
Abstract
Prolonged emergency department (ED) length of stay (LOS) is associated with detrimental effects on patient care quality and outcomes. There is evidence that certain groups of patients experience longer LOS based on their gender or race, especially with regard to the part of LOS that is attributable to waiting to be seen by a clinician. This work tackles the patient prioritization and placement aspects of ED operations with the goal of improving throughput and wait time in a fair, equitable way. We present a novel Mixed Integer Linear Programming (MILP) predictive-prescriptive formulation that incorporates a breakdown of predicted patient ED LOS into actionable pieces. We incorporate considerations for fairness and reformulate the MILP formulation into a compact and computationally tractable formulation that can be solved efficiently in real time. To deal with uncertainty, we propose a sampling-based solution, and provide provable guarantees regarding its convergence, stability and sample complexity. The proposed solution increases the throughput of the ED by
Keywords
Introduction
The emergency department (ED) is the entry point for unscheduled admissions to a hospital, and the efficiency of ED operations has direct impact on the operations of the hospital as a whole. EDs typically use the Emergency Severity Index (ESI) to prioritize patients with different conditions (Gilboy et al., 2012). However, capacity imbalances and long wait times are commonly experienced in the ED, with low-priority patients often remaining in the queue for extensive periods (Ferrand et al., 2018). There is evidence also that human factors and hidden biases can affect wait times and access to care for patients from particular genders or racial groups (Owens et al., 2020).
Improving ED operations has been the subject of numerous studies. Approaches have focused on different aspects: Patient scheduling and prioritization schemes, e.g., ensuring that mandatory targets imposed on each patient’s door-to-provider time and length of stay (LOS) can be collectively met with the largest probability (He et al., 2019) or suggesting discrete choice frameworks for triage decisions (Ding et al., 2019); better ED task management, e.g., early task initiation during the triage process to reduce treatment time (Batt and Terwiesch, 2017); and ED design, e.g., the availability of a clinical decision unit (Freeman et al., 2021) or fast-track and other structures within EDs (Ferrand et al., 2018). A queuing theory perspective has been suggested for addressing operational fairness in the ED (Mandelbaum et al., 2012).
This paper focuses on the patient prioritization and placement aspect of ED operations and proposes a novel predictive-prescriptive methodology for dynamically allocating patients to ED beds. There are two important and unique cornerstones of our approach. First, the approach takes advantage of findings from our collaboration with a US hospital and improves the predictability of ED patient LOS through a granular view of ED processes. Second, the approach incorporates considerations for operational and algorithmic fairness, aiming to reduce the occurrence of assignments that may result in disparate outcomes for subgroups of the ED patient population. We are concerned both with outcome fairness, i.e., actual distribution of outcomes, and with process fairness, i.e., ensuring that the process for generating the outcomes is fair (see, e.g., Trautmann and van de Kuilen (2016)).
We consider the ED setting of the hospital with which we collaborated, which is a large urban US academic medical center (AMC) with approximately 70,000 ED arrivals in a typical year. Arriving patients are first triaged (assigned an acuity level) by a nurse. They are placed in ED beds primarily on a first-come first-serve basis based on their case severity (acuity level). Patients with acuity level 1 are the most severe cases, and are assigned an ED bed with highest priority. Patients with acuity levels 2–5 wait until they can be assigned an ED bed. The wait for a bed is the patients’ wait time in the ED, and is referred to as the “arrival-to-room” part of their ED stay. Once assigned an ED bed, patients are evaluated by a physician who is responsible for several patients with similar acuity levels. The patients spend some amount of time in the ED until they are ready to be either discharged or admitted to the hospital. This is the “room-to-disposition” part of patient ED stay. Finally, patients with “disposition” status often spend an additional amount of time in the ED either waiting for transfer to the hospital wards (if they are admitted) or waiting to have their discharge completed. In the meantime, they continue to occupy a bed in the ED, preventing arriving ED patients from being placed in the ED. This is the “disposition-to-depart” part of ED stay.
