
Abstract
We study the effects of hospital consolidations on access to care in a competitive healthcare market in the presence of performance incentives. We consider a transition from a “pre-merger” market configuration where a payer delegates services to a market with two competing hospitals to a “horizontally consolidated” configuration under which the same entity manages two hospitals. We focus on two research questions: How should the payer set access-based performance incentives in response to a horizontal market consolidation? What are the effects of consolidation on patient access to care? We use queueing dynamics to describe patient care processes and analyze the strategic interactions between hospitals and the optimal design of performance-based incentives in different market configurations. Specifically, we consider contracts where hospital compensation for delivering care includes a combination of fee-for-service payments and bonus components tied to the level of access to care patients receive. We derive the optimal bonus-type contracts that the payer can use to adapt to changes in market concentration, and we quantify the resulting impact on patient access to care and social welfare. In our analysis, we consider two alternative settings: the “fixed-FFS” setting, where the fee-for-service component cannot be altered, and the “flexible-FFS” setting, where both the fee-for-service and the bonus components can be adjusted in response to changes in the market composition. Our analysis shows that the bonus-type performance incentives provide the payer with the ability to protect patient access to care upon hospital consolidation in a wide range of problem settings, provided that the intensity of competition between the hospitals is sufficiently strong. If, otherwise, the intensity of competition is relatively weak, horizontal consolidation may compromise access to care.
Introduction
Merger and acquisition (M&A) activities have increased significantly in healthcare markets over the past two decades. In the US,
Although the declared motives for hospital mergers often include efficiency and integration-of-care arguments, the change in bargaining power with payers that a merger provides may not always be accompanied by true, efficiency-improving integration. Consolidation can be either beneficial or harmful, as it reduces competition and enhances a hospital’s market power, which may have undesirable consequences. Diagnosing whether a particular merger will enhance or degrade patients’ access to and quality of care lies at the heart of anti-competitive analysis (see, e.g., a recent debate on the effect of consolidation and anti-competitive conduct in healthcare markets in the US House of Representatives 1 ). In the United States, the Federal Trade Commission (FTC) assesses M&A proposals and challenges them if significant anti-competitive effects are identified (see DOJ and FTC, 2023 and Pear, 2014 for several M&A cases blocked by the FTC).
Accessibility is one of the key performance metrics in any healthcare system. Access to care has been defined as “the timely use of personal health services to achieve the best possible health outcomes” (IOM, 1993) and consists of three major dimensions: coverage (gaining entry into healthcare systems, usually through insurance coverage), geographic availability (resources and convenience of access to resources), and timeliness of care (ability to provide care when the need is recognized). In its Quality Chasm report (IOM, 2001), the Institute of Medicine (IOM) defined timeliness as “reducing waits and sometimes harmful delays for both those who receive and those who give care” and recommended the adoption of six quality aims, namely, timeliness, safety, effectiveness, patient-centered care, efficiency, and equity, for improving the US healthcare system. Delays in receiving clinically required tests or treatments may also negatively impact health outcomes and the overall cost of care (Ryu and Lee, 2017).
Regulators closely monitor key timeliness performance indicators such as average waiting time for an appointment with a doctor (see, e.g., AHRQ, 2016, Siciliani et al., 2013, OECD, 2018). The UK’s National Health Service (NHS) sets waiting time targets (e.g.,
Despite the importance of access to care and the existence of an extensive body of empirical and theoretical literature on the effects of competition on the quality of and access to care (see Jiang et al., 2020 and the references therein), Gaynor et al. (2012) appears to be the only empirical study that systematically investigated the impact of mergers on hospital waiting times. Ryu and Lee (2017) argued that the fee-for-service (FFS) payment system rewards longer waits, which, in turn, leads to higher operating costs because of patient no-shows and patient dissatisfaction; the authors thus proposed value-based payment models. 2
Our article aims to complement this literature by investigating the effects of hospital mergers on access to care and the design of performance incentives. Note that mergers may impact access to care and other quality measures such as effectiveness of care (i.e., clinical outcomes) at the same time. However, analyzing the strategic interactions of both timeliness and other quality measures under competition and performance incentives at the same time is analytically challenging (see, e.g., Jiang et al., 2020 for an analysis that accounts for access and quality competition and performance incentives without considering consolidations). As a complement to the existing extensive literature on the effect of consolidation on quality of care (see Brekke et al., 2017b and the references therein), this paper aims to gain deeper insights into the effects of consolidations on the access to care and how these effects are influenced by the design of performance incentives.
