
Abstract
This study aimed to determine the association between muscle dysmorphia and emotion regulation difficulties among a sample of boys and men in Canada and the United States (N = 1553). Multiple adjusted linear regression analyses were used to determine whether boys and men with probable muscle dysmorphia had higher scores on the Difficulties in Emotion Regulation 18-Item (DERS-18) measure. Participants with probable muscle dysmorphia, compared to those without, had significantly higher total DERS-18 scores and scores on the goals, impulse, and nonacceptance subscales. These findings add to a small literature on emotion regulation abilities among individuals with muscle dysmorphia and build on the extensive literature documenting the association between emotion regulation difficulties and psychopathology. Clinicians can consider assessing emotion regulation among boys and men displaying muscle dysmorphia symptomatology. Targeting emotion regulation abilities in treatment may be effective at addressing the significant symptoms of muscle dysmorphia.
Muscle dysmorphia, a specifier of body dysmorphic disorder, is a complex mental health condition. Muscle dysmorphia, a condition that predominantly affects boys and men (Mitchison et al., 2022; H. G. Pope et al., 1997, 2017), is marked by obsessive preoccupation with perceived insufficient muscularity, drive for muscularity, and functional impairment (American Psychiatric Association, 2022). Individuals with muscle dysmorphia often engage in a variety of behaviors oriented towards attaining an ideal muscular body, including excessive exercise, obsessive dietary practices, and the use of muscle-building supplements and drugs (Ganson et al., 2023; Martenstyn et al., 2022). Indeed, the intense preoccupation with muscularity and obsessive engagement in muscularity-oriented behaviors are catalysts for high levels of functional impairment and distress. Given this impairment and distress, by some estimates 50% of individuals with muscle dysmorphia have reported a suicide attempt (C. G. Pope et al., 2005), which underscores the importance of elucidating emotional regulation capacities among those with muscle dysmorphia to inform intervention efforts.
Emotion regulation is a multifaceted construct that refers to one’s ability to influence emotions, including which emotions they experience, when their emotions occur, and how they express their emotions (Gratz & Roemer, 2004; Rottenberg & Gross, 2003). Research has linked emotion regulation/dysregulation with psychopathology (Aldao et al., 2010; Compas et al., 2017; Sheppes et al., 2015). Eating disorders, specifically anorexia nervosa, have symptoms and behavioral features similar to muscle dysmorphia, including intense body dissatisfaction and behaviors and obsessive and compulsive behaviors intended to change one’s body to fit an ideal (Blomeley et al., 2018). People with greater emotion regulation difficulties are more likely to experience eating disorders (Lavender et al., 2015; Leppanen et al., 2021; Prefit et al., 2019). For example, individuals with eating disorders experience greater emotion dysregulation, such as difficulty identifying their emotions (i.e., alexithymia; H. Kessler et al., 2006; Westwood et al., 2017) and regulating their emotions with adaptive techniques (e.g., reappraisal; Prefit et al., 2019). Despite this research connecting eating disorders with emotion regulation difficulties, there is a dearth of research on emotion regulation and muscle dysmorphia.
This limited prior research has described a positive association between emotion regulation difficulties and muscle dysmorphia. For example, a case report of a 20-year-old male documented that he engaged in muscle-building activities to manage emotional distress. Specifically, engagement in muscle-building exercise was reported to immediately reduce distress (Murray et al., 2012). This association was also described in a qualitative study of individuals with muscle dysmorphia, whereby compulsive exercise (i.e., muscle-building) was a primary mechanism to regulate emotions (Martenstyn et al., 2022). Furthermore, alexithymia has been documented to be associated with greater muscle dysmorphia symptomatology among undergraduate men (Leone et al., 2015).
Investigating emotion regulation among boys and men with muscle dysmorphia may be particularly important given the gendered aspect of this condition. For example, research has reported a strong association between conformity to masculine norms and muscle dysmorphia symptomatology (Blashill et al., 2020; Ganson et al., 2024). Similarly, traditional norms of masculinity have emphasized emotional stoicism, toughness, and avoidance of femininity (Kågesten et al., 2016; Levant, 1996; Rogers et al., 2021), which are characterized by the suppression of strong affective states, rather than the regulation of strong emotional experiences. Therefore, the underpinning of masculine gender norms on the experience of muscle dysmorphia and emotion regulation is particularly relevant for conceptualizing the association between these two constructs.
