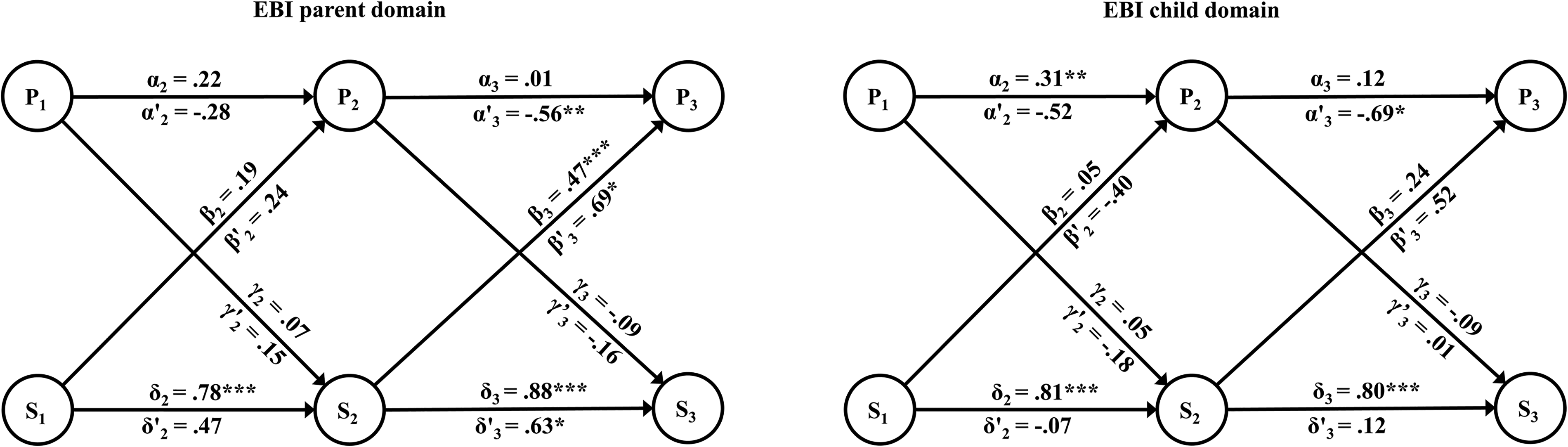
CLPM and RI-CLPM include the factors perceived partnership quality and parental stress. Note. Standardized parameter estimates with the CLPM are presented above the arrows and those with the RI-CLPM below the arrows, additionally marked with an apostrophe. P1 to P3 = perceived partnership quality for the three measurements; α2 and α3 = autoregressive parameters of perceived partnership quality; γ2 and γ3 = cross-lagged parameters of perceived partnership quality; S1 to S3 = parental stress for the three measurements; δ2 and δ3 = autoregressive parameters of parental stress; β2 and β3 = cross-lagged parameters of parental stress; *p < .05, **p < .01, ***p < .001.
The calculations were computed using the lavaan package (Rosseel, 2012) with version 4.1.1 of R (R Core Team, 2021). The model fit was evaluated with the following fit indices: comparative fit index (CFI), Tucker–Lewis index (TLI), and the root mean square error of approximation (RMSEA; e.g., Hu & Bentler, 1999). The handling of missing data was implemented with the full information maximum likelihood (FIML) estimation. In this procedure, the parameters for the sample are estimated by maximizing the likelihood function. The missing values are estimated in such a way that the distribution appears as plausible as possible for the observed data. Before applying the RI-CLPM, bivariate correlations were calculated to get an overview of the associations of parental stress and perceived partnership quality.
Results
Bivariate Correlations
Descriptive statistics and bivariate correlations between the EBI parent and child domain and partnership quality across the three measurements are reported in Table 2. There were positive correlations between the parent and the child domain of r = .56 and r = .83, p < .001. Over the course of the three measurement dates, the partnership scale correlates between r = .32, p = .002 and r = .62, p < .001. The main associations between parental stress and partnership quality are to be found in the parent domain, ranging from r = .31, p = .002 to r = .57, p < .001. The higher the stress in the parent domain, the better the quality of the partnership was perceived. In the child domain, there were no or only weak indications of connections between the two constructs (r = .04, p = .667 to r = .27, p = .009).