Performance-based incentives link financial payments by payers to the performance metrics of healthcare providers. Various pay-for-performance (P4P) programs have been prevalent in healthcare markets; see Milstein and Schreyoegg (2016) for a comprehensive review of various P4P programs in OECD countries, including those that were specifically designed to reduce waiting times. These financial incentives can come in the form of a bonus, a penalty, or a combination of both. For example, Canada and Australia introduced bonus incentives for emergency care to encourage hospitals to meet waiting time targets. In the United Kingdom, the NHS penalizes hospitals for breaching waiting time targets while introducing a set of best-practice tariffs on top of the DRG-based standard rate to reward the improvements in quality, including meeting the timeliness-of-care standard. A payment scheme can also incorporate “yardstick” contracts that include both bonuses and penalties (Savva et al., 2019). There is no consensus regarding what type of incentive is optimal (see Jiang et al., 2020 and references therein for the optimal design of performance-based contracts). In this article, we focus on bonus incentives and leave other performance incentive contracts for further consideration. We address two key research questions:
How should a payer design access-based performance incentives in response to market consolidation? What are the effects of horizontal hospital consolidation on access to care and social welfare?
To answer these questions, we adopt a two-stage competition model to represent the structure of the healthcare markets: in the first stage, the insurers design and negotiate contracts to acquire services from hospitals, while in the second stage, the contracted hospitals engage in non-price competition for patient volume. Gaynor and Pflum (2017) argue that such a market structure is due to the key institutional feature of healthcare markets: insurers are the primary payers for care and individuals are the consumers of care services. Hence, to account for the impacts of consolidations, we need to model the interactions between the payer and hospitals under a performance-based contract and the interactions between hospitals that are competing on timeliness of care.
To the best of our knowledge, our paper is the first in the operations management literature to investigate the effects of mergers and acquisitions on patient access to care and the ability of the payers to control these effects via performance-based incentives. To identify the effects of market consolidation and the interaction between performance-based incentives and competition, we analyze two different settings in a principal-agent framework: a setting with two competing hospitals, and a setting with a horizontal consolidation. Our main results indicate that the ability of the payer to adjust bonus-based performance incentives plays a key role in preserving patient access to care following a hospital merger, and that the effects of horizontal consolidation are driven by the intensity of competition between hospitals. Specifically, horizontal consolidation can preserve access to care when the intensity of competition is sufficiently strong. If, otherwise, the intensity of competition is relatively weak, horizontal consolidation may compromise access to care and also reduce the social welfare.
The rest of this article is organized as follows. Section 2 reviews the literature. Section 3 describes the problem, followed by models that describe a “pre-merger” setting and a setting corresponding to horizontal market consolidation. In Sections 4 and 5, we provide a detailed analysis of the models introduced in Section 3. In Section 6, we identify the effects of horizontal consolidation on access to care and social welfare. In Section 7, we provide a numerical study to examine the robustness of our findings with respect to alternative functional dependencies of patient benefits and hospital costs on patient access levels. Finally, we discuss our findings in Section 8. The proofs of all analytical results are in the Electronic Companion.
Related Literature
Our article contributes to three streams of literature: competition in healthcare markets, hospital consolidation, and performance-based contracting.
Competition in Healthcare Markets
There is a rich stream of literature on competition in healthcare markets, particularly, on the dimensions of price, clinical quality, and access to care; see Gaynor and Town (2012a), Gaynor and Town (2015) for comprehensive surveys of the theoretical and empirical studies on this topic. (For the studies on competition in general service industries, see Allon and Federgruen, 2007, 2008, 2009, Bernstein and Federgruen, 2004 and the references therein.)
If prices are regulated and providers are profit maximizers, both theoretical and empirical studies indicate that quality competition results in higher quality (see, e.g., Pope, 1989, Brekke et al., 2006, 2010a, Gaynor et al., 2012, Gaynor et al., 2013, Gaynor, 2021 and the references therein). However, if hospitals are semi-altruistic, quality competition may not lead to higher quality (Brekke et al., 2011). If both price and quality are endogenous, the effects of competition on quality become more complex. For example, using patient travel costs as an inverse measure of the degree of competition, Ma and Burgess (1993) and Gravelle (1999) found that more intense competition had no effect on quality because the direct and positive effect of higher competition level on quality is offset by the indirect and negative effect of lower prices. Economides (1993) showed that as the number of providers in the market goes up, the incentive to invest in quality is reduced, as greater competition dilutes per-provider demand and, consequently, the marginal benefit of increasing quality. Brekke et al. (2010b) argued that reducing patient travel costs or increasing the number of competing hospitals can increase quality in the presence of income effects.
Brekke et al. (2008) studied a healthcare market consisting of multiple public hospitals that differ in location and compete on waiting time, and patients who may choose between hospitals (competitive segment), as well as patients who can only choose their local hospital (monopoly segment). They showed that, compared with a monopoly, hospital competition leads to longer waiting times in equilibrium if the competitive segment is sufficiently large. Unlike our model, Brekke et al. (2008) did not consider performance-based contracts. Savva et al. (2019) studied how a regulator can design “yardstick” compensation contracts to incentivize monopoly service providers to compete on waiting times, demonstrating that yardstick competition can reduce costs and waiting times. Our paper differs from theirs in its focus on how bonus-type performance incentives and horizontal consolidation impact access to care.