Despite the preliminary evidence of the association between muscle dysmorphia and emotion regulation difficulties, small sample sizes with minimal geographic and sociodemographic diversity limit these prior studies. Thus, future research to further explore this association among larger, epidemiological samples can elucidate the scope of the problem. Therefore, the current study aimed to expand the evidence on emotion regulation in individuals with muscle dysmorphia by testing the hypothesis that boys and men who met the clinical criteria for a probable muscle dysmorphia diagnosis would show greater emotion regulation difficulties than those not meeting muscle dysmorphia criteria.
Methods
The data for this analysis were from The Study of Boys and Men, an online survey distributed via Qualtrics, aimed at investigating the body image experiences of boys and men across Canada and the United States. Participant recruitment occurred between March and April 2024 using Instagram and Snapchat advertisements, targeting males between 15 and 35 years old and without additional filters. Advertisements were generic in nature to recruit a broad range of participants (i.e., “Don’t miss your chance to make your voice heard! Participate today in: The Study of Boys and Men, an international research study of the contemporary lives of boys and men.”). To ensure data quality, several recommended anti-bot measures were employed, including honeypot questions, open-response options, attention checks, restrictions on multiple submissions, and reCAPTCHA verification (Xu et al., 2022). Data validation involved screening for issues such as straight-lining, incomplete responses, and nonsensical entries in open-response questions. From an initial sample of 1791 respondents, exclusions were made for a range of reasons: incorrect responses to attention checks (n = 1), skipping attention checks (n = 11), leaving more than 50% of the survey unanswered (n = 4), completing the survey in under 10 minutes (n = 6), failing reCAPTCHA (n = 212), and submitting duplicate responses (n = 4). The final dataset consisted of 1553 participants after these exclusions. All respondents provided informed consent via checkbox, and the study was approved by the Health Sciences Research Ethics Board at the University of Toronto (Protocol #45880).
Participants
Descriptive Characteristics of a Sample of Boys and Men From Canada and the United States (N = 1553).
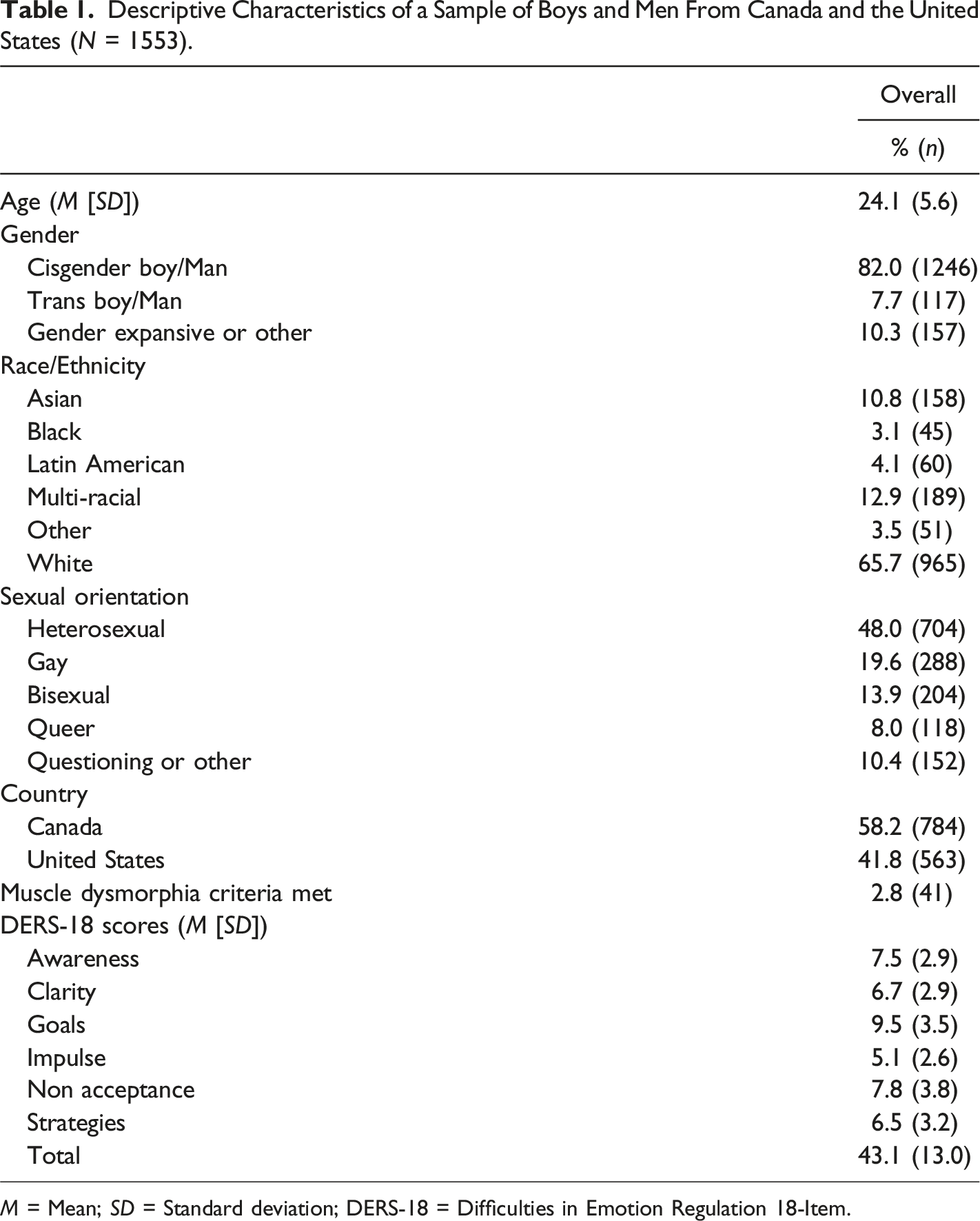
M = Mean; SD = Standard deviation; DERS-18 = Difficulties in Emotion Regulation 18-Item.
Measures
Muscle Dysmorphia
