
Abstract
This study explores the perceptions and experiences of providers of eating disorder services towards men to understand the challenges and barriers experienced by both professionals and patients in addressing the gender bias within this field. A total of 21 professionals took part in the study. Using interviews and focus groups, the study explored service providers’ experience, understanding and knowledge in working with men with eating disorders using thematic analysis. Findings suggest that the growing issue of eating disorders affecting men, while a serious concern for practitioners, remains a ‘touchy subject’, a difficult and sometimes even uncomfortable topic for service providers to tackle. These findings provide insight into the challenges and barriers faced by professionals and men seeking help or treatment for an eating disorder and highlights the need for targeted training and resources to improve the eating disorders health literacy of service providers in relation to men’s experiences.
Introduction
Historically, men and boys have been overlooked in most approaches to eating disorders in socio-cultural and medical discourses. The focus has predominantly been on women and girls and on Anorexia and Bulimia Nervosa (Andersen, 1990; Wiseman et al., 1992; Weltzin et al., 2005; Greenberg & Schoen, 2008; Halbeisen et al., 2022a). This gender-biased narrative surrounding eating disorders is starting to change, most notably the adjustments made to the DSM-5 criteria to remove amenorrhea as a gendered criteria (Dakanalis et al., 2016). While there is little consensus on prevalence figures within the field, studies have suggested that men account for up to 25% of all eating disorder cases (Hudson et al., 2007). These findings indicate that the risks for men of both the onset and persistence of disordered eating behaviors are greater than previously thought (Dakanalis et al. 2015a; 2015b; Dakanalis et al., 2016), yet this group remains underdiagnosed, undertreated, and misunderstood (Strother et al., 2012; Murray et al., 2017). The reason for this underdiagnosis has started to be debated in recent years.
While prevalence figures vary greatly, evidence suggests that similarities outweigh the differences between genders in regards to psychopathology (Blashill, 2011), with studies suggesting that men and women do not appear to differ in terms of eating disorder severity (Dakanalis et al., 2017b, 2017a, 2018b, 2018a). Evidence has found that the core features, such as drive for thinness, impulse regulation, and body dissatisfaction remain similar across both genders (Fernandez-Aranda et al., 2004; Hay et al., 2005; Fairburn, 2008; Bunnell, 2010; Nunez-Navarro et al., 2012). Similarly, research has shown that treatment modalities are equally valid when tested with men and boys (Halbeisen et al., 2022a; Woodside & Kaplan, 1994; Fairburn et al., 2008; Dakanalis et al., 2014) and that being a man is not a predictor for poor treatment outcomes (Fairburn, 2008). As a result, there is an emerging field of literature exploring men’s experience of eating disorders (Robinson et al., 2012; Räisänen & Hunt, 2014; Griffiths et al., 2015).
However, the core diagnostic symptoms for eating disorders continue to be understood from a women’s perspective. A drive for thinness and “…intense fear of gaining weight or of becoming fat” remain central symptoms for diagnosing both Anorexia and Bulimia Nervosa (APA, 2013). However, these key determinants do not accurately account for the body dissatisfaction that underpins disordered eating in men. Men’s body concerns have been found to be different, and there is a clear prevalence for a drive for muscularity as opposed to thinness (Dakanalis & Riva, 2013; Lennon & Johnson, 2021). Furthermore, studies have shown behaviors and presentations in men are likely to stray from the traditional criteria presented in the Diagnostic Statistical Manual (APA, 2013). Many assessments place a focus on girls and women therefore do not account for such differences and may be considered unsuitable for men and boys (Darcy & Hsioa-Jung Lin, 2012; Nagata et al., 2020b; Spillane et al., 2004; Stanford & Lemberg, 2012).
Furthermore, these definitions and criteria for eating disorders largely ignore the growing recognition the presentations more common among men such as the drive for muscularity, a construct to represent the desire to achieve the Western ideal male physique, as a parallel to the established drive for thinness (McCreary & Sasse, 2000). It has been long established that men are less likely to engage in compensatory behaviors such as vomiting, and instead are more likely to use over-exercising as a form of compensatory behavior (Anderson & Bulik, 2004; Bunnell, 2010; Abebe et al., 2011; Striegel et al., 2012; Nagata et al., 2020a), however much of the research and policy on eating disorders remain focused on the thin ideal and have been female-centric (Murray et al., 2017). This is of relevance when considering the increases observed in male hospital admissions for eating disorders in the UK, with the prevalence of eating disorders in young men in hospital having increased by 98% between 2010 and 2018 (NHS Digital, 2019). This evidence in unity reinforces the growing social impact of eating and body dysmorphic disorders and the exponentially increasing health consequences for men. Despite this growth, men remain underserved and marginalized in both research and clinical practice (Murray et al., 2017; Nagata et al., 2020a). The National Institute for health and Care Excellence (NICE, 2017) eating disorder recognition and treatment guidelines, for example, remain female-centric with most referral criteria and descriptors relating to thinness concerns (e.g., criterion 2: rapid weight loss). Men and women often report distinct idealized appearances, namely men reporting a drive for muscularity compared to the thin body ideal often pursued by women, thus has the potential to cause distinct disordered eating behaviors (Cunningham et al., 2021). Instead, it is likely that men’s disordered eating will become characterized within obsessive-compulsive categories of diagnosis such as muscle dysmorphia or exercise addiction (Murray & Rodgers, 2022). As a result, there remains a underestimation of the prevalence of disordered eating in men due to nosological gender bias (Anderson & Bulik, 2004).
