
Abstract
Youth between ages 13 and 25 who experience homelessness face numerous barriers to excellent health, including social stigma and discrimination. Applying socio-ecological model and intersectionality theory, an integrative literature review was conducted. Peer-reviewed studies (N = 29) representing 808,296 participants extracted from four databases (CINAHL, MEDLINE, PsychINFO, SocINDEX) were analyzed. The studies included sources of discrimination and stigma from interpersonal interactions with support services staff upwards to policy and systemic levels with housing and justice systems. Health outcomes include poorer physical and behavioral health status from increased likeliness of denied access to support services, prolonged time spent being homeless, and higher incidences of experiencing violence. School nursing has power to push for recommended changes and support unhoused youth towards excellent health. Proposed changes include adapting Housing First framework, engaging with unhoused youth in program planning, policy writing, and public education that address the causes of poverty.
Keywords
Youth progress through transformative experiences during the period of 13–25 years of age. In a span of 12 years, youth can have life-lasting positive health outcomes if their needs are adequately met; however, youth who experience homelessness (YEH) do not have similar opportunities to fulfill basic needs. Federal definitions of YEH vary by programs. McKinney-Vento Homeless Assistance Act defines YEH as people who “lack fixed, regular, and adequate nighttime residence,” meaning loss of housing, living in temporary residences, public spaces, transportation, suboptimal housing, and migrant children (The McKinney-Vento Homeless Assistance Act, 2009, pg. 1). YEH also include street youth, runaway youth, throwaway youth, and systems-involved youth (Hammer et al., 2002; youth.gov, n.d.). Systems-involved youth are youth who have been part of the juvenile justice system, child welfare system, or both (also known as crossover youth).
Nearly 4.5 million youth experience homelessness each year, more than the population of the city of Los Angeles (Morton et al., 2017). Roughly 50% of YEH reported that it was their first time being unhoused (Morton et al., 2017). There are several known precipitating factors of youth homelessness. Domestic violence, interpersonal conflicts, lack of affordable housing and household financial insecurity, ageing out of the foster care system, history of incarceration, untreated mental health conditions, and inadequate social network support or rejection are major causes of homelessness (Aratani, 2009; Kelly, 2020). Youth may have additional social vulnerabilities to homelessness through oppression based on race, ethnicity, sex, gender, ability, and age. Youth who are Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ+), females, Black, non-White Hispanic, 18–25 years old, and/or have disabilities experience disproportionate rates of homelessness (Morton et al., 2018). Therefore, solutions to address youth homelessness call for a socially committed, interdisciplinary, and equitable approach.
Nursing and Homelessness
YEH encounter various negative social determinants of health (SDOH), such as food insecurity, lack of safe shelter and hygiene facilities, unstable access to electricity and internet, disconnection from supportive social networks, changing education and lack thereof, limited employment opportunities, and insufficient healthcare access (Substance Abuse and Mental Health Services Administration [SAMHSA], 2019). YEH have a higher risk of exposure to adverse childhood experiences (ACEs) than housed youth (Barnes et al., 2021). ACEs can lead to more vulnerability to chronic diseases, worse mental health outcomes (Gewirtz O’Brien et al., 2020), being victims of interpersonal violence (Tyler & Schmitz, 2018), and increased risk of contracting communicable diseases (Strashun et al., 2020). Caring for youth experiencing homelessness calls for the combined disciplines of public health and nursing. The Public Health Nursing model emphasizes relationship-building, population-based, holistic, health-promoting factors, systems-based interventions, and commitment to social justice (Keller et al., 2011). Nurses act as mediators to improve health and advocate for YEH. Nurses provide essential healthcare to unhoused youth in school settings, hospitals, community clinics, and outreach services (Weber 2019). Nurses also have the capacity to advocate for primary prevention of homelessness, such as identifying causes of poor health outcomes, building community, collecting epidemiological data, and writing policies through community-based partnerships (Weber 2019). Therefore, the nursing profession is called to identify how youth homelessness is perpetuated within society, participate in drafting goals for lasting positive health outcomes, and advocate for social interventions that place health promotion at the center.
Intersectionality in Stigma and Discrimination
Social stigma and discrimination contribute to the perpetuation of youth homelessness. Social stigma represents the gap between sets of expectations socially assigned to groups of individuals to categorize people for effective interaction and the complete representation of each person who may share backgrounds (Goffman, 1986). Unhoused youth experience frequent social stigma, preventing them from accessing support services due to an unwelcoming environment. Through society-driven stereotypes and judgment, unhoused youth are assigned labels and viewed as outcasts. Discrimination manifests as actions derived from stigma that intentionally limits and disadvantages certain groups of people, rooted in differences in power and access to resources (Kohler-Hausmann, 2011). Discrimination against YEH denies access to appropriate shelters and high-quality healthcare, criminalizes disproportionately, and prevents youth from exiting homelessness. Based on the frequency and pervasive nature of social stigma and discrimination against YEH, it is imperative to map how, where, and who drives these consequential inequities.
Unhoused youth also experience other forms of identity-based mistreatments. Intersectionality theory allows a fuller examination of how stigma and discrimination interact across identities. In 1989, Dr. Kimberlé Crenshaw wrote a paper originating the term “intersectionality.” Crenshaw argued that discrimination against Black women has to consider structures against both being Black and being a woman (1989). By acknowledging the dynamics of both racism and sexism, oppression and how to address it can be seen as a more complete phenomenon. In this paper, intersectionality is used to include how racism, sexism, ableism, and other forms of structural oppression further compound challenges experienced by unhoused youth.
