
Abstract
Dominant gender norms among South African males promote ideals of masculinity characterized by control, emotional stoicism, and power, which can impact overall health. This study explores South African men’s perceptions of the “ideal” man, societal expectations, and how sexual identities intersect with masculinity, health-seeking behaviors, and HIV prevention. We conducted 40 interviews with men who have sex with women and men who have sex with men, aged 18–35 years who resided in Johannesburg or Cape Town municipal areas. Participants described their idea of the “ideal man” as a provider, protector, and role model, though these ideals varied across contexts. High family and community expectations created both stress and motivation. Barriers to sexual healthcare included resistance from male-dominated communities and stigma towards non-heteronormative sexual identities, particularly among men who have sex with men. Addressing these challenges requires promoting more inclusive understandings of masculinity and improving healthcare access by challenging gender norms.
Gender norms and expectations are shaped by a complex interplay of historical, cultural, and socio-political factors, influencing how individuals experience and express masculinity and femininity (Connell, 2005; Harrison, 2008; Mshweshwe, 2020; Walker, 2005). Masculinities are not static; they are constructed and reconstructed in response to broader social forces, varying across different contexts. Hegemonic masculinity, as originally defined by Connell (Connell, 1987) and later refined by Connell & Messerschmidt (Connell & Messerschmidt, 2005), refers to the dominant form of masculinity that reinforces patriarchal structures. This dominant form coexists with other subordinated or marginalized masculinities, which are shaped by factors such as class, race, and sexual identity. In South Africa, hegemonic masculinity has historically been associated with power, control, and emotional stoicism, shaping men’s engagement with public life and health services (Colvin, 2011; Jewkes & Morrell, 2010; Morrell, 1998).
Scholars have explored how apartheid and post-apartheid dynamics influenced the construction of South African masculinities. During apartheid, “White” hegemonic masculinity was dominant, while Black masculinities were often constructed in opposition, forming around resistance to systemic oppression (Morrell, 2001; Walker, 2005). In the post-apartheid era, Black masculinities have become more associated with control, economic power, and evolving social expectations (Morrell, 1998; Ratele, 2013). Some scholars have critiqued oversimplified portrayals of African masculinities, emphasizing that they are dynamic, contested, and shaped by both local traditions and contemporary realities (Peacock & Levack, 2004; Ratele, 2013, 2016). This diversity underscores the importance of examining masculinities in their specific cultural and historical contexts.
The idea of an “ideal man” is also complex, as conceptions of masculinity vary across societies. Several studies have shown that masculine ideals are shaped by social norms, identity, and socio-economic factors, and they often shift in response to changing circumstances (Jewkes, 2002; Reid, 2013; Van den Berg et al., 2013). As a result, what constitutes an ideal form of masculinity is not universal but varies within and between different communities, sometimes creating tensions as men navigate multiple, sometimes conflicting, gender expectations.
The relationship between gender norms and men’s health behaviors has been well-documented in African settings. Several authors have demonstrated how hegemonic masculinities negatively influence men’s engagement with healthcare, particularly in the context of HIV prevention and mental health services (Campbell, 2003; Dworkin et al., 2013; Gittings et al., 2021; Jacques-Aviñó et al., 2019; Jewkes, 2002). Men who align with rigid masculine ideals may avoid seeking help for conditions like depression or anxiety, viewing such behaviors as incompatible with their understanding of masculinity (Seidler et al., 2016; Sileo et al., 2019). Studies have also shown how traditional masculine ideals can marginalize non-heteronormative men, particularly in the context of HIV prevention among men who have sex with men (MSM) (Jacques-Aviñó et al., 2019; Reid, 2013; Zeglin, 2015). Others have argued for the need for gender-transformative approaches to healthcare, particularly in addressing sexual and reproductive health concerns among men (Barker et al., 2007, 2010; Peacock & Levack, 2004).
Further research highlights how societal expectations, such as being the primary provider and suppressing emotions, contribute to negative mental health outcomes amongst men, exacerbating feelings of inadequacy, leading to heightened stress, anxiety, and depression (Powell et al., 2016; Seidler et al., 2016; Sileo & Kershaw, 2020). Additionally, stigma around vulnerability discourages men from seeking mental health support, reinforcing dynamics that perpetuate emotional suppression (Griffith et al., 2011; Sileo & Kershaw, 2020).
Several studies have examined how hegemonic masculinity affects healthcare access, particularly in relation to HIV testing and treatment. Findings suggest that societal expectations of strength and invulnerability deter men from accessing healthcare, further entrenching health disparities and contributing to the HIV epidemic (Colvin, 2019; Ezeugwu & Ojedokun, 2020; Nardell et al., 2022; Sileo et al., 2018). There is a growing call for interventions that address these gender norms and encourage men to seek care in ways that align with their sense of identity without compromising their masculinity (Barker & Ricardo, 2005; Colvin, 2019). Moreover, the concept of “traditional” gender roles has often been critiqued for simplifying African masculinities. Several authors have argued that understanding African masculinities as static reinforces stereotypes and overlooks how men navigate their identities in response to rapid social and economic changes (Ratele, 2016; Reihling, 2013). Others have highlighted that hegemonic masculinities, while context-dependent, are pervasive across many South African cultures, complicating efforts to reshape gender norms in ways that promote health equity (Duby et al., 2023; Sikweyiya et al., 2014).