In light of such issues the need for creating services that have a “male-friendly environment” to reduce these barriers and encourage men to engage with services have been noted (Dearden & Mulgrew, 2013, p.850). While there has been a recognition of the need for such options within treatments, there remains no consensus or guidelines about the best means to provide such an environment (Kinnaird et al., 2018). The need to explore service providers’ views regarding this area will not only inform insights into how we could create such environments but may also highlight the preconceptions and knowledge surrounding the needs of men and boys using services. Research has highlighted that staff apathy, misunderstanding and preconceptions directly impact on men’s experiences of services (Thapliyal et al., 2018; Corral-Liria et al., 2022).
One key barrier to providing an appropriate environment for men with eating disorders is that few healthcare professionals have experience of recognizing or treating these illnesses in men or women. In a range of studies results have shown that up to 30% of service providers, including practice nurses and general practitioners, have never screened for an eating disorder or had experience working with patients with an eating disorder diagnosis (Bursten et al., 1996; Dichter et al., 2002; Boulé & McSherry, 2002; Doherty & McNamee, 2015). Healthcare providers have identified that they do feel nervous assessing and treating such illnesses (Clarke & Polimeni-Walker, 2004; Hay et al., 2007). Across all genders, health professionals report feeling less confident in managing eating disorders in practice citing a lack of eating disorder experience and knowledge/understanding, as well as inadequate training and skills (Johns et al., 2019).
Exploring the experiences and perspectives of service providers on male eating disorders has scope to inform some of their challenges and needs in the provision of specialist treatments for men who experience eating disorders. This, in turn, may address some of the barriers faced by men in seeking and engaging in ED treatments and lead to improved outcomes for this patient population.
Research Aim
The aims of this paper are to explore health professionals’: (1) Experiences, understandings, and knowledge of male eating disorders, including in the identification of obstacles faced by service providers in their assessment and treatment of male EDs; and (2) Perceptions of some of the barriers encountered by men who experience EDs that impact on their help-seeking and treatment engagement.
Findings seek to offer further understanding into key issues facing service providers in delivering eating disorder interventions in men.
Method
The findings reported within this paper are part of a larger UK-based study which explored the variables and barriers impacting on the onset and maintenance of eating disorders, which has been published elsewhere (Foye et al., 2019). The study used a sequential, mixed methods design made up of two phases. During the qualitative phase of this wider study, eating disorders in men were discussed by a number of participants as an area of concern. To further understand this area, we conducted a secondary analysis on the qualitative data.
Design
The study used a qualitative design, using an underpinning critical realist ontological perspective. While there are objective and measurable understandings to human behavior, the design of this study acknowledged that there must be an incorporate of the subjective interpretations of how individual meaning is shaped by independent experience and subjective perception (Snape & Spencer, 2003). As a result, a qualitative design as used to give the study a real worldview that explored the experiential knowledge and learning shared by participants in the sample.
Participants
This study recruited professionals and service providers working in the healthcare, community or education sectors and are thus involved directly with eating disorders intervention and/or treatment. Participant groups were selected to give a breadth of experiences and perspectives to explore the current obstacles that may prevent professionals with lesser training in providing pastoral care services for individuals with eating disorders. In addition, these groups were also able to share their insights into the barriers experienced by men who are service users across a range of service interfaces. The groups included healthcare staff recruited from NHS eating disorder services providing therapeutic services. Community services included third sector and charitable organizations involved in providing support and advocacy for eating disorders. Participants from the education sector included staff working in pastoral care roles within a range of secondary or high school level education, recruited from a forum of teachers and pastoral staff working to develop eating disorder training and policies in local schools.
A total of twenty-one (n = 21) participants were recruited to take part in the study from a range of professional backgrounds, including Specialist Eating Disorder Therapists (n = 5), staff working within eating disorder charities (n = 3), counsellors working within the community (n = 6) and education staff working within pastoral care for secondary education (n = 7). All 21 participants had at least 1 year of direct experience working with eating disorders either as part of treatment or within prevention and early intervention strategies across the UK. Only three of the participants were men (n = 1 counsellor, n = 2 education staff). All participants worked in Northern Ireland, therefore worked in adherence to national UK eating disorder guidelines and mental health regulations.