The “arrival-to-room” part of patient ED stay is most reliably predictable from operational factors related to the ED (Canellas et al., 2021, 2024). Thus, improving operations when it comes to patient placement can have a substantial impact on overall ED patient LOS. Improving bed management processes significantly affects patient satisfaction and wait times, in some studies more so than increasing the ED capacity or workforce (Abo-Hamad and Arisha, 2013). “Arrival-to-room,” or wait time in the ED, is also the component of ED LOS most affected by human bias. The predictive-prescriptive approach proposed in this paper aims to maximize ED throughput while ensuring fair bed allocation by combining prediction for the “room-to-disposition” and “disposition-to-depart” component of patient LOS with a novel prescriptive patient allocation scheme. The algorithm prioritizes patients according to their ESI acuity levels while incorporating patient type arrival uncertainty, the tradeoff between patient wait time and ED throughput, and de-biasing weighting schemes for the allocation of patients from different subgroups. Our contributions can be summarized as follows:
We propose a novel Mixed Integer Linear Programming (MILP) predictive-prescriptive formulation that incorporates a breakdown of patient ED LOS into actionable pieces and allows for a more granular model of ED operations. The “room-to-disposition” and “disposition-to-depart” components of patient ED LOS are predicted and used as an input to our prescriptive framework that determines the “arrival-to-room” part of patient ED LOS. We reformulate our proposed prescriptive formulation into an equivalent one with fewer constraints and state variables that is computationally tractable in real time. We propose efficient solution methods to deal with uncertainty in the constraints and prove guarantees about solution convergence, stability and sample complexity. Our proposed prescriptive model balances multiple objectives, is fast and efficient for realistic instances, and performs consistently close to a clairvoyant oracle with knowledge of the patient arrival process even for a small number of training scenarios. It is flexible enough to incorporate different patient prioritization schemes and preferences when it comes to throughput and patient wait time optimization, and relies only on data available at the hospital at the time of patient arrival. Our approach enforces process fairness and demonstrates desirable characteristics when it comes to outcome fairness in patient prioritization, showing potential for addressing hidden biases in patient wait times. This is accomplished in two ways. First, because our predictive approach breaks down patient LOS into three parts and utilizes only predictions of the parts of ED LOS associated with the patient condition, the part of patient LOS that according to the literature and our own observations is subject to most bias—waiting to be seen by a physician—can be managed algorithmically in a fair way within our prescriptive framework. Second, we suggest de-biasing weighting schemes to ensure process fairness. In tests with real data from the US hospital with which we collaborated, we find that the gender effect observed in wait times realized in the ED disappears in the wait times realized for patients allocated by our algorithm. Our approach does not sacrifice performance to accomplish fairness, supporting the idea that there is not necessarily a trade-off between utility and fairness (De-Arteaga et al., 2022). Our algorithm improves throughput by We illustrate how the output of complex predictive-prescriptive models can be translated into practical recommendations by developing an interpretable metamodel based on our framework. The metamodel is consistent with current ED practices but provides a more informed view of patient allocation in the ED with consideration for capacity balancing based on historical trends for patient arrivals and conditions. Developing such interpretable metamodels provides a path towards the implementation of complex algorithms in practice and increases the likelihood that their operationalization will happen.
In addition to methodological contributions to the literature on patient allocation and scheduling, which we review in more detail in Section EC.1 in the electronic companion, our work contributes to the growing literature on algorithmic bias, specifically in patient diagnosis and treatment. For example, multiple empirical studies have shown that gender can affect wait times and treatment. Chapman et al. (2001) find that women are undiagnosed for chronic obstructive pulmonary disease more often than men and that although diagnostic tools that help reduce this bias exist, they are underutilized by physicians. Primary care is more frequently utilized by women (van der Waals, 1991; Suominen-Taipale et al., 2006; Ruiz and Verbrugge, 1997), yet short-stay services favor men, at least within certain age groups (Ronda et al., 1995; Anson et al., 1991). Women have been also found to wait longer in EDs before being evaluated (Heston and Lewis, 1992; Mondschein et al., 2020).
