
Abstract
There has been little attention to personality in research on school refusal (SR). This study examined personality traits among 41 adolescents receiving cognitive–behavioral therapy (CBT) during participation in a School Refusal Program in the Netherlands. Traits were examined via clinical scales and 2-point code types derived from the Minnesota Multiphasic Personality Inventory–Adolescent. The influence of personality traits on treatment outcome was examined at post-treatment and 1-year follow-up. At pretreatment, eight of the 10 clinical scales were disproportionately skewed toward the “high to very high” range relative to a norm group. Social introversion and depressive symptomatology were significantly increased relative to the norm group, and nearly one-half of the adolescents were characterized by code type 2-3/3-2 (depression/hysteria) or 2-0/0-2 (depression/social introversion). Adolescents characterized by a 2-0/0-2 code type were almost twice as likely (odds ratio = 1.78) to be treatment responders at post-treatment. There was no relation between personality traits and treatment outcome at follow-up. The small sample size limits generalization of the study’s findings. If the results are replicated, personality traits may provide useful indications for personalizing treatment when employing interventions recommended in CBT manuals for SR.
School refusal (SR) is a type of school attendance problem said to occur when a young person is reluctant or refuses to attend school, in conjunction with emotional distress such as anxiety or depression (Heyne et al., 2019). It may result in weeks, months, or years of absence from school which can have short- and long-term negative effects on youths (i.e., children or adolescents), families, schools, and the community (Heyne & Brouwer-Borghuis, 2022). Between 1% and 7% of youths in the general population experience SR (Egger et al., 2003; Havik et al., 2015a; Heyne & King, 2004; Steinhausen et al., 2008) as do 5% to 16% of clinic-referred youths (Al Husni Al Keilani & Delvenne, 2021; Burke & Silverman, 1987; Hersov, 1985; Honjo et al., 1992; McShane et al., 2001; Roué et al., 2021). SR is often associated with psychiatric disorders and somatic complaints. Among adolescents receiving treatment for SR, the more common anxiety disorders are social anxiety disorder and generalized anxiety disorder (Heyne et al., 2011; Melvin et al., 2017). Somatic complaints occur among 50% to 80% of referred youths displaying SR (Berg, 1980; Honjo et al., 2001).
Cognitive–behavioral therapy (CBT) is the most commonly evaluated intervention for SR (Heyne et al., 2015), and it is associated with improved school attendance (Maynard et al., 2018). However, CBT for SR appears to be less effective among adolescents relative to children (Heyne et al., 2014). Heyne (2022) discussed factors that may contribute to different outcomes according to developmental level, noting that SR in adolescence is more severe and the clinical presentation more complex. For example, older youths displaying SR are more likely than younger youths to experience social anxiety disorder (Last & Strauss, 1990), which is often treatment-resistant (Bernstein et al., 2001; Heyne et al., 2011) and predictive of poorer response to treatment for SR (Layne et al., 2003; McShane et al., 2004). Furthermore, one-quarter to two-thirds of adolescents displaying SR and participating in treatment experience a depressive disorder (Carpentieri et al., 2022; McShane et al., 2001; Walter et al., 2014). Authors have suggested that depression can interfere with an adolescent’s ability to participate in CBT for SR (Bernstein et al., 2001; Tolin et al., 2009).
Personality may also impact treatment outcomes, but it has received little attention in empirical research on SR. It is conceivable that adolescents displaying severe SR experience personality problems that negatively influence their response to treatment. Following, we review studies of the relationship between personality factors, absenteeism, and SR. Thereafter, we consider two lines of research which lend support to the notion that adolescents with SR may respond less well to treatment because of associated personality problems.
Personality, Absenteeism, and School Refusal
Personality is mentioned in a multifactorial framework for understanding absenteeism (Melvin et al., 2019), and personality problems were grouped with “risky coping” variables in a meta-analysis of risk for absenteeism (Gubbels et al., 2019). We identified two studies that directly addressed the association between personality and absenteeism (i.e., not SR specifically). Lounsbury et al. (2004) reported that absenteeism was negatively associated with the Big Five personality traits of openness, conscientiousness, and emotional stability among adolescents (10–18 years) in Grades 7, 10, and 12, and with agreeableness among adolescents in Grades 10 and 12, but the correlations were modest in size. Petrides et al. (2005) used the Eysenck Personality Questionnaire—Revised (S. B. G. Eysenck et al., 1985) and found that the traits extraversion and psychoticism were significant negative predictors of attendance among adolescents (mean age 16.5 years).
Four community studies addressed the relationship between personality traits and SR or a construct similar to SR. Honjo et al. (2003) studied self-reported school avoidance and personality in a sample of Japanese youths (junior high or high school) using a School Refusal Personality Scale developed for the study. The personality scale yielded factors representing “obsessive–compulsive,” “passive–unsocial,” and “socially introverted.” “Passive–unsocial” and “socially introverted” showed low but significant positive correlations with school avoidance while the correlation with “obsessive–compulsive” was negative. The authors suggested that obsession–compulsion may inhibit an increase in feelings of school avoidance.
Ingul and Nordahl (2013) studied factors differentiating anxious youths with high absenteeism or low absenteeism based on a Norwegian sample (16–21 years). The Iowa Personality Disorders Screen (Langbehn et al., 1999) comprised items corresponding to Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for personality disorders. In univariate analyses, the anxious attenders and anxious absentees did not differ with respect to personality problems, but in multigroup discriminant analysis, negative personality traits were an important risk factor for absence among anxious youths. The authors argued that “current treatments for anxious school refusal may be too narrow” (p. 8).
The other two studies examined personality in relation to child-motivated absenteeism. Child-motivated absenteeism includes SR and truancy (Heyne et al., 2019), so it is unclear to what extent findings apply specifically to youths displaying SR. In the first of these, Filippello et al. (2018) investigated the relationship between personality factors and risk for child-motivated absenteeism in a sample of Italian youths (average age 14 years) using the Big Five Inventory (BFI; John et al., 1991). The School Refusal Assessment Scale–Revised (SRAS-R; Kearney, 2002) was used to assesses four functions served by child-motivated absenteeism. Neuroticism and maladaptive emotion regulation strategies were positively related to risk for child-motivated absenteeism, while extraversion, agreeableness, conscientiousness, and trait emotional intelligence were negatively related. The authors concluded that personality traits may play a role in predicting child-motivated absenteeism, but it is important to note that they did not measure school absenteeism. Nonetheless, the study suggests that individual difference variables have a role in child-motivated absenteeism. In a similar study, Martín et al. (2021) used the BFI and SRAS-R with Spanish youths (8–11 years), focusing on two functions of child-motivated absenteeism. Findings related to the first function of the SRAS-R—avoiding school-related stimuli provoking negative affectivity—are of specific interest because this function is characteristic of youths displaying SR. There was a significant positive correlation with neuroticism, and significant negative correlations with extraversion, agreeableness, conscientiousness, and openness.
