
Abstract
The relative contribution of long-term acute care hospital (LTACH) to short-term acute care hospital (STACH) Medicare patient readmissions is important because of the high acuity of LTACH patients. A retrospective cohort study was conducted to determine the magnitude of LTACH Medicare heart failure (HF) and pneumonia (PN) inpatient readmissions to STACHs within 30 days of LTACH admission and the relative contribution of LTACH patient readmissions to each STACH’s total readmissions. Seventy-five for-profit LTACHs and their associated host or primary referral STACHs were studied. An average of 8% HF and 8% PN LTACH Medicare inpatients were readmitted to host or primary referral STACHs within 30 days of admission, representing 0.4% and 0.8% of the total number of HF and PN Medicare patients, respectively, readmitted to the STACHs in fiscal year 2010. The low rates of readmission from LTACHs to STACHs suggest an appropriate level of care for the LTACHs studied.
Reduction of readmissions to short-term acute care hospitals (STACHs) has been a major focus related to health care quality from policy makers, Medicare, health care providers, and the general public. Approximately 20% of all Medicare patients are readmitted to STACHs within 30 days of hospital discharge and represent 17% of total Medicare hospital spending. 1 In general, readmissions may be the result of poor quality of care transitions—patients may not have been ready for discharge, there was a lack of postdischarge planning, or the quality or capability of the discharge destination was not appropriate or adequate. 2 In an attempt to improve the quality of care associated with Medicare beneficiaries, the Centers for Medicare & Medicaid Services (CMS) has implemented payment penalties for STACHs based on higher-than-expected rates of 30-day, all-cause readmission for patients with 3 medical conditions: heart failure (HF), pneumonia (PN), and acute myocardial infarction (AMI).3,4 The financial penalty associated with high readmission rates has resulted in an increased provider focus on the care transition process.5-7
Some patients are readmitted to STACHs within 30 days because of factors not related to the initial STACH stay, the quality of care, or the quality of the transition process. 8 This can be especially true for patients with high acuity 9 or critically ill patients who do not completely recover during the STACH stay. Long-term acute care hospitals (LTACHs) specialize in the treatment of patients who require long-term acute care services for chronic critical illness, a syndrome of prolonged dependence on intensive care therapies such as mechanical ventilation, for complex medical issues such as multiorgan or multisystem failure, postsurgical or organ transplant complications, complex wounds, multiple injuries, and brain injury. LTACH patients are transferred back to STACHs when surgeries or selected tests are required, or when extreme medical conditions occur.
Few studies have compared the relative proportion of STACH readmissions from different discharge health care settings. 10 The aim of the present study was to assess the relative number of LTACH Medicare inpatients readmitted to STACHs within 30 days of discharge and to determine the impact of LTACH to STACH inpatient readmissions for HF and PN patients using published STACH data and proprietary LTACH data (Select Medical, unpublished data, January 31, 2012). AMI readmissions were not studied because the number of AMI patients discharged from STACHs to LTACHs was insufficient for accurate statistical analysis.
Methods
STACH readmission is typically measured from an “index hospitalization,” which is the first STACH hospitalization for a particular clinical condition; subsequent admissions within a specified time period after the index hospitalization are considered readmissions. 11 Because the Medicare Provider Analysis and Review (MedPAR) data file used did not allow identification of the STACH index hospitalization for each patient, a conservative approach was adopted that counted all readmissions (including discharges) to STACH occurring within 30 days of LTACH admission as a STACH readmission. On average, 97% of the study LTACH patients were admitted directly from STACHs.
Data Sources
Three data sources included the following: (a) the fiscal year (FY) 2010 MedPAR data file, consisting of claims data for services provided to beneficiaries admitted to all Medicare-certified inpatient hospitals; (b) a proprietary LTACH admission-discharge-transfer (ADT) database containing FY2010 data from 75 LTACHs (29 freestanding and 46 Hospital-within-Hospital [HwH] LTACHs); and (c) the CMS Hospital Compare database, which contains STACH readmission rates for HF, PN, and AMI patients. 12 STACHs were selected for analysis if they were either a host hospital for the study HwH LTACHs or if they were the primary referral source for the study freestanding LTACHs.