More recently, Jiang et al. (2020) explored the interactions between performance incentives and joint quality and access competition. Using a principal-agent framework, they examined how performance incentives interact with competitiveness and information asymmetry between the payer and hospitals. Our paper limits its focus to patient access and builds on earlier studies by analyzing the effects of changes in market concentration that preserve the overall composition of the payer-provider ecosystem.
Hospital Consolidation
Despite a growing body of empirical literature on the impact of hospital consolidation on prices, timeliness, and the clinical aspects of care quality, the results of such studies are mixed. Although some studies found that mergers are associated with decreases in both the costs and revenues of merging hospitals (Alexander et al., 1996, Dranove and Lindrooth, 2003, Neother et al., 2017, 2019), others found that hospital mergers resulted in higher prices (Dafny et al., 2019). Although Neother et al. (2019) showed that mergers led to statistically significant improvements of the outcome measures of quality, many of the previous studies on hospital mergers reported no significant impact on those measures (Ho and Hamilton, 2000, Gaynor et al., 2012, Neother et al., 2017). In addition, the studies on the effects of competition in healthcare markets have provided extensive evidence of higher operating costs, lower quality, and higher prices associated with increased market concentration (Kessler and Geppert, 2005, Gaynor and Town, 2012b, Gaynor et al., 2013, Gaynor and Town, 2015, Gaynor, 2021). Regarding access to care, Gaynor et al. (2012) empirically examined the impact of mergers within the NHS on both financial and quality performance, including clinical outcomes and waiting times, finding that mergers led to worse financial performance and longer patient waiting times with no indication of clinical quality improvement.
There are only a few theoretical studies on hospital mergers. Calem et al. (1999) studied the social welfare effects of mergers in a duopoly, with hospitals competing on both quality and price, showing that mergers may enhance patient welfare since they may mitigate the over-utilization externality induced by insurance. Brekke (2004) analyzed the profitability of mergers when hospitals compete on either price and quality or solely on quality during wage negotiations with physician unions. He discovered that the profitability of hospital mergers depends on the bargaining structure, the nature of competition (price or non-price competition), and patient co-payment rates. Brekke et al. (2017b) focused on the effects of a hospital merger in a spatial competition framework where three symmetric semi-altruistic hospitals choose quality and make cost containment efforts. They showed that, although a merger almost always leads to some efficiency gains (cost reduction), the effect of competition on quality of care depends on the degree of altruism and the effectiveness of post-merger cost-containment efforts. None of the aforementioned papers on horizontal hospital mergers has addressed access to care.
We contribute to the literature in this area by addressing the effects of horizontal mergers on access to care in the presence of access-based performance incentives.
Performance-Based Contracting
There is a growing body of literature on performance-based contracting in operations management (see Akan et al., 2011 for general services, Ren and Zhou, 2008 and Hasija et al., 2008 for call center services, and De Fraja, 2000, So and Tang, 2000, Fuloria and Zenios, 2001, Jiang et al., 2012, 2020, Lee and Zenios, 2012, Andritsos and Aflaki, 2015, Zhang et al., 2016, Ghamat et al., 2018, Adida and Bravo, 2019, Andritsos and Aflaki, 2019, and Savva et al., 2019 for healthcare services). Most of these papers have focused on a setting with a monopolistic service provider. Kim et al. (2022) conduct a comprehensive literature review of performance-based contracts in several industries. Fainman and Kucukyazici (2020) provide an in-depth survey of healthcare payment models, including performance-based contracts.
Andritsos and Aflaki (2015) compared the monopolistic and two duopolistic settings to reveal that introducing competition can hamper a hospital’s ability to achieve economies of scale and may increase patient wait times. Zhang et al. (2016) analyzed the effectiveness of the Hospital Readmissions Reduction Program (HRRP) in encouraging hospitals to reduce readmissions. They showed that this competition fostered by HRRP can be counterproductive: it increases the number of non-incentivized hospitals, which prefer paying penalties over reducing readmissions in any equilibrium. Ghamat et al. (2018) examined performance-based payment contracts to promote the optimal use of an optional diagnostic test for newly diagnosed cancer patients, and show that, in the presence of information asymmetry, a healthcare payer should never incentivize an oncologist to use a diagnostic test for all patients, even if the diagnostic test is available for free. Adida and Bravo (2019) studied outcome-based penalty contracts to replace inefficient FFS contracts for healthcare referral services and showed that a penalty contract can generally coordinate the effort decisions with either the system optimum or the social optimum. Andritsos and Aflaki (2019) compared the relative effectiveness of performance-based and bundle contracts in reducing readmissions while keeping combined patient costs and funder payments to the hospital low. Savva et al. (2019) considered a performance-based contract based on yardstick competition, and Jiang et al. (2020) studied bonus-based contracts for two hospitals that compete on quality of and access to care, with cost information asymmetry between the payer and two hospitals. Arifoglu et al. (2021) investigated how various payment models can incentivize care providers to reduce treatment failures and hospital readmissions. Rajagopalan and Tong (2022) highlighted the benefits of performance-based reimbursement policies in two-level referral-based healthcare systems. However, none of these papers considered horizontal market consolidation.
Model Formulation
We consider a healthcare system consisting of a payer (e.g., a government agency) and healthcare service providers (hospitals), indexed by
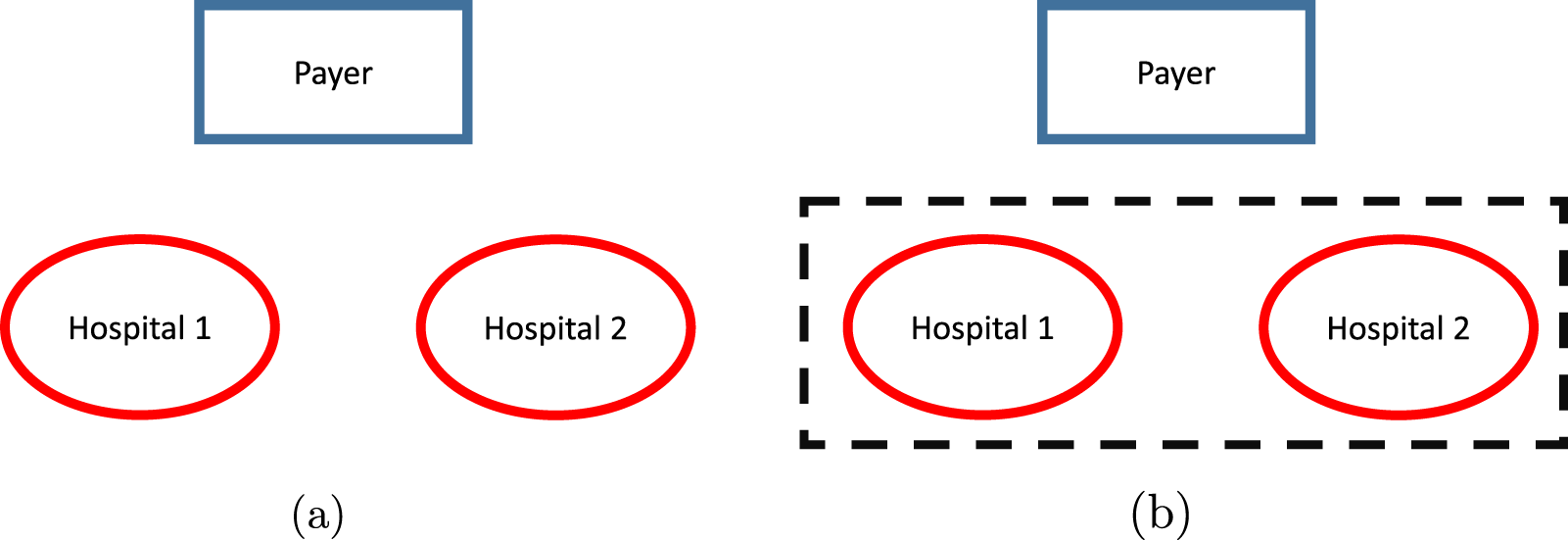
Market configurations: (a) pre-merger market and (b) horizontal consolidation.
In modeling the demand for hospital services in a duopoly, we consider two markets separated by a distance