The relationship between personality and SR has also been studied in clinical samples. Early work was based on less rigorous methods. For example, Morgan (1959) classified the clinical characteristics of 35 school phobic Welsh youths (most in the 11–13 years age range) using a checklist incorporating items about personality (the authors also used the terms “refusal to go to school” and “school anxiety” when referring to these youths). Almost two-thirds of these youths referred for treatment were rated as having “hysterical personality traits” or “obsessional behavior.” In Kahn and Nursten’s (1962) literature review, SR was discussed in relation to personality development. One category of youths displaying SR was labeled “character disorder,” referring to youths whose lack of growth of personality meant that their limited internal resources were drained by the experience of school.
Subsequent studies from the United States and the United Kingdom provided descriptive accounts of youths participating in treatment for SR. Coolidge et al. (1964) suggested that a large number of youths were “experiencing a delay or an arrest in personality development” (p. 684); Berg (1970) alleged that one-third of treated youths were “severely handicapped by neurotic problems and inter-personal difficulties” (p. 45); and Berg et al. (1976) described severe schizoid personality traits in two youths. Blagg and Yule (1984) used an established instrument to investigate personality traits among youths (most in the 11–16 years age range) participating in treatment for SR. The Junior Eysenck Personality Questionnaire (H. J. Eysenck & Eysenck, 1975) revealed changes in self-reported personality scores following treatment; extraversion scores increased and neuroticism scores decreased.
Xueqing et al. (2018) compared the underlying structure of personality among youths displaying SR (the authors did not specify their operationalization of this construct) and those not displaying SR, drawing on a Chinese sample of youths (12–18 years) from a mental health outpatient clinic. The Junior Temperament and Character Inventory (Luby et al., 1999) was used to assess four dimensions of temperament (novelty seeking, harm avoidance, reward dependence, and persistence) and three dimensions of character (self-directedness, cooperativeness, and self-transcendence). The SR group scored higher on harm avoidance and lower on all other dimensions except self-transcendence. Xueqing et al. (2018) argued that youths who are “too scrupulous, nervous, sensitive, and unsociable in personality traits have moderately poor social adaptive ability and tense interpersonal relationships which will more easily lead to the incidence of school refusal” (p. 1282).
In the most recent study of personality traits among clinic-referred youths, Italian help-seeking youths (14–18 years) displaying SR were compared with those not displaying SR (Carpentieri et al., 2022). Based on the Shedler-Westen Assessment Procedure for Adolescents (SWAP-A; Westen et al., 2005), adolescents displaying SR exhibited fewer adaptive personality features and more schizoid and schizotypal characteristics. In multivariate analyses, the groups did not differ on personality variables. The authors also described the subset of 28 youths displaying SR. The mean scores for two SWAP-A personality profiles reached the threshold for personality pathology, namely “emotionally dysregulated” (e.g., feel unhappy, emotions spiral out of control) and “inhibited self-critical” (e.g., feel ashamed and embarrassed, avoid social situations due to fear of humiliation). They concluded that more research with larger samples from clinical settings is needed to better understand the role that personality plays in order to personalize treatment and improve clinical interventions.
The Potential Influence of Personality on the Outcome of Treatment for School Refusal
Two areas of research support the notion that adolescents with persistent SR may respond less well to treatment because of associated personality problems. The first comprises studies of the relationship between the persistence of SR and: (a) personality factors, and (b) treatment outcome. The second comprises adult studies of: (c) the relationship between personality factors and internalizing problems, (d) the persistence of internalizing problems, and (e) the outcome of treatment for internalizing problems.
First, the persistence of SR is associated with personality factors and treatment outcome. Baker and Wills (1978) compared youths displaying persistent SR or acute-onset SR. Youths displaying persistent SR had a significantly greater proportion of abnormal premorbid personality traits such as anxious or withdrawn personalities and a higher degree of neuroticism. Hersov (1960) compared personality types across three groups, those displaying persistent SR, those displaying persistent truancy, and a control group. Fifty-two percent of those in the persistent SR group were described as excessively passive, dependent, and inhibited, compared with 28% of the persistent truancy group and 28% of the control group. Okuyama et al. (1999) found that the personality traits introversion and nervousness were significantly related to the persistence of SR. Furthermore, treatment outcome was predicted by the duration of school absence (months between onset of school absence and first evaluation), amount of absence (complete non-attendance, ≤50% attendance, or >50% attendance in the month prior to the first evaluation), and motivation to go back to school. The authors argued that personality should be assessed to understand the likely outcome of treatment and to inform the choice of therapeutic approach.
Second, adult studies point to a relationship between personality factors and internalizing problems. A meta-analysis by Friborg et al. (2013) revealed that the risk of adults having a personality disorder was high across all anxiety disorders, varying between 35% for posttraumatic stress disorder and 52% for obsessive-compulsive disorder. Cluster C personality disorders were twice as common as Cluster A and Cluster B personality disorders. Social anxiety disorder, a common diagnosis among adolescents displaying school refusal (Heyne et al., 2011), was highly correlated with Cluster C avoidant personality disorder. Moreover, the early onset of social anxiety disorder (i.e., by age 15 to 18) was a significant moderator that increased the risk of a comorbid personality disorder. Numerous studies also indicate that personality disorders negatively affect the persistence of adult anxiety and the outcome of treatment (Friborg et al., 2013; Skodol et al., 2014; Van Velzen et al., 2000). An earlier review by Reich (2003) concluded that dysfunctional personality traits have a negative effect on the outcome of treatment for anxiety and depressive disorders. As noted, anxiety and depressive disorders are common among adolescents displaying school refusal. Thus, adolescents displaying SR and experiencing an anxiety or depressive disorder may respond poorly to treatment for SR because of concurrent personality factors.
Aim
There is limited empirical research on personality traits among youths displaying school attendance problems, and SR more specifically, despite the suggestion that the influence of personality traits on absenteeism might vary according to the type of absenteeism (Lounsbury et al., 2004). Research also suggests that adolescents displaying SR are less responsive to treatment, relative to children. This applies to CBT for SR (Heyne, 1999; Last et al., 1998) and to other forms of SR intervention (Prabhuswamy et al., 2007; Rodriguez et al., 1959; Valles & Oddy, 1984). No studies have evaluated the extent to which personality traits influence the outcome of treatment among youths referred for treatment of SR.
The current study explored personality traits in a sample of Dutch adolescents participating in clinic-based CBT because of SR. The two main research questions were:
In relation to the first question, it was hypothesized that personality traits observed among adolescents displaying SR would differ from the normative group. In relation to the second question, it was hypothesized that personality traits would have predictive value for treatment outcome.