STACH MedPAR Data
The MedPAR database contains indicators for hospital identification, primary and comorbid diagnoses, discharge destination, length of stay, and other claims-related variables. For each STACH, HF and PN patients were identified in the MedPAR FY2010 database by identifying the presence of HF or PN primary diagnosis International Classification of Disease, Ninth Revision (ICD-9) codes. The absence of patient identifiers in the MedPAR database used in this study prevented HF and PN patients identified in the LTACHs from being matched with their STACH stay. The STACH discharge-to-LTACH indicator in the MedPAR database was not used because it was found to be inaccurate, similar to previous studies. 13
CMS Hospital Compare Data
The CMS Hospital Compare database contains risk-standardized readmission rates (RSRR) for each STACH for 3 diagnoses (HF, PN, and AMI). The RSRR is the ratio of predicted-to-expected number of readmissions multiplied by the national unadjusted readmission rate for each diagnosis. Predicted and expected readmissions are calculated based on case mix and patient age for each STACH and an “average” STACH. The STACH RSRR rates available are representative of a more recent time frame than FY2010; however, the confidence interval (CI) for each STACH RSRR, which is included in the CMS Hospital Compare database, includes variability of the RSRR during FY2010.
There are 3 groups of STACHs in this study: (a) STACHs that are either the host or primary referral STACH for the study LTACHs; (b) nonhost and nonprimary STACHs that also provided patients to the study LTACHs, and (c) a random group of STACHs that did not provide patients to the study LTACHs. The first 2 groups of STACHs were identified based on their association with the study LTACHs; the third group of STACHs that did not provide patients to the study LTACHs (N = 75) were randomly selected from a pool of STACHs that met the minimum criteria of at least 90 beds, the presence of HF and PN patients, and a minimal proportion (>0.4%) of patients discharged to LTACH (determined from MedPAR discharge destination data, although the actual percentage was not used in any calculations).
LTACH Data
Admission from and readmission to STACH were identified for each patient from the LTACH ADT data. Initially, 75 LTACHs were available for study; LTACHs were eliminated from further study if they had fewer than 8 HF and 8 PN Medicare admissions during FY2010. For HwH study LTACHs (N = 46), an average of 49% of the patients came from the host STACH and 51% of the patients came from other, nonhost STACHs. For freestanding study LTACHs (N = 29), an average of 43% of the patients came from 1 STACH that was identified as the primary referral STACH. Although administrative data may contain inaccuracies, 14 LTACH HF and PN Medicare patients admitted from STACHs were identified based on whether they had an admitting HF or PN ICD-9 diagnosis, a primary HF or PN ICD-9 diagnosis, or a comorbid present-on-admission HF or PN ICD-9 diagnosis in the LTACH, based on the ICD-9 codes that CMS uses to determine STACH readmission rates. 15 A small proportion of LTACH patients had a primary diagnosis of HF or PN present on admission (1% and 4%, respectively); most LTACH patients had HF or PN as comorbid present on admission conditions (13% and 18%, respectively). Patients who died in the LTACH were not removed from counts of HF and PN admissions. The average LTACH length of stay of HF and PN patients was 26.7 days, resulting in an average of 20% of HF and PN LTACH Medicare patients from referring STACHs being discharged after the 30-day readmission cutoff; these patients were not included in the analysis.
Analysis
HF and PN LTACH Medicare inpatients admitted from STACHs and readmitted to any STACH within 30 days of LTACH admission were counted as readmissions. STACH readmission was further defined as all patients with either a final discharge destination of STACH or at least 1 interrupted stay between 4 and 9 days. Read-mission calculations that count each readmission event, rather than a count of patients who readmitted, could be larger because some patients had multiple readmissions. The patient-based readmission count was selected because it is closest to the methods used in the calculation of the CMS RSRR, which counts only 1 readmission per patient within a 30-day window after STACH discharge. For each STACH associated with a study LTACH, the estimated number of total STACH readmissions for HF and PN patients from all discharge destinations was first calculated by multiplying each STACH-specific HF and PN RSRR by the number of HF and PN patients, respectively, identified from FY2010 MedPAR data. A ratio of the number of readmissions from LTACHs to STACHs divided by the estimated number of total STACH readmissions from all discharge locations was calculated for each STACH–LTACH pair. This ratio represents the relative impact of LTACH readmissions on the total population of patients readmitted to these STACHs. The estimated total number of HF and PN readmits was used as the denominator of the readmission impact ratio for each STACH.