A probable muscle dysmorphia diagnosis was assessed using an algorithm based on the work of Mitchison et al. (2022), which was adapted from the diagnostic criteria originally developed by Pope et al. (1997) and is consistent with the Diagnostic and Statistical Manual of Mental Disorders, fifth Edition, Text Revision (DSM-5-TR; American Psychiatric Association, 2022). The algorithm encompasses various validated instruments alongside two additional items created by the research team to capture key criteria of muscle dysmorphia, including preoccupation with muscularity, the drive for muscularity, and associated distress and functional impairment. Validated tools used in the algorithm included the Muscle Dysmorphic Disorder Inventory (Hildebrandt et al., 2004), the Drive for Muscularity Scale (McCreary et al., 2004), the Eating Disorder Examination Questionnaire 6.0 (Fairburn & Beglin, 2008), the Pediatric Quality of Life Inventory (for both adolescent and young adult populations; Varni et al., 2001; Varni & Limbers, 2009), and the Kessler Psychological Distress Scale (R. C. Kessler et al., 2003). Internal consistency using Cronbach’s Alpha for the full measures used in the algorithm ranged from good to excellent (α = .86–92). The two research-developed items focused on evaluating adherence to a high-protein diet and the use of anabolic-androgenic steroids. Full criteria for muscle dysmorphia are detailed in Supplemental Table 1.
Emotion Regulation Difficulties
The Difficulties in Emotion Regulation Scale (DERS) 18-Item (Victor & Klonsky, 2016), which is based on the original 36-item DERS (Gratz & Roemer, 2004), was used to assess emotion regulation abilities. The DERS-18 is composed of 18 total items, with three items for each of the six subscales. The subscales included awareness (i.e., lack of awareness of one’s emotions), clarity (i.e., lack of clarity about the nature of one’s emotions), nonacceptance (i.e., lack of acceptance of one’s emotions), strategies (i.e., lack of access to effective emotion regulation strategies), goals (i.e., lack of ability to engage in goal-directed activities during negative emotions), and impulse (i.e., lack of ability to manage one’s impulses during negative emotions; Gratz & Roemer, 2004; Victor & Klonsky, 2016). Response options ranged from 1 (almost never) to 5 (almost always). Scores for each subscale and total score were summed, including the three reverse-coded items (Gratz & Roemer, 2004; Victor & Klonsky, 2016). Internal consistency using Cronbach’s Alpha for the DERS-18 ranged from good (awareness: α = .80; clarity: α = .85; impulse: α = .87; strategies: α = .83) to excellent (goals: α = .90; nonacceptance: α = .92; total score: α = .90).