Patterns of existing healthcare disparities are captured in healthcare data and can be perpetuated through algorithms built on these data. Strategies to evaluate and ensure fairness within a group can involve adjusting the input data, training objective, or algorithm output so that parity of fairness metrics across subgroups is achieved. Importance weighting (Kamiran and Calders, 2012; Krasanakis et al., 2018; Celis and Keswani, 2019) is a pre-processing technique used to address the issue of imbalanced datasets, particularly when it comes to protected subgroups. This technique involves assigning higher weights to infrequent samples belonging to the protected subgroups, thereby balancing the dataset. Another possible technique is regularization (Celis and Keswani, 2019; Kamiran and Calders, 2012; Kim et al., 2018). Carefully selected penalty terms are added to the model’s objective function to discourage it from relying too heavily on features that could lead to biased predictions.
Our predictive-prescriptive algorithm setting extends beyond predictive fairness to operational fairness. Operational fairness is concerned with fair allocation of resources and has been studied extensively in fields like computer science (Li et al., 2021; Kulkarni and Patil, 2015), supply chain management (Ho et al., 2014), and pricing (Cohen et al., 2022). However, operational fairness in the healthcare context presents complex and unique challenges that are difficult to resolve (Armony et al., 2015). Previous work on operational fairness in healthcare has included fair allocation of organ transplantation (Bertsimas et al., 2013) and fair appointment scheduling (Qi, 2017). To the best of our knowledge, ours is the first work on optimal fair patient allocation. In particular, our prescriptive algorithm employs a weight-selection technique that dynamically balances the selection of patients from different subgroups and directly integrates it into recommendations for patient allocation. A specific important contribution of this work is the idea—transferable to other applications in healthcare and beyond—of identifying a breakdown of ED operations into parts that allow for the most biased processes to be addressed with fairer prescriptive algorithms and incorporated holistically into ED patient flow management.
The structure of the paper is as follows. Section 2 sets up our prescriptive model formulation and outlines our approach to integrating fairness in patient allocation decisions. Section 3 describes steps we take to optimize the problem formulation and solution. Section 4 contains a computational case study of the application of our method to the ED with which we collaborated. It discusses findings of gender equity in patient wait times using our proposed approach, the performance of the prescriptive formulation relative to a clairvoyant oracle, and the performance of the overall approach relative to current practices in the hospital. Section 5 describes our proposed generalized approach to increasing the interpretability and the likelihood of operationalization of a complex algorithm by generating an implementable metamodel that is trained to imitate the recommendations of the complex predictive-prescriptive algorithm. It also contains a detailed explanation of the specifics of generating and applying the interpretable metamodel at the hospital with which we collaborated. Section 6 concludes. The electronic companion contains detailed positioning of our work with regard to the broader literature (Section EC.1), proofs (Sections EC.2-EC.4), additional computational experiments (Section EC.5), and sample path analysis to analyze the recommendations of the algorithm to actions taken by the hospital (Sections EC.6-EC.7).
We consider an ED with
Notation.