Results
STACHs
It is possible that differences in STACH hospital characteristics could account for differences in readmission impact. On average, there was no difference in the proportion of Medicare patients or the PN readmission rate between the host/primary STACH group and STACHs that did not provide patients to the study LTACHs (Tables 1 and 2). However, host/primary referral STACHs had proportionately more HF patients, higher case-mix index, higher bed count, fewer PN patients, a lower HF patient readmission rate, and longer overall lengths of stay (for all patients) than STACHs not associated with study LTACHs (Tables 1 and 2). Specifically, host/primary referral STACHs had significantly longer PN patient length of stay (mean = 7.12 days) than STACHs not associated with study LTACHs (mean = 6.72 days), F(1, 148) = 6.236, P = .035 (data not shown).
STACH Demographics for 75 STACHs Associated With Study LTACHs and 75 STACHs Not Associated With Study LTACHs. a
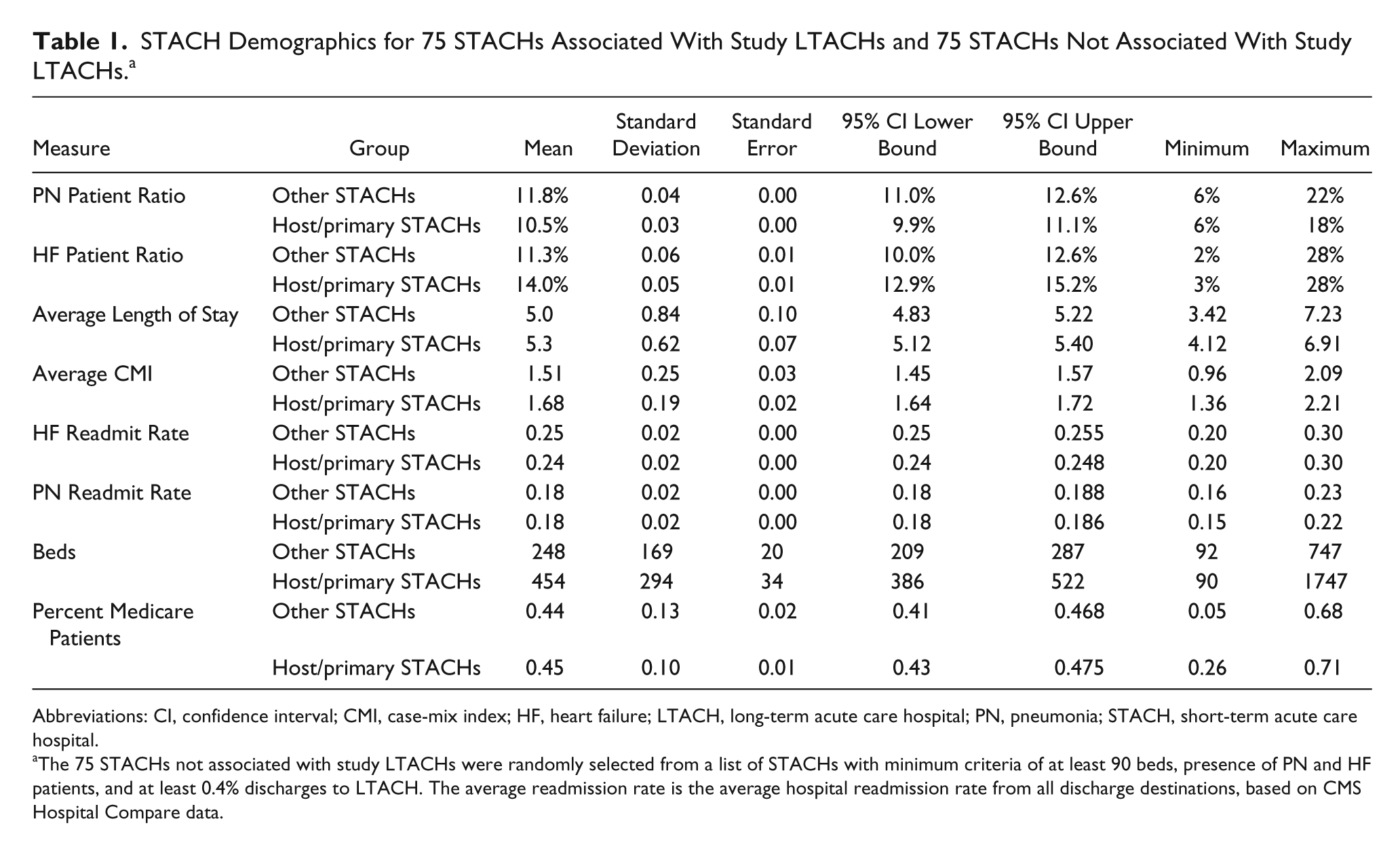
Abbreviations: CI, confidence interval; CMI, case-mix index; HF, heart failure; LTACH, long-term acute care hospital; PN, pneumonia; STACH, short-term acute care hospital.