Method
Participants
Participants were adolescents (ages 12 to 17 years) displaying SR and presenting to the outpatient School Refusal Program of the Child and Adolescent Mental Health Service (CAMHS) in The Hague, the Netherlands. Referrals to the School Refusal Program were made by external mental health professionals, general practitioners, school attendance officers, and other health care professionals within CAMHS. Adolescents were admitted to the program if they: (a) were enrolled in secondary school; (b) fulfilled Berg’s (2002) criteria for SR; (c) were diagnosed with a DSM anxiety, depressive, or somatoform disorder; (d) had been unable to reintegrate in their regular school; and (e) had parents willing to cooperate with the treatment program. Exclusion criteria were: (a) Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnosis of autism spectrum disorder or severe psychiatric disorders where the sense of reality was disturbed (e.g., psychosis); (b) a school attendance problem other than SR (e.g., truancy); (c) extreme acting-out behavior (e.g., self-harming behavior); and (d) family inability to adequately support treatment (e.g., not able to provide transport to school during treatment; a parent experiences a severe psychiatric disorder).
Between 2011 and 2017, 56 adolescents were referred to the School Refusal Program. Of these, 41 adolescents (15 boys and 26 girls) with a mean age of 14.8 years (SD = 1.2) were included in the current study. Of the 15 adolescents not included, 1 was diagnosed with autism spectrum disorder, 1 was diagnosed with psychosis, and 13 had not been administered the key instrument used in this study, the Minnesota Multiphasic Personality Inventory–Adolescent (MMPI-A; Van Dijk et al., 1993).
Across the 41 adolescents included, the average length of complete absence from school was 7 months (SD = 7, range = 0–36). Indeed, nearly half (49%) of the adolescents had not attended school at all for at least 6 months. DSM-IV classifications were based on assessment by psychologists or psychiatrists at the CAMHS. Primary diagnoses at the start of treatment were social anxiety disorder (n=12), psychosomatic disorder (n=9), anxiety disorder not otherwise specified (n=6), generalized anxiety disorder (n=3), separation anxiety disorder (n=3), dysthymia (n=2), posttraumatic stress disorder (n=2), major depressive disorder (n=1), somatization disorder (n=1), reactive attachment disorder (n=1), and personality disorder not otherwise specified (n=1). Sixty-one percent (n=25) of the adolescents were diagnosed with at least one comorbid disorder. More specifically, 17 (41%) of the 41 adolescents had one comorbid disorder, 7 (17%) had two comorbid disorders, and 1 (2%) had three comorbid disorders. Regarding intelligence level based on Full Scale IQ (Kort et al., 2005), scores were above 120 for 2 (5%) of the 41 adolescents, between 110 and 119 for 5 (12%) adolescents, between 85 and 109 for 24 (59%) adolescents, between 80 and 84 for 5 (12%) adolescents, and below 80 for 5 (12%) adolescents. Seventeen adolescents (41%) lived with both parents, 18 (44%) lived with one parent and had contact with the other parent, 5 (12%) lived with one parent and had no contact with the other parent, and 1 (2%) adolescent lived with a widowed parent.
Design
This was a retrospective study based on anonymized data retrieved from the case files of adolescents participating in the CAMHS School Refusal Program. Data extracted from the files included: demographics; pretreatment information about SR, absenteeism, diagnosis, and MMPI-A scores; post-treatment school attendance; and school attendance at 1-year follow-up.
Procedure
A file review was conducted by the first author. Permission to access this data was granted by Parnassia Academy which deemed formal ethics approval unnecessary because the study used retrospective anonymized data. All procedures in this study were aligned with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The CAMHS School Refusal Program is a Tier 3 intervention (Kearney & Graczyk, 2014) offered to adolescents displaying severe SR (i.e., nonresponse to earlier attempts to address SR; average school non-attendance of 7 months, at least 2 psychiatric disorders). Adolescents received individual or group CBT (average of 1 session per week) alongside family therapy and/or parent coaching sessions. Additional individual therapy was provided when indicated (e.g., trauma therapy, eye movement desensitization and reprocessing). This therapeutic aspect of the School Refusal Program continued for as long as the adolescents participated in the special school, described next.
When treatment started, the adolescents started attending school part-time in a special class with a small number of students (no more than 7), within a school located at the mental health service. This special school provides education for youths with special needs, many of whom receive services through the CAMHS. By attending the special class in this school, the adolescents in the School Refusal Program were helped to face their fears by participating once again in an educational setting. As is customary in the School Refusal Program, attendance in the special class increased across a 4-month period from two lessons per day to four lessons per day, for 4 days per week. After 4 months, adolescents were placed in a larger class with between 12 to 17 students, and the expectation for attendance increased to four lessons per day for 5 days a week (all lessons were held in the afternoon). When an adolescent was able to attend all these lessons, they further increased their school attendance in a graduated fashion by also attending morning lessons. Each adolescent attended the special school for at least 1 school year, during which time they were helped to develop a plan for return to a mainstream or special (educational) needs school.
Reintegration into the school of origin rarely occurs among youths in the School Refusal Program. The plan for return to a mainstream or special (educational) needs school involved gradual engagement at the new school. The CAMHS school mentor or therapist helped the young person with the development of the plan. For example, the adolescents attended open days and visited their new school several times prior to the actual “starting date.” Once the adolescents started attending their new school, they were offered ongoing support by the therapist in the form of monthly booster sessions aimed at relapse prevention, for the first 2 to 3 months of the school year.
To gather attendance data at post-treatment and 1-year follow-up, staff at the special school contacted each adolescent’s new school or the parents. This occurred at the end of October (after autumn school holidays) for the first and second school year after treatment concluded. The information was recorded in the CAMHS case file and accessed for the purposes of the current study.
Measures
Personality Traits
The MMPI-A (Butcher et al., 1992) was used to assess adolescents’ personality traits. This self-report questionnaire for adolescents ages 13 to 18 years consists of 478 true–false items developed to identify personal, social, and behavioral problems. There are eight validity scales, 10 clinical scales, 15 content scales, and six supplementary scales. The official Dutch version of the MMPI-A (Van Dijk et al., 1993) includes T-scores for the validity scales and clinical scales based on a norm group of 1,182 adolescents. The validity scales used in the current study were L (Lie, unsophisticated lying); F and subscales F1and F2 (Low Frequency, tendency to answer affirmative to items rarely endorsed by a normal population, also indicating psychopathology); and K (Correction, sophisticated lying). The clinical scales used in the current study were: Scale 1, Hs (Hypochondria); Scale 2, D (Depression); Scale 3, Hy (Hysteria); Scale 4, Pd (Psychopathic deviation); Scale 5, Mf (Masculinity-Femininity, measuring the adolescent’s identification with traditional gender roles); Scale 6, Pa (Paranoia); Scale 7, Pt (Psychasthenia, indicating inter alia compulsions, obsessions, abnormal fears, and difficulties in concentration); Scale 8, Sc (Schizophrenia); Scale 9, Ma (Hypomania); and Scale 0, Si (Social Introversion).