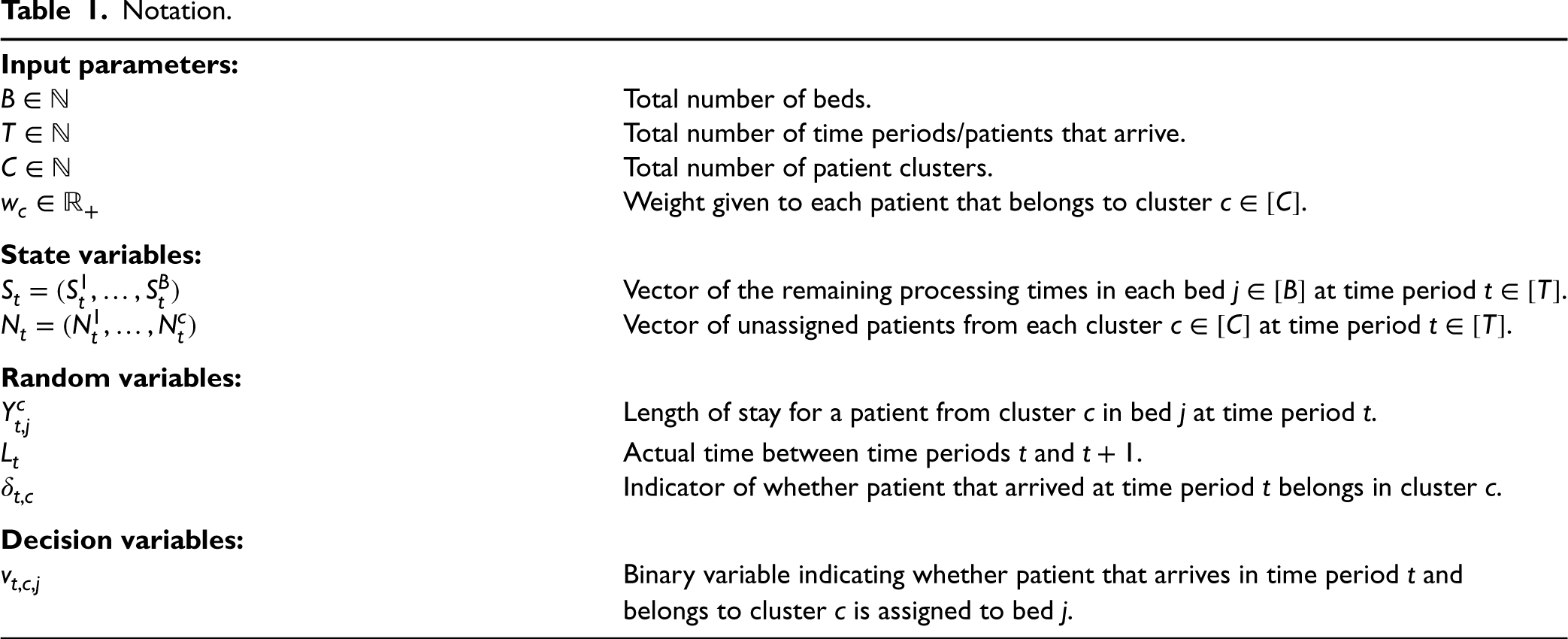
Notation.
The evolution of the state variables is given by the following equations:

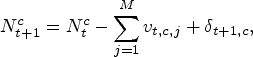
The number of unassigned patients
We propose the following formulation to solve the allocation of patients to ED beds:

Formulation (3) minimizes the expected number of waiting patients under (i) the evolution constraints of the remaining LOS/processing time in each bed and the evolution of the number of waiting patients (first three sets of constraints), (ii) the constraint that no patient can be allocated to a bed if the bed is occupied (fourth set of constraints), (iii) the constraint that the number of allocated patients cannot be more than the patients who are waiting at each time (fifth set of constraints), and (iv) the constraint that we cannot allocate more than one patient to each bed at the same time period (sixth set of constraints). These constraints are dependent on the realizations of random variables. The allocation of patients of the same acuity to beds is performed in first-in first-out order.