The 75 STACHs not associated with study LTACHs were randomly selected from a list of STACHs with minimum criteria of at least 90 beds, presence of PN and HF patients, and at least 0.4% discharges to LTACH. The average readmission rate is the average hospital readmission rate from all discharge destinations, based on CMS Hospital Compare data.
Differences Between 75 STACHs Associated With Study LTACHs and 75 STACHs Not Associated With Study LTACHs. a
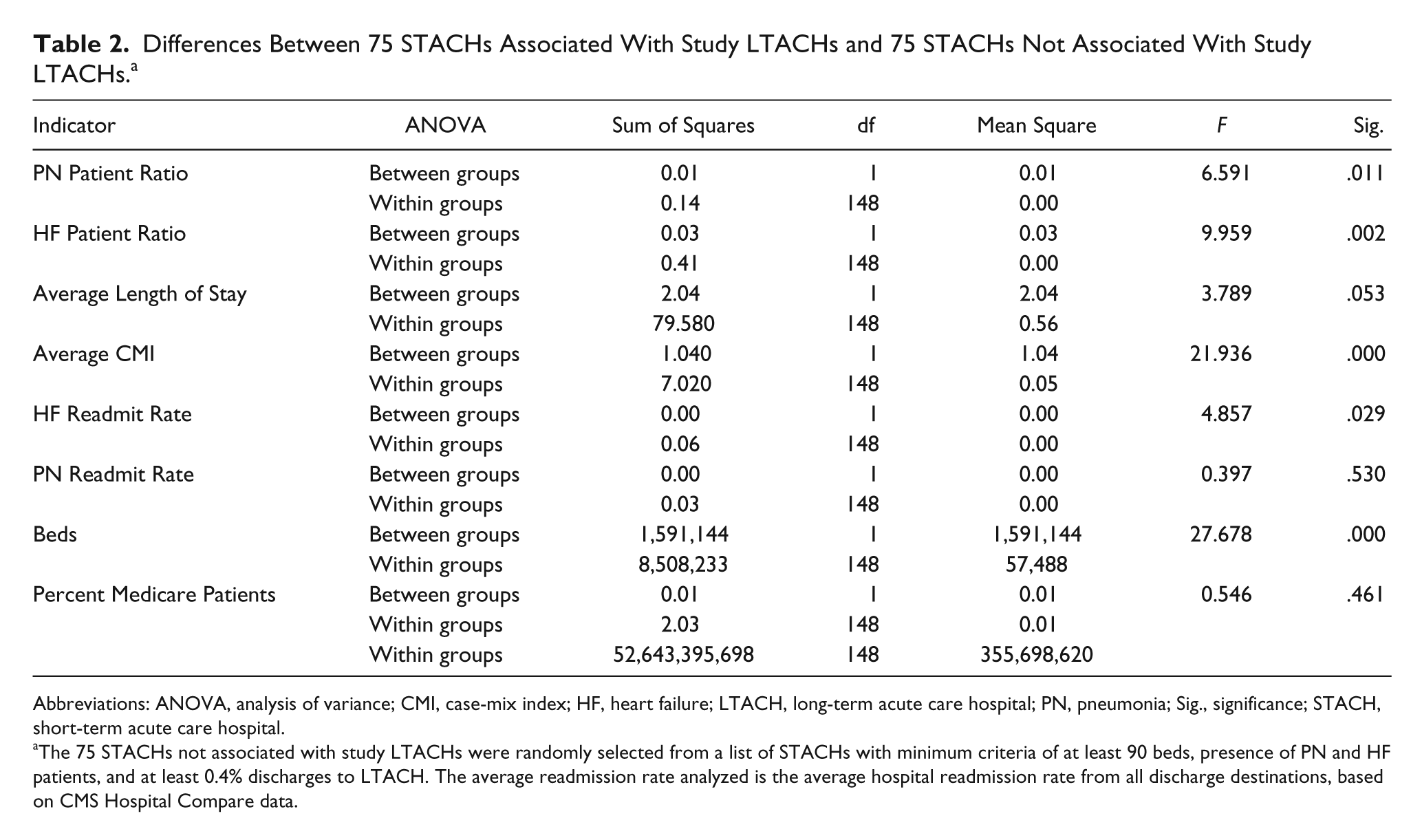
Abbreviations: ANOVA, analysis of variance; CMI, case-mix index; HF, heart failure; LTACH, long-term acute care hospital; PN, pneumonia; Sig., significance; STACH, short-term acute care hospital.