Procedure
Institutional ethical approval was granted prior to the study commencing. Participants were provided with the context and wider study aims were explained in a Participant Information Sheet prior to data collection to invite participants to take part in the study. This included an overview of the study and information regarding the research team to allow them to ask any questions or seek further information. Interview guides were developed for the wider study, using a semi-structured approach with open-ended questions regarding a range of topics related to onset and maintenance factors of eating disorders generally, alongside exploration of the barriers and facilitators for help-seeking.
Participants were invited to take part in a semi-structured interview at a time and date that was convenient to them. Due to time constraints and participant requests two focus groups were carried out with the Eating Disorders Specialist Therapists and education staff. Interviews and focus groups were scheduled to take 1 hour with an additional 15 minutes allocated before and after the data collection to gather consent and allow participants to ask questions regarding the study and how the data would be used by the research team. All interviews and focus groups were audio-recorded and transcribed for analysis. Participation was voluntary and participants were free to withdraw at any time during or after the data collection. One researcher conducted all of the interviews and focus groups to ensure consistency across data collection.
Data Analysis
Thematic analysis was used to interpret the qualitative data collected following the thematic analysis phases outlined by Braun and Clarke (2019). Initially, we familiarized ourselves with the data. Guided by the overarching study aim to explore the experiences of staff in providing physical health care for people with mental health problems, a member of the team read over the transcripts and then re-read them, noting aspects of interest. Following this, a list of codes was generated. Codes were defined as a single idea associated with a segment of data, identifying what is of interest in the data (Braun & Clarke, 2019). We used N-Vivo12 to record the extracted chunks of data and associated codes. Following initial coding, related codes were sorted, grouped and labelled as preliminary themes, defined as the central concepts that capture and summarize the core point of a coherent and meaningful pattern in the data. Themes were checked and discussed with other members of the team to ensure they were capturing something significant or noteworthy in the data related to professionals experiences, determined by prevalence in the data or whether it captured an important aspect relative to the research goal. To check for quality, the themes were re-reviewed as a group in relation to the coded data and to discuss the entire data set. To ensure the analysis was robust and credible, we used independent analysis by more than one researcher, and verbatim quotations. In the analysis presented within this paper, we will use general descriptors of frequency around a theme or meaning. Extracts of data illustrate each of them and key analytic points.
Findings
Four themes were developed to encompass the invisibility that eating disorders in men have among professions and in wider society, the barrier that masculinity creates for men seeking help, the gender bias that exists in services, and the lack of capacity and competency among providers to provide treatment or support to men with eating disorders. These themes overlap into two categories outlined in Figure 1. Categorization of themes.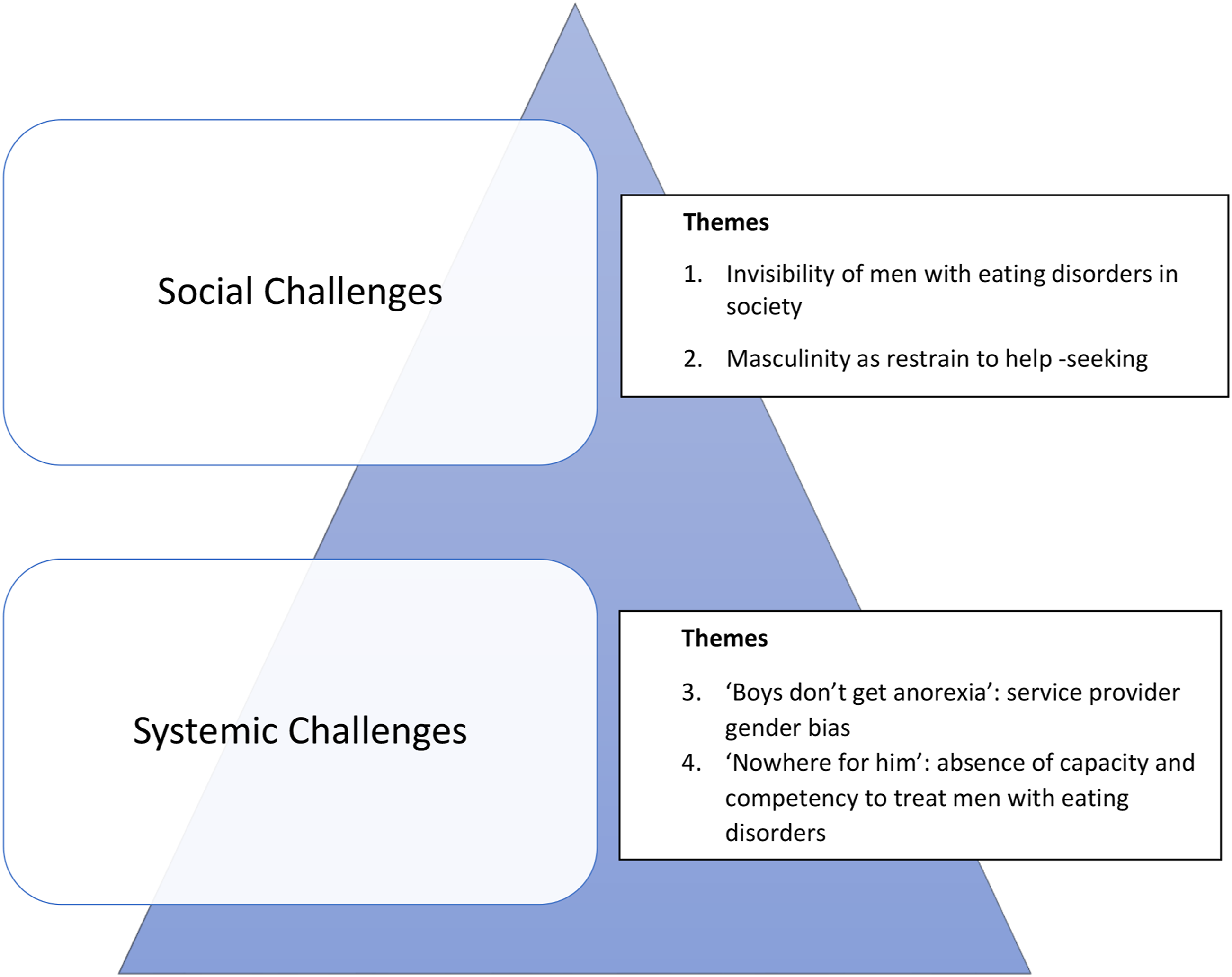
Invisibility of Men With Eating Disorders in Society