If a patient is served by hospital

Parameter
Although, following Jiang et al. (2020), we use the assumption of identical market sizes for the two markets for algebraic convenience and analytical tractability, our analysis can be easily extended to settings with non-identical market sizes. Let
The expected daily demand function for hospital

The condition
Jiang et al. (2020) demonstrated how to derive linear approximation (3) from a multinomial choice (MNL) model with the first-order Taylor polynomial. The coefficient
Patient hospital care is a complex, multi-phase process, and our modeling approach aims to focus on the essential, macroscopic features of this process rather than on a detailed, high-resolution picture of a patient’s hospital treatment and recovery. The overriding rationale behind our modeling approach is to highlight the connection between a hospital’s investment in the treatment capacity (e.g., the number of certified beds, personnel, and equipment) and patient choice of hospitals, with the conduit being the main non-financial measure of patient access to care, which is reflected by the expected time a patient must wait before receiving care. Our treatment of patient care dynamics follows an approach frequently used in the literature (see, e.g., Allon and Federgruen, 2008 and the references therein, Jiang et al., 2020 and Wang et al., 2010) that employs a general
Within the queuing modeling framework, the patient access level at each hospital is set by the interplay between daily patient service rate,
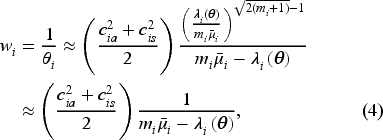
Denoting

For simplicity, we assume that competing hospitals are symmetric in terms of patient service dynamics, so that
Note that an alternative way to measure accessibility is the expected waiting time. Under this alternative approach, the patient benefit can be defined as a linearly decreasing function of the expected waiting time
Hospital Cost and Compensation Functions
In terms of supplying patient care capacity, we assume that a hospital
(H ospital Cost Functions)
The hospital cost functions are

The cost functions (6) reflect, in the simplest form, the facts that improvements in patient access to care are costly, and that the marginal improvements are more costly at high levels of service rate/care capacity. The convex shape of the hospital costs is a standard assumption in the literature. Note that
In our model, we focus on the general, increasingly popular compensation mechanism that combines a fixed FFS rate with adjustable access-level-based components. Note that most performance-based incentive systems define a base compensation for achieving the basic standard of service and then reward performance improvements with bonus incentives (see, e.g., Milstein and Schreyoegg, 2016, Jiang et al., 2020 and references therein). Following Jiang et al. (2020), we consider a linear bonus-based compensation function.
The payment function for both hospitals is given by

The compensation function (7) captures the compensation rate, which combines the base compensation for delivering a service with the incentives that reward greater access levels with the bonus payment
Note that in real healthcare settings, the two incentive components in (7), the FFS rate
In our model, the payer is assumed to possess complete information about the parameters of hospital-based care, including the details of patient care dynamics and, most importantly, the hospital cost parameters. This simplifying assumption leaves out complicating factors associated with potential information asymmetry between hospitals and the payer. It allows the payer to precisely calibrate its financial incentives to the operational characteristics of a particular hospital.
While bonus incentives are prevalent in performance-based incentives (see, e.g., Cashin et al., 2014, Milstein and Schreyoegg, 2016, Jiang et al., 2020 and references therein), it is possible to structure the incentives as penalty-based compensation functions. For example, under the “standard contract” used by the NHS in the United Kingdom (Department of Health, 2022), a step-wise penalty is imposed on a hospital when patients’ delays in accessing elective hospital services exceed a threshold of
Moreover, for simplicity, we impose a lower bound on the FFS rate.
(M inimum FFS Rate)
Assume that
As it becomes clear later, this assumption ensures that hospitals’ profits are non-negative when both access levels are zeros without bonus incentives, which implies that it suffices to restrict hospitals’ access levels to
The set of Assumptions 1–6 outlines a model of a patient care delivery system where better access to care at a hospital, on the one hand, increases patient demand for care at that hospital (and decreases the patient demand at the competing hospital), as well as, potentially, the compensation amount that the facility receives from the payer. On the other hand, better access to care comes at extra operational costs. These qualitative modeling features closely follow the realities of many service markets, including any healthcare market. What makes our model uniquely suited for healthcare contexts is the presence of the payer that imposes, on behalf of patients, a uniform set of performance-based incentives that induce hospitals to deliver acceptable levels of access to care.
In using Assumptions 1–6, we closely follow the literature in modeling the effects of access to care, patients’ benefits, hospital costs, and the payer’s compensations using the simple functional dependencies. Such a streamlined approach is dictated by our focus on the broader societal effects of changes in the structure and the composition of the care delivery ecosystem, along with the need to analytically characterize the access-level equilibria when hospitals and the payer may actively react to such changes. The assumptions about the homogeneity of patient care needs, the symmetry between two hospitals, and a one-dimensional view of hospitals’ treatment capacity are driven by the same rationale. The resulting parsimonious character of our model ignores many of the finer operational and financial details associated with actual patient care and, therefore, precludes us from making precise quantitative predictions. At the same time, we believe that our approach correctly captures the existing trade-offs faced by the parties in the patient-care process; therefore, the qualitative insights resulting from our analysis will display a similar degree of fidelity as those produced by more detailed and complex models.
For notational convenience, in what follows, we normalize the value of
Compensation Rates and Access Levels Under Alternative Market Configurations
We next outline how compensation rates, including the FFS rate and the bonus parameter
Performance-Based Incentives in the Pre-Merger Configuration
In modeling hospital decision-making, we treat each hospital as a risk-neutral, profit-maximizing entity. The choice of profit as a hospital objective is justified in many practical settings. For example, in the United Kingdom, NHS hospitals are funded by the public; however, they are granted substantial managerial and financial autonomy. In particular, hospitals are allowed to retain surplus cash. As a result, UK hospitals are often described as profit maximizers (De Fraja, 2000, Miraldo et al., 2011).
To identify the effect of performance-based incentives on patient access levels, we consider another “pre-merger” configuration where bonus incentives are introduced in addition to the fixed FFS rate specified in Assumption 5. Given any bonus term


Our model allows for a general characterization of the payer’s objective. In particular, we aim to cover a broad set of payers: from a profit-driven private insurance company to a private company that also accounts for social welfare implications of its decisions to a government agency that exclusively focuses on social welfare. Specifically, we follow the literature (see, e.g., Gravelle and Sivy 2010; Makris and Siciliani 2010) to specify the payer’s objective function as
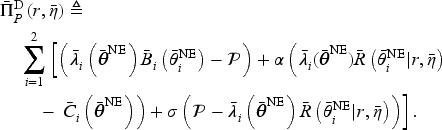