In light of these complexities, this study seeks to contribute to the evolving literature on gender norms and masculinities in South Africa. We examine how young South African men, recruited from two metropolitan areas, define their concept of an “ideal” man and how they perceive the expectations placed on them. Additionally, we investigate how differing sexual identities intersect with masculinity, shaping men’s experiences of gender expectations, health-seeking behaviors, and outcomes related to HIV prevention.
Methods
Study Design and Population
South African Male User Research on Acceptability of Implants and Injections (SAMURAI) is a socio-behavioral and clinical multi-stage study that aims to assess the acceptability of, and preferences for, novel long-acting HIV pre-exposure prophylaxis (PrEP) delivery formulations among key end-users in South Africa: heterosexual men – defined as cisgender men who have sex with only cisgender women (MSW) and men-who-have-sex-with men (MSM) – defined as cisgender men who have sex with men. MSM could sexually identify in a number of ways such as bisexual, gay, or straight, and could have sex with different types of people, including women. However, they were only eligible to enroll in this subgroup if they also had sex with men. More information on the study design and procedures is reported elsewhere (Atujuna et al., 2024).
We conducted formative research using qualitative methods to inform the development and refinement of clinical study materials, messages, and strategies for successful recruitment and implementation of the research. We focused on gender and sexual orientation as topics of interest to prepare for a clinical study that would include cisgender men of varying sexual orientations. Participants were recruited from databases and records from prior HIV prevention studies to generate initial recruitment lists of participants representing each of the target samples. These lists were supplemented by community-based recruitment and peer-driven recruitment to ensure that the overall sample included a greater proportion of study naïve participants than study-experienced participants.
Data Collection and Settings
Data was collected for this study through qualitative in-depth interviews (IDIs) with MSW and MSM from resource-restricted communities in Cape Town (n = 20) and Johannesburg (n = 20), South Africa. A total of 40 IDIs were conducted, with 20 participants identifying as MSW and 20 as MSM. All participants were between the ages of 18–35 years, self-reported as being HIV-negative, and currently sexually active. The research team consisted of local male and female interviewers who were fluent in either isiZulu or isiXhosa, which facilitated rapport-building with participants. Interviewers and study staff received gender-focused training prior to data collection. Interviews were conducted face-to-face in private locations in the language(s) of participants’ choice (English, isiZulu, or isiXhosa) using a semi-structured interview guide and lasting an average of 60 minutes. Topics explored for this analysis included sexual behavior and relationships, masculinity and gender identity, and other factors influencing attitudes towards LA-PrEP. Interviews were audio recorded, transcribed, and translated into English by study site staff or through translation agencies. Transcripts underwent a quality control process, which involved review by study site interviewers and qualitative analysts, before coding and analysis. Since data collection took place during the COVID-19 pandemic, both interviewers and study participants adhered to pandemic guidelines, including distancing, masking, or video interviews.
Data Analysis
A codebook was developed for analysis based on the study’s questionnaires and the structured IDI guide. The codebook included descriptive codes that directly corresponded to the topical areas relevant to the SAMURAI study (e.g., long-acting HIV prevention products, HIV knowledge and attitudes, side effects, community) as well as analytical codes that highlighted narrative text reflective of an analytic theme (e.g., masculinity, sexuality). The codebook was developed in collaboration with study staff who lived in the same cultural context as the participants. We also explored questions aligned with the socio-ecological model to understand how individuals' self-perception as an “ideal” man, with regards to their sexuality, is influenced by factors such as the self, family, community, and external systems (including culture, geographic location, policies, tradition, and history) (Kilanowski, 2017). Transcripts were uploaded into Dedoose software version 9.0.17 (Dedoose, 2021) and coded by a team of four trained South African qualitative analysts. Weekly coding meetings were held over a 2-month period to test intercoder reliability and reach consensus of the interpretation and application of codes. To ensure quality and accuracy of data interpretation, the lead author conducted thematic analysis of data focusing on masculinity and sexuality/sexual identity, acknowledging her positionality and biases. Using an inductive approach, she remained sensitive to the sociocultural context of South African men’s interviews, avoiding gendered assumptions. Two additional analysts reviewed and discussed summary memos, offering external perspectives to enhance the depth and reduce bias. All co-authors, reviewed and approved the interpretation of quotes and results, ensuring a nuanced and robust interpretation of gender norms within the South African context.