Participants raised concerns about a lack of awareness and subsequent low referral rate to specialist services amongst the wider healthcare sector for the constantly growing health problem of eating disorders in general and eating disorders in men in particular. All participants saw a rising prevalence of men and boys with eating disorders in society. This was an unquestioned statement among many of the service providers and professionals: “Certainly men are suffering from eating disorders” (ID3/f; ED Charity Staff).
This belief that the prevalence of men with eating disorders was higher than official statistics suggested was consistent across participating service providers. A number of service providers questioned the low official prevalence figures of less than 10%, stating they believed the true incidence rate of men with eating disorders was likely to be significantly higher than is truly seen in services: … there is a reservoir of males suffering out there who don’t present. It’s out there, no question. (ID4/f; Counsellor)
All participant groups stated that few men, seeking support for EDs, use their services. A number of individuals labelled men and boys with eating disorders as something that was a rarity for services to see: How often do we see males who are suffering … rarely. (ID3/f; ED Charity Staff) We have very few males presenting. (ID4/f; Counsellor)
With all services reporting low service uptake by men, participants expressed a growing concern for this gender disparity. Particularly within the education sector, it was noted that despite a slowly increasing media attention and awareness around eating disorders in men the number of men using services was not seen to be increasing comparatively: “There is a lot more focus on that…. I’ve only seen a few males” (ID7/m; Counsellor).
Many made reference to their concerns that they do not see men in services and reported that they were actively working on trying to increase uptake of services by men and boys with these disorders: “We are concerned that there aren’t more (men using services). There should be more coming to the service. We are concerned the numbers aren’t high enough and I know other teams are concerned as well…. We are looking at that as a region to try and connect with that particular group. (ID21/f; ED Therapist)
A number of those participants working in specialist eating disorder services and within the community sector reported that this challenge extended to continued engagement with services reporting that “Men that do come [for treatment] don’t tend to stay” (ID24/f; Eating Disorder Therapist).
These findings indicate that eating disorders service providers have major concerns regarding the uptake of services by men. They recognize that men and boys with eating disorders face challenges and barriers to treatment engagement that affect the uptake of their services. With low uptake of services, such beliefs that there is a potential for an epidemic of eating disorders in men to appeared which was a cause anxiety in some service providers. A number of participants reported feeling unsure and wary of how services can proceed to address the needs of this patient population in light of the disparity between the real and expected levels of service use by men: “I’m not quite sure how we begin” (ID3/f; Counsellor).
Masculinity as Restraint to Help-Seeking
When exploring key reasons why men are invisible within the realm of eating disorders, as well as the key barriers stopping men from seeking help for their eating disorder, a key theme that was explored was the concept of masculinity. Currently, the prevailing narrative that surrounds eating disorder discourses has focused almost entirely on the female stereotype and societal perception that eating disorders are women’s illnesses. These stereotypical beliefs were recognized by service providers who discussed that the perception of eating disorders in society and practice remains dominated by the belief that these illnesses are a problem affecting girls and women: “The stereotypical view of eating disorders would be, and these are not my words—I would never use these—it’s a woman’s problem” (ID7/m; Counsellor).