School Nursing
Youth between the ages of 13 and 25 years spend a great deal of time in school. School is an essential part of the socialization of all children in the United States. It is also a place where children and youth begin to experience the discrimination and stigma that accompany any attribute that makes them stand out as different from the majority. School nursing is a vital component of the Public Health discipline that is committed to promoting the health and well-being of children and youth (Kindi et al., 2021). The American Academy of Pediatrics (2016) recommends that every school has at least one registered nurse, but there is no current data available from the Department of Education to determine if this recommendation is being met (National Center for Education Statistics, 2020).
School nurses often witness how the SDOH affect the wellbeing of students, but school nurses may lack sufficient tools to support the unique needs of unhoused students and address structural causes of homelessness. SDOH are referred to as social factors, such as housing, education, environment, food, transportation, safety, social networks, etc. that can influence health outcomes. In this case, school nurses must seek additional preparation through continuing and advanced education to understand drivers of social stigma and discrimination processes. Their communication with and support of all students is an important first step in modeling acceptance of all ways of being. School nurses are well-positioned as coordinators in connecting unhoused students to essential resources by building trusting relationships and collaborating with community partners (Hindman & Mincemoyer, 2014). School nurses can develop programs that promote safe learning environments and address misinformation that drives stigma and discrimination against unhoused students. They can also work with their School Board to establish policies that encourage the acceptance of all youth despite their backgrounds. It is important to recognize that school nurses are often under-resourced within their scope of practice. School administrators need to create protected times for school nurses to learn, create, and manage initiatives supporting unhoused students.
Unhoused students may experience other identity-based stigma and discrimination, such as homophobia and transphobia. A study of health professionals, including school nurses, in New Mexico showed that they lacked preparation in providing safety and support for LGBTQ+ students (Mahdi et al., 2014). Many of the school nurses in this sample were not aware of the connection between loneliness and stress experienced by this group of students and their risk for suicide. Moreover, they felt ill-prepared to address the health disparities and health risk behaviors of these students. In another study of LGBTQ+ students and school health professionals in Massachusetts, researchers found that these students had many unmet health needs, including being harassed and experiencing sexual violence at school (Sava et al., 2021). These findings highlight the need for school nurses to be equipped with knowledge on intersectionality and structural competency to address social stigma and discrimination among unhoused students. This integrative literature review aims to raise awareness of complex social dynamics experienced by unhoused youth for school nurses so that holistic care can be achieved.
Theoretical Frameworks
We thus propose to answer the following research questions in this integrative literature review:
How do unhoused youth experience social stigma and discrimination? What are YEH health outcomes associated with social stigma and discrimination? How can healthcare and society-at-large take evidence-based suggestions to build an equitable and inclusive support system for unhoused youth?
An integrative literature review includes both quantitative and qualitative data, effectively mapping the prevalence and nature of social stigma and discrimination against YEH. A socio-ecological model was used to conceptualize how each layer of society interacts with each other in producing a negative image of unhoused youth and prevents optimal health outcomes (Kilanowski, 2017). Socio-ecologcial model is composed of internalized/individual, interpersonal, community, institutional, public policy, and society levels. Internalized/individual level is considered how one views oneself, inclusive of lived experiences. Interpersonal level depicts the quality of relationships and interactions, such as connecting with a friend. The community level can be analyzed through social public spaces, local politics, and community attitudes around geo-spatial access. Institutional-level examples are schools, hospitals, churches, employers, and service organizations. At public policy level, factors such as conditions to qualify for housing, school disciplinary policies, intensity and scope of policing, and who gets access to basic resources are studied to conceptualize how laws and ordinances shape communities, institutions, and people's behaviors. Zooming out to the society level, norms towards a certain group of people are used to maintain differential levels of power, privilege, and access, such as classism, racism, etc. Intersectionality, a critical framework showing how systems work interconnectedly to produce outcome differences, was used to understand how YEH and who manifest oppressed identities further intensifies the impact of stigma and discrimination (Crenshaw, 2019). For example, up to 30% of unhoused transgender individuals experience shelter access denial and more than 20% experience sexual assault from shelters staff or residents in comparison to cisgender unhoused individuals; transgender women are at higher percentage of shelter access denial in comparison to transgender men (34% vs. 20%) (Grant et al., 2011). Furthermore, this study further brings visibility to youth homelessness and provides actionable steps toward a future of acceptance, acknowledgement, accessibility, and availability of resources.
Methods
The primary literature review method used is an integrative literature review, following general guidelines by Fink (2020) and recommendations by Whittemore and Knafl (2005).
Eligibility Criteria
Inclusion criteria for studies included participants between the ages of 13–25 years, conducted in the United States, peer-reviewed, addressed the experience of homelessness, and discussed social stigma and/or discrimination. Through consultation with a university-affiliated librarian, other search terms related to homelessness were included: Unhoused, houseless, street living, unsheltered, unstable living. Additionally, other search terms related to stigma and discrimination were included: Exclusion, marginalization, attitudes, alienation, prejudice, welcome, and acceptance. Excluded studies included op-eds, commentaries, letters to editors, reviews, case reports, abstract only or lack thereof, and dissertations.
