
Abstract
Men represent a proportion of those with eating disorders yet are neglected in the existing literature. One area with limited research is how men with eating disorders experience body image. This study investigated how men with eating disorders make sense of their experience of body image. Ten male participants with diagnosed eating disorders were recruited from four National Health Service specialist adult eating disorder services. Semi-structured interviews were conducted, and data analysed with Interpretative Phenomenological Analysis. Analysis identified three themes: ‘Focus on Self’, ‘Focus on Others’ and ‘Systemic Influences and Pressures’. Findings indicated that body image was experienced intrapersonally, interpersonally, and systemically. This study adds to the limited accounts of body image among men with eating disorders. It is recommended that future research explore body image in underrepresented gender and sexuality groups and that clinicians incorporate the nuances of men’s experiences of body image into clinical assessment and treatment.
Eating disorders are a group of mental health conditions characterised by a desire to lose weight, an extreme fear of weight gain, and over-valuation of body image (Morris & Anderson, 2021). Diagnostic criteria differ for the types of eating disorders: anorexia nervosa involves restricting food intake below energy requirements; bulimia nervosa involves recurring episodes of binge eating and compensatory behaviours to prevent weight gain; and binge eating disorder is defined by regular episodes of eating large quantities of food and feeling a loss of control (American Psychiatric Association, 2013). However, diagnostic requirements across the different types involve abnormal eating behaviour and preoccupation with food, accompanied by prominent concerns with weight or shape (World Health Organisation, 2022). Eating disorders often have a long-term and chronic presentation (Steinhausen, 2002; Ward et al., 2019) and are associated with a higher risk of mortality and a reduced quality of life (van Hoeken & Hoek, 2020). They also have a burdening impact for carers (Raenker et al., 2013), and high economic costs for health services and society (Kessler et al., 2009; Samnaliev et al., 2015; Streatfeild et al., 2021). Many individuals with eating disorders do not seek support from services (Bohrer et al., 2017; Hart et al., 2011). Of those who do seek treatment, a small proportion receive evidence-based eating disorder treatment (Mond et al., 2007; Von Ranson et al., 2013; Waller, 2016) and recovery rates are considered optimistic but slow (Hay, 2020), with lower rates for those with anorexia nervosa in comparison to bulimia nervosa (Eddy et al., 2017). Funding for eating disorder research is limited in comparison to other mental health difficulties (Woelbert et al., 2021), which may be due to the associated stigma with eating disorders among mental health professionals and researchers (Solmi et al., 2021). Therefore, further research is required to understand the nature and treatments of eating disorders to address their marginalisation in mental health research.
Men with eating disorders make up an estimated 10–25% of affected individuals (Hudson et al., 2007; Sweeting et al., 2015; Weltzin et al., 2005), with lifetime prevalence rates estimated to be around 2.2% for men and 8.4% for women (Galmiche et al., 2019). Despite the proportion of men affected, eating disorders are commonly viewed as a female issue, and cultural stereotypes portray them in such a way (Sweeting et al., 2015; Till, 2011; Wooldridge & Lytle, 2012). This portrayal is problematic because it may create barriers to recognising and treating eating disorders in men. Men may delay seeking help because of the perceived stigma associated with having an eating disorder (Räisänen & Hunt, 2014). Even when men seek treatment, they are more likely to receive a misdiagnosis, such as depression, and less likely to receive an eating disorder diagnosis than women, despite presenting with similar symptoms (Currin et al., 2007). Less than 1% of empirical eating disorder studies have investigated male presentations (Murray et al., 2016), contributing to an incomplete understanding of eating disorders among men (Mitchison & Mond, 2015; Murray et al., 2017), and the recommendation for future research to focus on men’s experiences (Scottish Intercollegiate Guidelines Network, 2022).
Differences in eating disorder presentations between men and women have been reported, though evidence is sparse. This research indicates a greater prevalence of physical activity and compulsive exercise among men as compensatory behaviours (Lewinsohn et al., 2002; Murray et al., 2014; Strober et al., 2006), whereas excessive use of laxatives is less common in men than women (Button et al., 2008). Men are also more likely than women to experience comorbidities with other mental health difficulties (Carlat et al., 1997; Striegel-Moore et al., 1999), although more recent evidence suggests this gender difference is small (Ulfvebrand et al., 2015), and appear to have a later onset of eating disorders than women (Gueguen et al., 2012; Hoek, 2006; Hudson et al., 2007). Clinicians working with men have identified male-specific eating disorder features, such as a focus on fitness, and a need to adapt treatment for men, with some reporting not feeling confident to make these adaptations (Kinnaird et al., 2018). Previous research suggests that there is a notable gender difference with body and shape concerns among individuals with eating disorders, with men having less of a desire for thinness than women (Darcy & Lin, 2012; Joiner et al., 2000; Stanford & Lemberg, 2012). Men with anorexia nervosa often have body shape concerns related to muscularity (Murray et al., 2012), and men are more likely to have a preference to lose fat and develop muscle than women with eating disorders (Núñez-Navarro et al., 2012). However, research is limited, with few studies investigating men’s body image concerns in clinical samples and little detailed understanding of how men with diagnosed eating disorders experience body concerns.
Studies with non-clinical samples have established gender differences in body ideals between men and women (Grossbard et al., 2009; Jones & Crawford, 2005; Murray & Touyz, 2012; Ridgeway & Tylka, 2005; Tiggemann et al., 2008). Body ideals shift according to sociocultural context, with current Western ideals promoting not just a thin ideal, but a toned and slim body (Aniulis et al., 2021), and a ‘slim-thick’ body for women (McComb & Mills, 2022; Overstreet et al., 2010; Webb et al., 2013). For men, Western ideals emphasise a muscular and lean body (Edwards et al., 2014; Thornborrow et al., 2020), and the promotion of this ideal on social media (Holland & Tiggemann, 2016) is potentially detrimental to men’s body image (Gültzow et al., 2020; Tiggemann & Anderberg, 2020). High levels of body dissatisfaction are associated with an increased risk of developing eating disorders in men and women (Dakanalis et al., 2015; Olivardia et al., 2004; O’Gorman et al., 2020), and body image concerns related to muscularity have been found to predict increased disordered eating in men (Calzo et al., 2016; Compte et al., 2015; Hoffmann & Warschburger, 2017). Disordered eating behaviours directed towards building greater musculature or muscle leanness include severe dietary restriction of non-protein foods, excessive protein consumption, continued eating despite feeling full, and use of appearance-enhancing substances (Mosley, 2009; Murray et al., 2012). Murray et al. (2016) note that these behaviours are distinct from traditional eating disorder behaviours, and that men with these concerns experience challenges with diagnosis and treatment, given that diagnostic classifications focus on thinness-oriented concerns and behaviours. This focus may marginalise men with muscularity-oriented eating disorder behaviours, maintain the view that eating disorders among men are rare, and contribute to preventing men accessing eating disorder treatment.