There are different methods for interpreting MMPI-A profiles (Archer, 2017). One method is to interpret the clinical elevations of the single clinical scales and another is to interpret the 2-point code types, whereby the two highest clinical scales of a profile are taken into account. Both methods stem from the interpretation of the MMPI-2 (adult version) but they can also be used for the MMPI-A (Archer, 2005) with some modifications (Archer, 2017). The function of coding is to provide a convenient way to identify salient characteristics in the profile by organizing the information into a simple-to-read summary for clinical and research purposes (Friedman et al., 2014).
Both methods of interpretation were used in the current study. In relation to the first method, elevated single-scale interpretation was based on the Dutch manual, applying the following descriptions: T-scores above 75 were “very high,” T-scores between 65 and 75 were “high” (considered as clinical scores); T-scores between 60 and 64 were “moderately increased”; T-scores between 45 and 59 were “normal range”; and T-scores below 45 were considered “low.” In relation to the second method, a code type was defined by the two most elevated T-score values on the clinical scales, with at least one scale ≥60 based on the MMPI-A norms. A no-code profile was defined as a profile in which there was no clinical scale T-score ≥60 (Archer, 2017).
Treatment Outcome
The measure of treatment outcome was school attendance after completion of the School Refusal Program and at 1-year follow-up. School attendance information was gathered via telephone in October/November of the new school year (for post-treatment assessment), and again the following October/November (for follow-up assessment). The information was recorded in the School Refusal Program file. At post-treatment and follow-up, adolescents were considered to be “responders” when information gathered during the telephone call indicated that they: (a) did not meet criteria for a concerning level of absenteeism according to Dutch law (i.e., no more than 16 hours unauthorized absence across 4 weeks, which is equivalent to 16–18% of absenteeism; Brouwer-Borghuis et al., 2019), for the 2 to 3 months since the new school year began (i.e., mid-August to October or November);(b) had full-time employment; or (c) attended school part-time and were employed for the rest of the time (McShane et al., 2004). Adolescents not meeting one of these criteria were described as “non-responders.”
Statistical Analyses
Analyses were performed using the Statistical Package for the Social Sciences, version 25.0 (IBM Corp., 2017). Validity scales of all MMPI-A profiles were screened to determine whether these scales were within acceptable ranges to thus permit interpretation of the profiles.
To address the first research question, descriptive statistics were used to describe the personality profiles of the adolescents in terms of mean T-scores for the clinical scales and frequencies of the 2-point code types. Chi-square analyses were used to determine whether adolescents displaying SR scored higher on the clinical scales relative to the normal population, using the following three categories of scores: “low to normal,” “moderately increased,” and “high to very high.” Three categories were used instead of five to avoid empty cells.
To address the second research question, chi-square Fischer Freeman Exact Tests (2-sided) were performed, and odds ratios (OR) were calculated to determine whether personality profiles, based on 2-point code types (independent variable), predicted treatment outcome (i.e., school attendance at post-treatment and 1-year follow-up, as dependent variables).
Results
Personality Traits of Adolescents Presenting With School Refusal
The validity scales of each adolescent’s MMPI-A profile were within the normal range, permitting interpretation of the profiles. Figure 1 presents the mean MMPI-A profile across 41 adolescents.
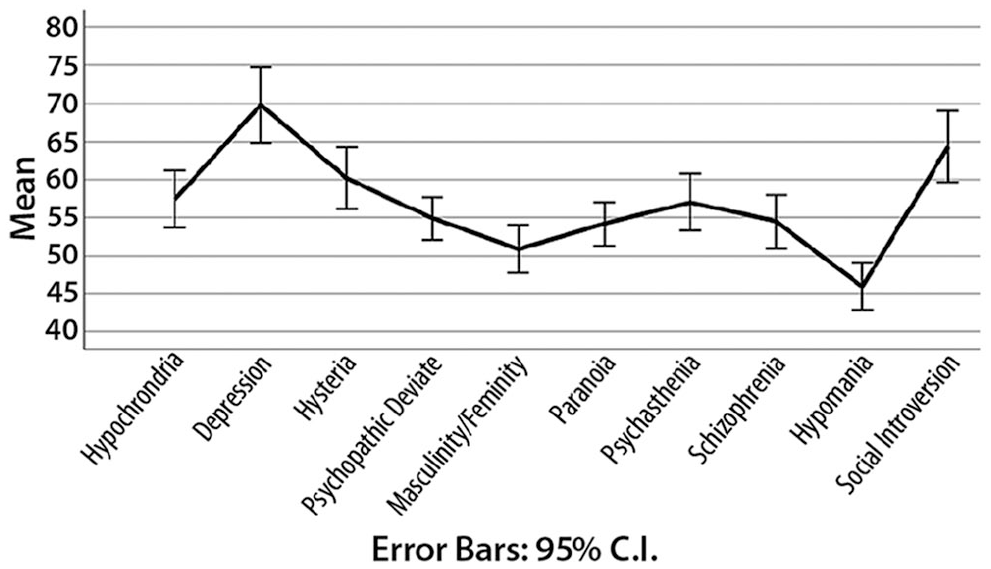
Mean MMPI-A Profile for Adolescents Displaying School Refusal.
To address the first research question, comparisons were made between clinical scale scores for the current sample and the norm group. Significantly increased scores, relative to the norm group, were found on the clinical scales Depression and Social Introversion. The mean T-score on the Depression scale was high (t ≥ 65; confidence interval [CI] 95%, t = 2.38, p = .022). Within the Depression scale, the subscales Subjective Depression and Psychomotor Retardation were moderately increased (t ≥ 60; CI 95%, t = 3.04, p = .004 and t = 3.488, p = .001). The mean T-score on the Social Introversion scale was also moderately increased (t ≥ 60; CI 95% t = 2.32, p = .026) as was the subscale Social Avoidance (t ≥ 60, CI 95%, t = 3.41, p = .002).
When analyzing the ratios between the three categories (i.e., low to normal [< 60], moderately increased [60–64], and high to very high scores [>65]) for each of the 10 clinical scales, it was found that adolescents displaying SR reported significantly higher scores on eight of 10 scales, relative to the norm group. In other words, they reported more serious complaints relative to the normal population (see Table 1).
T-Score Ranges on the MMPI-A Clinical Scales.