Search and Article Selection Process
Through the suggestion from the librarian for high-yield studies, CINAHL, MEDLINE, PsychINFO, and SocINDEX databases were searched to find studies related to YEH and social stigma and discrimination. The resulting studies were extracted from these databases in April of 2021. There is no parameter for year selected in order to be as comprehensive as possible. A sample of 279 articles from CINAHL, 140 articles from MEDLINE, 234 articles from PsychINFO, and 63 articles from SocINDEX were used for further analysis, totaling 716 articles. Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) model as guidance (Figure 1), practical screening removed 170 duplicate articles and excluded 421 articles based on applying inclusion and exclusion criteria to abstracts. Full-text examination of 125 articles further reduced the final number of articles to be included in the critical appraisal for this integrative literature review. A final sample of 28 articles was selected for data extraction and critical appraisal (Table 1). The search terms and filters applied for each database are presented in Figure 2.
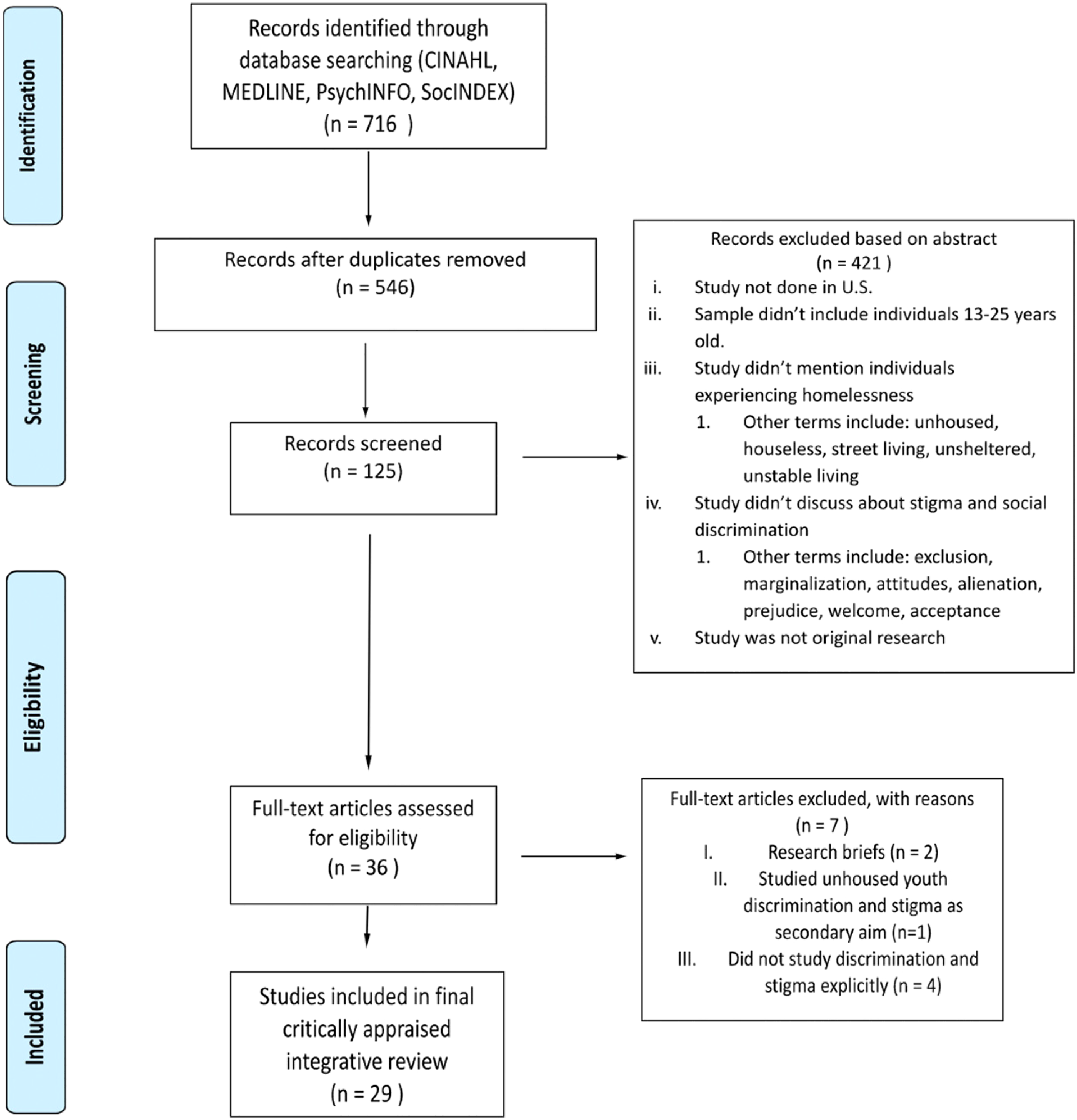
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram showing identification, screening, eligibility, and included articles.