Results
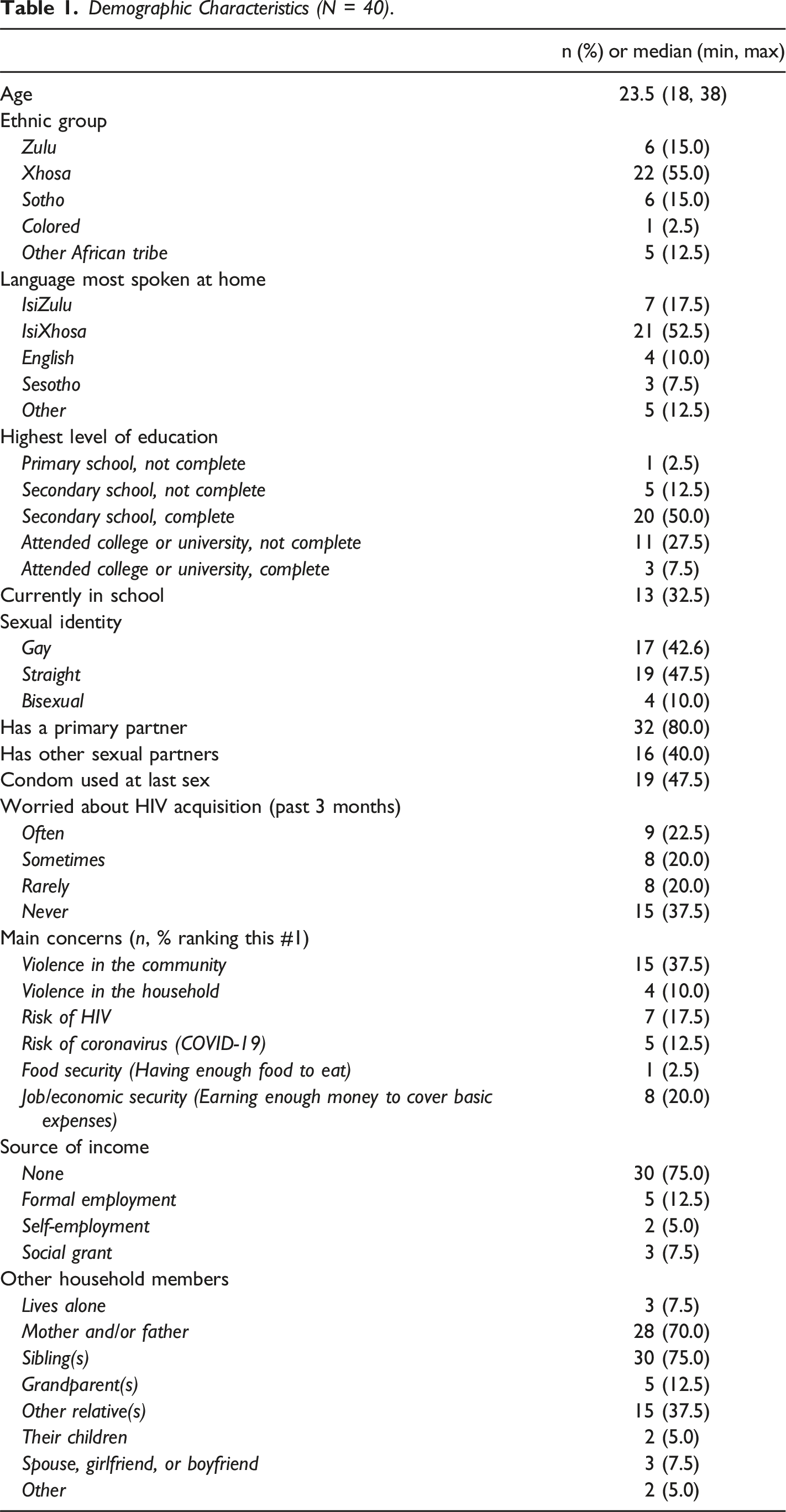
Participant Demographics
Demographic Characteristics (N = 40).