Finally, the participation constraint (11) ensures that hospitals cannot lose money. We use
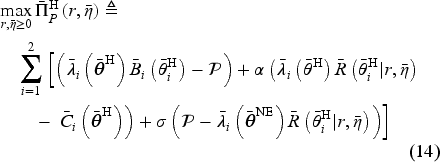
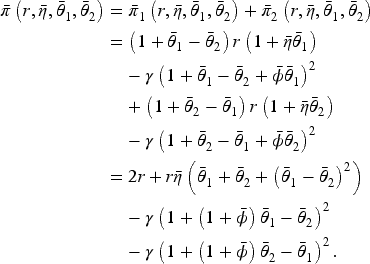
In the setting where the two hospitals merge, the payer faces a single agent that sets the access levels for both hospitals in response to the payer’s incentives. The merged hospital’s optimization problem is



In this section, we analyze the benchmark setting, where two hospitals compete in the presence of the performance-based incentives designed by the payer.
Nash Equilibrium Access Levels
We start by characterizing the competing hospitals’ Nash equilibrium access levels. For convenience, define
Moreover, in the presence of multiple Nash equilibria, we focus on the Pareto-dominant (efficient) Nash equilibrium for ease of analysis. Specifically, a Nash equilibrium is a Pareto-dominant if the resulting payoffs of both hospitals are no less than those would be under any other Nash equilibrium.
Under a contract
(N ash Equilibrium in Pre-Merger Duopoly)
Under any contract Assume Assume
where
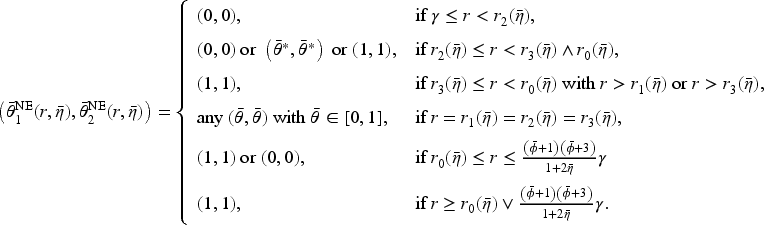

The results in Proposition 1 are intuitive. In particular, for any fixed bonus parameter
The symmetry of Nash equilibria characterized by Proposition 1 implies that the payer’s objective function under a symmetric equilibrium access level (

The “Fixed-FFS” Setting
First, we consider the “fixed-FFS” setting with a fixed FFS rate
(P re-Merger Market: “Fixed-FFS”)
In the pre-merger market under a fixed FFS contract with
If If If If If If

Proposition 2 shows that the equilibrium access level under optimal bonus contract in the fixed-FFS setting increases in the FFS rate
The analysis of the fixed-FFS setting presented in Proposition 2 is very general in that it accounts for any fee-for-service rate
In a pre-merger market in the absence of bonus incentive, the optimal FFS rate,
For For
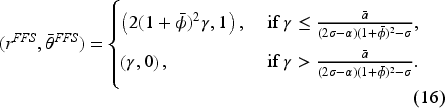
In investigating the impact of the merger in the “fixed-FFS” setting, we will be using the combination of the results in Propositions 2 and 3.
The following proposition characterizes the optimal compensation contract in the pre-merger market under “flexible-FFS” setting.
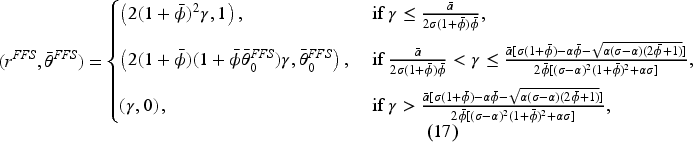
(P re-Merger Market: “Flexible-FFS”)
In the pre-merger market, the optimal FFS rate is always equal to
Assume Assume