CLPM and RI-CLPM
For comparison, the parameter estimates for the CLPM and the RI-CLPM are shown in Figure 1. In order to better differentiate the results from RI-CLPM, they are marked with an apostrophe in the following part. The RI-CLPM fits the data significantly better than the CLPM, as shown by the fit-indices CFI and RMSEA and the likelihood-ratio-test in both domains (p < .001): parent domain CLPM: x2 (4) = 27.69, p < .001, CFI = .91, TLI = .65, RMSEA = .19; parent domain RI-CLPM: x2 (1) = .04, p = .846, CFI = 1.0, TLI = 1.06, RMSEA = .00; child domain CLPM: x2 (4) = 36.58, p < .001, CFI = .84, TLI = .39, RMSEA = .23; child domain RI-CLPM: x2 (1) = .25, p = .618, CFI = 1.0, TLI = 1.06, RMSEA = .00.
EBI Parent Domain
High autoregressive paths were found in the parent domain using the CLPM (δ2 = .78, p < .001, SE = .064 and δ3 = .88, p < .001, SE = .071), which were less pronounced (δ′3 = .63, p = .026, SE = .241) or no longer present (δ′2 = .47, p = .063, SE = .236) in the RI-CLPM. The autoregressive paths in the partnership quality showed no significant effects in either model (CLPM: α2 = .22, p = .050, SE = .121; RI-CLPM: α′2 = −.28, p = .171, SE = .234). While α3 had an insignificant positive value in the CLPM (α3 = .01, p = .951, SE = .116), the path showed a negative prediction in the RI-CLPM (α′3 = −.56, p = .004, SE = .178). At the within-person level, the negative autoregressive effect in the RI-CLPM suggests that for those parents for whom partnership quality is high at T2, compared with their own average partnership quality, it is likely that partnership quality at T3 is below their own average. Both models showed a positive cross-lagged effect in path β3 (CLPM: β3 = .47, p < .001, SE = .117; RI-CLPM: β′3 = .69, p = .021, SE = .338). At the within-person level, the positive path (β′3) showed that those parents who rated their stress lower than their own average at T2 tended to perceive their partnership quality to be worse than their own average four months later (T3). Increased stress appears to have a positive impact on the partnership. β2 showed no effect in both models (CLPM: β2 = .19, p = .080, SE = .102; RI-CLPM: β′2 = .24, p = .301, SE = .270). Also, there were no cross-lagged effects in either CLPM or RI-CLPM that are based on partnership quality (CLPM: γ2 = .07, p = .349, SE = .076 and γ3 = −.09, p = .198, SE = .070; RI-CLPM: γ′2 = .15, p = .350, SE = .149 and γ′3 = −.16, p = .299, SE = .106). Contrary to expectations, partnership quality does not seem to reduce parental stress. On the between-person level in the RI-CLPM no significant correlation was found (.39, p = .104, SE = .061).
EBI Child Domain
In the child domain, there were no cross-lagged effects in either CLPM or RI-CLPM (CLPM: β2 = .05, p = .659, SE = .114; β3 = .24, p = .083, SE = .139; RI-CLPM: β′2 = −.40, p = .547, SE = 1.251; β′3 = .52, p = .139, SE = .561; CLPM: γ2 = .05, p = .462, SE = .061 and γ3 = .01, p = .894, SE = .078; RI-CLPM: γ′2 = −.18, p = .721, SE = .330 and γ′3 = −.15, p = .510, SE = .159). In the autoregressive paths, a significant effect from T1 to T2 was found in CLPM in partnership quality (α2 = .31, p = .002, SE = .109), which was no longer present in the RI-CLPM (α′2 = −.52, p = .290, SE = .585). In the path from T2 to T3, there was an insignificant effect in CLPM and a significant effect in RI-CLPM (CLPM: α3 = .12, p = .373, SE = .121; RI-CLPM: α′3 = −.69, p = .011, SE = .242). The CLPM showed significant autoregressive effects in the child domain, which were no longer present when using the RI-CLPM (CLPM: δ2 = .81, p < .001, SE = .063; δ3 = .80, p < .001, SE = .091; RI-CLPM: δ′2 = −.07, p = .924, SE = .718; δ′3 = .12, p = .924, SE = .718). Similarly, on the between-person level in the RI-CLPM no significant effect was found (.20, p = .143, SE = .042).
Discussion
We investigated how parental stress and partnership quality of parents to children with ASD impact each other during the first eight months of support at the autism therapy center using longitudinal data and modeling techniques. Almost no substantial bivariate correlation and no cross-lagged effects were found between the quality of the partnership and the stress resulting from the characteristics and behavior of the child (child domain). It seems, that the parental stress resulting from the child's behavioral problems, in particular ASD-related symptoms, has no connection with the quality of the partnership. Rather, a connection was found between the partnership and the stress resulting from limitations or an overload of parental functioning (parent domain).