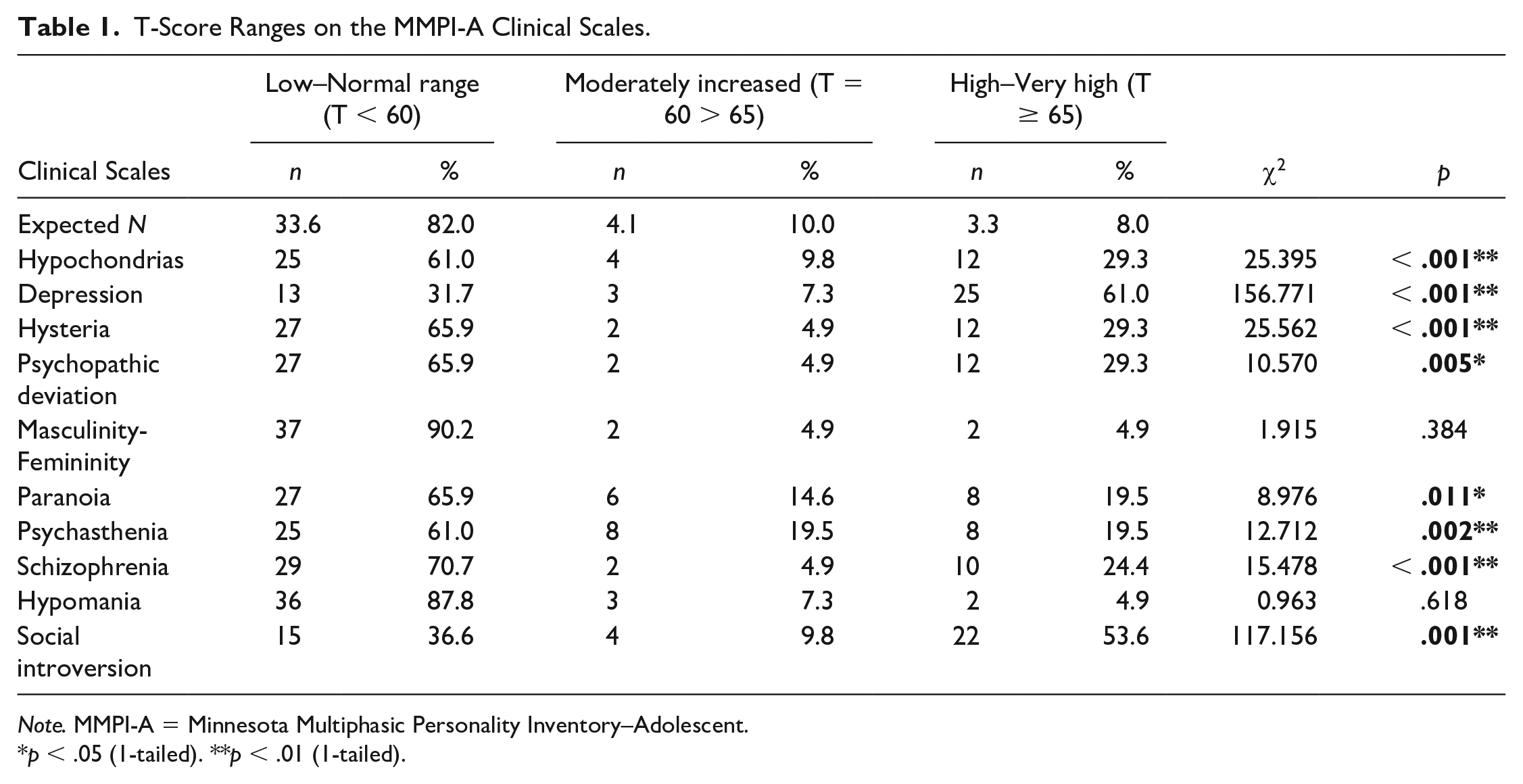
Note. MMPI-A = Minnesota Multiphasic Personality Inventory–Adolescent.
p < .05 (1-tailed). **p < .01 (1-tailed).
Table 2 presents the frequencies of the 2-point code types (i.e., profile classification is based on the two most elevated clinical scales; Archer, 2017). Approximately one-half (54%) of the sample was classified as MMPI-A code type 2-0/0-2 or 2-3/3-2. The most common profile (34% of adolescents) was the 2-0/0-2 code type, which means that Scales 2 (Depression) and 0 (Social Introversion) were the highest clinical scales. This is not surprising given the mean MMPI-A profile presented in Figure 1. The second most common profile (20% of the sample) was the 2-3/3-2 code type, whereby the highest scales were 2 (Depression) and 3 (Hysteria).
MMPI-A Code Type Frequencies for 41 Adolescents Displaying School Refusal.
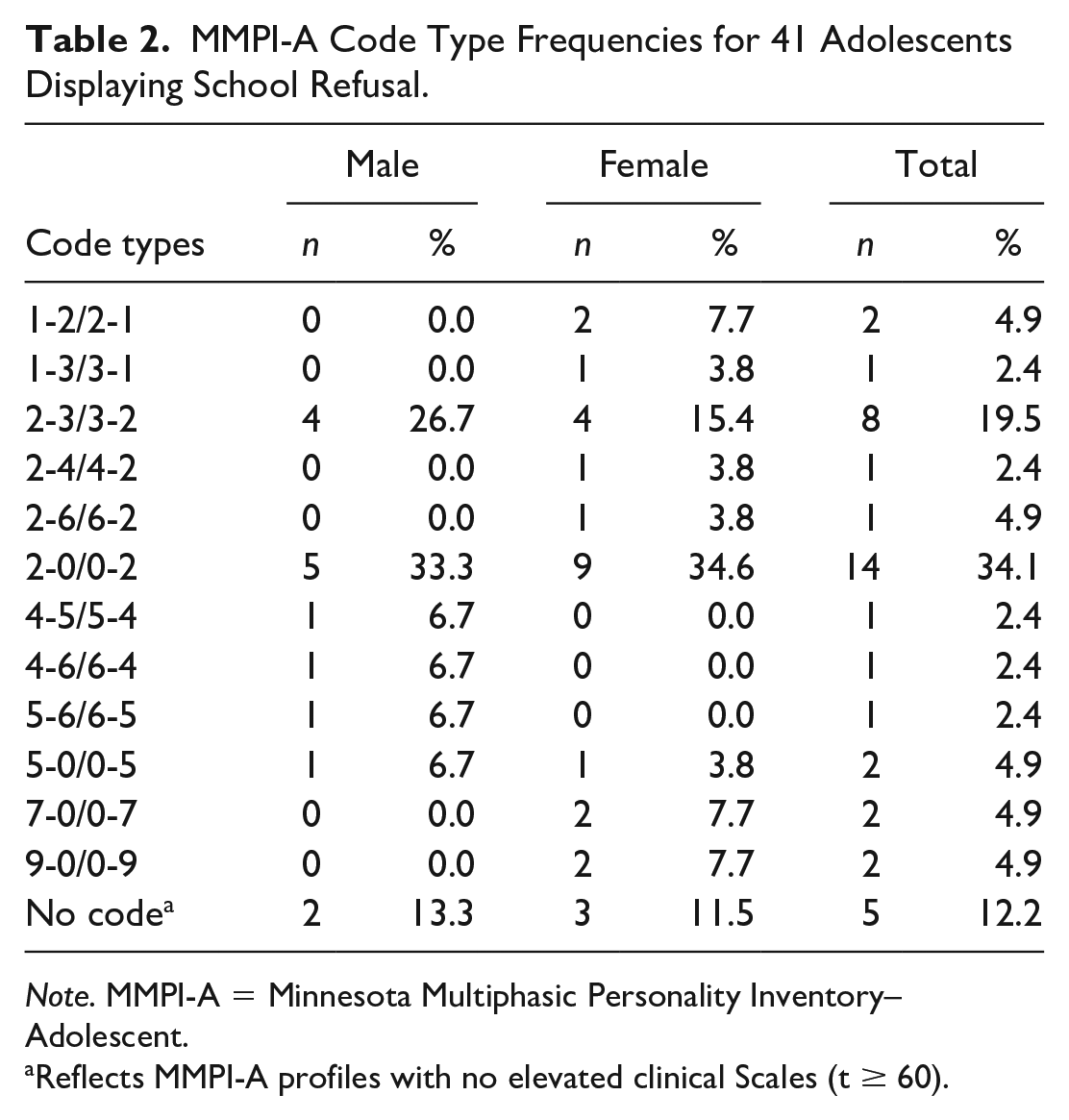
Note. MMPI-A = Minnesota Multiphasic Personality Inventory–Adolescent.