The results in Proposition 4 generate several important observations. First, the payer is not in a position to always induce the maximum access levels from the hospitals unless the cost parameter
In this section, we describe how the payer adjusts to changes in provider market concentration and how these changes alter patient access levels under optimal compensation incentives.
Consider a horizontal consolidation/merger between the two hospitals. We assume that this market consolidation does not lead to hospital closures but instead removes competition between them and allows them to coordinate their access levels. Under a given contractual payment function
Patient Access Levels Under Performance-Based Incentives
We start by describing the patient access levels in the consolidated market under a given performance-based compensation contract
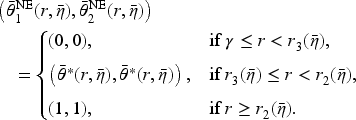
(B est-Response Access Levels in the Consolidated Market)
Consider the contract
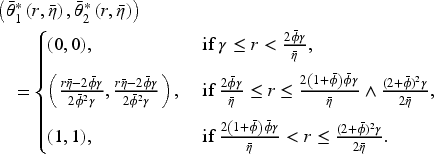
Proposition 5 shows that the optimal hospital access levels under horizontal consolidation are symmetric when
Given the consolidated entity’s best response, we are now ready to characterize the optimal design of the compensation incentives in both “fixed-FFS” and “flexible-FFS” settings.
Optimal Bonus Contracts in a Consolidated Market
Similar to the pre-merger market, we start our analysis with the “fixed-FFS” setting.
The “Fixed-FFS” Setting
Below we characterize the optimal bonus and the resulting access levels.
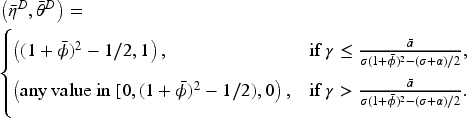
(C onsolidation: “Fixed-FFS”)
In a fixed-FFS setting for a consolidated market with Assume Assume
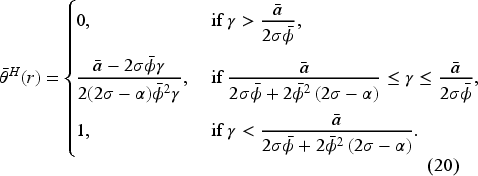
Proposition 6 reveals that the equilibrium access level under horizontal consolidation with an optimal fixed-FFS bonus contract is independent of
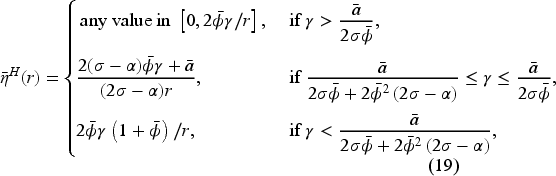
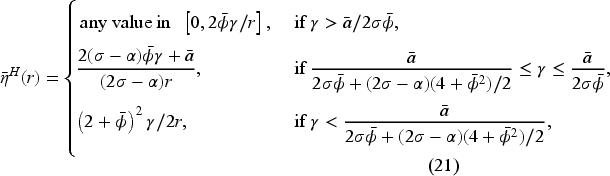
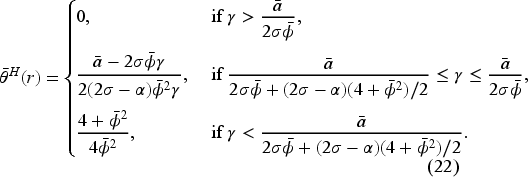
(C onsolidation: “Flexible-FFS”)
In a flexible-FFS setting for a consolidated market, consider a set of bonus contracts such that Assume Assume
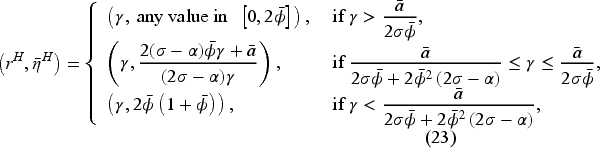
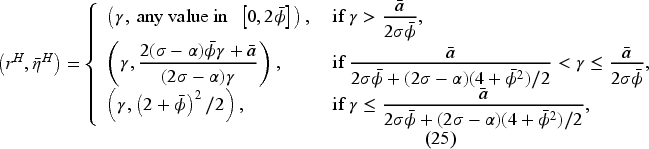
The results in Proposition 7 show that the consolidated market inherits some of the structure of the optimal bonus contract from the pre-merger market, with the optimal FFS rate being
The analytical characterization of the optimal contracts and patient access levels presented in Propositions 1–7 enables the comparison between the pre-merger and consolidated markets under a wide range of market conditions and payer objective functions. In this section, we use these results to focus on the impact of horizontal consolidation on patient access and social welfare for the social planner, that is, the payer whose objective is characterized by


We conduct our analysis separately for the “fixed-FFS” and “flexible-FFS” settings.
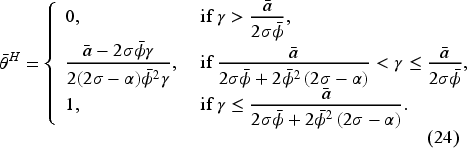
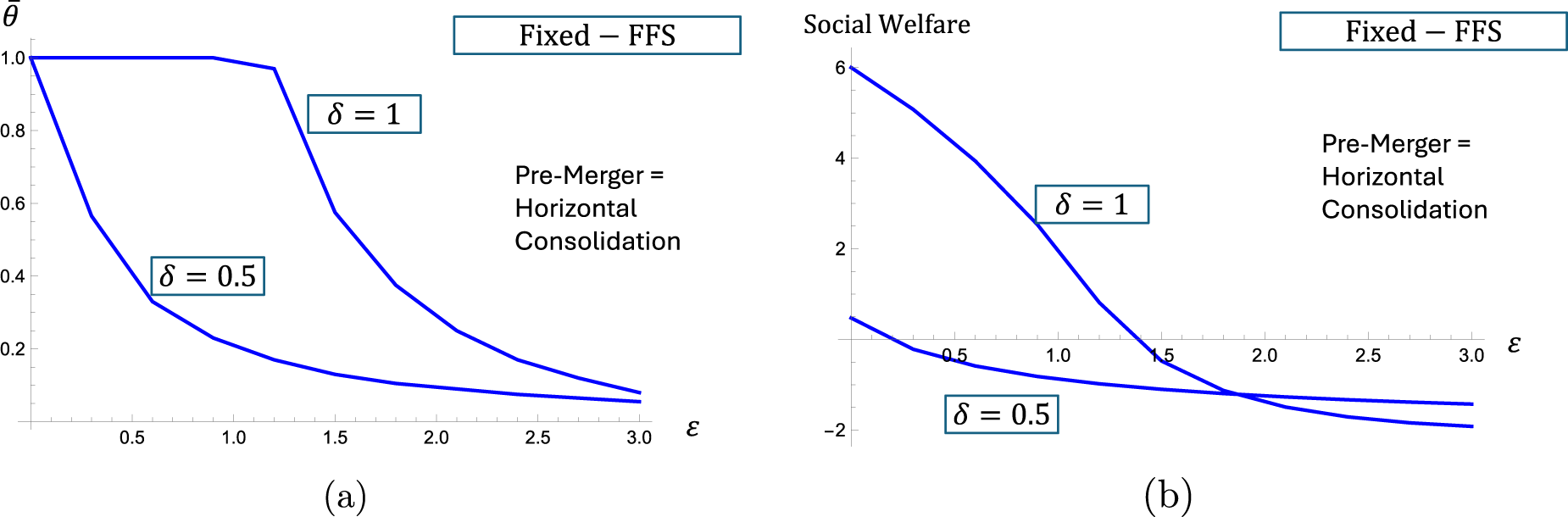
(E ffects of Consolidation: “Fixed-FFS”)
Suppose that the FFS rate is set to
Assume Assume
If If If
Proposition 8 shows that when the FFS rate is anchored at the optimal FFS rate for the pre-merger market without any bonus term,
Effects of consolidation on access levels (AL) and social welfare (SW) under “fixed-FFS.”