The 75 STACHs not associated with study LTACHs were randomly selected from a list of STACHs with minimum criteria of at least 90 beds, presence of PN and HF patients, and at least 0.4% discharges to LTACH. The average readmission rate analyzed is the average hospital readmission rate from all discharge destinations, based on CMS Hospital Compare data.
The related-samples Wilcoxon signed rank test resulted in no significant differences in overall, HF, or PN readmission rates between host/primary referral STACHs and STACHs that also provided patients to the study LTACHs (95% significance level [Overall: 1, 75, P = .080; HF patients: 1, 44, P = .244; PN patients: 1, 35, P = .717]). Except for the number of beds, Mann–Whitney U tests determined that there was no significant difference between STACHs that had HwH study LTACH associations and STACHs that had freestanding study LTACH associations for any of the hospital characteristic measures; STACHs with HwH, mean beds = 421; STACHs with freestanding association, mean beds = 516, z = −2.416, P < .05. In addition, results of a Mann–Whitney U test showed no significant difference in readmission rates overall or for HF and PN patients between HwH LTACHs and freestanding LTACHs from either host/primary STACHs or from other STACHs; overall host/primary STACH, z = −0.713, P = .476; overall other STACH, z = −0.256, P = .798; PN host/primary STACH, z = −1.384, P = .166; PN other STACH, z = −0.650, P = .516; HF host/primary STACH, z = −0.722, P = .470; HF other STACH, z = −0.766, P = .444.
The Study LTACHs