Reflects MMPI-A profiles with no elevated clinical Scales (t ≥ 60).
Personality Traits as Predictors of Treatment Outcome
To address the second research question, single clinical scales and 2-point code types were examined in relation to treatment outcome (“responder” versus “non-responder”) at post-treatment and 1-year follow-up.
At post-treatment, there was no significant difference between adolescents who were classified as responders and those who were non-responders, with respect to T-scores for any of the clinical scales. As presented in Table 3, a relation was found between the 2-point code types and treatment outcome. Adolescents with a 2-0/0-2 code type were significantly more likely to be responders (p = .041) while adolescents with the 2-3/3-2 code type were significantly less likely to respond to treatment (p = .040).
Frequencies of the Code Types in Relation to Treatment Outcome.
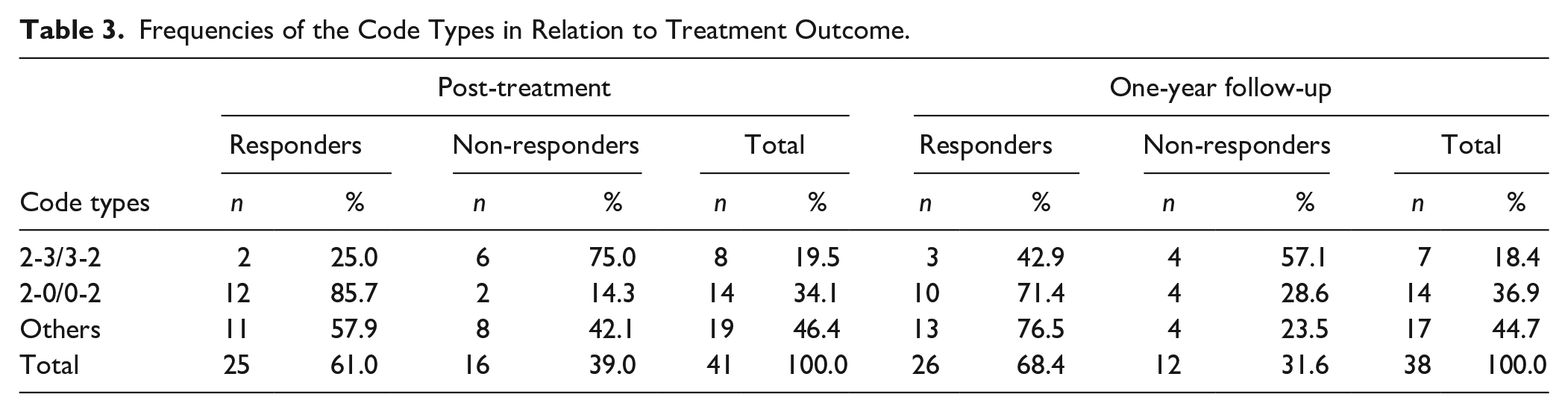
Adolescents with a 2-0/0-2 code type were almost two times more likely to be responders compared with adolescents having all other code types (OR = 1.78, 95% CI [1.140, 2.781]), and this difference was significant. Adolescents with a 2-3/3-2 code type were significantly less likely to be responders, although the odds ratio (OR = .36, 95% CI [.106, 1.216]) was not significant because the confidence interval includes 1.
At 1-year follow-up, information about school attendance was available for 38 (93%) of the 41 adolescents. For 32 (84%) adolescents, treatment outcomes remained stable at the 1-year follow-up. Only two (5%) adolescents who were responders at post-treatment were no longer classified as responders at 1-year follow-up. Four (11%) adolescents, who were classified as non-responders at post-treatment, were classified as responders 1 year later. Regarding the relationship between personality traits and treatment outcome, no significant relations were found between the T-scores of the single clinical scales and treatment outcome at follow-up. Analyzing the code types in relation to treatment outcome, there was no significant difference in treatment outcome at follow-up between the group of adolescents with a 2-0/0-2 code type and all other adolescents with a different code type or no code type (χ2 = .761, p = 1.00). Furthermore, there was no significant difference in treatment outcome at follow-up between the group of adolescents with a 2-3/3-2 code type and all other adolescents (i.e., adolescents with a different code type or no code type; χ2 = .107, p = .176).
Discussion
To our knowledge, this is the first study to use the MMPI-A to investigate personality traits among adolescents with SR, and the first study to examine the relationship between personality traits and the outcome of treatment for SR. Results support the first hypothesis that adolescents presenting with SR would display personality traits differing from a normative group. Significantly increased scores were found on the MMPI-A clinical Scales 2 (Depression) and 0 (Social Introversion). In addition, the most common 2-point code types among adolescents displaying SR were 2-0/0-2 (34% of adolescents) and 2-3/3-2 (20% of adolescents). With respect to the second hypothesis, adolescents with the 2-0/0-2 code type were more likely to be classified as responders at post-treatment, and adolescents with the 2-3/3-2 code type were less likely to be classified as responders at post-treatment. Although there was little change in treatment response between post-treatment and 1-year follow-up, no significant relationship was found between personality traits and treatment outcome at 1-year follow-up.