Although previous studies provide useful findings for body image concerns and disordered eating in men, these mostly relate to non-clinical samples. There is limited research focusing on specific aspects of body image in men with diagnosed eating disorders, when body and shape concerns become pathological; that is, when there are disturbances in the experience of body shape and weight, as reflected in diagnostic criteria for anorexia nervosa and bulimia nervosa (American Psychiatric Association, 2013), and control of body shape and weight are central to a person’s self-evaluation as part of eating disorder psychopathology (Fairburn et al., 2003). This differs from body dissatisfaction, which is relatively common in the general population, affecting around 10%–30% of men and 20%–40% of women (Frederick et al., 2012). Understanding how pathological concerns with body image are experienced by men with eating disorders is an important focus for research to ensure that clinical practices recognise and respond appropriately to men’s experiences.
Given current limited understanding, qualitative research exploring body image in men with eating disorders could provide valuable insights into clinical presentations (Murray et al., 2017). A qualitative approach is concerned with rich descriptions and capturing the individual person’s perspective (Denzin & Lincoln, 2000), allowing for in-depth understanding of complex and under-researched phenomena (Korstjens & Moser, 2017). A number of published qualitative studies have examined different aspects of men’s experiences of eating disorders (for a review see Coopey & Johnson, 2022), such as seeking and receiving treatment (de Beer & Wren, 2012; Dearden & Mulgrew, 2013; Räisänen & Hunt, 2014; Robinson et al., 2013; Thapliyal et al., 2020), recovery (Pettersen et al., 2016), differences in symptoms between males and females (Arnow et al., 2017), and role of masculinity (Drummond, 2002). Findings have highlighted men’s experiences of tension between being thin versus muscular (Arnow et al., 2017), a preoccupation with body size and disgust towards their personal appearance impacting masculine identity (Drummond, 2002), and that pursuing fitness is linked with a physical identity of being slim and muscular (de Beer & Wren, 2012). However, none of these studies specifically explored how men with eating disorders experience body image. The aim of this study was therefore to obtain detailed insights into the perceptions and meanings of body image in men with eating disorders. The research questions were: 1. How do men with eating disorders experience body image? 2. How do men with eating disorders make sense of their experiences?
Method
Design
Interpretative Phenomenological Analysis (IPA) was used to guide the study design, data collection, and analysis. In line with the principles of IPA, this study aimed to understand the experience (phenomenology) of men with an eating disorder (idiography) and how they make sense of body image as part of their experience (hermeneutics). Being ‘double hermeneutic’ is key within IPA, where the findings reflect the researcher’s interpretation of each participant’s retelling and understanding of their experience (Smith et al., 2009). Semi-structured interviews were employed to allow for detailed, personal, and contextualised accounts of participants’ lived experience (cf. Smith et al., 2009).
Participants
Participant Demographic Information.
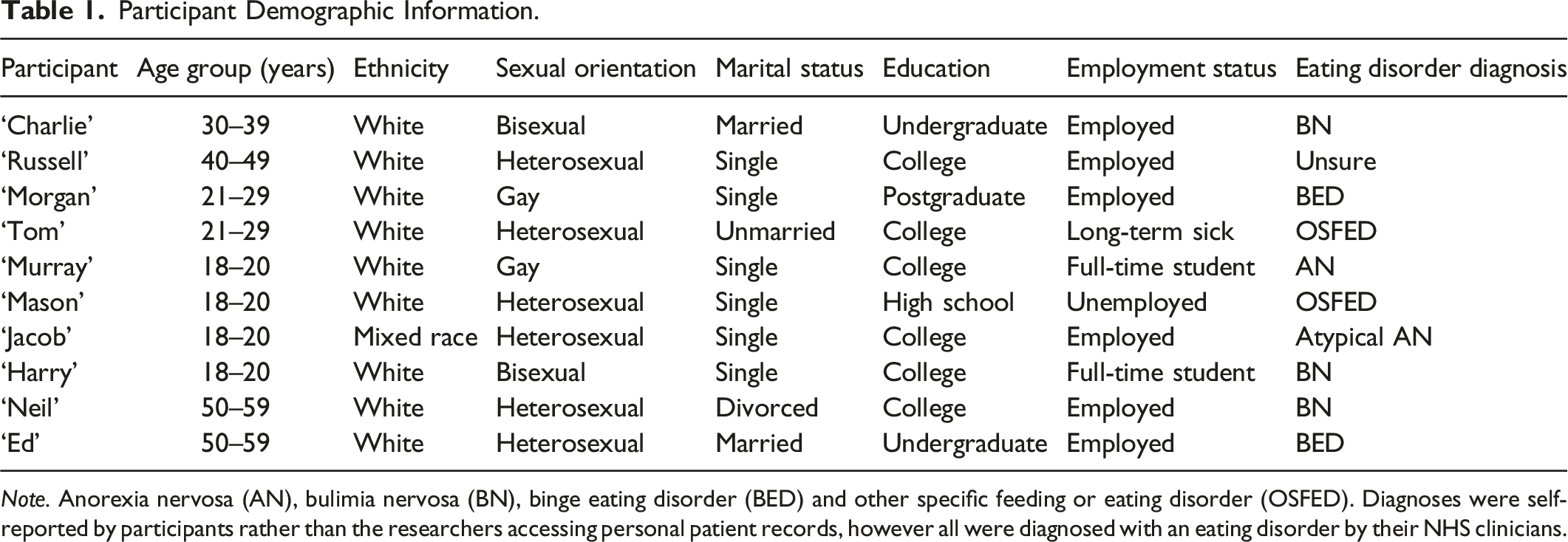
Note. Anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED) and other specific feeding or eating disorder (OSFED). Diagnoses were self-reported by participants rather than the researchers accessing personal patient records, however all were diagnosed with an eating disorder by their NHS clinicians.