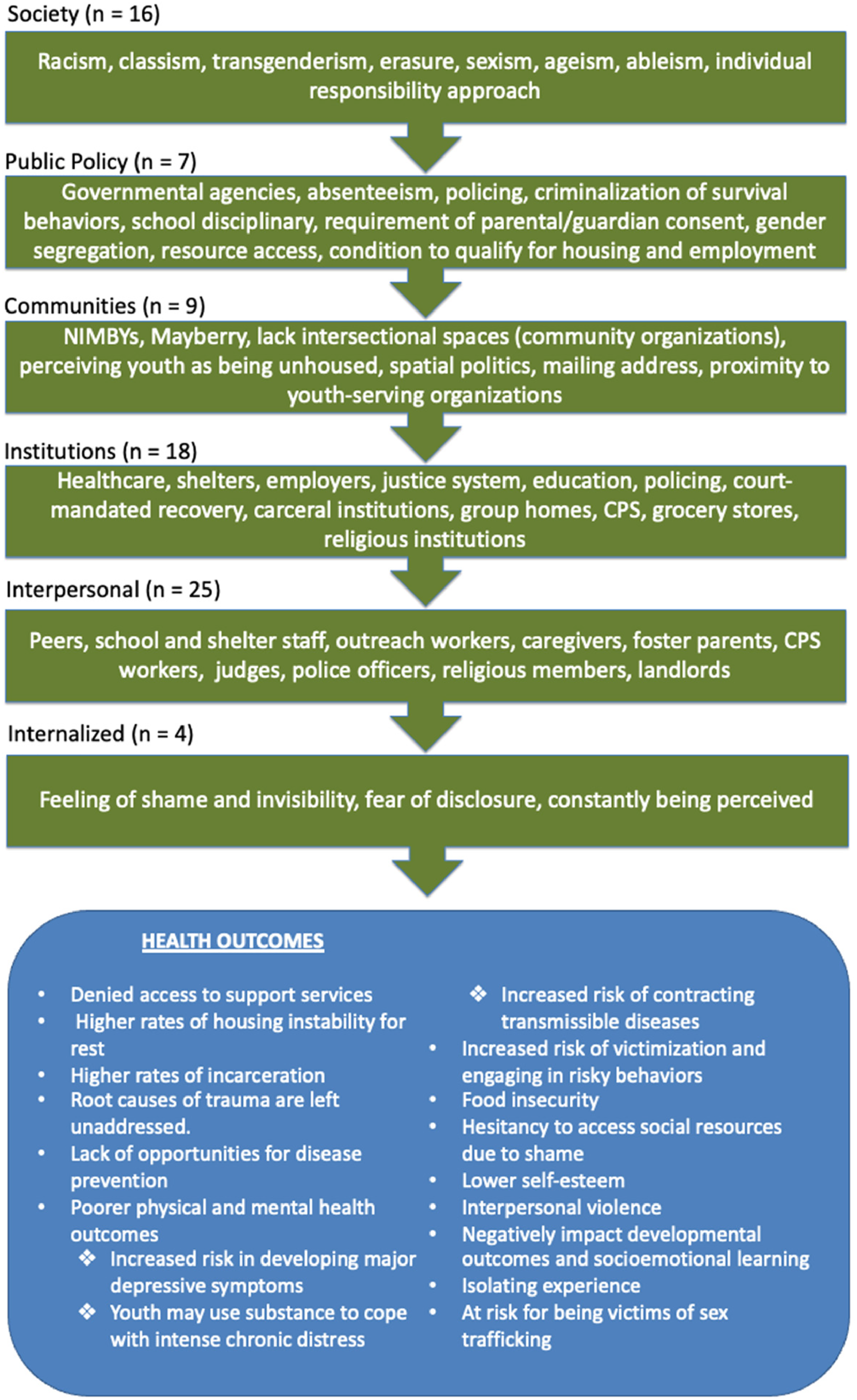
Socio-Ecological model of stigma and discrimination origins, and how they impact youth's health outcomes.
Summary of Data Extracted for Integrative Review of Literature on Stigma and Discrimination of Unhoused Youth.
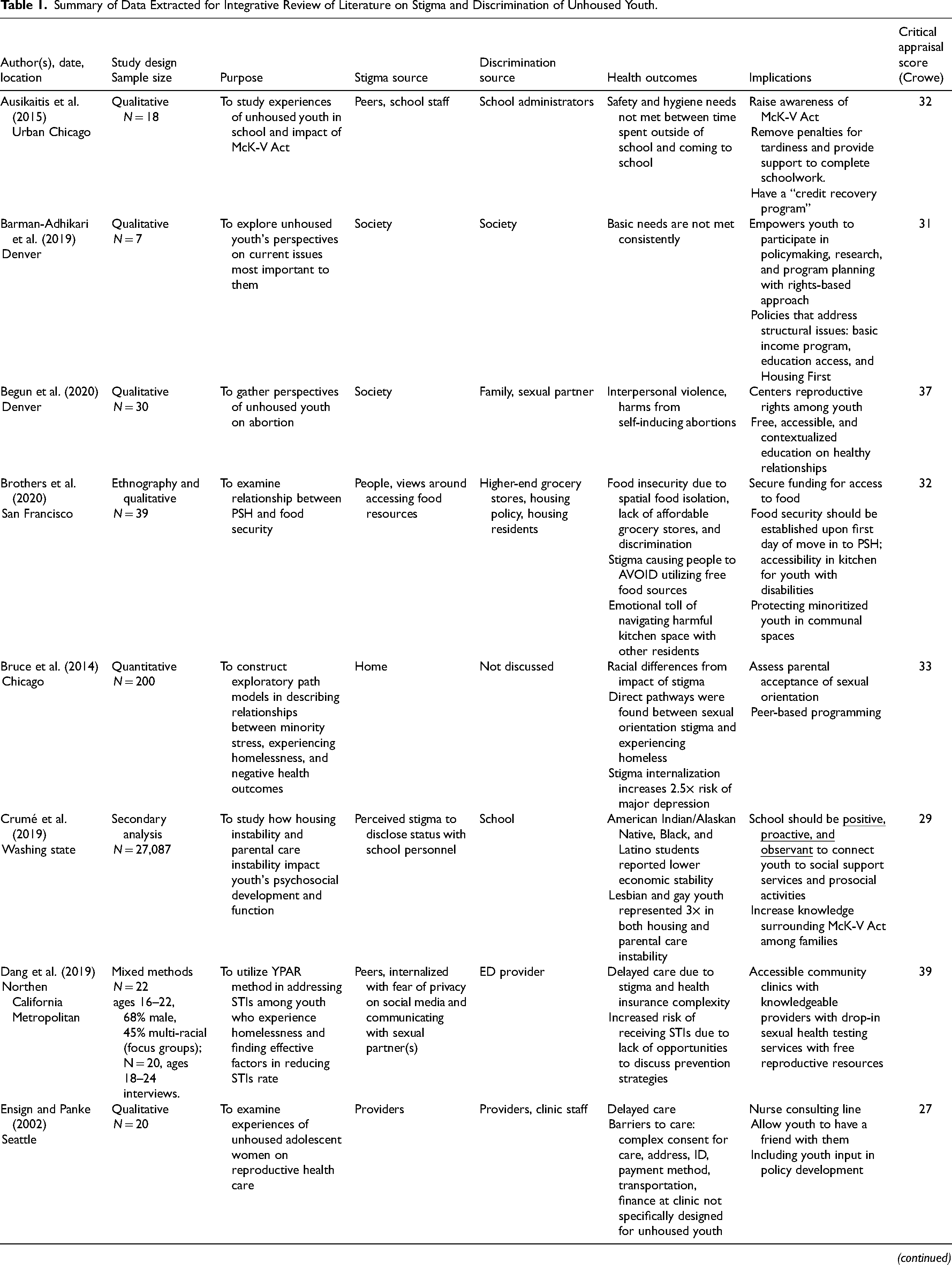
CPS = child protective services; DFPS = Department of Family and Protective Services; ED = emergency department; ESSA = Every Student Succeeds Act; LGBTQ + = Lesbian, Gay, Bisexual, Transgender, and Queer; IPV = interpersonal violence; McK-V: McKinney-Vento; NIMBY = not-in-my-backyard; PSH = permanent supportive housing; RHYA = Runaway and Homeless Youth Act; YPAR = Youth Participatory Action Research; PSH = permanent supportive housing.
Critical Appraisal
The Crowe Critical Appraisal Tool (CAT) was used to determine the quality of research studies with a potential 40-points format. The Crowe CAT asks questions about quality in eight sections: preamble, introduction, design, sampling, data collection, ethical matters, results, and discussion (Crowe et al., 2012). The preamble includes details about the title, abstract, tables, and figures. Each of the eight sections can be scored from 0 to 5 points, with the total of 40 potential points. This CAT has evidence of validity and reliability and has the versatility of being applicable to any research design, including those that are qualitative and quantitative (Crowe et al., 2012).
Data Extraction Process
The 28 peer-reviewed articles selected were analyzed by both authors to extract information on article authors, date, location, study design, sample size, purpose, sources of stigma and discrimination, health outcomes, implications, and CAT scores. Both authors met regularly to compare findings, reconcile disagreements, and reach consensus on data extracted. Data is presented in Table 1.
Results