Sociodemographic Variables
Sociodemographic variables included self-reported age, race/ethnicity (White, Black, Asian, Latin American, other race/ethnicity, multi-racial), sexual orientation (heterosexual, gay, bisexual, queer, questioning, or other), and country of residence (Canada, United States [based on provided zip codes and postal codes]). Gender was determined based on self-reported sex assigned at birth and current gender identity (cisgender boy/man, transgender boy/man, gender expansive or other). These variables were controlled for given that they may be potential confounders to the relationship between muscle dysmorphia and emotion regulation abilities (Amodeo et al., 2022; Ganson et al., 2023; Nolen-Hoeksema, 2012; Tylka, 2011, 2021; Weiss et al., 2022).
Statistical Analysis
Descriptive statistics using frequencies, means, and standard deviations were conducted. Seven linear regression analyses were conducted to determine the association between meeting criteria for a probable muscle dysmorphia diagnosis, as the independent variable, and DERS-18 total score and subscale scores as the dependent variables. Linear regression analyses adjusted for the sociodemographic covariates. All assumptions of linear regression were checked and were met for linearity (residual plot, augmented component-plus-residual plot), homoscedasticity (Cook-Weisberg test for heteroscedasticity), normality (kernel density plot, standardized normal probability plot), and absence of multicollinearity (variance inflation factors). Listwise deletion was used to account for missing data given that there was minimal missing data (<5% across variables) and because the sample size was relatively large, raising minimal issues with statistical power (Allison, 2002; Parent, 2013). Statistical significance was determined using the Benjamini-Hochberg procedure with a false-discovery rate of 10% (Benjamini & Hochberg, 1995). All analyses were conducted using Stata 18MP (StataCorp LLC, 2024).
Results
Among participants, 2.8% met the clinical criteria for a probable muscle dysmorphia diagnosis (Table 1). Mean scores for the DERS-18 were 7.5 (SD = 2.9) for the awareness subscale, 6.7 (SD = 2.9) for the clarity subscale, 9.5 (SD = 3.5) for the goals subscale, 5.1 (SD = 3.5) for the impulse subscale, 7.8 (SD = 3.8) for the nonacceptance subscale, 6.5 (SD = 3.2) for the strategies subscale, and 43.1 (SD = 13.0) for the total score.
Associations Between Muscle Dysmorphia and Difficulties in Emotion Regulation Scale Scores.
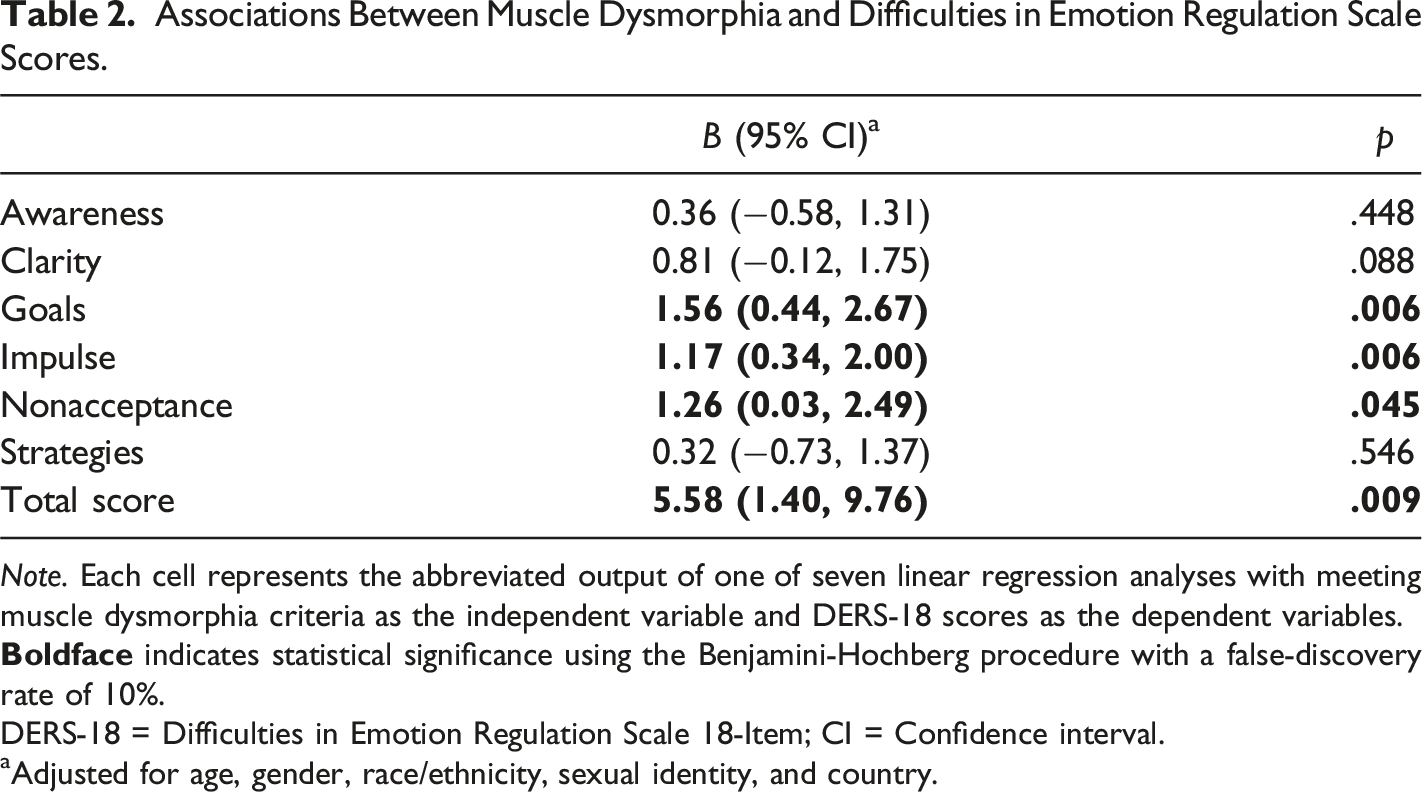