Interpretation of the Single-Scale Elevations
The findings point to the presence of specific personality traits among adolescents displaying SR. Compared with the expected proportions of youths scoring in the low to normal T-score range, moderately increased range, or high to very high range on the MMPI-A clinical scales, adolescents displaying SR more often had a higher proportion of increased scores on 8 out of the 10 clinical scales. Thus, youths in the current study experienced more affective distress in terms of depression symptomatology and social introversion, observed in the increased scores on clinical Scales 2 and 0. These findings are consistent with earlier findings that social introversion was correlated with school avoidance (Honjo et al., 2001) and that personality traits such as introversion, passivity, and dependent personality were related to persistent SR (Hersov, 1960; Okuyama et al., 1999). In addition, previous studies have shown that a large proportion of adolescents displaying SR experience depressive symptoms (Heyne, 2022).
To better understand the relation between the elevated scales and SR, it is helpful to consider the characteristics of the two scales that were elevated. Scale 2 (Depression) measures adolescents’ general feelings of dissatisfaction with their life situation, lack of hope in the future, and low self-esteem. Although Scale 2 (Depression) is sensitive to state factors (e.g., the adolescent’s emotional state at the time of completing the MMPI-A), it is not regarded as an indication of a depressive mood disorder. Moreover, Scale 2 is often elevated in profiles of youths for whom depression is not the primary diagnosis (Friedman et al., 2014). In our sample, the most common primary diagnoses were anxiety disorders. Moreover, most adolescents had not attended school for at least 6 months. It is conceivable that these youths experienced high levels of stress, reflected in the elevation of this scale, due to the combined presence of an anxiety disorder and school non-attendance. Absence from school can contribute to distress when one realizes that they are not able to do “what all the other kids do” in terms of going to school (Heyne & Sauter, 2013). Scale 0 (Social Introversion) measures the degree of social introversion and is the most stable scale of the MMPI-A, reflecting a biological component and behavioral stability (Friedman et al., 2014). The elevations on this scale may reflect more stable characteristics of social anxiety and social avoidance found to be related to SR (Ingul & Nordahl, 2013).
Interpretation of the 2-Point Code Types
The frequencies of the 2-point code types identified among adolescents in the current sample differ from those found in other samples of adolescents receiving mental health services. For example, frequent code types in the current study included Scale 2 scores (63%, n = 26) and relatively infrequent code types included Scale 4 scores (7%, n = 3). Archer (2005) examined MMPI-A 2-point code types among more than 1,600 adolescents receiving mental health services, finding that code types including Scale 2 were very infrequent (15%) while code types including Scale 4 occurred in more than one-third of the sample. Scale 4 generally reflects a tendency to impulsiveness and to convert inner conflicts into behavior (Archer, 2017; Eurelings-Bontekoe & Snellen, 2017). In the current study, the frequency of these code types suggests that adolescents displaying SR express their feelings of aggression less, are less likely to act impulsively, and feel more inferior, pessimistic, apathetic, and dissatisfied with their situation, compared with the population of adolescents referred to psychiatric settings.
It is also noteworthy that more than half of the adolescents in the current study were classified with a 2-0/0-2 or a 2-3/3-2 code type. Archer (2005) found that a 2-0/0-2 code type occurred among 2% of males and 4% of females in a large sample of adolescents receiving mental health services, whereas 33% of males and 35% of females in the current study were classified with a 2-0/0-2 code type. According to Archer (2017), adolescents with a 2-0/0-2 code type typically present with “problems such as tension and anxiety, apathy, shyness, lethargy, and excessive interpersonal sensitivity” (p. 185). He also noted that teenagers with the 2-0/0-2 code type were, as children and then as adolescents, “meek, socially isolated loners who conform to parental demands and who do not engage in alcohol or drug abuse” (p. 185). These youths expressed “feelings of inferiority, social rejection, and a self-perception of unattractiveness” and the primary defense mechanisms included “social withdrawal, denial, and obsessive-compulsive mechanisms” (p. 185). Moreover, many were noted to lack social skills. Based on these descriptions, it is conceivable that the adolescents in the current study who had a 2-0/0-2 code type had poor school attendance as a result of a primary defense mechanism that involves protecting those parts of themselves characterized by a lack of social skills and feelings of inferiority. Indeed, the inherently social nature of the school is argued to contribute to absenteeism among those with social concerns (Blöte et al., 2015).
The 2-3/3-2 code type occurred among 27% of males and 15% of females in the current study, compared with 2% of males and 4% of females in the general psychiatric population of adolescents (Archer, 2005). According to Friedman et al. (2014), those with this code type have difficulty expressing negative emotions in a direct way. In particular, expressing anger or being confronted with anger yields much stress. They also suggested that hypochondria and somatization are common defense mechanisms for these youths to repress their negative feelings. Archer (2017) described adolescents with a 2-3/3-2 code type as emotionally overcontrolled, noting that the adjectives frequently applied to these individuals include “passive, docile, and dependent” (p. 181). Furthermore, “the majority of these adolescents were referred for treatment because of poor peer relationships,” they were seen as anxious students who were socially isolated and had few friends inside the school environment (p. 141). These personality traits are consistent with the behavioral presentation of youths displaying SR, but they also help explain the problems that SR youths can have with respect to emotion regulation, whereby emotions are suppressed such that their emotional distress is difficult to observe (Hughes et al., 2010). For example, the feelings of anxiety observed among youths in the current study with a 2-3/3-2 code type could be considered a defense mechanism to suppress feelings of anger.
Similarities and Differences Between the Common 2-Point Code Types
The two most common code types observed in this study (i.e., 2-0/0-2 and 2-3/3-2) share similar personality traits. Both code types refer to passive and socially isolated adolescents who present as socially insecure, withdrawn, and having difficulties connecting with peers. However, the function served by social avoidance appears to differ across the two code types. Within the 2-0/0-2 code type, social avoidance seems to arise from a degree of social disability and a degree of introversion, with little desire to engage in large groups. Within the 2-3/3-2 code type, the social avoidance is related to a fear of confrontation with anger/hostility when in contact with others and within oneself, and avoidance is related to a fear of rejection. Thus, despite similarities in the presentation of symptoms, different treatment approaches are recommended for each code type (Friedman et al., 2014). This is consistent with Lounsbury and colleagues’ (2004) recommendation that particular personality profiles may help to tailor interventions for school absenteeism. These authors imply that personality traits have an influence on absenteeism that may exceed environmental influences such as “school, classroom, teacher, neighbourhood, or community” (p. 464). Because personality characteristics are less stable in adolescence, there may be ample scope for personality change (Lounsbury et al., 2004), so attention to traits during treatment may benefit treatment outcome.