A total of 808,296 participants were in the final sample of this review. Participants lived across the United States in 13 states: California, Colorado, Georgia, Illinois, Louisiana, Minnesota, Missouri, Nebraska, New York, Ohio, Texas, Washington, and Wisconsin. All studies included a discussion on how unhoused youth experienced social stigma and/or discrimination. Table 1 is included to show how unhoused youth experience social stigma and/or discrimination. Categorization through the application of the socio-ecological model resulted in 16 studies categorized at the societal level, seven studies at the public policy level, nine studies at the community level, 18 studies at the institutional level, 25 studies at the interpersonal level, and 4 studies at the internalized/personal level. Most of the studies were qualitative (n = 18), with almost equal numbers of studies that were quantitative (n = 6) and mixed methods (n = 5).
Researchers discussing stigma sources (n = 24) highlighted shame around accessing social services, judgments from peers and school staff, lack of intersectional spaces, looking down on survival strategies, and additional stereotypes around race, ethnicity, LGBTQ+ status, and disability. Healthcare (n = 2), school (n = 2), shelters and service-providing organizations (n = 4), policing (n = 3), and public policy (n = 1) were discussed on misconceptions around unhoused youth. Harter et al. (2005) reported how Mayberry Not-In-My-Backyard (NIMBY) public policies tended to limit youth-serving organizations from existing and categorized unhoused youth behaviors as unsafe.
Studies discussing discrimination sources (n = 26) highlighted treating unhoused youth with harsh requirements, degrading a youth's ability to care for themselves, excluding services due to criminal history background, perpetuating racism and transgenderism, and criminalizing survival behaviors. Healthcare (n = 4), school (n = 5), shelters and service-providing organizations (n = 10), policing (n = 5), and public policy (n = 1) were identified as potential sources for the constant violence against unhoused youth at services supposedly intended to help them survive, thrive, and exit homelessness.