Procedure
Ethical approval was granted by the West of Scotland Research Ethics Committee (reference: 21/WS/0125). The researchers’ educational institute acted as the sponsor for the study. Recruitment took place in four specialist NHS services in Scotland which provide outpatient treatment to adults with eating disorders. Clinicians were asked to approach patients on their caseloads who met the inclusion criteria and provide them with information about the study. Potential participants could either consent for their clinician to pass their contact details to the lead researcher or contact the researcher directly.
All participants provided written consent to participate and attended a semi-structured interview conducted by the lead researcher (two face-to-face at NHS clinics, three by telephone call, and five by video call). A semi-structured interview schedule was developed based on IPA guidelines (Smith et al., 2009), themes in existing literature, and consultation with three experts by experience (men with lived experience of eating disorders who responded to an advertisement from the researchers’ research group Twitter account). Interview questions were developed to be expansive and open, and elicit participants’ experiences of body image and how it related to their eating disorder. Participants were encouraged to discuss their experiences at length, and prompted when necessary to move from the generic to the specific, and the descriptive to the affective. Each interview started with an unrecorded informal discussion to help build rapport, ease any anxiety, establish a plan for the interview, and confirm participants’ consent to record. At the end of the interview, participants were reminded of the study aims, had the opportunity to ask the researcher any questions, and were thanked for their participation. Participants then also completed a demographic questionnaire (age, ethnicity, sexuality, gender, marital and education status). Interviews took place between May and December 2022, and ranged in length from 51 to 93 minutes. They were digitally recorded on an encrypted dictation device and/or via secure Microsoft Teams and uploaded to a secure NHS server. Interviews were transcribed verbatim and anonymised by the first author. Pseudonyms are used throughout for participants’ anonymity.
Data Analysis
Data were analysed by the first author following the inductive and iterative ‘cycle’ described by Smith and colleagues (2009) involving a six-stepped procedure to generate themes: reading and re-reading transcripts, initial noting, developing emergent themes, searching for connections across emergent themes, moving to the next case, and looking for patterns across cases. Smith and colleagues (2009) suggest measuring recurrence across cases to help determine the key themes at a group level. The status of ‘recurrent’ was defined by a subordinate theme being present in half the interviews.
Given that the researcher facilitates the sense-making of the phenomenon in IPA (Smith et al., 2009), reflexivity is of upmost importance; that is, the process in which researchers evaluate and develop explicit awareness of themselves during the research process (Shaw, 2010). The first author considered their prior experiences of working with those with eating disorders as an assistant and trainee clinical psychologist, and how these experiences may have influenced existing ideas of what it means to have an eating disorder. The researcher has an interest in how men experience eating disorders, has their own experience of being male and what this means to them, as well as their own relationship with eating and body image. Prior understandings of the phenomena could both facilitate and neglect aspects of the research process, such as decisions to expand or not on experiences shared in the interviews, or how certain experiences were understood during analysis. The researcher took a reflexive stance throughout the research process by maintaining a reflexive diary, as recommended by Newton and colleagues (2012).
Quality in qualitative research can be demonstrated, enhanced, and evaluated with the following principles: sensitivity to context, commitment and rigour, coherence and transparency, and impact and importance (Yardley, 2000, 2008). To address sensitivity to context, relevant previous research was outlined in the Introduction and a questionnaire was used to gather demographic and background information about participants. IPA is centred on close engagement with the idiographic and verbatim extracts from interviews were used here to demonstrate sensitivity with evidence from the raw data (cf. Smith et al., 2009). Commitment and rigour refer to sufficiently detailing the analysis to ensure that the validity of results can be evidenced (Yardley, 2000). The first author conducted the analysis, which was discussed, challenged, and revised with co-authors throughout the process. A credibility check was conducted through a ‘mini-audit’ (Smith et al., 2009) completed by a co-author (EN) and a further audit by a researcher independent of the research team and research field (MZ) on the analysis of another participant’s data. It was designed for the study to include interviews with eight to ten participants to collect enough data to ensure a sufficient analysis was achieved and to represent individuals’ experiences in depth, as recommended for professional doctoral IPA studies (Smith et al., 2009; Turpin et al., 1997). Given the large sample size, extracts were judiciously selected to allow for appropriate illustrations for each theme and accounts drawn on even-handedly. Coherence and transparency are the extent to which the interpretation is clearly derived from the data and all relevant research processes are disclosed (Meyrick, 2006). A ‘transparent pathway’ (Meyrick, 2006) was implemented through an audit trail, to evidence the process of developing transcript data to the final write-up. Impact and importance were considered when relating the interpretation of findings to existing literature and theory and clinical practice.