Similar to other research on and with CLPM and RI-CLPM (e.g., Bailey et al., 2020; Hamaker et al., 2015), different results are shown in the two models, especially in the autoregressive effects where, for example, effects occurring in CLPM are no longer statistically significant in RI-CLPM. In the following part, only those results of RI-CLPM will be discussed since this model fits the data better according to fit indices.
The results show no negative association between parental stress and partnership quality over the course of their child's first 8 months of therapy. The assumption that parents require many resources for their child every day (e.g., time and energy for care work), which are then no longer available to them for the partnership (e.g., time for common activities as a couple) cannot be confirmed. The findings at within-person level suggest that if the parental stress level decreases during the course of therapy, partnership quality is perceived to be deteriorating as the therapy continues. The theory of the parenting alliance (Cohen & Weissman, 1984) can be used as an explanation here. Coping with demands in parenting in stressful times ties parents together and strengthens their relationship (Marciano et al., 2015). Both parents form a unit to tackle the challenges of parenting together with each parent supporting the other. Therefore, when the stress reduces and mutual support is not as urgently needed, the partnership is perceived to have a lower quality than at a time of severe stress. One reason for this could be that parents then perceive their relationship to be less of a team. It can be assumed that the effects found between stress reduction and deterioration of partnership quality are generated by the therapy program. If the parents have gained more confidence and self-efficacy in handling their child and the ASD symptoms through the therapeutic programs at the autism therapy center (e.g., through parent talks, psychoeducation or involvement in the child's therapy), they might thus be less dependent on the support of their partner. In this regard, an imbalance between the partners could arise especially if only one of the parents has participated in the programs offered by the therapy center (57% of parent talks and 18.8% of child's therapy sessions attended together). Thus, the active parent develops new skills in dealing with the child and its disorder whereas the other parent does not, so that the parenting alliance is weakened. In addition, the parents might have learned to reflect on their different roles (parents, relationship partners) due to the support in the therapy center. While issues in the partnership were overshadowed when parental stress was high, they appear when stress decreases. Possibly the parents rediscover their role as partners in a romantic relationship and the associated challenge of a partnership, while their functional role as parents, in which they are acting as an alliance, takes a back seat. As described above, the ESF partnership scale consists of, among other things, support from the partner and agreement on educational questions. It could be that new educational issues have arisen during the course of therapy where the parents disagreed and therefore the agreement in education part of the scale was given a lower rating.
Those parents whose partnership quality initially improved in the first four months after the start of therapy (between measurements one and two) are likely to perceive a reduced partnership quality after eight months (measurement three). It can be hypothesized that the parents are generally more optimistic at first, because the therapy has started and they are excited about the newly gained support, which has an effect on the quality of the partnership. This initial euphoria might subside in the further course of the therapy and explain the effect.
During the first four months of therapy, there seemed to be no effects since neither the autoregressive pathways nor the cross-lagged pathways between the first two survey dates showed effects. Only in the later course of therapy changes appeared to occur and influences became evident. Therefore, a longer period of time should be determined in follow-up studies to be able to make more reliable statements.
Implications for Counselors
The results of the present study suggest a need for action in practice, which is not only relevant for autism therapists, but also for marriage and family counselors.
In practical work with families, it may be beneficial to encourage parents to participate together in the therapy program in order to counteract an imbalance and a weakened parental alliance between them. Autism therapists could involve parents as a team in their child's therapy so that newly acquired skills or routines can be implemented by both parents equally in everyday life. Those parents could thus continue to perceive themselves as an alliance going through the process of their child's therapy together. In this context, it appears reasonable to offer additional support structures especially geared toward fathers since they are underrepresented in the programs offered by the therapy centers. Autism therapists could also be trained by marriage counselors to analyze parental partnership quality so that they can identify needs among families. If the quality of the partnership is perceived to be low, therapists should point out options to parents as to what support and therapy services are available locally and establish contacts with these. Marriage or family counselors should then be used to provide adequate support for parents. From the present results, it can be deduced that the quality of the partnership deteriorates after the parental stress subsides in the first months of therapy. Often, the beginning of the child's therapy marks the end of a long waiting period, which is stressful for the whole family (Jungbauer & Meye, 2008). In this new process, parents need to be seen and cared for not only as parents, but also as a couple, so that their parenting relationship (or alliance) as well as their relationship as partners can be strengthened. A possible starting point is open and successful communication between the partners so that their cohesion is strengthened again (Cheatham & Fernando, 2022). This requires trained therapeutic professionals and an available adequate offer. An issue that may arise is that many parents to children with ASD have little time for such programs due to the increased care load. One possibility would be to expand the range of services offered by the autism therapy centers to include couple therapy carried out by marriage or family counselors as staff members, so that families could receive holistic care at the centers without having to visit different practices. It is important to research the topic of stress of parents to children with ASD because empirical evidence shows the urgency for policy-makers. Based on these empirical results, new structures can be developed to support families of children to ASD holistically and centrally by the state by creating and funding new family therapeutic services. However, it is important to also note that parents to children with ASD develop substantial strengths from their parenting such as resilience or hope, and experience enrichment in their lives through their child with ASD (Bayat, 2007; Kozachuk et al., 2022; Phelps et al., 2009). Therefore, in both practice and research, apart from focusing on challenges to parenthood, a focus on resources is imperative to fully map the needs of parents to children with ASD.