The perception that an eating disorder is a woman’s illness was believed to create barriers in recognition, and discussion by participants moved towards relating this perception to help-seeking. Those working as therapists had observed that when men recognized they had an issue with their eating they faced the dilemma of asking for help as this was perceived as creating a threat to their masculine identity. Defined by the characteristics, behaviors, and roles attributed to boys and men, shaped by biological, sociological and cultural factors, there is a societal pressure that men must adhere to these traditional expectations and behave accordingly to be seen as a ‘real man’ (ID7/m; Counsellor). Having an eating disorder, an illness widely associated with women, is not congruent with this traditional masculine identity: There is the belief that men should be stronger than this and should be able to deal with it—One mother has said to me “this is a women’s illness, my son won’t come forward for support” … the label eating disorder literally stopped him getting help. (ID7/m; Counsellor)
Service providers had been told by service users that admitting to being a man with an eating disorder felt like admitting to “being half a man” (ID3/f; Counsellor). This experience of shame of being a man with a woman’s illness, and the resulting perceived threat of emasculation, was considered highly salient because “it’s a man’s world” (ID3/f; Counsellor). With this threat looming over men wanting to seek help for their eating disorder it was considered as no surprise that men were reluctant to attend their services: “…men and sensitivity don’t go together, for women it’s a good characteristic, but for men it’s difficult and it’s a man’s world out there” (ID6/f; Counsellor).
Almost all of the professionals acknowledged that women seeking treatment for their eating disorder face stigma, the related that this stigma was intensified for men: “Women are facing stigma (about their eating disorder) … but there is an even bigger stigma for male clients than female clients” (ID6/f; Counsellor).
Participants drew the conclusion that they saw it as easier for patients to admit that they were suffering from other mental health illnesses such as depression or schizophrenia than to admit to having an eating disorder. These other illnesses did not come with feminine labels and did not make them feel “less of a man” (ID7/m; Counsellor), exemplifying the direct impact that the gender bias related to eating disorders has on men’s help-seeking behaviors.
Service providers further discussed that a fixed perception of masculinity was the key barrier to men engaging with services in regard to the action of asking for help as being perceived as a feminine trait. A number of participants held beliefs that regardless of the availability of appropriate eating disorders services men would still not come forward for help because asking for help is not something men do: ...because of that macho thing, boys are afraid to look like they have a weakness. They don't want to look like they have weakness and go and seek help... There is also the belief that men should be stronger than this and should be able to deal with it—to man up. (ID8/m; Teacher)
Men with eating disorders were also reported to have difficulties with aspects of talking therapies to address their illness. This was seen as an issue that needed to be considered when creating and delivering treatment for men to ensure that men could engage with services: Men generally are more guarded in what they say, even in society with emotions. And we see that in the therapeutic relationship, they struggle with the whole emotional thing…. Men that do come don’t tend to stay. (ID24/f; Eating Disorder Therapist)
By emphasizing what can be regarded a ‘double threat’ to masculinity, through being a man with a ‘woman’s illness’ and having to seek help which is considered feminine and emasculating behavior, most participants related that getting men into services, support groups or prevention programs was extremely difficult. Many participants considered the threat to masculinity to be the most difficult barrier for men with eating disorders to overcome and admitted that this was a wider societal issue that makes approaching it “very difficult” (ID3/f; ED Charity Staff).
Boys Don’t Get Anorexia’: Service Provider Gender Bias
Participants expressed concerns that men were excluded and widely discounted because of a lack of awareness and knowledge amongst general healthcare providers that men get eating disorders too: Thinking about a male sufferer who went into his GP, he went to this GP, the GP launched into “you are looking so well, you’re fit and this and that”, and he stopped him and just said "I'll not beat about the bush, doctor I'm here because I have anorexia". And the GP grabbed him by the arm and said: "Son you don't need to worry about that because boys don't get anorexia". What do you do with a GP that does that? Here he is telling the doctor he has an eating disorder and for the doctor to have it in his head that boys don't get eating disorders. This isn’t 20 years ago, this was last year! (ID1/f; ED Charity Staff)
Many participants admitted that before working in the field of eating disorders, or having contact working with a man with an eating disorder, their awareness and knowledge of the issue and specific needs for this population was limited. One participant admitted that they would not have considered men with eating disorders before having direct experience of the issue: “I realize now with all that we now know [about eating disorders in men] I realize how little we knew back then. We knew nothing!” (ID27/f; Community Worker).