Results
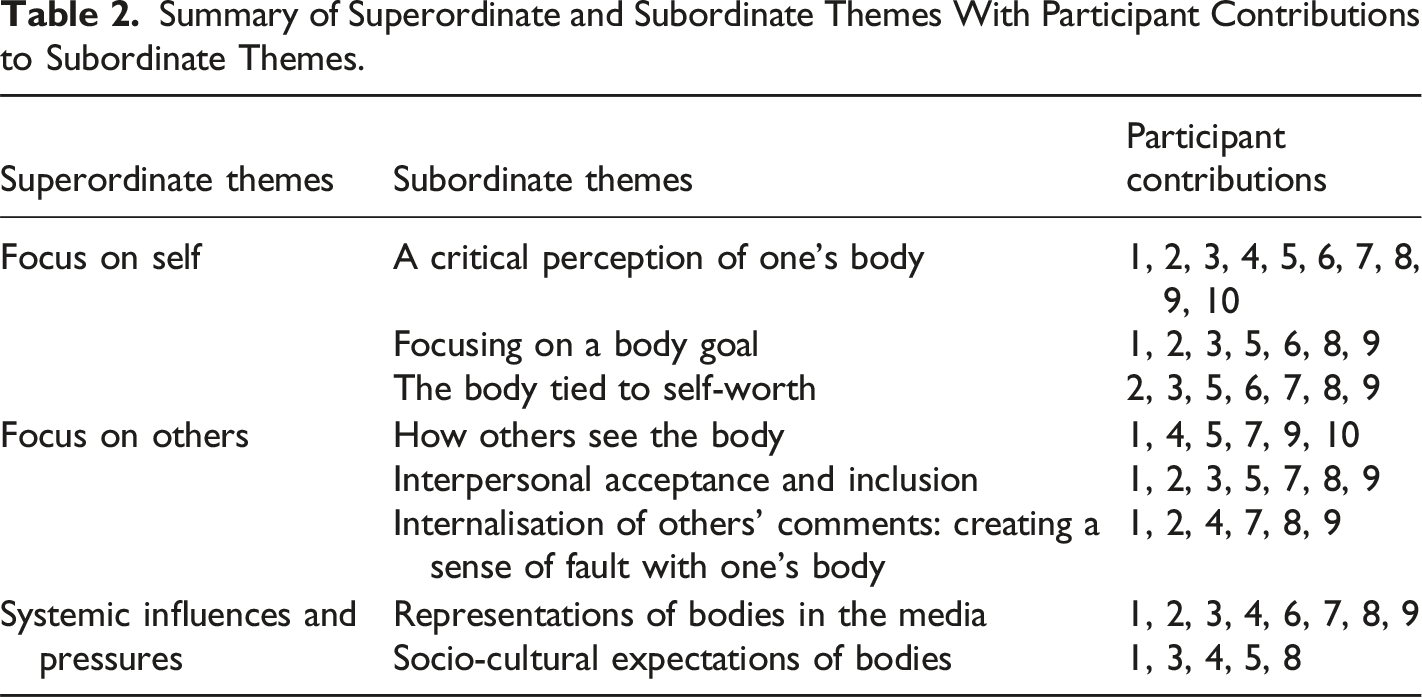
Summary of Superordinate and Subordinate Themes With Participant Contributions to Subordinate Themes.
Superordinate Theme One: Focus on Self
The first superordinate theme captures how participants experienced body image with a specific focus on themselves and their inner world, and different emotional meanings attached to their bodies.
Subordinate Theme One – A Critical Perception of One’s Body
All participants described a negative and critical perception of their bodies. It was felt “everyone is their own worst critic” (Charlie), with a critical internal dialogue towards the self and the body, such as participants reflecting “I’m quite critical of myself” (Mason) and “there’s a bit of self-loathing in there” (Neil). This is captured intensely by Tom: You’re your own worst critic. Anytime that I look in a mirror, I look at something and it could be anything and be like, ‘ohh you’ve got this wrong. You’ve got that wrong’. Um, I hate looking in the mirror, it makes me feel like I resent my body. But at the same time…. I’m trying to change how I look, but I’m going the wrong way about it. – Tom
Tom’s account suggests he is highly critical towards his body, with his repetition of “wrong,” following scrutinising and focusing on perceived defects with his body. His use of “I resent my body” indicates the strong negative emotional reaction to his body. Tom alludes to attempting to address his perception and emotions around his body with his eating disorder, but he acknowledges this is problematic, with use of “I’m going the wrong way about it”. A negative perception of and emotional response to the body is similarly experienced by Russell, who focused on fatness: I think just…. I don’t like fat (laughs)…. I don’t like a huge amount of excess weight and I find that really kind of repulsive (laughs). I know that sounds terrible…. I used to look at myself in the mirror and if anything was kind of hanging, I’d think ‘this is disgusting’. – Russell
Russell’s internal dialogue when he perceives fat on his body is fatphobic towards himself, which he acknowledges as problematic. Nevertheless, his emotions are strongly negative, with his use of powerful descriptors, such as “repulsive” and “disgusting”. His laughter when describing this represents some discordance between his language and manner, suggesting humour possibly being a coping mechanism to minimise or detach from distressing emotions and thoughts.
Others experienced difficulties with their perception of their bodies, some perceiving it negatively and some experiencing a distorted perception of the body. Participants recognised that their perceptions were not always reliable or accurate: Uh, so like, I mean, whenever I look in the mirror, it’s like different (laughs). So yeah, it’s…. I don’t know. Uh, yeah, it’s… Yeah, I, I don’t…. I don’t like it. Uh, but like it changes. But I’m never, I’m never like…. I don’t know, happy with it… Umm, it’s… just sometimes I look in the mirror and I’ll see myself as thin. And then sometimes I still see myself as like fat, so it just kind of alternates…. You don’t trust what you see and so you listen to that critical voice. – Murray
Murray’s confusion with his perception of his body is illustrated by his repetition of “I don’t know,” suggesting an uncertainty of his own perception; from perceiving his body as “fat” at times, but also as “thin.” Even though his perception changes, the emotional relationship with his body remains negative, and because of the mistrust, he relies on further critical self-talk towards his body.
Subordinate Theme Two – Focusing on a Body Goal
The majority of participants shared desires and goals for their bodies. Many experienced distress if their body was incongruent with their goals. Three participants reflected on this, two similarly wanting “to be as thin as possible” (Charlie) and to “be as thin as possible … like, the most bones showing” (Murray). Harry explained what a goal for thinness meant to him: I always had this weird sort of image in my head of … you know, you’re somehow sort of… slim, but not to the point where it was like you were a toothpick, you know?.. I would always sort of find… a part of myself, whether it be sort of like ‘ohh yeah no my lower back is too, is too thick’. – Harry
Harry’s account indicates a want to be slim, though not too thin, with his use of the “toothpick” metaphor. He illudes to an unhelpful cycle where he would look for perceived defects with his body and if his body did not meet his thinness goal, this would be distressing and his fixation on his body would increase.