We note that formulation (3) utilizes predictions of the “room-to-disposition” plus the “disposition-to-depart” part of patient LOS
Random variables
As will be explained in more detail in Section 4.1, the assignment of ESI scores to patients (i.e., patients to clusters) is an established practice in the hospital, and explicit rules are used by triage nurses to make those assignments. However, these assignments can still be subject to human bias. We propose using the selection of the weights
Specifically, the expression for a particular cluster 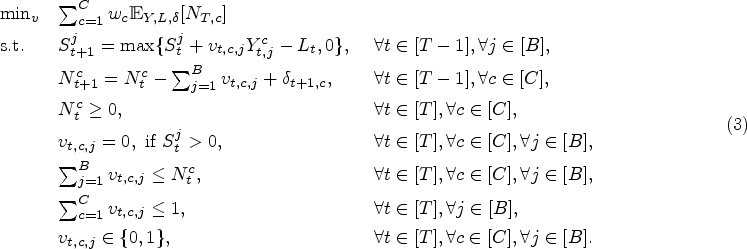


In summary, given expression (4) and requirement (6), the determination of the decision variables
In practice, condition (6) can be enforced by optimizing over all newly defined subclusters with appropriate weights
This section discusses efficient solution approaches to problem (3). First, in Proposition 1 we show that formulation (3) can be written in a more favorable form, with fewer decision variables and easier-to-compute objective. We propose a solution approach that relies on information derived from existing data or generated scenarios, and derive guarantees on the proximity of the solution to the optimal solution. We also discuss solutions to practical issues such as regularization to make sure that the algorithm keeps wait times small. Our findings are valid for any weights Formulation See Section EC.2 in the electronic companion.

By defining the multivariate random variable 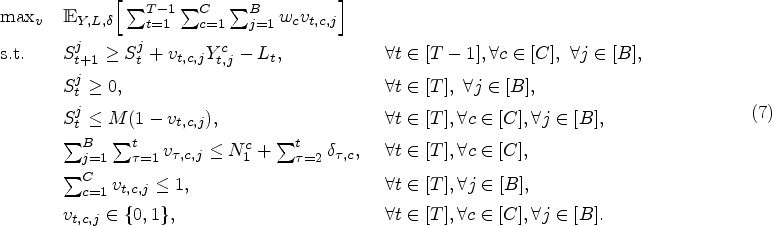

Each time a patient arrives, the hospital has knowledge of the initial conditions (number of patients waiting per cluster, the number of occupied and unoccupied beds) and the cluster (which is usually the acuity level) to which the patient that arrived belongs. By denoting the decision of placing patients at that time as 

As shown in Section Ec.4 of the electronic companion, our method also has three important provable advantages: (i) stability, (ii) low sample complexity, and (iii) asymptotic convergence.
Although formulation (7) provides the optimal solution in terms of throughput, it does not always provide the lowest average wait time. Because both throughput and wait time are important metrics for EDs, we introduce a regularization term in the objective function that penalizes excess wait times. Given a (small) 
We study the insights from our predictive-prescriptive approach in computational experiments with actual data provided to us by a large urban AMC, as described in Section 1. We first provide more details about our dataset (Section 4.1) and discuss the issue of gender imbalance in patient ED wait times. In Section 4.2, we use scenarios from the actual dataset, both to evaluate the performance of our approach compared to existing allocation mechanisms at the ED with which we collaborated and to demonstrate the effect of using our algorithm on reducing gender imbalance in wait times. Sections EC.5.1 and EC.5.2 report additional results to assess the prescriptive part of our approach in particular and gain deeper understanding of its performance relative to a clairvoyant oracle. Sections EC.5.3-EC.5.5 present additional robustness checks with regard to the importance of de-biasing weights, generating prescriptive models for different times of the day, and provider workload. Overall, our experiments demonstrate that reducing bias does not come at the expense of strong performance.
Description of the Data
The dataset used in our computational studies was collected from the Web Intelligence database that links to the ED’s electronic health records in the AMC with which we collaborated. The ED is a level 1 trauma center with 53 licensed ED beds serving approximately 70,000 patients per year. The IRBs at our institutions approved this study as exempt from obtaining informed consent.
Patients presenting to the ED between July 2019 and February 2020 (more than 40,000 patients) were eligible for inclusion if they were 18 years or older in age, were not immediately treated in the resuscitation bay (e.g., trauma activation patients, ST-elevation myocardial infarction patients), and did not leave without being seen (LWBS), elope, leave against medical advice, or expire in the ED. The inclusion dates were chosen to avoid confounders as nine ED beds were added in the summer of 2019 and coronavirus disease 2019 (COVID-19) operational changes began in March 2020. Patients who left the ED prior to formal departure or expired were not included because the disposition and departure timestamps in the electronic health record for these patients are not reliable.