Note. Each cell represents the abbreviated output of one of seven linear regression analyses with meeting muscle dysmorphia criteria as the independent variable and DERS-18 scores as the dependent variables.
DERS-18 = Difficulties in Emotion Regulation Scale 18-Item; CI = Confidence interval.
aAdjusted for age, gender, race/ethnicity, sexual identity, and country.
Discussion
This study aimed to test the hypothesis that boys and men with probable muscle dysmorphia diagnosis would have greater emotion regulation difficulties compared to those without muscle dysmorphia. The findings indicate that boys and men who met clinical criteria a probable muscle dysmorphia diagnosis had higher scores on the DERS-18 total score, indicating greater overall emotion regulation difficulties, which confirms the study hypothesis. This finding aligns with the clinical criteria for muscle dysmorphia that emphasizes the functional impairment and distress that arises from the symptomatology (i.e., severe preoccupations and obsessive behaviors) of the condition (American Psychiatric Association, 2022; H. G. Pope et al., 1997). Additionally, prior research has documented the emotion regulation difficulties among individuals with muscle dysmorphia (Martenstyn et al., 2022; Murray et al., 2012), which aligns with research that has connected emotion regulation difficulties across psychopathology (Aldao et al., 2010; Compas et al., 2017; Sheppes et al., 2015).
Among the sample, meeting clinical criteria for a probable muscle dysmorphia diagnosis was positively associated with several specific constructs of emotion dysregulation, namely, the lack of ability to engage in goal-directed activities during negative emotions (goals subscale), the lack of ability to manage one’s impulses during negative emotions (impulse subscale), and the lack of acceptance of one’s emotions (nonacceptance subscale). The difficulty with goal-directedness may be due to the significant distress and overwhelm that arises from the obsessive and compulsive preoccupations and behaviors underpinning muscle dysmorphia symptomatology (American Psychiatric Association, 2022; Martenstyn et al., 2022). For example, during negative emotions that arise from the preoccupation with insufficient muscularity, a boy or man with muscle dysmorphia may struggle to redirect their thoughts onto activities that may help them reach their overall life goals (i.e., educational, occupational, social). Indeed, this level of functional impairment is a marker of muscle dysmorphia (American Psychiatric Association, 2022; H. G. Pope et al., 1997). Prior research has similarly documented a positive association between muscle dysmorphia and reduced goal-directedness (Cunningham et al., 2020; Murray et al., 2012).