Rather than striving for thinness, four participants shared a goal for their bodies to be “muscular” (Morgan), with a focus “all about fitness and strength” (Russell). Mason’s experience encapsulated his intense drive to achieve muscularity: Erm, so that’s what I’d always work towards … is being really lean and strong, but that’s really difficult to achieve so that’s why it comes with the high standards…. I thought ‘right, I’m really going to go for this fitness thing’. I was going to do as much as I can for it. Er, so that made it a lot worse I think. That was my new goal… perfect health, perfect fitness, you know. – Mason
Mason acknowledges that his perfectionistic goal for leanness and muscularity requires high standards and is hard to achieve. Reaching his ‘perfect’ body goal required him acting towards this goal “as much” as he could. Mason recognises in hindsight this was problematic for his eating disorder, with his use of “that made it a lot worse”.
Subordinate Theme Three – The Body Tied to Self-Worth
The third subordinate theme encapsulates the majority of participants’ experiences with their body image being key to their self-worth. This was highlighted as a varying emotional experience, positively and negatively impacting the self, evidenced in part by Harry: …if you think of like a pie chart of how people would sort of think about… their own self, like, body image would take up some sort of part of that. And overtime, that sort of body image section of the pie chart sort of slowly and slowly got more eaten up by sort of actual… erm, sort of control…. And then that will mean ‘OK, so how do I make myself feel good about my body or how do I make myself feel less terrible about my body? If I have some sort of control over it, well I’ll binge and purge’ … the pie chart just started to grow and grow and grow because the more control I felt I had over my weight … was the more … good I was able to feel about myself. – Harry
Evident in Harry’s description is that his body image is increasingly significant in how he determines his self-worth. Harry uses a pie chart analogy to represent ways of determining his self-esteem and how his body, then control and his weight, has become the dominant way of judging his self-worth. Harry reflects on how controlling his body made him feel good about himself and “less terrible” about this body. This pie chart analogy is common in cognitive behavioural therapy for eating disorders and may be how Harry’s eating disorder and self-esteem were conceptualised during treatment, impacting how he made sense of his experience. Similarly, Murray reflected that “body image is kind of what I’m like worth or who like who I am”, but elaborated on the positive impact controlling his body had on his sense of self-worth: It’s, it’s … you find achievement in it. You find success in it. You finally feel like you’re good enough and if there’s progress… quite often like there is. Like with losing weight, like it’s…. I can lose weight quite quickly. So I got like really hooked on to that … um … and so that kind of … so there’s a lot of like achievement and just trying to be like…. And then there’s also the kind of thing of being like the best anorexic. – Murray
Like Harry, Murray’s experience echoes positive ways controlling the body, as well as weight, can influence self-esteem. Losing weight seems to boost his self-esteem, particularly when having an overall negative view of himself, as suggested with “feel like you’re good enough” when he was able to control his weight and body. Engaging with disordered eating behaviours to influence his self-esteem is described in an almost addictive way, with use of “really hooked”, in relation to the sense of accomplishment he feels. Mason also experienced his body in this way, as “the main driver of my self-esteem and how I would feel about myself”, but he acknowledged the problematic nature of judging himself based on his body: It was … it was difficult because naturally not being able to look perfect would always mean that my self-esteem would never be great. I’d always be working towards improving it. It really, it really drains your confidence when you don’t like how you look. It makes you less sociable, just not yourself as much. - Mason
In Mason’s account the impossibility of his body meeting his standards of perfection resulted in his self-esteem being poor. His continued attempts to improve his body to feel good about himself negatively impacted his social life and meant he did not feel like himself. He reflected on these attempts as having been unsuccessful and in hindsight realising judging himself according to “perfect” body image is problematic.
Superordinate Theme Two: Focus on Others
The second superordinate theme describes the interpersonal experience of body image, in contrast to the intrapersonal experience encapsulated by the first superordinate theme.
Subordinate Theme One - How Others See the Body
More than half of participants experienced distress around their body image, not only in relation to how they view their own bodies, but how they assumed others would perceive their bodies. Body image was viewed as “how I see myself and how other people see me” (Tom) and “how I think other people see me, not only just how I see myself” (Murray). Neil’s experience of body image and the perception of others captured how others’ perspectives are taken into account: Everything I do is about… the end result is how, how I look… how I think I look and how I think I’m perceived by everybody else… But it’s just my perception of how my body looks… how others are going to perceive me. – Neil
Neil’s account emphasises how he perceives his body relates closely to how he believes others may think his body looks, giving this more credence than his own perception. His use of “everything” highlights how the behaviours he does to influence his body, “the end result”, is driven by how other people will view his body.
For several participants, thinking about how others perceived their bodies involved predicting that their perception would involve negatively evaluating their bodies and them as people based on their bodies, such as being “big and clumsy” (Tom) and believing others “hate me, um, because of my weight and the way I look” (Jacob). Charlie spoke of the intensity of this: … get that feeling that people are looking at you, judging you on how you look and think if I’m fat…. I will be constantly thinking that people are doing that to me … they’re looking at me and thinking, you know, ‘he’s letting himself go’. – Charlie
Charlie’s emphasis here is on judgement and negative evaluation of his body by others, but also about him as a person with his use of “judging you on how you look”; a sense that others’ perception of the body extends beyond the body itself, but to the person as a whole. Ed experienced this in a similar way but elaborated on the emotional experience of this: I probably feel self-conscious about what other people think, you know, whether ‘that fat bugger sitting over there’ type of thing … vulnerable in the way that, that how are other people perceiving me? How are other people thinking about me? What are other people seeing? Because I don’t like what I see. – Ed
Ed’s account captures negative comments about his body that he believes others may be thinking, in an evaluative way similar to Charlie, but he links these predictions to his own negative perception of his body. Predicting such body evaluations impacts the self emotionally in a negative way, as illustrated with his use of “self-conscious” and “vulnerable” which emphasises how hard this can be for him.