In our experiments, we will assume that patient clusters are determined by the patient ESI acuity level (
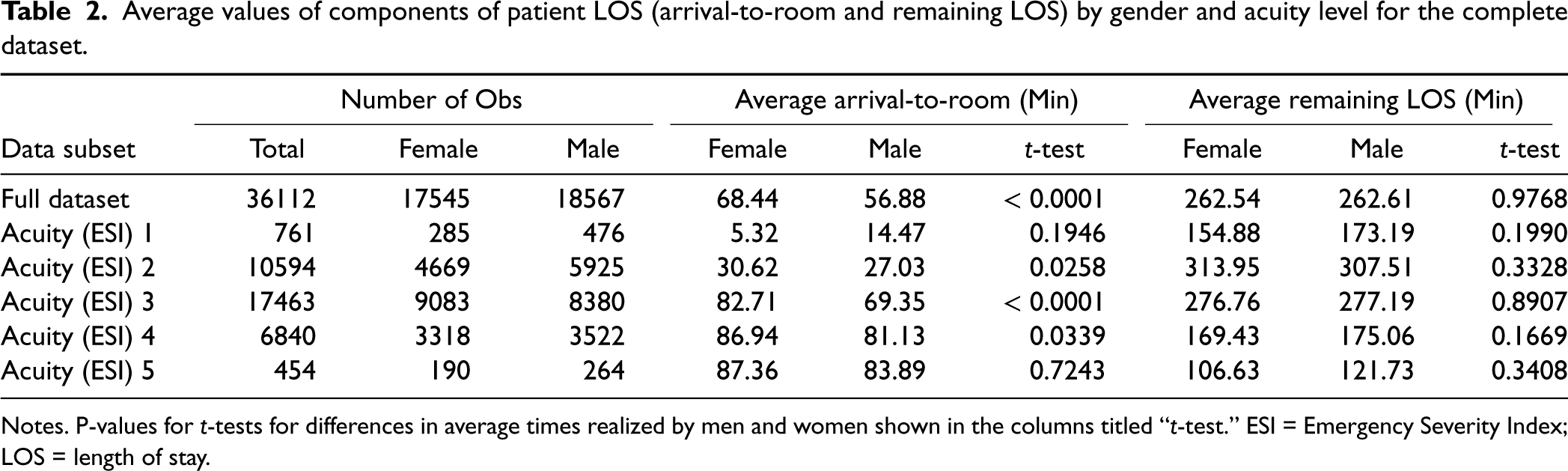
Table 2 displays summary statistics about gender differences in components of patient LOS in the ED. The overall dataset has
Average values of components of patient LOS (arrival-to-room and remaining LOS) by gender and acuity level for the complete dataset.
Average values of components of patient LOS (arrival-to-room and remaining LOS) by gender and acuity level for the complete dataset.
Notes. P-values for
The reasons for observing a discrepancy in average wait times for male and female patients can be complex, including underestimating the severity of female patients’ cases, misunderstanding female patients’ health conditions, differences in the way men and women perceive and experience their illness, unconscious prejudice, or even explicit discrimination. We cannot discern the exact causes for our specific context. Nevertheless, with data provided by the hospital, we were able to establish that there were indeed significant differences in wait times even after controlling for multiple factors: Patient chief complaint using official National Hospital Ambulatory Medical Care Survey (NHAMCS) categories (CDC, 2022), patient demographics (age and gender), vitals (blood pressure, temperature, oxymetry, respitory rate), time variables (hour of the day and day of the week), means of arrival (ambulance, walk in, etc.), and operational metrics related to the state of the ED at the time of patient arrival (nurse-to-patient ratio and number of patients in the last hour to LWBS). We built separate regressions for the full dataset as well as for each ESI level subset with the input variables listed, with arrival-to-room as dependent (output) variable. The regression coefficient in front of the genderMale input variable (
At the same time, Table 2 shows that there are no large discrepancies in female vs. male LOS once a patient is seen: the average remaining LOS is statistically the same for any acuity level. Hence, controlling algorithmically for bias in wait times before a patient is seen has the potential to reduce overall discrepancies in treatment based on gender.