The 75 study LTACHs varied in size: the smallest LTACH had 20 beds and the largest LTACH had 158 beds, with a median bed size of 36 and an average bed size of 45. Overall, STACHs associated with study LTACHs transferred an average of 147 Medicare patients, and of those, on average, 29 were HF and 39 were PN patients (Table 3). The average LTACH case-mix index, calculated from Medicare long-term care Medicare severity diagnosis related-group (MS-DRG) payment weights for patients admitted from associated STACHs was 1.07 (95% CI = 1.03, 1.10).
The Study LTACH Patient Population and LTACH-to-STACH Readmission Summary.
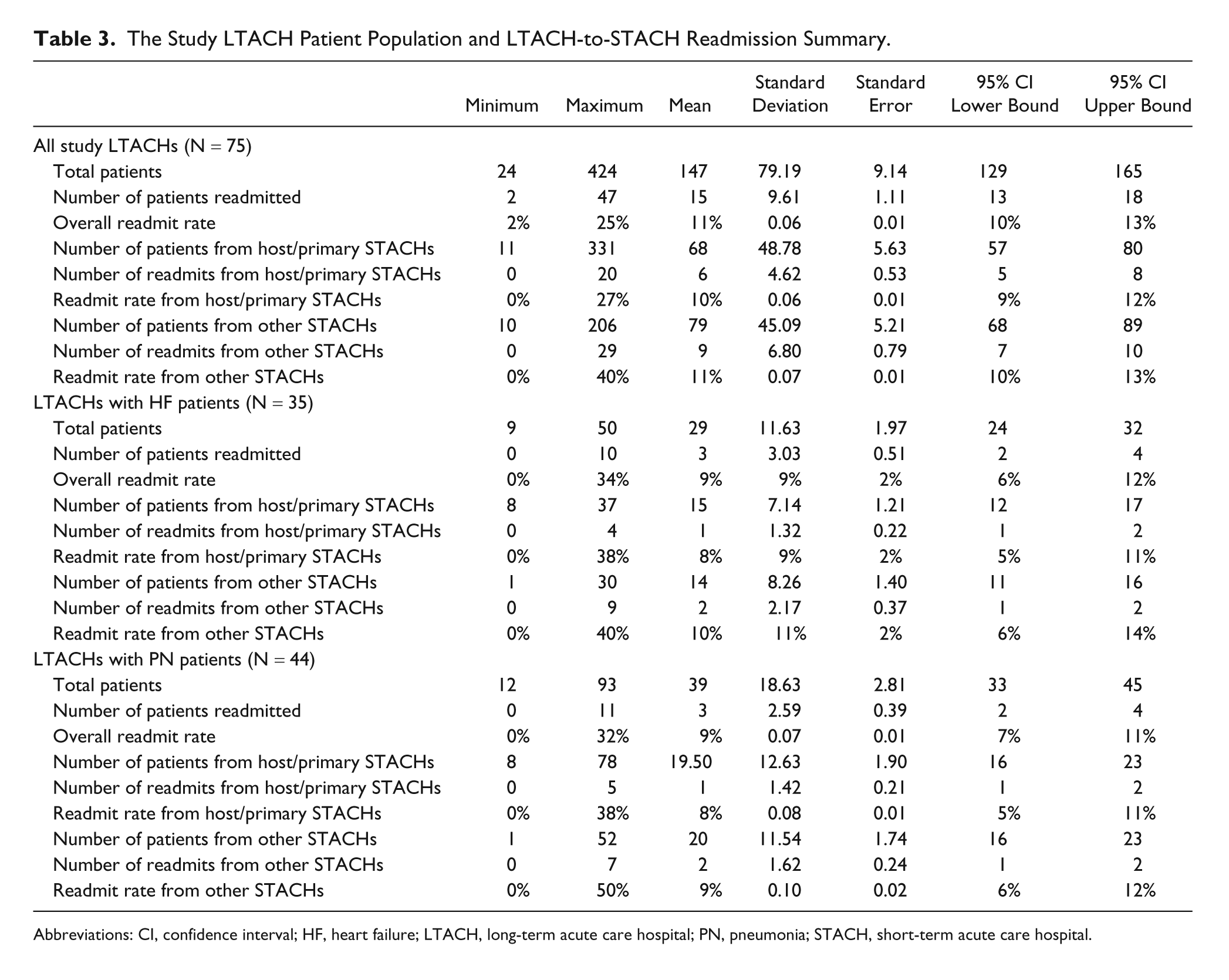
Abbreviations: CI, confidence interval; HF, heart failure; LTACH, long-term acute care hospital; PN, pneumonia; STACH, short-term acute care hospital.
The average number of readmissions to STACH for the study LTACHs is shown in Table 3, which includes counts and rates for HF and PN patients admitted and readmitted from host/primary referral STACHs and from other STACHs. Because of sample size requirements, if a study LTACH had fewer than 8 HF or PN Medicare patients admitted from host/primary referral STACHs in FY2010, the LTACH was not included in further analyses. On average, overall, the study LTACHs readmitted 10% of host/primary referral STACH Medicare patients and 11% of other STACH Medicare patients; a histogram showing the distribution of overall readmission rates for the study LTACHs is shown in Figure 1.
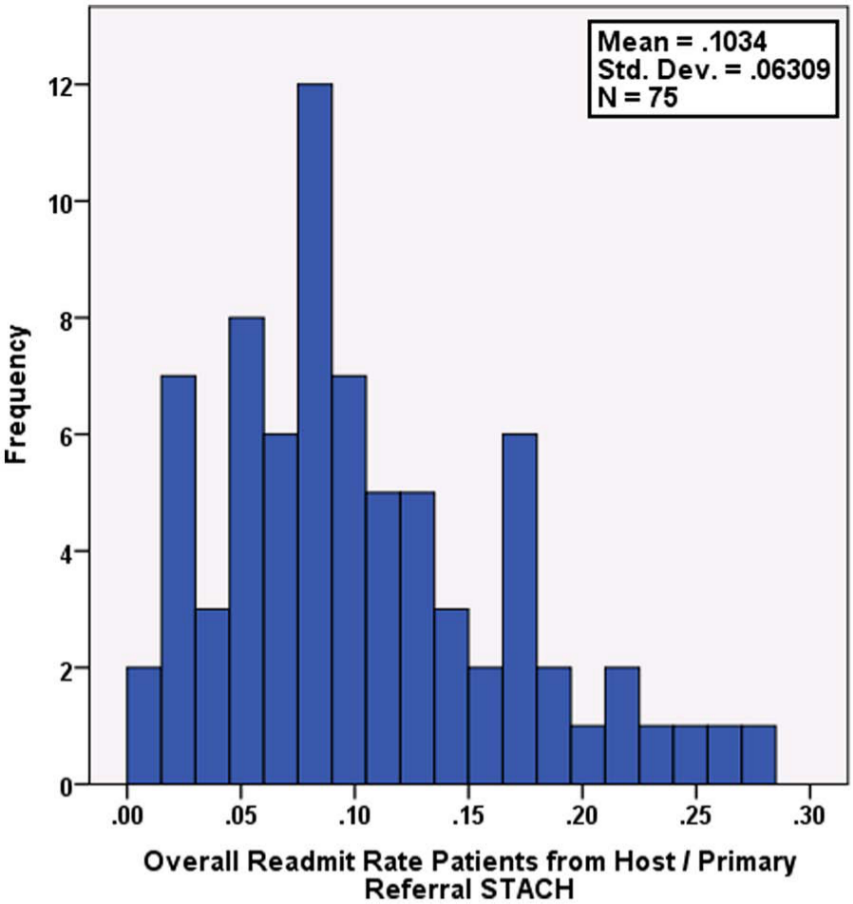
Distribution of overall 30-day readmission rates for each study LTACH; rates are for patients admitted only from each LTACH’s host or primary referral STACH.