Subordinate Theme Two – Interpersonal Acceptance and Inclusion
A focus on other people is a feature of the second subordinate theme with interpersonal relationships. The theme is captured succinctly by Neil stating that being “loved, liked or approved by other people is significantly impacted by what I would think, like ‘am I fat or not?’”. Charlie described how he experiences his body and romantic relationships to be linked when discussing a previous romantic relationship: So I was thinking ‘I can’t eat, I can’t eat and not do anything about it, she’s gonna leave me’. She was quite popular and she had quite a lot of friends… she had male friends … who I considered to be attractive and, um, she had a lot more friends than I did. So you’re almost thinking her friends are saying I’m not good enough for her…. I think that’s when I…. I recall, um, properly falling into the trap of an eating disorder. – Charlie
Charlie’s account highlights how he felt his body played a part in his relationship with his girlfriend at the time; feeling his body was inadequate and this would be a reason for potential romantic abandonment. His relational concerns linked with his body further when he described feeling the need to change his body through restricting his eating and the eating disorder intensity increasing. His comparison to the appearance of other men further added to his feelings of inadequacy. Morgan also spoke of the romantic interpersonal aspect to how he felt about his body in which he would use niche gay dating apps for men who like men with larger bodies: …if someone has said to me, you know, ‘I love the shape of your chest’ or ‘I love this about you’ and I’m like, you know, ‘yeah, I feel like good and I don’t know curvy or something today’. But … um … I think I’m very kind of focused on… the idea of the body as like a sexual object or a, you know, an object of attraction. So for me, feeling good about my body or not so good … obviously I want to be healthy and stuff, but good and not good as based upon how attractive I feel I am to others. – Morgan
Evident is that Morgan’s body image is influenced positively by being valued by other men viewing him in an objectified way. Yet, this interpersonal validation of his body is also conflicting for him, acknowledging the positive side to feeling attractive to others, but also problematic side with relying on this as the only criterion to feel good about his body.
Social acceptance and inclusion with the body was also experienced among four participants and is captured strongly by Jacob: I was getting compliments from people. I was getting compliments from the … ‘oh look how much weight you’ve lost, you’re looking great’. Um, it was… it kind of fuelled me a bit more, ‘you can keep going, you can keep going’…. A lot of people seemed to kind of take more of an interest in me and in my life, and how I feel. And it kind of made me feel, feel a way that I’d never felt before…. Um, it made me feel happy. It made me feel wanted, included. Especially for being bullied for … the majority of my life I kind of felt…. I kind of felt like you’ve finally been accepted. – Jacob
How others interacted with Jacob in a positive way, giving attention and compliments about his body as a result of weight loss, is a stark contrast to the experiences of being bullied from a young age and being socially deprived, which seemed to be a driving factor to motivating the eating disorder. Jacob experienced the change in his body and positive comments by others as rewarding as this meant he was socially accepted and he valued this.
Subordinate Theme Three – Internalisation of Others’ Comments; Creating a Sense of Fault with One’s Body
More than half of participants described negative early experiences of people commenting on their body and weight. These experiences were felt to have impacted their body image negatively, and were felt to have “stemmed from that, it’s followed me through” (Tom) and “made me feel alienated because … I, I was bigger” (Harry). Neil’s experience of weight and body bullying had a profound impact on him: Basically, basically my first memory was being in the village primary school and kind of kicked to the ground, er, with a circle of kids around me shouting ‘you fat bastard, you fat shit’, all this kind of stuff…. So that’s (laughs) kind of shaped everything really since then…. I think because of the trauma as a child, you know, and the experience that everyone was focusing on my weight. – Neil
Neil’s description of being emotionally and physically bullied based on his body illustrates a key experience, of many he described enduring, in which others attended to his weight and body negatively. His use of “trauma” captures the distress he still feels from others being critical of his body. His use of “shaped everything” highlights how these experiences were salient to him feeling negatively about his body and developing the eating disorder. Jacob also spoke of his internalisation of negative comments by others and the emotional impact this had on him: It was brought up quite a lot by people … people would call me ‘fat’ or call me things like that. Ever since people started kind of bringing that stuff up to me it, it kind of made me feel different to everybody else. I would feel ashamed and stuff like that…. Yeah, I should feel ashamed … and as if it’s…. I’m not right for it, erm, definitely… it definitely … ‘cause quite a lot of people pointed it out. - Jacob
Evident in Jacob’s experience is that he internalised these experiences cognitively in a self-evaluative way to feel abnormal about the self because of his body, with his use of “different to everybody else” and “not right for it”. Beyond influencing his cognitive internal world about the self and his body, these experiences led to shame-based emotions about his body.
Superordinate Theme Three: Systemic Influences and Pressures
The third superordinate theme described wider systemic influences on how participants perceived their bodies. This superordinate theme encapsulates experiences of other systems that operate around the participants and how these impact the self.
Subordinate Theme One – Representations of Bodies in the Media
The majority of participants experienced the media and representations of bodies in a negative way in relation to their body image. They particularly emphasised the distorted sense of reality of bodies the media portrays, reflected as “the social media lie, you know, it’s just a photograph” (Charlie), and acknowledged the inaccurate representations of bodies; “an app like Instagram people will post their best photos in the best lighting with the most, the most editing… I think it’s quite a distorted app in general” (Mason). Mason described how these depictions of bodies on social media impacted him: It feels like that’s what you need to be almost, erm, because you’re just viewing it so much. And you don’t even notice it at the time but it does over the long-term have an impact…. I think what I view as healthy is and a good body I think was really distorted by that, by that app specifically. Maybe Instagram and YouTube as well. I think deleting Tik Tok had a big impact on my self-esteem. - Mason
Here, Mason reflects on how seeing this content created a standard for what his body ‘should’ be in the long-term, evidenced with his use of “what you need to be”. His deleting of Tik Tok was powerful for him and illustrates how negatively Tik Tok content must have impacted his body image and self-esteem before. Morgan also spoke about the impact of the media, but queer media specifically: I feel like, you know, from an early age, you’re kind of … when you start to, you know, interact with queer media and obviously porn and stuff like that. Everyone has… there’s a higher bar for what the average person looks like and you’re made to feel even more kind of abnormal there. – Morgan
For Morgan, in a similar way to Mason, the media impacted his idea of the ‘standard’ of what bodies should look like. The portrayals of bodies in queer media influenced specifically his sense of what queer men look like, particularly high body standards for queer men. Viewing these bodies from a young age impacted Morgan’s self-esteem negatively, with his use of feeling “abnormal”, as he was not meeting the standard set as a precedent for queer men by the media he consumed.