The lack of impulse control during negative emotions may underpin the engagement in excessive exercise and the over control of eating behaviors common among individuals with muscle dysmorphia (Martenstyn et al., 2022, 2023). For example, as noted in prior research (Martenstyn et al., 2022; Murray et al., 2012), impulsive engagement in excessive and compulsive exercise may be a means to temporarily alleviate distress stemming from body and muscle dissatisfaction. Overall, individuals with muscle dysmorphia may also be more prone to impulsive and risky behaviors (e.g., anabolic-androgenic steroid use, substance use behaviors, suicidality; Ganson et al., 2023; C. G. Pope et al., 2005), which may be exacerbated during moments of negative emotions. Finally, the lack of acceptance of one’s emotions may be due to the core low self-esteem that is illustrative among people with muscle dysmorphia (Martenstyn et al., 2022). Relatedly, individuals with muscle dysmorphia may not want to accept negative feelings about themselves, particularly their bodies, which may perpetuate obsessive thinking patterns, preoccupations, and behaviors.
Implications
The findings from this study have important implications for assessment and clinical intervention. Clinicians should consider assessing for overall emotion regulation skills among boys and men who display symptoms of muscle dysmorphia, as well as consider emotion regulation difficulties as a potential marker of severity of symptomatology. Currently, a dearth of research exists on effective treatments for muscle dysmorphia (Grunewald & Blashill, 2021), despite evidence that cognitive behavioral therapy (CBT) is effective for treating body dysmorphic disorder (Harrison et al., 2016). Additionally, it has been proposed that other treatment methods that include targeting emotion regulation abilities, including acceptance and commitment therapy (ACT) and dialectical behavioral therapy (DBT), may be applied to muscle dysmorphia (Cunningham et al., 2017). Thus, the findings may provide further evidence that interventions aimed at increasing emotion regulation abilities, such as CBT, DBT, and ACT (Cunningham et al., 2017; Harrison et al., 2016), may be effective for individuals with muscle dysmorphia. Specifically, treatments that focus on increasing abilities to engage in goal-directed behaviors, reduce impulsive behaviors, and assist individuals with muscle dysmorphia in accepting their emotions are warranted and may be particularly helpful in reducing distress and functional impairment. Indeed, future investigation is needed to test the efficacy of these treatment interventions among individuals with muscle dysmorphia.
Limitations
There are limitations to this study that should be noted. First, the recruitment of participants using non-probability sampling methods poses challenges to the generalizability of the findings, primarily due to the risk of self-selection bias. While this may limit the broader application of the results, it is important to recognize that the sample itself was diverse. Participants varied across key sociodemographic characteristics, including age, education, gender, and sexual orientation, and resided in all 13 provinces and territories in Canada, as well as in all 10 major zip code (i.e., geographic) regions that group the United States. This broad representation lends some strength to the scope of the study’s sample and the findings. Other limitations include the use of self-report items and the absence of clinical interviews to assess muscle dysmorphia, which could have provided deeper diagnostic insight. Instead, the study relied on clinically defined criteria from the DSM-5-TR, using both standardized measures and custom-designed items (Mitchison et al., 2022). While this approach enhanced the reliability of the findings and provided a cost-effective method suitable for large-scale studies, future research would benefit from validating these results in clinical populations, where muscle dysmorphia can be more rigorously diagnosed. Finally, the cross-sectional design of the study limits our ability to draw conclusions about the directionality between muscle dysmorphia and difficulties with emotion regulation. To address this, future research should prioritize longitudinal designs that can better explore the directionality and underlying mechanisms of these associations.
Conclusion
Among a large and diverse sample of boys and men in Canada and the United States, participants who met clinical criteria for a probable muscle dysmorphia diagnosis were more likely to report greater emotion regulation difficulties, particularly related to goal-directedness and impulsivity, as well as nonacceptance of emotions. These findings underscore the importance of including emotion regulation abilities in screening and intervention efforts for muscle dysmorphia.
Supplemental Material
Supplemental Material - Muscle Dysmorphia and Emotion Regulation: Findings From the Study of Boys and Men
Supplemental Material for Muscle Dysmorphia and Emotion Regulation: Findings From the Study of Boys and Men by Kyle T. Ganson, Alexander Testa, Rachel F. Rodgers, Stuart B. Murray, and Jason M. Nagata in The Journal of Men’s Studies
Footnotes
Author Contributions
Kyle T. Ganson: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Validation; Visualization; Roles/Writing - original draft; and Writing - review & editing. Alexander Testa: Conceptualization; Writing - review & editing. Rachel F. Rodgers: Conceptualization; Writing - review & editing. Stuart B. Murray: Conceptualization; Writing - review & editing. Jason M. Nagata: Conceptualization; Writing - review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data may be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.