Spearman’s ρ revealed a statistically significant correlation between LTACH readmission rates for patients from host/primary referral STACHs and LTACH case-mix index, rs(75) = .262, P < .05, indicating that higher LTACH readmission rates (relative to the low rates observed) are associated with higher case-mix index. Within individual LTACHs, there was a significant correlation between their readmission rate for patients from their host/primary referral STACH and their readmission rate for patients from other STACHs, rs(75) = .669, P < .01. However, a Wilcoxon signed rank test showed no significant difference in readmission rates from each LTACH based on the type of referring STACH (host/primary vs other), z = −1.72, P = .085; the mean of ranks with readmit rates higher for host/primary referral STACHs was 39.7, and the mean of ranks with readmit rates lower for host/primary referral STACHs was 34.45.
Readmission Impact
Three (4%) of the STACHs associated with the study LTACHs and 3 (4%) of the STACHs not associated with study LTACHs had values above the range (according to the CMS definition) of readmissions for HF and PN patients, determined by the presence of overlap between the RSRR upper bound (confidence interval) and the national crude readmission rate, which was 0.248 for HF and 0.184 for PN. Nine STACHs (12%) associated with study LTACHs had readmission rates for HF patients that were outside the lower bound of the confidence interval for all STACH HF readmission; 4 (5%) STACHs had readmission rates for PN patients that were below the lower bound of the confidence interval for all STACH PN readmission. Two STACHs (3%) not associated with study LTACHs had readmission rates lower than the national average for HF patients; no STACH had a readmission rate lower than the confidence interval for PN readmission. For STACHs associated with study LTACHs, the average 30-day HF RSRR was 0.243 (for patients discharged to all locations); the average STACH 30-day PN RSRR was 0.183 (Tables 1 and 2).
An average of 8% of HF and PN patients admitted to the study LTACHs from host/primary STACHs were readmitted to a STACH within 30 days. Slightly higher readmission rates of 10% and 9% were observed for HF and PN, respectively, from other STACHs not studied that provided patients to the study LTACHs; however, only the HF readmit rate was significantly different between these STACH groups.
The impact of the number of patients readmitted from LTACH to the host/primary referral STACH was calculated by dividing the total number of patients readmitted from each LTACH by the total number of patients readmitted to the associated STACH from all other sources. For HF patients, LTACH-to-STACH readmissions comprised 0.4% (95% CI = 0.2%, 0.5%) of the estimated total number of HF patients readmitted to STACHs that were associated with the study LTACHs (mean number of readmits from all sources per STACH = 256, 95% CI = 221, 292). For PN patients, LTACH-to-STACH readmissions comprised 0.8%, (95% CI = 0.6%, 1.1%) of the estimated total number of PN patients readmitted to host/primary referral STACHs (mean number of readmits from all sources per STACH = 148, 95% CI = 124, 171).
Discussion
Readmission rates from LTACH to STACH for Medicare HF and PN patients were lower than readmission rates observed in previous studies using MedPAR data. 16 The low readmission rates observed for the study LTACHs could be because of similar practice patterns resulting from the single corporate ownership structure of the LTACHs; additionally, the large number of LTACHs examined in the present study represents 18% of all LTACHs in the industry, constituting a statistically valid sample. On average, the study LTACHs readmitted to STACHs 10% of all patients admitted from host/primary referring STACHs and 11% of patients referred from other nonhost or nonprimary referring STACHs. The low rates were not because of the relative number of HwH LTACHs, as shown by the lack of a significant difference between readmission rates for the 2 types of LTACH settings. It is also unlikely that the total number of STACH readmissions from all discharge locations was overestimated, because the same ICD-9 and DRG codes were used to identify HF and PN patients in the MedPAR STACH and the LTACH ADT data sets, using primary and secondary present-on-admission HF and PN diagnoses. Including patients who died in the denominator of total admissions might change the readmission rate from the LTACH perspective; however, it does not change the impact of the readmissions on the total number of patients readmitted to STACHs. The average length of stay of HF or PN patients who died was more than 20 days, which afforded some opportunity for readmission within the 30-day window.