A number of participants believed that there is a considerable lack of resources and information specialized for men: The information is very confusing I think, particularly for men. It is not targeted. It's a different kind of thing. For women, there is a clearer picture of what is an eating disorder … but for men it's bombarded by confusing information. (ID21/f; ED Therapist)
Information resources and awareness raising material, including prevention workshops and media reporting, were believed to contribute to this lack of awareness for eating disorders in men by health practitioners, the wider community and by men and boys themselves. These sources were perceived to perpetuate and reinforce the gendered focus of eating disorders being female bound illnesses that men “couldn’t possibly have” (ID27/f; Community Worker). As one participant reflected from their experience, men may consider weight loss and other symptomology as related to diabetes or physical causes such as cancer before even considering an eating disorder, because the information does not fit when it is “all about girls” (ID1/f; ED Charity Staff).
It was perceived by many participants that men’s perspectives, needs, and experiences remain missing from the narrative surrounding eating disorders, and therefore men and boys with eating disorders remain invisible. Without resources and information to combat this gender bias it was conveyed that men would continue to feel like they are “very much on [their] own with this” (ID3/f; ED Charity Staff).
These findings provide insight into the continued invisibility that men and boys with eating disorders face within society and practice, resulting in low awareness and a lack of visibility to service providers, which was seen as likely to lead to “…men slipping through the net”(ID19/f; Community Worker).
“Nowhere For Him”: Absence of Capacity and Competency to Treat Eating Disorders in Men
A number of participants disclosed that they did not feel comfortable in dealing with eating disorders in men due to several factors that included lack of information and knowledge but also lack of preparedness by themselves and others (e.g., colleagues or general public) to engage with it. One participant pinpointed that the issue of eating disorders in men as “so hush hush” even among those working in the field (ID3/f; ED Charity Staff): “Male eating disorders … it’s a touchy subject” (ID7/m; counsellor).
While the conversation around girls and women and eating disorders in non-eating disorder settings, such as education, general mental health, and youth work, was seen to be opening up, the issue for men was still seen as a “no go area” (ID7/m; counsellor). Community workers and staff involved in raising awareness in schools reported that they had little experience in delivering prevention and awareness workshops or direct support to young men within education and youth settings. Such work often only targeted young women. One community group reported that this was not from a “lack of trying” (ID3/f; ED Charity Staff) but as a result of difficulty creating appropriate resources and challenges in gaining access to this population.
On exploring the uneasiness with the topic even by professionals, it emerged that those working on the frontline with eating disorders, particularly within education and community settings, identified the following issues: while they are aware that eating disorder in men was a growing problem across schools and the youth sector, there is the lack of clarity, training and support with regards to how to best engage with boys and young men on this issue. Participating professionals identified particular difficulties with regards to services and even basic information available to men: No, I don’t feel confident with it! How do we deal with it? I think people are uncomfortable with it as an issue. It’s still very taboo. They think oh goodness … it’s scary to talk about so people shy away from it. This is an issue for our personal tutors - they are not equipped [for disclosures], they don’t get the information, it’s very difficult to train them and give that information if there’s nothing. There is a massive, massive gap for eating disorders, and that concerns me…. Consider a young man in Northern Ireland coming to you, where do you send them apart from back to their GP? There is nowhere for him really.” (ID18/f; Pastoral Care Worker)
This was highlighted by a number of service providers who felt there was a lack of resources and targeted information about this topic. A number of participants noted the lack of support to help them, as professionals, to understand this issue. They also raised concerns that it would be even more difficult to identify information and help for those men and boys looking for it.
Many participants acknowledged the deeply ingrained perception of eating disorders as a women’s illness and felt uncertain how to break down this barrier toward getting men involved in discussing eating disorders. Education staff, in particular, felt this issue was the most difficult to discuss; while they felt young men were open to conversations about mental health, suicide and sexual health. However eating disorders still proved to be a stigmatized and uncomfortable topic because of the negative, gendered stereotypes. Awareness and acceptance of eating disorders in men was seen as just too challenging as it made people “address their gender stereotypes” (ID21/f; ED Therapist) and rethink eating disorders within the context of gender as a concept, something that people “just aren’t ready to do … the conversations are not open to do that” (ID18/f; Pastoral Care Worker).
Discussion
The aim of this paper was to understand the experiences and perceptions of professionals providing care and support to men who are living with an eating disorder to help identify the gaps and challenges to help identify gaps and challenges in the provision of support and treatments. A key theme for service providers was highlighted as the lack of visibility that men with eating disorders had within the field and within services. With media reports and growing research suggesting an increased prevalence in men with eating disorders, there was a growing concern that at the coalface professionals were not seeing similar trends. Three key areas were identified as potentially having a considerable impact on this visibility.