Two-Point Code Types in Relation to Treatment Outcome
In line with the second hypothesis, we found that personality traits were related to treatment outcome at post-treatment. Adolescents with a 2-0/0-2 code type were significantly more likely to be responders. Adolescents with the 2-3/3-2 code type appear to be less likely to respond to treatment based on chi-square results but not based on effect size (odds ratio). In prior research, inpatient adolescents with a high score on Scale 2 were found to be motivated for psychotherapy and openly discussed their perceptions and feelings (Archer, 2017). Given that Scale 2 may bode well for treatment outcome, it would seem to be the combination of high scores on Scales 2 and 3 which may confer inferior treatment outcome.
In view of the similarities and differences between code types 2-0/0-2 and 2-3/3-2 as presented above (Similarities and Differences Between the Common 2-Point Code Types), it appears that the function of (social) avoidance—which is different between these two code types—could explain the seeming difference in outcome at post-treatment. For individuals with a 2-3/3-2 code type, the fear of losing control of their emotions, fear of confrontation with anger, and fear of rejection are so high that they repress their own negative emotions and display avoidant behavior in an effort to repress these emotions. The habit of suppressing negative emotions can make individuals unaware of their own thoughts and emotions, especially those related to anger, because they release their negative feelings by somatization (Friedman et al., 2014). It is thus conceivable that adolescents with a 2-3/3-2 code type will benefit less from standard CBT for SR because of the nature of CBT. Studies have found that cognitive and emotional skills, especially introspective ability, emotion regulation skills, emotion recognition, and emotion differentiation, are important for understanding and applying CBT (Kingery et al., 2006; Suveg et al., 2009). For individuals with a 2-0/0-2 code type, the tendency to conform to expectations could positively influence their treatment commitment and thus treatment outcome.
At 1-year follow-up, there was no relationship between personality traits and treatment outcome. The lack of a relationship at 1-year follow-up might be attributed to the smaller sample size at follow-up. It is also possible that during the year-long period after treatment concluded, factors other than personality traits came to have a strong influence on school attendance, such as poor academic achievement (Aucejo & Romano, 2016; Gershenson et al., 2017; Gottfried, 2014), problematic family functioning (Heyne & Sauter, 2013), and peer relationships (Havik et al., 2015b).
Strengths and Limitations
The current study employed a robust measure of personality, the MMPI-A. It is the most frequently used instrument for objective personality assessment with adolescents (Archer, 2017). By using the code types of the MMPI-A profiles we were able to conduct a nuanced analysis of personality traits among adolescents displaying SR.
Treatment outcome was evaluated at post-treatment as well as at 1-year follow-up, a longer follow-up period relative to other studies of treatment for SR (e.g., Heyne et al., 2011; Wu et al., 2013). It is also noteworthy that data were collected within a CAMHS setting. Data gathered in the context of real-life practice are likely to offer a more representative picture of how adolescents displaying SR respond to treatment, relative to outcome data derived from studies conducted in research-based settings (Johnsen et al., 2021).
Several limitations of the study warrant consideration. First, while the 2-0/0-2 and 2-3/3-2 code types contributed to a nuanced understanding of the relationship between personality traits and SR, these code types did not apply to almost one-half of the sample. For the adolescents for whom these code types did not apply, the relation between SR and personality traits is still unclear. Second, this was a retrospective study based on available data. Some school attendance data were missing, there was no predetermined plan regarding sources and timeframes for data gathering as per recent recommendations (Heyne et al., 2020), and variability in therapists and length of treatment can influence the outcome. Third, the generalizability of the results is limited because we studied a small sample of adolescents presenting to a single CAHMS setting servicing one part of the Netherlands.
Clinical and Research Implications
More than one-half of adolescents presenting to a mental health service with SR could be classified with a 2-0/0-2 or 2-3/3-2 code type measured by the MMPI-A, and results indicated that adolescents with the 2-0/0-2 code type responded better to treatment (CBT plus other interventions) than adolescents with the other code types. Individuals with the 2-3/3-2 code type responded less favorably based on chi-square results but not the OR. By using the MMPI-A when assessing adolescents presenting with SR, therapists can gain a better understanding of the role that presenting symptoms such as avoidant behavior, social isolation, shyness, and emotion regulation might play in the development or maintenance of SR.
This knowledge can help therapists tailor the treatment they offer. Friedman et al. (2014) recommended that when working with individuals with the 2-3/3-2 code type, an initial investigation of emotional awareness should be sensitively conducted (i.e., with a patient tempo). This allows more time for individuals with this code type to become aware of their negative emotions, so as to be able to experience them and work on them. Extending this recommendation, it seems that if the therapist is not aware of this personality trait and the adolescent is confronted too quickly with their negative emotions, there is a risk that the adolescent will feel rejected and drop out of therapy. In effect, the adolescent displaying SR also displays a refusal to attend therapy.
Within the 2-0/0-2 code type, the constitutional trait of shyness plays an important role in avoidant behavior. Adolescents with this code type are aware of the stress they experience in social situations. Because their emotional awareness is more developed, the therapist can work more congruently with the negative emotions of adolescents with a 2-0/0-2 code type. Thus, it is conceivable that CBT will be more suited to adolescents with this code type. Indeed, Archer (2017) recommended the use of CBT with these youths, to reduce depressive symptoms, in addition to social and assertiveness skills training to deal with shyness. Thus, the therapist’s understanding of the influence of personality traits in cases of SR, based on the use of the MMPI-A, could enhance the effectiveness of CBT when applied to this group of adolescents much in need of effective intervention (Last et al., 1998).
From a research perspective, it is evident that further attention to personality traits among adolescents displaying SR is needed. The MMPI-A could be implemented in larger studies with more power to detect the influence of personality traits on long-term outcomes. Within such studies, outcome variables not included in the current study warrant attention, such as relationships with friends and quality of life (McKay-Brown et al., 2019). Fundamental research is also required, whereby MMPI-A data are used to develop and test theories of the development and maintenance of SR. As noted by Lounsbury et al. (2004), the relative effects of personality and environmental influences on school absenteeism need to be studied.
Conclusion
This study supports the occurrence of particular personality traits among adolescents displaying severe SR, based on MMPI-A T-scores on the clinical scales and 2-point code types. More than half of the group could be described as displaying a 2-3/3-2 or a 2-0/0-2 code type. This study also provides preliminary support for the role of personality traits in treatment outcome. Adolescents with a 2-0/0-2 code type were more often classified as responders at post-treatment and those with a 2-3/3-2 code type were less often classified as responders at post-treatment based on chi-square results. While further research is needed to confirm these findings, the results suggest that some youths displaying SR—especially those with the MMPI-A 2-3/3-2 code type—may benefit from forms of therapy additional to CBT for SR, such as psychotherapy focused on emotional awareness.
Footnotes
Data Availability
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.