Crowe scores of the papers in this review had a median of 32 points, mean of 31.75 points, and a range from 22 to 39 points. Both authors of this review read all papers in the final sample and discussed differences in their assessments to reach consensus on the final scores. The majority of papers in this review scored above the mean, which meant that nearly 80% (31.75/40) of the items on the Crowe CAT were answered affirmatively. For those studies that scored below the mean and toward the bottom of the range (e.g., 22/40 = 42.5%) were less trustworthy. Those studies had a higher risk of bias than those with higher scores.
Health Outcomes
Housing instability. Many studies reported increased housing instability due to stigma and discrimination (Table 1). For example, Robinson (2018) stated that gender segregation housing and denial of correct gender housing placements can lead to increased evictions and limited permanency. Within shelters, forms of violence such as harassment and victimization can be rooted in minoritized identities against unhoused youth, especially by shelter staff and other residents. Through stricter requirements and enforced by policing, YEH are under more frequent surveillance, leading to an increased risk of incarceration (Robinson, 2018).
School violence. Strong protections against unequal treatment for unhoused youth are needed to prevent trauma and marginalization. Moore et al. (2020) highlighted that stigma and discrimination within school can negatively impact socioemotional learning and appropriate developmental outcomes. With fewer opportunities to build strong social networks and receive encouragements, unhoused youth are less likely to have access to a safe space for optimal learning (Crumé et al., 2019). Unhoused youth who encounter these harmful interactions every day at school are at risk of not being able to complete their education and have a higher chance of dropping out to avoid further trauma (Ausikaitis et al., 2015). School should be conducive for learning and socialization, where youth feel comfortable and trust the institution to support them.
Denied access to care. Healthcare providers may create a hostile environment where unhoused youth do not feel welcome in receiving care, as documented in Table 1. Ensign and Panke (2002) and Dang et al. (2019) stated that judgment, lower quality of care, and providers assuming unhoused youth as being ignorant about their health have contributed to limited discussion of prevention strategies. They also found that unhoused youth of minoritized identities experience other forms of oppression from providers and clinic staff, with little regard to privacy and confidentiality, misgendering, and stereotypes associated with racism, classism, sexism, ageism, and ableism, showing consistency with intersectionality theory.
Worse health outcomes. Numerous studies discussed internalization of stigma and pervasive discrimination on youth well-being (Table 1). Increased risk of contracting transmittable diseases (such as sexually transmitted diseases), developing mental illnesses from chronic stress, major depressive symptoms, suicidality, using substances to cope, food insecurity, exposure to violence, being victims of violence, and lower quality of life and opportunities in managing chronic diseases were commonly found health outcomes that are consequences when unhoused youth are not recognized as humans deserving equitable treatments and support services (Ausikatitis et al., 2015; Brothers et al., 2020; Bruce et al., 2014; Crumé et al., 2019; Dang et al., 2019; Gattis & Larson, 2016; Hudson et al., 2010; Reck, 2009; Santa Maria et al., 2015; Semanchin Jones, Bowen, & Ball, 2018; Shelton, 2015; Shelton, 2016; Toolis & Hammack, 2015). These health disparities further marginalize the population from thriving.
Discussion
It is evident that unhoused youth experience interconnected social stigma and discrimination. Numerous aspects of youth's lives, such as accessing education, healthcare, and community spaces, are often highly regulated on how youth should present themselves. Using the socio-ecological model and intersectionality framework, unhoused youth have shown to be victims of classism amplified by other forms of identity-based oppressions, such as racism, sexism, transphobia, ableism, etc. NIMBY and Mayberry public attitudes and policies contribute to the call for increased policing and surveillance. NIMBY was defined as opposition to development of housing and other community facilities, usually rooted in the assumption that current residents’ home values and quality of life would decrease (Pendall, 1999). Mayberry, on the other hand, denoted the lack of awareness of community issues, such as youth homelessness, and highlighted the need for order and utopia (Harter et al., 2005). Without an acknowledgment that youth homelessness exists and that social community resources such as supportive permanent housing are needed, unhoused youth face immense challenges in exiting homelessness.
It is concerning that spaces intended to be supporting unhoused youth toward journey of being permanently housed safely can become extremely harmful as to limiting access. In mapping out a nonexhaustive list of how, where, and who drive stigma and discrimination (Figure 3), this integrative literature review offers a starting point to eliminate barriers for unhoused youth.