First, at the individual level, it was identified that there was a considerable impact of masculinity on men’s personal help-seeking behaviors, which was felt to have a role in the low levels of men seeking help from the range of services available. This aligns with the wider mental health literature regarding men’s help-seeking behaviors in which men who align closely to these hegemonic gender roles are found to view help-seeking negatively (Mendoza & Cummings, 2001), resulting in a decreased likelihood of seeking the necessary support (Good et al., 1989). A growing number of contributions in eating disorder literature reflect upon such stereotypes. They highlight the highly questionable status of anorexia in particular as “classically […] viewed as occurring primarily in young Caucasian women, perhaps particularly in those of high socioeconomic status” (Crow, 2010, 397), warning that such stereotypical understanding of eating disorders as a woman’s illness can lead to the preconception that men do not get eating disorders (Räisänen & Hunt, 2014; Robinson et al., 2012). Consequences of this may be threefold: the development of the fear of not being a “real man” because of the illness thus presenting a considerable barrier for engaging in help-seeking (Drummond, 2002; Griffiths et al., 2015); an attempt to endure negative symptoms of maladaptive behaviors to gain masculine capital (Cranswick et al., 2020; Edwards et al., 2017); and difficulties in discussing eating disorder experiences post-recovery as a result of feeling intense shame (Björk et al., 2012). The accumulation of the gendered bias towards eating disorders has created a prevailing narrative of eating disorders that has led society as a whole to associate the illness with women only and assume a certain masculine stereotype. Findings from this study show that these gender roles remain engrained within the field and continue to have an impact on men seeking help and may provide insight into the difficulties that services have in being able to attract men to use such support.
These assumptions are also reflected at practice level with service providers and health professionals being part of public life and its socio-cultural influences and conscious and unconscious biases, just like the rest of the population. The realm of medicine and healthcare is not isolated from the socio-cultural realm and its prevailing assumptions and stereotypes and professionals need to constantly reflect upon their practices and approaches to provide unbiased and open support and not confirm tight gender roles for men to adhere to (Harland, 2008). This practice level can be reflected in the themes associated with professional awareness and understanding of men’s experiences of eating disorders. The findings in this study reflect a notion of uneasiness and uncertainty around the topic due to both personal reflections as well as the lack of training and information accessible to them on the topic. This again points to the influence of the prevailing narrative of eating disorders remaining focused on women’s experience with most research and literature reflecting this gendered understanding of what it is to experience and to support or provide treatment for an individual with an eating disorder. As a result, there is an increasing acknowledgement for the need to address diversity within eating disorder research (Halbeisen et al., 2022b). Recent investigations into men’s experiences link disordered eating to muscularity-oriented issues and muscle dysmorphia, which are identified as male-specific and associated with perceived masculine discrepancies (Cunningham et al., 2020). The lacking awareness surrounding these subjects has led to difficulties in the identification of symptomology, co-morbidities and eating disorder diagnosis, as shown in Murray et al.’s case study (Murray et al., 2018). Within this literature we see that excessive drive for muscularity has resulted in reports of uncontrollable muscle-building exercising, eating behavior and related use of steroids (Nagata et al., 2020a). The perceived lack of awareness within this study signifies a significant issue facing men, as despite the evidence regarding increased prevalence of men experiencing eating disorders, professionals continue to lack awareness and knowledge of eating disorders in men and boys. The problem identified by participants, that eating disorders in men are invisible to most health care professionals, has not only had an effect on early recognition by men themselves but also with regards to recognition within the practice by professionals in the field. This invisibility of eating disorder in men does not mean that they do not suffer from eating disorders, but instead emphasizes the invisibility of the illness to professionals and individuals who “have to first think of it as a possibility” (Andersen, 1990, p. 133). Poor awareness of men’s experience has led to a complete dissociation of men from the field of eating disorders (Dalgliesh & Nutt, 2013). The results of this study further emphasize that there seems to be a parallel process of invisibility not only to the health professional who treats him, but also to the man himself, thus highlighting the need for resources and awareness materials to continue to target men themselves (Richardson & Paslakis, 2021).
The third key area identified within this paper places a focus on the institutional level, highlighting the poorer levels of capacity and competency in managing the care and support of men presenting to services with eating disorders. This theme moves beyond a level of understanding or awareness that men can get eating disorders at a practice level toward identifying that service providers, caregivers and professionals at the coalface of eating disorder services feel that they are inadequately supported to have the capacity and competency to provide the best for men and boys with eating disorders. It is evidenced that men’s experiences remain “overlooked, understudied and underreported” (Greenberg & Schoen, 2008, p.464), and professionals across sectors admit it is still a struggle. Further training and awareness work within professional spheres are clearly necessary to help reduce the stigma of this touchy subject, as a step towards reducing the internal stigmatization and shame felt by men with these illnesses (Griffiths et al., 2015).