We use a large
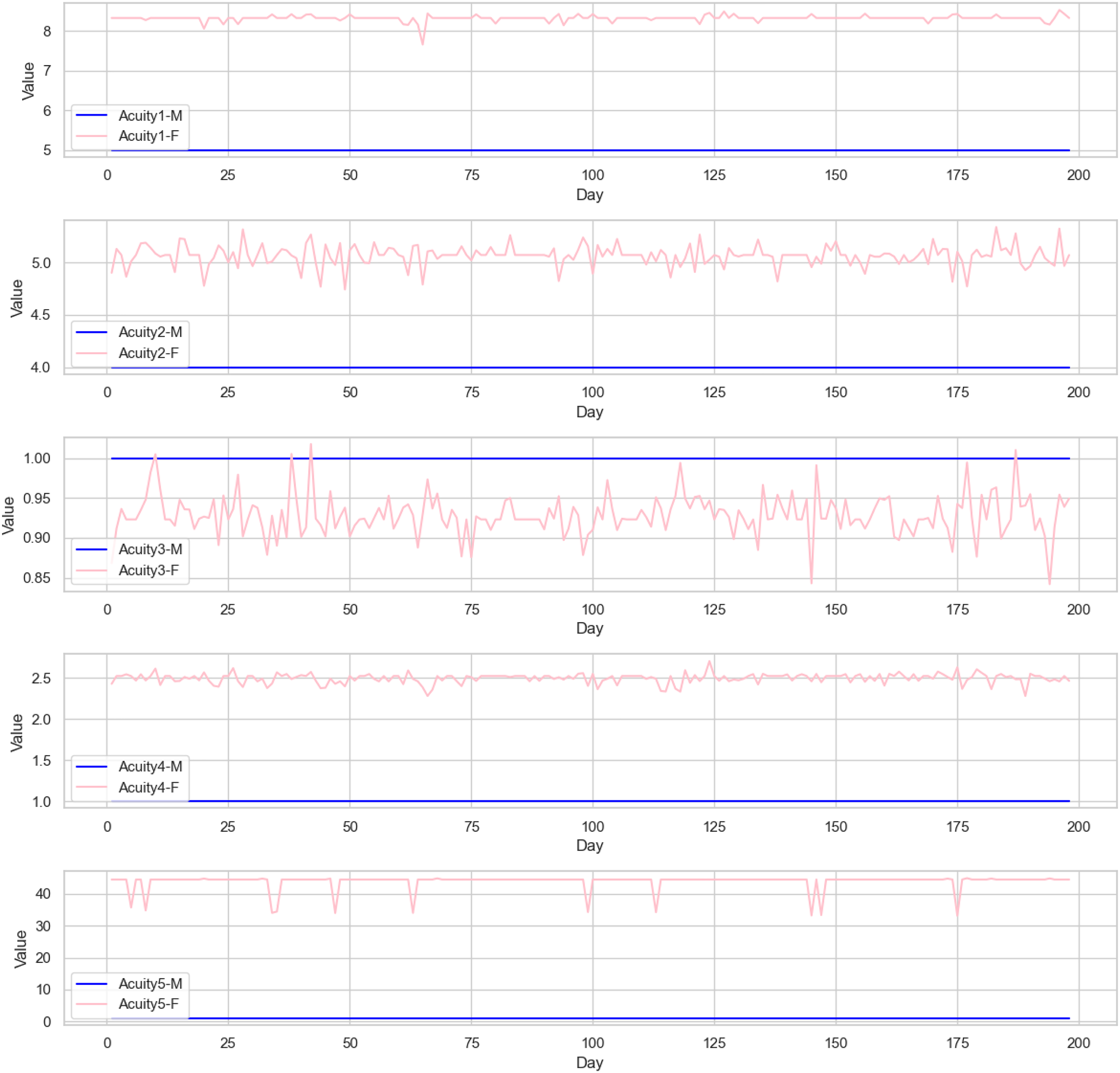
Weights for female (pink) and male (blue) patients for Emergency Severity Index (ESI) acuity levels 1-5 across time, test set.