Overview
In the IDI semi-structured interview guide, participants were asked to describe, from their own perspectives, an “ideal” man. Participants portrayed the “ideal man” as embodying responsibility and protection, shaped by both individual attributes and societal expectations. This “ideal” is deeply influenced by cultural norms, gender dynamics, and historical factors. Our findings reveal a complex interplay between acceptance, discrimination, and personal responses, particularly for LGBTQ + individuals. Additionally, the data highlights how notions of masculinity impact health-seeking behaviors, especially regarding sexual health and well-being. Figure 1, informed by the socio-ecological model (SEM) was used to organize the findings from this analysis, according to multiple levels of influence on masculinity and health behaviors. Interconnections shaping perceptions of the ideal man: self, family, community, and other external factors.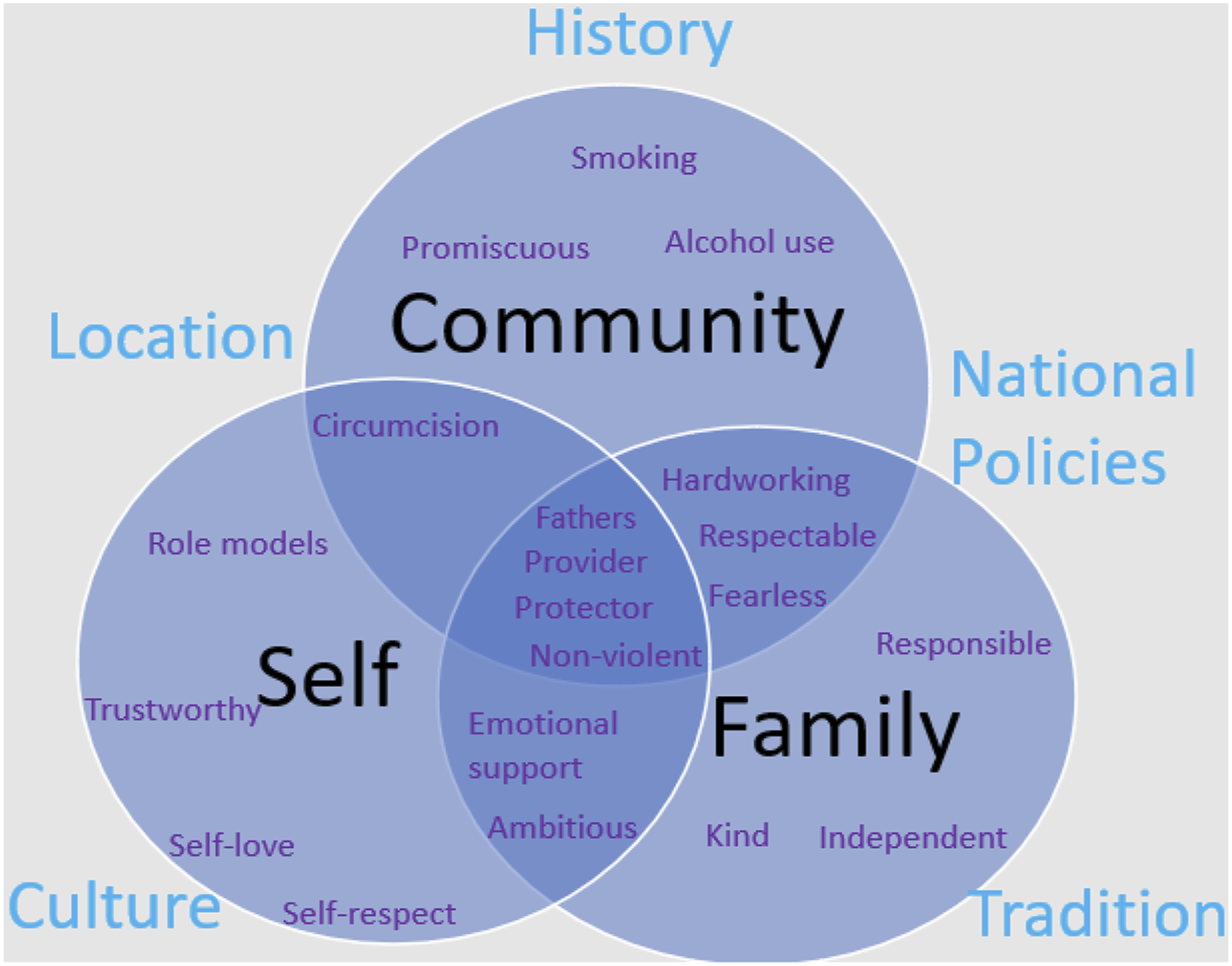
The “Ideal Man”: Self, Family, and Community Perceptions
Both MSW and MSM participants described the “ideal” man as someone responsible, protective, and a provider for his family. This ideal was influenced by personal beliefs but was also shaped by expectations from family members and the broader community. For many, being a man meant fulfilling specific roles, such as ensuring the financial stability and safety of their family. Men were expected to meet the basic needs of their households, such as food and financial security, while also acting as protectors and role models for younger generations. One participant noted, “A man’s goal is to have a family that is well in future and build a brighter future for his children.” [MSW, Cape Town]
Two other participants added: To be a man … means to be someone that is respected because most of the time the man is a breadwinner in the household…. He is the one that puts bread on the table…he is the person that protects the family in everything that happens. If there is something that will happen in your family it must start with you before it reaches everybody in the family. [ MSM, Cape Town] Look at me … my father is not around. I’m the one that follows, so traditional things will be taken care (of) by me those are my expectation at home, if father is not there women expect you to provide for them, those are the expectation I need to look after home, I must protect the family. [MSM, Cape Town]
Beyond family responsibilities, participants discussed the role of men in the broader community. Many felt that an ideal man not only provided for his immediate family but also contributed to the welfare of the community. “Those things that make you a man, being a son to the community and being a father to your community; being all of those things that you can be to those who don’t have.” said one MSW participant, highlighting the expectation that men should be community leaders and protectors, even in situations that did not directly benefit them. [MSW, Cape Town]
The pressure to meet these expectations, however, was experienced differently by participants. Some found the responsibilities overwhelming, particularly when traditional masculine roles such as being the primary breadwinner or protector were difficult to fulfill. One participant shared, “Because the expectations are too high and I cannot meet them and it makes you feel less of a man” (MSW, Cape Town). This sense of inadequacy was common among men who felt they could not live up to societal ideals of masculinity: These expectations like sometimes they make me feel like they are too much, who made them? They make me feel like they are stereotypes you see, why can’t we just live life why should there be an expectation on how guys should be, it doesn’t make me feel happy at all. I feel every person should set their own view of life, and not being told that this is how you should live. [MSW, Johannesburg]
For others, however, the expectations were seen as motivating rather than burdensome. Several participants viewed these expectations as opportunities for personal growth and a way to establish themselves as respected figures in their families and communities. One MSM participant said, “They [expectations] relieve me instead of holding [me] back as if there is nothing I can’t do to succeed, one day I will be a role model in other people’s lives.” [MSM, Cape Town]
However, another participant from Johannesburg highlighted the stigma they encountered when accessing healthcare services. Their experience underscores the challenge of navigating community assumptions and the fear of being labeled based on where they seek care: Not really but obviously in the community when you go to the men’s clinic for example, they know that only gay people go there so they assume that you are gay. [MSM, Johannesburg]
Some participants spoke about being teased or discriminated against if they did not act like “a man”, for example not engaging in masculine activities such as drinking alcohol, having multiple sexual partners, going to bars, or smoking. Teasing, particularly from family members, was also reported among men unable to provide financially. I feel it’s too much for me to always satisfy those expectations because I can’t always fit in … it’s like l am a different cut…. I don’t fit into all those expectations and it’s very difficult for me to sometimes express that ‘no … I can’t fit into this, you expect me to do this but I am not comfortable with that’. [MSM, Johannesburg] Some people look down at you as if you are not a man because they want you to do what they do, like chilling at the tavern, drink alcohol, and smoke. I don’t even smoke, so they would look down on me because they want me to smoke…. They think you are not a man enough; they don’t know that you are taking care of your life by not doing these things. [MSW, Cape Town]