Subordinate Theme Two – Socio-Cultural Expectations of Bodies
Half of participants spoke about wider societal and cultural systems which impacted their eating disorder, body image and overall sense of self. Murray highlighted the impact at a systems-level of societal and cultural beliefs of bodies and eating: …it’s an actual experience which involves a relationship between you and like society or another community, like you’re not gonna want to … um, leave that. And you know, and also like… it is also you… I mean, in our society like dieting and diet culture like it’s such a huge like part of like our... people are always like dieting and stuff. And it’s, you know, and there’s all these different like … um … so, we live in a … a bit of a … like a like a Pro Ana society, a little bit almost. Everything’s kind of … like weight loss is like praised and weight gain is like shamed. And there’s a lot of emphasis on how you look. – Murray
Murray highlights the relationship between the self and society as a system, and the impact that society has on the self in valuing thinness, dieting and appearance. Murray’s body and eating attitudes are impacted by pervasive societal messages about the importance of appearance; his intra-psychic experience of attitudes to his body and eating link to his social context. His use of “Pro Ana” illustrates how strongly he feels what society values is akin to niche content which is positive towards and encourages eating disorder behaviour. Charlie’s experience of societal views of bodies offers some similarity, but some divergence to Murray: You know, men are kind of criticised and they use jokey terms like ‘dad bod’ and … ‘moobs’… and that actually is… it’s the same as those horrible magazine articles that put circles around women’s love-handles and that kind of thing…. And, erm, and the way men are talked about for having a dad bod … you all want to avoid that at all costs…. So there’s that kind of stuff … do I look feminine? Or, you know, I’m not a macho man…. I don’t look like a man…. I’m not a man. – Charlie
Charlie highlights a similarity of body shaming and fatphobic narratives in society for men’s bodies to how women experience this too. The prospect of his body being spoken about in such way seems to evoke distress and a want to avoid this, as suggested with “avoid that at all costs”. He also touches on the impact of societal standards of bodies to how he experiences masculinity; feeling his body does not fit the mould of a masculine body and how this impacts his sense of masculinity by equating not looking manly to not being manly.
Away from general societal views of bodies, three participants spoke of how views of bodies within queer community impact them. Murray spoke of how particular bodies are valued within the gay community: …like in the gay community like, men like it, there’s … there’s kind of like you either have to be like, really muscly or like really like, like thin or like, I mean, like twinkish (laughs) … but then like in the gay community is different because, like really like skinny guys are like desired. – Murray
In this excerpt, Murray highlights his experience as a gay man of body preferences within the gay community and identities or sub-groups being attached to particular bodies. Murray emphasising “really like skinny guys” being desirable to some gay men, may indicate a shift from the external, the queer community, to the internal, Murray, valuing a thin body. This may help contextualise why Murray idealises having a thin body as part of his eating disorder experience. Harry’s experience of being a queer man, identifying as bisexual, and operating as an individual within the queer community with an eating disorder was also experienced as difficult: I feel like … (pause) in the queer community there’s a much bigger emphasis, especially within men who love men … that, you know, body image does kind of come first… These feelings of ‘well, even that I have an eating disorder I need to conform to these sort of rigid stereotypes of how queer men should look. I should participate in that sort of circuit anyway’…. Even though it makes me incredibly uncomfortable to do so … Because otherwise you’re just not … you’re not queer enough. Otherwise you’re not really going to be accepted. – Harry
Harry’s reflection here is that for queer men body image is prioritised and views of bodies within the queer community holds different meanings to him. He describes an inner conflict for him to conform to body ideals for queer men, in order to be accepted, even though this painful for him and at odds with his recovery.
Discussion
This study is the first to explore body image in depth using a qualitative approach among men with diagnosed eating disorders. Three themes were identified: Focus on Self, Focus on Others, and Systemic Influences and Pressures. Participants were preoccupied with, and critical towards, the body, which was associated with shame and resentment. Body dissatisfaction is a common clinical feature of eating disorders among men and women (Dakanalis et al., 2015; Glashouwer et al., 2019; O’Gorman et al., 2020) and body shame has been found to be strongly related to eating disorder pathology (Nechita et al., 2021). Ways of addressing body dissatisfaction varied, with some focusing on muscularity and others striving for thinness. Previous evidence indicates that men with eating disorders are more concerned with muscularity than thinness (Darcy & Lin, 2012; Murray et al., 2012; Núñez-Navarro et al., 2012; Stanford & Lemberg, 2012) but this was not the case for all interviewed. The body, and ability to control it, was connected to participants’ sense of self-worth, which is consistent with cognitive behavioural conceptualisations of eating disorders pathology (Fairburn et al., 2003) and findings in women (Fairburn et al., 1993; Trottier et al., 2013).
Participants were highly concerned about other people evaluating their bodies, and judging them negatively as people. For some, a concern with others’ judgements may stem from early negative interpersonal interactions around their bodies. The interpersonal environment in which a person is raised is important to the development of body image (Duffy et al., 2021). Weight- and shape-bullying have been positively associated with purging and muscularity-oriented behaviour (Day et al., 2021), and appearance criticism from peers and pressure to increase muscularity are strong predictors of body dissatisfaction in men (Barker & Galambos, 2003; Jones et al., 2004; Xu et al., 2010). Participants felt that their bodies continued to affect relationships in adulthood, for example fearing rejection. Difficulty with interpersonal relationships is a predisposing and maintaining factor for eating disorders (Cardi et al., 2018; Treasure et al., 2020). Participants’ experience support theories that early experiences shape beliefs about self and other (Beck 1967, 1976; Young, 1999; Young et al., 2003). People with eating disorders are likely to report negative beliefs or early maladaptive schemas regarding the self and relationships with others (Boone et al., 2013; Maher et al., 2022), with body dissatisfaction found to correlate with several early maladaptive schemas (Maher et al., 2022). No studies have examined how men with eating disorders specifically experience early maladaptive schemas.