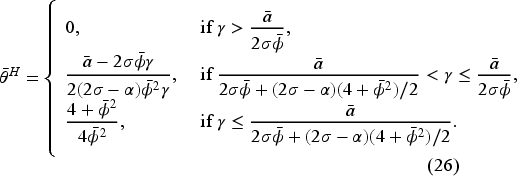
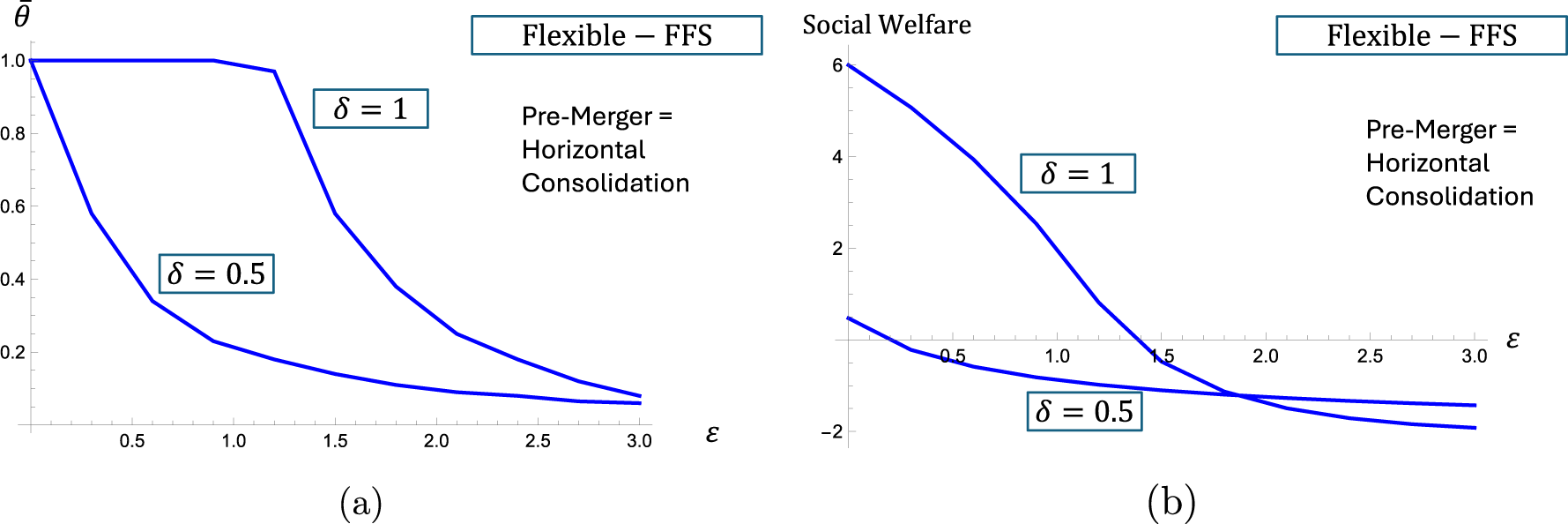
(E ffects of Consolidation: “Flexible-FFS”)
Suppose Assume If If If If Assume Assume If If
Proposition 9 shows that if the social planner has a freedom to adjust the FFS rates away from the value optimal in a pre-merger, no-bonus market, the access levels can be preserved after the merger in a wide range of problem settings.
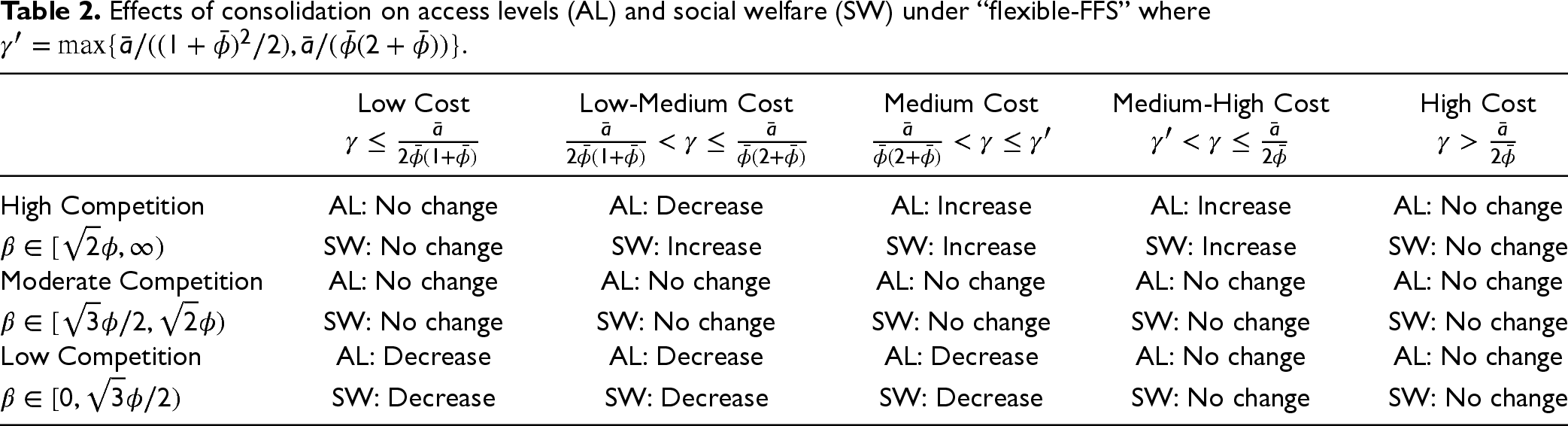
More specifically, when competition intensity is relatively high (i.e.,
When competition intensity is moderate (i.e.,
When competition intensity is relatively low (i.e.,
In sum, the effects of horizontal consolidation are strongly driven by the competition intensity, with horizontal consolidation having no effect on the access to care when the competition between hospitals is sufficiently strong. However, if the intensity of competition is relatively weak, bonus incentive structure may not be able to mitigate the reduction in access to care and social welfare upon horizontal consolidation. The results are summarized as Table 2.
Effects of consolidation on access levels (AL) and social welfare (SW) under “flexible-FFS” where
In our model, we have used the simplest, linear functional forms to describe patient sensitivity to access-to-care levels, and the quadratic functional dependence of the hospitals’ costs on the level of care capacity they provide. In this section, we explore the impact of alternative modeling assumptions with respect to the influence of access-to-care levels on the resulting system outcomes described in Section 6. Specifically, we consider an extended class of patient benefit/utility functions

The shape of the patient benefit function directly influences the shape of the demand function. Following the MNL-based derivation in Jiang et al. (2020), we translate (29) into