Another participant noted that traditional masculinities suppress emotional reactions to stress and pressure in men, suggesting the need for its evolution. Increasingly, some men are challenging these norms, recognizing the importance of emotional expression and self-respect as key aspects of modern masculinity. One participant explained: We grow up in the community whereby as a Black man you are not allowed to cry, not allowed to show emotion. I think the next generation or our next young black men growing up, we need to teach them to show respect, take accountability, be responsible and that it is okay to cry and show emotions… [MSM, Johannesburg]
Similarly, several participants emphasized the role of self-love and self-respect in redefining what it means to be a man in contemporary society. This evolving view of masculinity included both physical and emotional boundaries as a means of self-protection. As one participant explained: ...if he has self-respect first, he should love himself. I think if you love yourself you can protect yourself better (he later adds that by protecting oneself he means physically, emotionally, and mentally) and people around you. [MSW, Johannesburg]
Another participant added: [To be a real man] He must have self-love…. You must respect your body. There are people who do not care about HIV, they have sex without using condoms, you need to have boundaries. [MSW, Johannesburg]
Sexual Identities and Societal Expectations
For MSM participants, the challenge of fulfilling traditional masculine roles was compounded by societal stigma related to their sexual identity. In addition to the typical expectations placed on men, MSM participants described additional layers of complexity, particularly in communities where gender roles were rigidly defined. In some communities, people associated MSM individuals with femininity, and this makes it difficult for men to come out as gay. Interestingly, a few participants voiced the perception that individuals identifying as lesbians are often more accepted than gay men in some communities because they are not perceived as a threat to the masculinity by heterosexual men. The following quotes support the narrative above regarding acceptance in various communities: Us boys, most boys don’t have the problem sitting with lesbians but once you see them with a gay guy, and someone sees you sitting with the gay guy, they will think that you are also gay and that will make you uncomfortable. [ MSW, Johannesburg] In my community the gay people [gay men] are not accepted at all, and I feel like the lesbians are more understood more than gay [gay men] people. They love them, admire them, but when it comes to gay people [gay men] it is a very different scenario. [MSM, Johannesburg]
Many MSM talked about being subjected to negative comments and behaviors from peers and community members, who challenge their masculinity and manliness. I was born male, but I don’t subscribe to whatever that is expected of being a man, so obviously at home and the community they bullied me so much. So obviously when you are born your parents have expectations and they already planned your wedding they’ve already planned they are going to have grandchildren, so you see those things. So, my mom was shouting at me when she saw me playing with dolls, because I was [gay]my entire life. I didn’t want to be sexually attracted to the same gender ... my mom use to hear complains at school saying am playing with girls, so she use to beat me and swear at me things like that so even when you don’t get protection from home it becomes difficult when it comes outside. Even outsiders they used to bully me a lot…. [But] my mom in the long run she started understanding that this thing is nature, its natural meaning she’s been like this, she started protecting me. People around me started seeing that there is love, there is protection coming from home then what can we do? [MSM, Johannesburg]
A significant cultural factor that emerged was circumcision, particularly among participants from Xhosa communities. Circumcision was seen as a traditional rite of passage into manhood, and those who did not undergo this ritual or had it performed in non-traditional ways were often not regarded as “real” men. One MSM participant recounted an incident in his community, where a man was discriminated against after being circumcised by a female doctor, violating cultural expectations that the procedure be conducted by a male surgeon. He explained, There is situation like that happened in my street before, my neighbor since he was going to circumcision and there was no surgeon and this have to be done by a female person…. So he was circumcised by a female person and when [he is] sitting with other men then they [are] telling [him] … you are not a man… [MSM, Cape Town]