Sociocultural norms and values, such as body and weight shaming and valuing thinness (Brewis et al., 2011; Pearl, 2018), as well as social exclusion and isolation related to consequences of weight stigma (Arias Ramos et al., 2018; Carr & Friedman, 2006), were felt to influence body image and contribute to fears about acceptance and inclusion. Some participants raised the importance of appearance within the queer community, where particular body types are valued. A recent review similarly highlights greater appearance-related pressure in queer men (Bonell et al., 2023). To the researchers’ knowledge, these findings offer new insights into how body image is experienced by queer men with eating disorders, though narratives of fitting in based on their bodies align with previous qualitative research on body image in queer men (Austen et al., 2022; Jones, 2015; Morgan & Arcelus, 2009; Tran et al., 2020). Internalisation of body ideals, and media distorting their view of how normal bodies look, was highlighted as contributing to negative perceptions of the body. Previous findings also indicate that exposure to ideal bodies can significantly impact body dissatisfaction among men (Blond, 2008; Tiggemann & Anderberg, 2020), and appearance-focused social media is associated with eating disorder symptoms in women (Donovan et al., 2020; Fitzsimmons-Craft et al., 2020) and men (Griffiths et al., 2018; Holland & Tiggemann, 2016).
Strengths and Limitations
This is the first qualitative study exploring how men with eating disorders experience body image and addresses existing gaps in the literature in this area (Murray et al., 2017; Scottish Intercollegiate Guidelines Network, 2022). By recruiting through NHS services, only participants with clinician validated diagnoses were included, rather than relying on self-report. The sample was comprised of individuals with various eating disorder diagnoses which share similar psychopathology. This can be considered a strength, given that studies tend to focus on anorexia nervosa and bulimia nervosa and research into body image difficulties among those with binge eating disorder is sparce (Lewer et al., 2017). However, it is recognised that homogeneity may have been enhanced by focusing on particular diagnoses. Similarities and differences in body image among men with specific diagnoses could be addressed in future research. As participants were receiving treatment within NHS eating disorder services, gathering information on treatment type, length, and exposure may have offered further context for analysis. For example, some participants used concepts and terminology aligned with cognitive behavioural therapy for eating disorders. The lead researcher was familiar with this from professional experience in eating disorder services, therefore this was reflexively noted during analysis, as it potentially affected how experiences were interpreted. The first author aimed to maintain a reflexive stance at all stages and consider how some of the accounts of the participants were related to personal and professional experiences. Negative interpersonal interactions about appearance when young, identification with experiences of body preferences and stigma in the queer community, and professional interest in psychological therapies and systemic thinking may have impacted sense-making and interpretations. Most interviews were conducted by telephone or video call, and although rapport was built across all interview formats, it is recognised that attending to non-verbal cues was easier in face-to-face interviews, which helped guide the interview. A further limitation is that participants were predominately of white ethnicity. Indeed, participants were sampled from Scotland where the majority of the population identify as white (Smith & Simpson, 2015). The current analysis therefore does not capture the intersectionality of ethnicity and gender in experience of body image among men with eating disorders. Previous research has highlighted the need to understand eating disorder experiences within different ethnic groups (Rodgers et al., 2018) and the relevance of intersectionality in women’s body image (Brady et al., 2017). Therefore, this is an important area for future research to explore.
Implications for Research and Practice
Based on novel findings from this study, future qualitative research could explore in more detail how queer men with eating disorders experience body image. As only cis-men with male gender identities were included, qualitative research could also investigate how body image is experienced by people with eating disorders across the gender spectrum, including those who are transgender and non-binary. Both recommendations may lead to new understandings in these populations, given that lesbian, gay, bisexual, and transgender (LGBT) people experience greater incidences of eating disorders and disordered eating behaviours than heterosexual and cis-gender people (Parker & Harriger, 2020). To expand on the interpersonal aspects of body image that the present analysis revealed, future research could explore whether body image concerns are correlated with or predicted by interpersonal difficulties, fear of negative evaluation by others, or maladaptive schemas among men with eating disorders. Previous qualitative research on male body image among non-clinical populations has found health physiology and physical appearance to be of importance to men, and external factors to have an influence on the body image experience (Hargreaves & Tiggemann, 2006; Morgan & Arcelus, 2009). This is similar to some of experiences captured by the intrapersonal and systemic themes found in the current study. However, the interpersonal experience to body image has not been demonstrated in previous research among non-clinical samples, which was strongly captured as part of the body image experience among men with eating disorders by the current findings.
Findings support previous recommendations that muscle-orientated body image concerns should be assessed and considered within treatment for men with eating disorders (Murray et al., 2016). The same argument can be made for thinness, which was a concern for some men in the sample. Where interpersonal concerns with body image are present, clinicians could consider formulating and addressing these within recommended treatments for eating disorders (National Institute for Health and Care Excellence, 2017; Scottish Intercollegiate Guidelines Network, 2022), such as cognitive behavioural therapy for eating disorders (Fairburn, 2008; Waller et al., 2007) or the Maudsley model of anorexia nervosa treatment for adults (Schmidt et al., 2014). Men presenting with considerable interpersonal concerns may benefit from psychological therapies with a greater focus on interpersonal relationships, such as interpersonal psychotherapy (Rieger et al., 2010), cognitive analytic therapy (Newell, 2012) or schema therapy (Simpson & Smith, 2019) for eating disorders, as an adjunct or alternative as recommended by other guidelines (NHS Education for Scotland, 2014; Scottish Intercollegiate Guidelines Network, 2022). Compassion-focused therapy for eating disorders (Goss & Allan, 2014) may offer a useful adjunct or alternative (Steindl et al., 2017) for those with high levels of shame and self-criticism.
Conclusion
Men with eating disorders identified a critical perception of their bodies and specific goals for their bodies, with body image central to their self-worth. Body image was strongly linked with how others might perceive and evaluate them, which was related to early experiences of appearance-based bullying, and wider systemic influences and discourses. Future research should investigate novel findings regarding interpersonal concerns and body image among men with eating disorders, and explore how body image is experienced by people with eating disorders across the sexuality and gender spectrum. Clinicians working with men with eating disorders should consider the complexities of body image as part of assessment, formulation, and treatment.
Footnotes
Acknowledgements
The contribution of the NHS clinicians of all four services is greatly appreciated. The support with recruitment from the consultant clinical psychologists of services within other health boards is much appreciated – thank you Dr Sam Aitcheson, Dr Charlotte Nevison and Dr Louise Randell. Miriam Zoeller’s assistance with quality checking during the analysis process provided valuable feedback and input.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Committees: West of Scotland Research Ethics Committee 3 and The University of Edinburgh School Health in Social Science Research Ethics.