Limitations
The major limitation of the study is the large drop-out between the first and third measurement point, the latter of which showed only 36.9% of the initial sample. This fact may especially have an impact on the significance of the lagged effects estimates. The reasons for the dropout from the study could not be fully elucidated. Some parents no longer took their child to the autism therapy center for various reasons (e.g., successful completion of therapy, termination of therapy due to external circumstances). Other no longer wanted to participate in the study for unknown reasons. In this context, parents with increased stress taking part in the study might create a selection effect. Especially those parents who feel stressed are more motivated to participate in a study on this topic and, above all, to finish it, as they find the topic important and recognize the relevance of the research on it. The drop-out of parents perceiving lower stress levels from the study then results in lower mean stress levels at the first measurement point compared to the later points. Thus, at T2 and T3, the mean stress level would increase due to the omission of parents who are generally less stressed. There may also be biases in the quality of the partnership. It can be assumed that those parents who stay together despite the high demands and stress due to child characteristics (e.g., ASD symptoms) have a strong partnership.
Furthermore, fathers are underrepresented in the present study. Rivard et al. (2014) showed in their study that fathers of children with ASD have higher stress levels than mothers. This could be related to the fact that in families where parents adopt traditional gender roles, fathers are less involved in active care and educational work and therefore benefit less from therapy and counseling services. For further research it would therefore be desirable to have a more balanced sample in terms of gender and to consider the extent and nature of each parent's involvement in child parenting. Both of these aspects would enable an examination of gender-specific effects. In addition, it would have been useful to collect data from both partners rather than one in order to make clearer statements about perceived partnership quality.
Another limitation of the study is the scale used to measure the quality of the partnership. In the ESF, the scale used is a subscale in the larger context and comprises only seven items. The construct of the perceived partnership could have been surveyed in more detail and in all its facets. There are numerous research results on the connection between dyadic coping and marital quality (e.g., Bodenmann et al., 2006). Parental coping strategies were not explicitly taken into account in the analyses. In this case, it would have been particularly interesting to know whether the parents use interpersonal and/or dyadic coping strategies. Longitudinal study results by Bodenmann (1997) showed that stress triggers an increased risk of break-up both directly and indirectly through individual and dyadic coping. Dyadic coping has also been identified as an important resource for parents to children with childhood behavioral problems and represents an important resource for coping with the demands of parents to children with behavioral problems (Gabriel & Bodenmann, 2006). This component should be considered in future studies in order to enable a specific support, for example, in the form of couples therapy offers for parents to children with ASD.
Regarding the chosen method, it should be noted that in the RI-CLPM time-invariant confounders but no time-variable confounders can be controlled by the random intercepts. Thus, for causal interpretations, the control of time-variable confounders, such as the severity of autism symptoms, would be necessary. Studies show that the severity of autism symptomatology (Lyons et al., 2010), the number of comorbid disorders (Zablotsky et al., 2013), and the point in time the diagnosis has been received (Rivard et al., 2014) can influence parental stress. These variables should be considered in future research.
In summary, the representativeness of the sample of this field study is limited. Nevertheless, it must be noted that practitioners deal with such a heterogeneous clientele on a daily basis, which is why the results are relevant.
Footnotes
Acknowledgments
We would like to thank the parents who participated in our longitudinal study “ELKASS” for their commitment, as well as the therapists from the ten cooperating autism therapy centers for their support during the process of data collection during the study. The study was funded by the German Autism Association and the participating autism therapy centers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.