Another participant, a Xhosa MSM from Cape Town reported that some community members told him he was not a “full” man because he was gay and should not have been circumcised because only “real” men get circumcised. Additionally, a participant from Johannesburg, shared their experience of being teased for playing soccer, considered a male sport, with others suggesting they should be at home playing with dolls instead of on the field with “real” men: Why do you want to play soccer, you are feminine why are you running like this, why are you doing this … do you have a doll? [MSM, Johannesburg]
Acceptance of differing sexual identities among families varied. While some family members, especially female relatives, were supportive—often viewing happiness as the most important factor—others, particularly fathers and brothers, were less accepting. The following participants describes how supportive his family has been including his father (which is not always the case for everyone): Like at home my mom is accepting everything that I do. My dad is protective of me, yes, many people they support me they even ask me questions about who I am and what’s going on with me. I just answer them and am free when it comes to my sexuality, I am not hiding anything. [MSM, Johannesburg]
Participants spoke of MSM individuals being teased, dishonored, or even sent away due to their sexuality, often attributing stigma to a lack of understanding from male family members. Some of them they were accepted but others are chased away even in their homes … it’s only few who has family who are mostly women/females at their homes then maybe they will be accepted and stay with their families but most of them they chased away. [MSW, Cape Town]
Health-Seeking Behaviors
The pressure to conform to societal expectations of masculinity significantly impacted men’s health-seeking behaviors. Many participants, particularly MSM, described how fear of judgment and stigma in healthcare settings prevented them from seeking care. One MSM participant shared: In the community, when you go to the men’s clinic, they know that only gay people go there, so they assume that you are gay. [MSM, Johannesburg]
Participants expressed diverse views about men in their communities and HIV risk perceptions. Some individuals mentioned that men often underestimated the seriousness of HIV and tended to avoid discussing it. One participant reflected: We as men, we don’t like going for help [clinic]. Even if you can feel, “No man, I can’t go there I’ll rather die at home.” They don’t like talking about HIV. That issue makes them sweat. Some are 20 years old but they never tested for HIV…. Even when they see container that is standing right there with HIV written on it they sweat because they don’t know their HIV status. [MSW, Cape Town]
It was also noted that some men held the belief that relying solely on condoms offered sufficient protection. However, despite this belief, men in their communities did not always consistently or correctly use condoms and were unwilling to adopt additional precautions such as oral PrEP or regular HIV testing. One participant described how some men in his community avoided publicly obtaining condoms: People [other men] will come to me and ask for condoms, but they don’t go and take them from where they’re accessible to the public. I don’t know whether they’re afraid of people seeing them. [MSW, Cape Town]
Participants also highlighted that some men believed they were immune to HIV or not at risk. Additionally, many men were noted to prioritize societal expectations, such as being financially secure, being in a relationship, providing for family, and being employed, over their own health. Alcohol use was specifically highlighted as impeding men’s safe sexual decision-making and their focus on health concerns like HIV and STIs. Despite these barriers, some men did seek care. However, those experiences varied. One participant described his discomfort when seeking medical care: When I went there, they referred me to another room, then the lady [nurse] who was there asked me what’s wrong, when I told her that I have hemorrhoids, she started asking me questions like were you arrested, or are you eating white bread, what happened, were you raped. I felt she wanted to ask me if I was having anal sex, but the way she went about it made me uncomfortable. [MSM, Johannesburg]
The fear of being judged or outed by healthcare providers contributed to the reluctance of many men to seek sexual health services, particularly in clinics that were not LGBTQ + or male-friendly. Some men described feeling more comfortable seeking care from pharmacies or specialized clinics for men’s health. One participant noted: Some men do go to the clinic, but some men don’t go to the clinic.... For me personally when I go to test I don’t like to go to a clinic … we know a lot of nurses they are rude it’s not easy if it’s an environment or community you grew up in to get tested because you know the chances of the nurse or the doctors knowing you are very high. You go to test let’s say positive the next thing the whole community knows…. I feel that most men feel comfortable testing at pop up testing centres that are run by non-governmental organizations. [MSW, Cape Town]
Privacy concerns were also a recurring theme in many men’s narratives: The staff is uptight and always fussy and impatient, there’s less privacy it’s easy to know everyone’s business, you would know who is there, say for ARVs, who is there to testing. So many people avoid going to the clinics, they go there when they are in desperate need of help and by then for some it’s already too late [very sick]. [MSW, Johannesburg]