Differences were observed between the STACHs associated with the study LTACHs and STACHs not associated with the study LTACHs. Further study is necessary to determine whether having an associated LTACH affects STACH length of stay and readmission rates for different groups of LTACHs. The pseudorandom group of 75 STACHs used for comparison in the current study was selected based on several criteria, including 90 beds or greater, treatment of PN and HF patients, and a minimal number of patients discharged to LTACHs. STACHs associated with the study LTACHs had a significantly higher case-mix index and longer average length of stay than STACHs not associated with the study LTACHs, possibly reflecting higher patient acuity. It is possible that the single corporate ownership of the study LTACHs resulted in a biased selection of associated STACHs that have a relatively higher proportion of more severe patients requiring LTACH services. Further matching of STACHs based on more stringent criteria may provide an interpretation of the differences observed between the STACH groups.
The observed significant correlation between readmission rates and case-mix index is not surprising,17,18 although it is a unique finding for the LTACH setting, which could account for some of the observed variability in overall readmission rates among the LTACHs studied. For both HF and PN patients, the low 30-day STACH readmission rates from the study LTACHs could be interpreted to be a result of high-quality care, the absence of nonclinical factors contributing toward readmissions, the medical and technical capability to handle emergent medical conditions within the LTACH, or some combination of such factors. Because many LTACH patients stay longer than 30 days, further study would determine whether extending the readmission time line to 60 or 90 days would result in increased readmission rates from the LTACHs studied.
Follow-up examination of LTACH HF patients readmitted to STACHs in 2011 indicated that approximately 14% of LTACH-to-STACH readmissions required surgery and 79% occurred for significant medical reasons, including respiratory, cardiovascular deterioration, and sepsis. Of the LTACH PN patients readmitted to STACHs in 2011, approximately 14% required surgery and 76% were readmitted for medical reasons, primarily respiratory, cardiovascular, and sepsis. Other nontreatment-related reasons for readmission could include family requests based on geographic location convenience or physician preferences. Further study is necessary to determine whether there are unique reasons for readmission that are associated only with LTACHs. It is likely that LTACH patient transfers to STACH would occur for patients with more serious conditions than would occur in other care settings because LTACHs have the capacity to treat critically ill patients.
There has been recent debate regarding whether readmission rate is a measure of quality. 19 It is possible that factors that best predict readmissions may be nonmedical and unrelated to disease severity, 20 may be related to patient safety climate and patient satisfaction,21,22 or may be affected by hospital location and patient race. 23 However, clinical and health-related factors such as malnutrition appear to predict and affect hospital readmission rates.24-26 Several models that predict risk for readmission have had relative poor performance; 27 model sophistication and interpretation are also limited by the difficulties in using claims data to accurately differentiate patients clinically.28,29 Using ADT data increases the accuracy of tracking patients from specific STACHs, identifying clinical conditions that are present on admission, and establishing the reasons for a readmission. However, no information is available on patients who are discharged within 30 days from the LTACH to other destinations who subsequently return to a STACH within the 30-day time period. After a patient leaves the LTACH (before 30 days from LTACH admission), health care capacity and quality may no longer be representative of the LTACH. Yet readmissions to the STACH are still relevant according to Medicare payment rules, which consider readmissions up to 30-days after discharge from the STACH.
Because the majority of STACH Medicare patients who are not discharged home are discharged to skilled nursing facilities, the majority of STACH readmissions also come from skilled nursing facilities, which also have proportionately higher readmission rates to STACH than LTACHs. 30 LTACHs may have a lower impact on STACH readmission rates compared to the larger proportion of patients who remain in the STACH intensive care unit for long-term treatment. In a recent study that corrected for differences in STACH and LTACH use with an instrumental variable analysis, despite a statistically equivalent readmission rate, patients who transferred to an LTACH incurred significantly lower hospitalization costs and reduced their utilization of other post–acute care services. 31 With respect to CMS payment rules, the low LTACH-to-STACH readmission rates would have a minimal impact on STACH readmission rates for HF and PN LTACH patients for the LTACHs studied. If these results can be generalized to other LTACHs and LTACH organizations, LTACHs may be an ideal care setting for patients susceptible to readmission.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.