To account for hospital cost dependence on care capacity, consider a more general cost function:

Below, we illustrate the impact of varying the degree of convexity of the hospital cost functions (
Figure 2(a) and (b) considers the “fixed-FFS” setting and illustrate the impact on “steeper” cost functions, on achieved access levels as well as social welfare, respectively, for two fixed values of the patient responsiveness coefficient,
The patient access levels (a) and social welfare (b) in “fixed-FFS” setting as functions of the cost parameter
The patient access levels (a) and social welfare (b) in “flexible-FFS” setting as functions of the cost parameter
In healthcare markets where the payer (e.g., a government agency or insurer) acts as the patients’ agent, can patients ultimately benefit from market consolidation? A typical argument raised against provider mergers states that a merger can eliminate competitive pressure, leading to a decrease in patient welfare, which is a key driver for antitrust regulators like FTC and DOJ to challenge merger cases (DOJ and FTC, 2023). While it may be valid in settings where the payer for healthcare services is “inert,” it may need to be carefully examined in settings where the payer can actively react to the merger by adjusting provider compensation. Our article looks at the setting where the payer can use the performance-based incentives to influence the outcomes of provider consolidation.
Specifically, our paper studies the interaction between performance-based incentives and market consolidation in shaping hospitals’ levels of patient access to care. To this end, we start with a non-consolidated market configuration consisting of a payer and two identical healthcare providers/hospitals. In our model, patient access to care is the main factor that determines hospital compensation, patient demand for care, and achieved social welfare levels. The payer adopts a bonus-type performance-based contract to procure medical care services from the hospitals on behalf of the patients. The problem is formulated as a principal-agent model, with the care dynamics of two providers being approximated by two independent
To establish the baseline, we first analyze the optimal contracting problem under the pre-merger configuration with two competing providers. Next, we analyze a horizontal M&A market configuration that is one step short of total centralization. The horizontally-consolidated M&A limit emerges from the decentralized setting upon the merger between care providers, leaving the payer to deal with a completely consolidated provider entity. This horizontally-consolidated setting serves as the limiting case of the actual outcomes of the M&A process, where the final degree of provider-initiated consolidation exceeds the degree of payer-initiated consolidation. In our analysis, we separately look at two distinct settings: the one where the fee-for-service component of hospital compensation is fixed, and the one where the fee-for-service can be adjusted along with the bonus component to mitigate the consequences of hospital merger.
Our study focuses on the potentially negative effect of horizontal consolidation on access levels and on the payer’s ability to use bonus-type performance-based incentives to mitigate the potential threat to social welfare stemming from concentrated provider power. Our main finding is that the ability of the payer to counter the effects of consolidation crucially depends on the strength of inter-hospital competition (or substitution effects) and incentive structure. In particular, when the strength of competition is low, the payer may need to look beyond bonus incentives to retain the same patient access to care since the additional market power enables hospitals to decrease access levels even when faced with “best” payer incentives. However, when the competition is strong, the payer can induce the hospitals to maintain patient’s access to care using bonus incentives.
Thus, our results show that consolidation may not always lead to worse access levels for patients, contrary to the typical inference drawn from consolidation. This is because incentives designed by the payer can alter access levels hospitals provide, despite hospitals gaining more market power from consolidation. Our results offer additional insights into the current debate on M&A processes in healthcare industry; see https://docs.house.gov/Committee/Calendar/ByEvent.aspx?EventID=109024. Although our parsimonious model is unlikely to provide a quantitatively precise characterization of actual market outcomes, we believe that the qualitative conclusions from our analysis are indeed applicable to real-life settings, indicating that if market concentration becomes high, payers may need to look beyond simple provider compensation schemes.
The conclusions we outline above rely on the payer using bonus compensation to incentivize care providers. Such an approach to structuring bonuses belongs to a wider class of performance-based schemes that tie non-FFS provider payments to a provider’s own performance based on a set of performance metrics that the payer associates with a higher societal value of delivered care (access to care, rate of in-hospital infections, mortality rates associated with specific treatments, etc.), with performance measured in relation to absolute pre-specified levels. Such performance-based compensation approaches are likely to be considered fair by the providers because they depend largely on outcomes that providers can control. In practice, payers may pay special attention to such fairness considerations because they affect the payer’s often limited ability to successfully implement performance-based incentives. An alternative and, arguably, more effective approach to system coordination is to use the providers’ relative performance when assigning non-FFS compensation. One example of such compensation is the yardstick-type approach used in the HRRP recently introduced by the Centers for Medicare and Medicaid Services (CMS, 2020). The payer’s ability to implement such performance incentives depends on the degree of market power that the payer has: combined Medicare/Medicaid/SCHIP programs administered by the federal and state governments are responsible for the largest share of national healthcare expenditures in the United States.
The analytical results and the insights we propose have two important limitations that stem from our modeling assumptions. First, we assume that care providers are identical in terms of demand and cost parameters, although we carefully follow the literature in making such assumptions. In other words, we expect our conclusions to hold up to only a certain degree of provider heterogeneity. Establishing the degree of provider heterogeneity that would lead to qualitative changes in our results would provide an important extension of our analysis. Second, we assume a symmetric information setting where the payer knows the provider cost structure with certainty. Analysis of the effectiveness of performance-based incentives in the presence of both changes in provider market concentration and information asymmetry is another promising direction of future research.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478251349889 - Supplemental material for Horizontal Consolidation in Healthcare Markets: Can Performance Incentives Preserve Access to Care?
Supplemental material, sj-pdf-1-pao-10.1177_10591478251349889 for Horizontal Consolidation in Healthcare Markets: Can Performance Incentives Preserve Access to Care? by Houyuan Jiang, Zhan Pang and Sergei Savin in Production and Operations Management
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Houyuan Jiang's research was sponsored by EPSRC Cambridge Centre for Mathematics of Information in Healthcare, grant number EP/T017961/1.
Notes
How to cite this article
Jiang H, Pang Z and Savin S (2026) Horizontal Consolidation in Healthcare Markets: Can Performance Incentives Preserve Access to Care? Production and Operations Management 35(2): 586–605.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.