However, not all participants had negative experiences in general clinics. Some found supportive environments where they felt respected and comfortable. One participant described a positive experience: When you enter here [a non-tailored clinic], the treatment is right, better than [at public clinics]. The nurses are friendly, and they don’t make you feel scared. [MSW, Cape Town]
Another MSM participant explained how a small, intimate clinic provided efficient and respectful service: So [Clinic] is very intimate its very small, it’s very accommodating, the service there is very efficient. So, you go there you get there they help you they take your card, they test you they give you PrEP then you leave they like you don’t feel embarrassed, you don’t feel harassed, you don’t feel discriminated in any particular way. [ MSM, Johannesburg]
These positive experiences illustrate that while stigma and fear of judgment are barriers in many healthcare settings, there are clinics that offer inclusive, respectful care. Participants emphasized the importance of privacy and sensitivity from healthcare providers as well as less waiting time, suggesting that such factors could make a significant difference in men’s willingness to seek care. One participant noted: There are times like that, you want to go to the clinic and you changed your mind because in some clinics they are over-crowded, it’s the only issue that makes me not to go to the clinic, even though I want to go to the clinic and I end up changing my mind, it gets overcrowded. [MSW, Cape Town]
Others expressed a preference for community-based services, where they felt less judged and more supported. One participant shared: Pop-up testing centers run by NGOs are better than local clinics. You feel comfortable going there, but in the [public] clinics, it’s different … you don’t feel like going back. [MSM, Johannesburg]
Discussion
In this analysis, we explored men’s perceptions of an “ideal man” and the gender expectations and masculinities endorsed by their families and communities. Participants described an “ideal” man as responsible, protective, supportive, and primarily expected to provide for and protect their families and the community. These expectations align with broader cultural norms shaping masculinity in South Africa, where hegemonic masculinity emphasizes emotional stoicism, physical toughness, and dominance in both familial and social settings (Connell, 1987; Hunter, 2006; Jewkes & Morrell, 2010; Langa, 2017; Morrell, 1998). However, it is important to note that participants’ descriptions of the “ideal” man may reflect societal gender norms rather than their own idealized forms of masculinity. This distinction highlights how societal expectations can shape, and sometimes constrain, individual perceptions. In our sample, this pressure often resulted in feelings of stress and inadequacy, particularly for men unable to meet these rigid standards (Hunter, 2006; Langa, 2017).
Participants’ narratives corroborate global findings that men’s social value is often tied to their ability to provide, protect, and contribute to their communities (Fazli Khalaf et al., 2013; Hunter, 2006; Idris et al., 2019). However, a shift is emerging, with some men increasingly emphasizing self-love and self-respect as markers of positive masculinity. This shift, seen in some participants’ views, signals a transformation away from external validation and toward a focus on emotional well-being (Langa, 2017; Seidler et al., 2016). These evolving gender norms are significant as they may alleviate the psychological toll associated with hegemonic masculinity, which has been linked to adverse mental health outcomes, including anxiety, depression, substance use, and suicide (Gough & Novikova, 2020; Herron et al., 2020). Despite this emerging trend, the rigid gender roles still contributed to negative health outcomes among men. The pressure to conform to societal expectations was a source of anxiety and stress, particularly for those unable to meet the idealized image of masculinity (Hunter, 2006; Langa, 2017; Mkhize, 2006). These findings are consistent with studies that highlight the link between hegemonic masculinity and negative health behaviors, such as delayed healthcare seeking and problematic substance use (Nardell et al., 2022; Odimegwu & Okemgbo, 2008; Sileo & Kershaw, 2020). In this context, recognizing and addressing the impact of traditional gender norms on mental health is crucial, particularly as they relate to both MSW and MSM.
The interplay between sexual identity and masculinity also emerged as a significant theme. MSM participants, in particular, faced compounded pressure, as their sexual identities often clashed with the traditional expectations of masculinity. They reported experiencing discrimination from family members and broader communities, which aligns with findings from other studies on the stigmatization of LGBTQ + individuals in South African communities (Duby et al., 2018; Shangani et al., 2018). Despite the legal recognition of same-sex relationships in South Africa (SANAC, 2023), societal attitudes toward homosexuality remain complex, with MSM individuals often facing discrimination and exclusion from male-dominated spaces. Global data on the acceptance of homosexuality shows that while acceptance has increased in some regions, stigmatization persists, particularly in African contexts (Poushter & Kent, 2020).