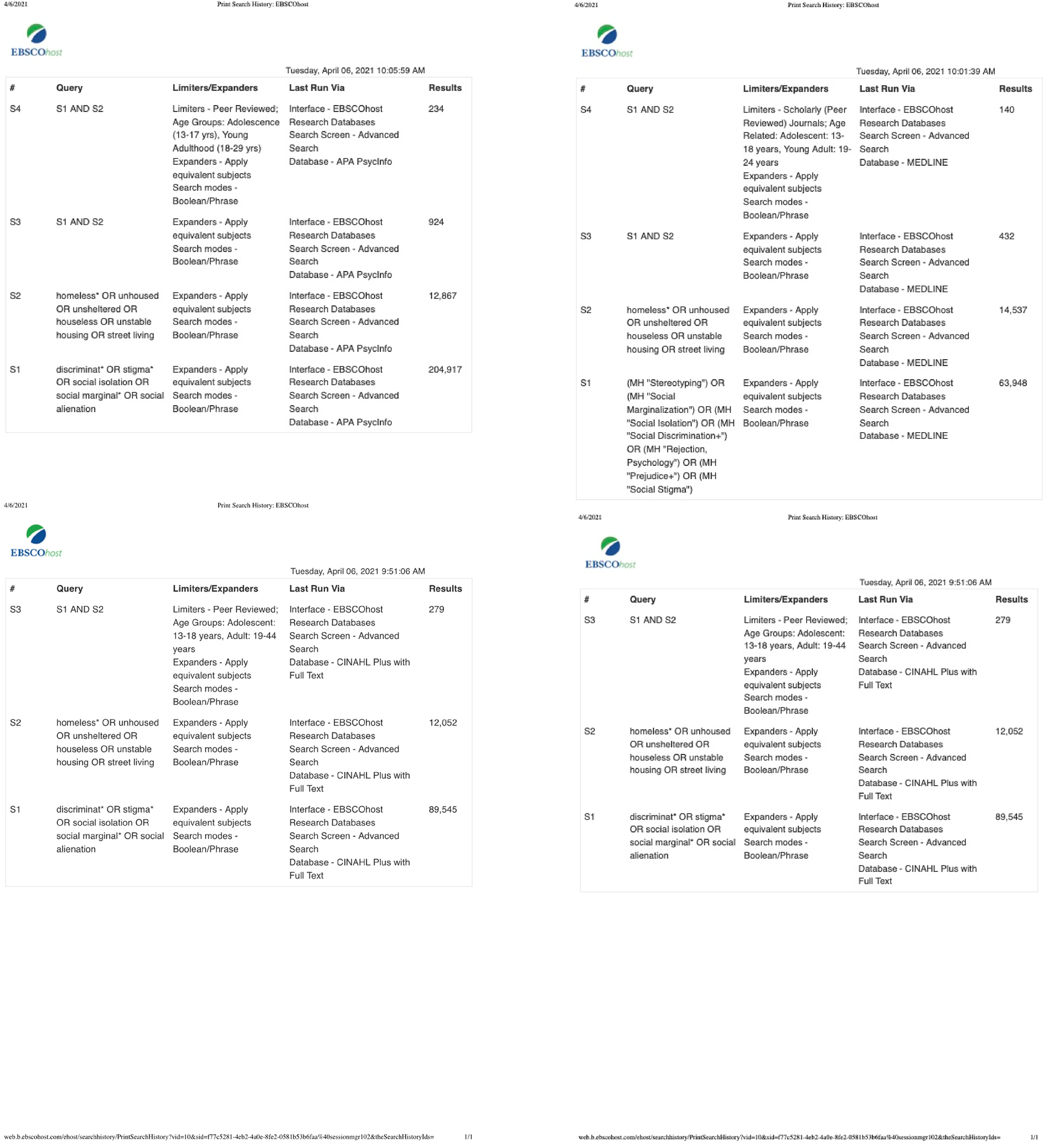
Search terms and filters used to find articles from CINAHL, MEDLINE, PsycInfo, and SocINDEX.
Implications
Nursing. Nurses work in inpatient and outpatient settings with a holistic view of the patients, as well as nonclinical settings. Nurses should ask for inclusive healthcare delivery training that includes continuously reflecting on their own assumptions, involving youth in decision-making, knowing how to assess social needs, and understanding how health disparities are perpetuated for unhoused youth. Nursing as a profession can hold an individualized and systems-level critical view towards the patients; understanding that systems drive certain health behaviors that produce certain health outcomes, and currently, systems supporting unhoused youth do not allow space for them to make decisions that achieve economic mobility and facilitate their exit from homelessness. Nor do these systems help to prevent re-entry into homelessness. Nurses are called upon to use a trauma-informed care model to acknowledge youth experiences and establish trust within therapeutic relationships. Nurses can become engaging health educators in making prevention health information more accessible to youth and how they can be connected to resources for applying this knowledge. Nurses need to be at the forefront to advocate for antiracist, gender-affirming, and inclusive built-care environments to address compounding the effects of stigma and discrimination through the lens of intersectionality. Public health nurses have skills to collaborate with street outreach workers and address health and social issues at the same time.