It is clear that there are significant challenges for men when seeking help or treatment for their eating disorder but also for health practitioners in their approaches to diagnosis and treatment. In combination, these two factors need to be considered as reasons contributing to the low incidence figures for men in services. Lack of awareness that men do get eating disorders, as well as detailed knowledge of their needs—be they similar to or different from their female counterparts—is likely to have a direct impact on the recognition and diagnosis of men with eating disorders. If men are invisible to frontline healthcare staff, service providers and professionals, they remain invisible as a patient population. Sweeting et al. outline the vicious circle caused by this underestimation of the problem that leads to vanishingly low figures of eating disorders in men to be circulated in the media which, in turn, may “affect evaluations of [men’s] personal susceptibility and hence help-seeking behaviour” (Sweeting et al., 2015, p.1). This invisibility of men as a patient population also means that health care workforce is inexperienced, and thus underprepared and undertrained in developing interventions that are tailored to their unique needs and preferences (Sangha et al., 2019).
Strengths and Limitations of the Study
While the study provides insights into experiences and views of service providers in regard to men with eating disorders, there are limitations to generalizing these results widely due to the small sample size and the specific nature of the sample included in the study. While the sample size is considered appropriate for the qualitative design of the study, it provides only initial steps towards understanding the needs and barriers of men with eating disorders as part of a generalizable framework. Furthermore, this sample consisted of professionals working with eating disorders rather than men with personal experience themselves. While this sample has provided a unique perspective by exposing the weaknesses related to working with men in practice limitations must acknowledge that this sample does not allow for the experiential learning needed within the field.
While the study has limitation in regards to rigor compared to other methodological approaches, for instance a national cross-sectorial survey of service providers, the scope of this study was to explore the experiences of this group of healthcare professionals to highlight the challenges faced and the needs of this group. A strength of this study is the honesty and vulnerability of participants to acknowledge their own inexperience and the challenges they face to help understand the gaps that exist. Such data can be triangulated alongside the experiences of men with eating disorders who have experienced such service provision to help direct how “male-friendly” eating disorder spaces and resources can be developed and implemented effectively.
Study Implications
By identifying the challenges that face men with eating disorders it is possible that more targeted programs can be developed and applied at primary, secondary and tertiary levels of intervention to address the key areas that create difficulties for men with eating disorders. Based on the findings of this study there is considerable work to be carried out in relation to both societal and professional understanding of eating disorders and the knowledge that surrounds such illnesses, as it is evident that there are gendered beliefs surrounding eating disorders that influence practitioners. The presence of such stereotypes and misinformed views regarding eating disorders and help-seeking strategies as “women-only” can be seen to have a significant impact on individuals living with such disorders through preventing or delaying recognition and help-seeking. A vital step in improving outcomes for men with eating disorders is to address gendered biases within the profession. An unbiased and self-reflective healthcare environment where this “touchy” subject is approached openly can also help to remove the stigma, shame, and secrecy that remains problematic for these men.
To strive towards clearer visibility of men within the field of eating disorders it is vital that work focuses on addressing specialist medical and public knowledge of these disorders. A rising number of published narratives by men about their lived experience with eating disorders have emerged in recent years as one unexpected way to give this population greater visibility increase knowledge in both public and medical practitioners. These narratives reveal the patient’s perspective of living with an eating and deliver personal insights into gendered perceptions of the illness. Such autobiographical writings are being read, with growing interest, by the public but also for research in the fields of eating disorders and medical humanities (Thapliyal et al., 2018; Bartel, 2019). These texts, and the resulting increased visibility, should be utilized and transferred into available resources for training professionals and researchers. Such tools will assist in reducing stigmas and improving help available to boys and men experiencing eating disorders.
Concluding Remarks
This study provides insight into eating disorder service providers needs regarding their understanding and knowledge of eating disorders in men. While research into the field of eating disorders in men has increased over the past decade, there remains a lack of understanding in relation to how services can be improved to meet this populations needs. This study highlights the lack of visibility that men continue to experience in this area of healthcare, with insights from these results noting the gender bias that remains among professionals, and lack of expertise that service providers have in this area. By exploring service providers concerns and inexperience in meeting the needs of men, it is possible to begin to shape learning to address the gaps in knowledge that exist.
Footnotes
Author Contributions
All authors have read and approved the manuscript. Author UF created the protocol for the study, conducted the recruitment for the study, conducted the interviews and focus groups, and coded data. UF, GM and HB contributed to the thematic analysis. All authors supported drafting and development of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All methods were carried out in accordance with Declaration of Helsinki and GDPR guidelines. The protocol was approved by University of Ulster Research Ethics committee (REC/12/0303) and the NHS/HSC Research Governance Ethics Committee (Ref: ST1314/01) in accordance with the Declaration of Helsinki prior to data collection with a later amendment to move data collection online in response to COVID-19 restrictions and guidance.
Informed Consent
All participants provided informed consent prior to enrolment in the study, including consent for publication of anonymised quotes.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author Biographies
![]()