Our study also highlighted the significance of cultural traditions, such as circumcision, in defining masculinity, particularly within Xhosa communities. Circumcision in Xhosa culture is a key rite of passage into manhood, and men who do not undergo the traditional ritual, or who experience it in a non-traditional manner, are often stigmatized and excluded from male-dominated spaces (Duby et al., 2023; Magodyo et al., 2017; Meintjes, 1998; Morrell, 1998; Peltzer & Kanta, 2009; Vincent, 2008). Some studies further highlight the growing tension between traditional circumcision and voluntary medical male circumcision (VMMC), where adherence to the former is often seen as the more authentic route to manhood, while the latter may lead to perceptions of reduced masculinity (Mfecane, 2016). This underscores the deep-rooted cultural connection between circumcision and masculinity in Xhosa communities, where failure to conform to these expectations may result in social isolation and diminished status as a “real man.” These findings underline the importance of developing culturally sensitive interventions that respect traditions while promoting inclusivity and support for diverse sexual identities (Mfecane, 2020). Incorporating an understanding of traditional practices, such as circumcision, into health interventions is critical for fostering acceptance while addressing the negative health and social consequences tied to rigid gender norms.
The study further explored how male gender norms shaped participants’ health-seeking behaviors, particularly regarding sexual health and HIV prevention. Men described the stigma associated with seeking healthcare, especially in settings perceived as unfriendly or judgmental, which discouraged them from accessing services. These barriers, including long waiting times and unfriendly healthcare providers, have been documented in studies on men’s health-seeking behaviors (Cheatham et al., 2008; Daniels et al., 2021; Eley et al., 2019; Leone et al., 2017). Participants also highlighted the fear of breaches in confidentiality, particularly among MSM, as a key deterrent to seeking HIV services. MSM participants described how fear of being outed or judged in healthcare settings led them to avoid clinics. This aligns with findings from Shangani (Shangani et al., 2018) and King (King et al., 2020), which emphasize the need for LGBTQ + -friendly healthcare services to reduce stigma and improve access to care. Community-based services and pop-up clinics were suggested as potential solutions, as participants reported feeling more comfortable accessing these services than public clinics (Duby et al., 2019; Novak et al., 2019). Importantly, some men expressed a preference for avoiding healthcare altogether, viewing it as a sign of vulnerability. This is consistent with studies showing that men often delay or avoid seeking care for fear of being perceived as weak or less masculine (Cheatham et al., 2008; Hunter, 2006; Leone et al., 2017). Future interventions should focus on normalizing health-seeking behaviors by linking them to protective masculinity ideals. Studies have shown that men who view their health as essential to fulfilling their roles as providers and protectors are more likely to seek care (Daniels et al., 2021; Idris et al., 2019; Sileo et al., 2018). Therefore, public health efforts should capitalize on these ideals to promote men’s engagement in HIV prevention and broader healthcare services.
The study has some limitations to consider. Firstly, many participants were research-experienced and there may have been a level of social desirability bias where participants were more likely to say what they thought researchers would want to hear (white coat effect), versus what they really felt. A key limitation is that men’s responses regarding gender norms may have been influenced by dominant structural beliefs and societal stereotypes rather than reflecting their personal ideals of masculinity. As a result, participants may have conformed to socially accepted narratives, which could obscure more individualized or aspirational views of masculinity. This social desirability bias may have limited the depth of insight into the participants’ personal attitudes toward gender norms. However, we counteracted this potential bias by asking men what they thought themselves, and how they thought other men might feel to minimize social desirability around issues of potential discrimination. Additionally, the study focused on peri-urban and urban dwellers, and perspectives might differ in rural settings, particularly in terms of acceptance of individuals with differing sexual identities. Lastly, the study’s inclusion of participants from only two cities in South Africa limits the generalizability of findings. Nevertheless, these insights remain valuable for informing health and community interventions and support systems promoting positive masculinity and men’s well-being.
Conclusion
In conclusion, the study highlights the complex interplay between gender norms, sexual identities, and health-seeking behaviors among men in South Africa. While traditional masculinity continues to shape men’s roles and expectations, there is an emerging recognition of self-love and emotional well-being as essential components of masculinity. For MSM, the compounded pressures of gender and sexual identity highlight the need for culturally sensitive interventions that address both mental health and healthcare access. Further research in diverse populations and settings is needed to deepen our understanding, inform targeted interventions, and ultimately address the complex dynamics of self, family, and community perceptions of an ideal man, which is crucial for promoting healthier masculinities and improving the well-being of men.
Footnotes
Acknowledgements
The authors would like to thank the men who participated in the SAMURAI study, site leaders, and protocol team members who contributed to the development, implementation and/or analysis of this study. The authors would also like to thank the site qualitative staff, Miriam Hartmann, and Zoe Duby for their contribution to codebook development and coding.
Author Contributions
AMY and ETM managed qualitative data and ZD and ST did coding. AMY and MM generated qualitative themes and did qualitative analysis. AMY, ST, MA, TP, AMM, and ETM, conducted data collection and quality control of transcripts. MA, TP, AMM, and ETM, all over saw study implementation. AMY led manuscript writing with support from MM, ZD, and ETM. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institute of Mental Health of the National Institutes of Health under award number R01MH121148. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.