School. Schools are encouraged to implement evidence-based strategies, especially because schools are often the primary and only place in which unhoused students can access care. School nurses can be advocates and leaders in developing and directing programs and practices for this vulnerable population. Throughout stages of engagement, unhoused youth need always to be included in planning and decision-making, such as serving on advisory boards. Additionally, school nurses can utilize Every Student Succeed Act (ESSA) to request more funding for supporting unhoused youth through Titles I, II, and IV for activities, including school-wide housing needs assessment, providing trauma-informed care, creating antidiscriminatory learning environment, supplying items to fulfill basic needs (clothing, hygiene, food, sleep, and social network), coordinating with local partners in supplying housing, and advocating for housing to be included as a measurable indicator for academic success (Blackborow et al., 2017; Moore et al., 2019). School nurses can further request funding for the professional development of staff, particularly in areas of applying structural competency and intersectionality to view homelessness as a solvable structural problem (Blackborow et al., 2018). Some other interventions that schools can implement:
Use Positive Youth Development Framework, such as providing opportunities for group and individual recreational activities (Benson et al., 2006). Implement alternative pedagogy that engages traditional knowledge and lived experiences. Provide opportunities for healthy identity exploration and relationship building among classmates and school staff. Advertise the role of McKinney-Vento Act liaison to increase outreach to youth living in unstable housing (National Center for Homeless Education, 2018). Proactively screen students and households for risk of homelessness, as well as social needs. Compile local resources for unhoused youth and support in navigating those resources Transition towards a model of compassion and support in understanding causes of why students may miss school or changes in behaviors, and away from the model of punishment and criminalization. Believe in youth when they choose to disclose about housing status and other health concerns. Investing in schools to ensure that they are staffed with nurses, particularly for schools in under-resourced communities Advocating for expansion and protection of youth's human rights in areas such as housing, anti-racism, reproductive health, LGBTQ+, disability, etc. Investing in community organizations, clinics, building intersectional spaces, and programming activities that foster positive relational health and keep youth safe. Expanding policies that promote economic mobility, such as tax credit, raising minimum wage, basic income program, access to affordable healthcare, affordable education, and job training programs, etc. Unhoused youths’ needs span beyond educational spaces. Additional policy recommendations are discussed in addressing youth homelessness, stigma, and discrimination that require larger societal responses. The Housing First model has proved its powerful effectiveness in improving health outcomes, reducing visits to emergency rooms, and increasing housing stability long term (Baxter et al., 2019). Housing First model is guided by the core principles of: Everyone has the right to housing, little to zero conditions in accessing housing, using support services is voluntary, and rapid entry to housing (Baxter et al., 2019). Therefore, Housing First should be considered as a standard in addressing homelessness on organizational and public policy levels. Social services can then be provided as wrap-around, with basic needs being prioritized at the same time as housing placement. For non-HUD-funded social housing, policies containing language like the Equal Access Rule should be adopted, especially in state, city, and privately funded housing. Shelters and other forms of housing need to re-examine cisgender policies to be more inclusive of transgender individuals. Unhoused youth who are 21 years of age and older should also be considered a particular focus for public policy support, as they face immense challenges navigating young adulthood, a demanding workforce, and independent living. Healthcare systems have an opportunity to re-examine their triage and discharge policy guidelines for unhoused youth, collaborate with community partners, and train their staff on structural processes impacting re-admission for unhoused youth. The evidence of stigma and discrimination against unhoused youth within healthcare is enormous. Therefore, healthcare systems and their clinicians need to incorporate access to housing as part of the discharge process, effective triage processes that do not exclude people who experience homelessness and instead prioritize objective health needs, and employ health system navigators who are contextually aware and proficient in cross-system communications. Clinical nurses are often the first members of the care team who unhoused youth encounter in hospital settings. Therefore, nurses are a powerful force in shaping positive experiences of accessing healthcare. Some other include nondiscrimination clauses and an enforcement mechanism into Runaway and Homeless Youth Act (Family and Youth Services Bureau, 2018) Hold law enforcement accountable for discrimination based on profiling and unjust civilian violence. Adopt policy to ensure adequate affordable housing and limit gentrification that displaces people. Create safeguards for successful transition out of foster care, justice system, and mental health care that prevent (re)entry into homelessness and victimization. Expand technology and broadband access. Remove criminalization of survival strategies. Provide incentives for employers to hire youth with a criminal history.
Policy. Policy changes are cornerstones for producing sustainable impacts, especially at the structural level. Education systems can pursue the following policy recommendations that support school nurses’ efforts to address social stigma and discrimination against unhoused students and youth at large.
Limitations
Despite the extensive nature of this review, several limitations are important to address. Studies included are written in English and conducted within the United States. Therefore, the experiences of unhoused youth may not be fully captured in other contexts. The decision to exclude op-eds, case reports, and commentaries may have also limited the extent of stigma and discrimination against unhoused youth. However, this creates an opportunity to acknowledge that this issue spans more than personal responsibility; it calls for a system approach, policy-driven, and greater involvement of nurses in ensuring the excellent health of unhoused youth. The Crowe Appraisal tool asks users to provide a subjective score after considering reflective questions. It can create disparity in scoring article quality. Four of the included studies scored below 28 points (below 1 standard deviation to the median of the critical appraisal score), with 24 studies scoring above 28 points. Future research studies should also explore how stigma and discrimination are perpetuated within the research realm, the effectiveness of housing-related programs, and how to drive culture around addressing homelessness away from criminalization and towards strong social commitments. Additionally, the article selection process was completed in April of 2021, which does not contain any new studies published after that time. Since then, more studies may have also addressed the issue of social stigma and discrimination against unhoused youth. Future research studies should examine articles after April 2021.
Conclusion
Unhoused youth experience multi-level challenges to survive and balance a dynamic period in their lives. Social stigma and discrimination complicate those challenges even further, limiting youth from opportunities that can ensure their wellness and positive developmental outcomes. Every nurse within schools and the community needs to be committed to creating a welcoming environment for unhoused youth, working in partnership with them in addressing their needs, and advocating for a just system through policy changes that prioritize unhoused youth's perspectives, health, and access to housing.
Footnotes
Author's Note
Change of affiliation. Huy Le is now a Registered Nurse at The Johns Hopkins Hospital based in Baltimore, MD
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.