Arrival-to-room times (in minutes) realized by the hospital and the algorithm by gender and acuity level for the large dataset.
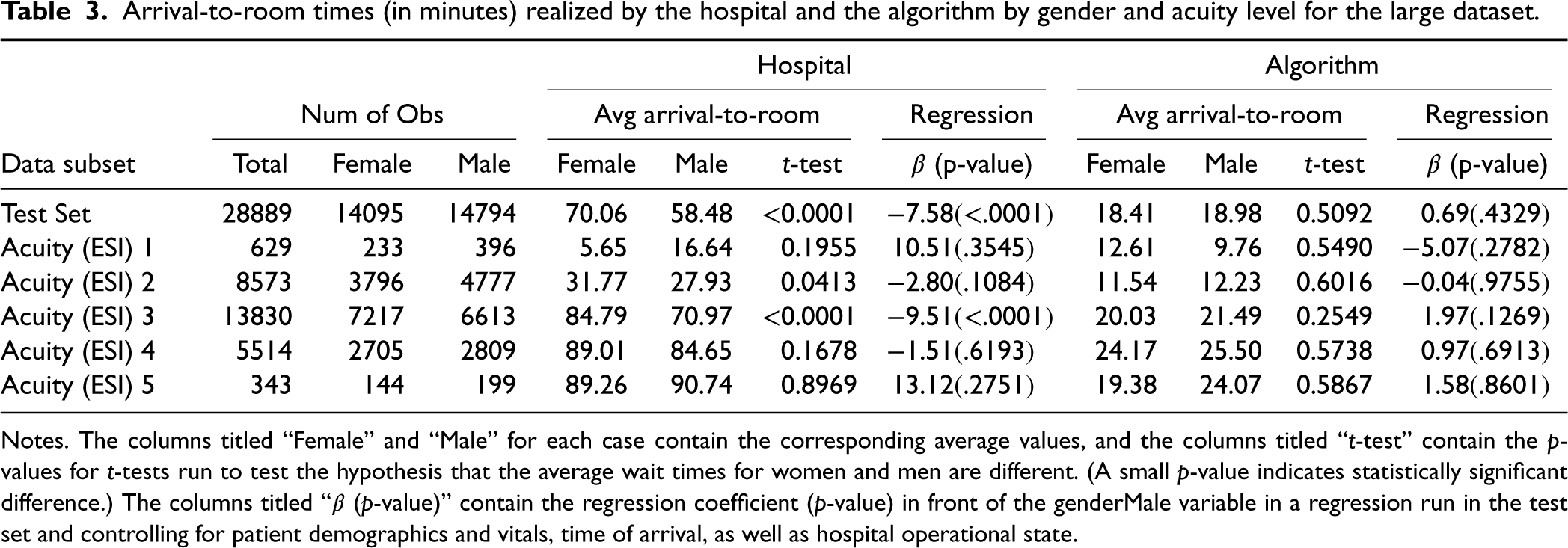
Notes. The columns titled “Female” and “Male” for each case contain the corresponding average values, and the columns titled “
In this section, we compare the allocations recommended by our method (formulation (7) with objective function (11) and weights (6)) with the actual allocation performed by the ED with which we collaborated.
Wait Time Discrepancy Correction
There are
There are statistically significant differences between average female and male patient wait times at the hospital (
Wait times by gender and method (algorithm vs. hospital practice), test set.
We analyze the nature of the allocations made by our algorithm and their consistency with medical practice. Prioritization across Acuity Levels and NHAMCS Diagnoses. Figure 3 shows the average wait times realized for patients of ESI Acuity levels
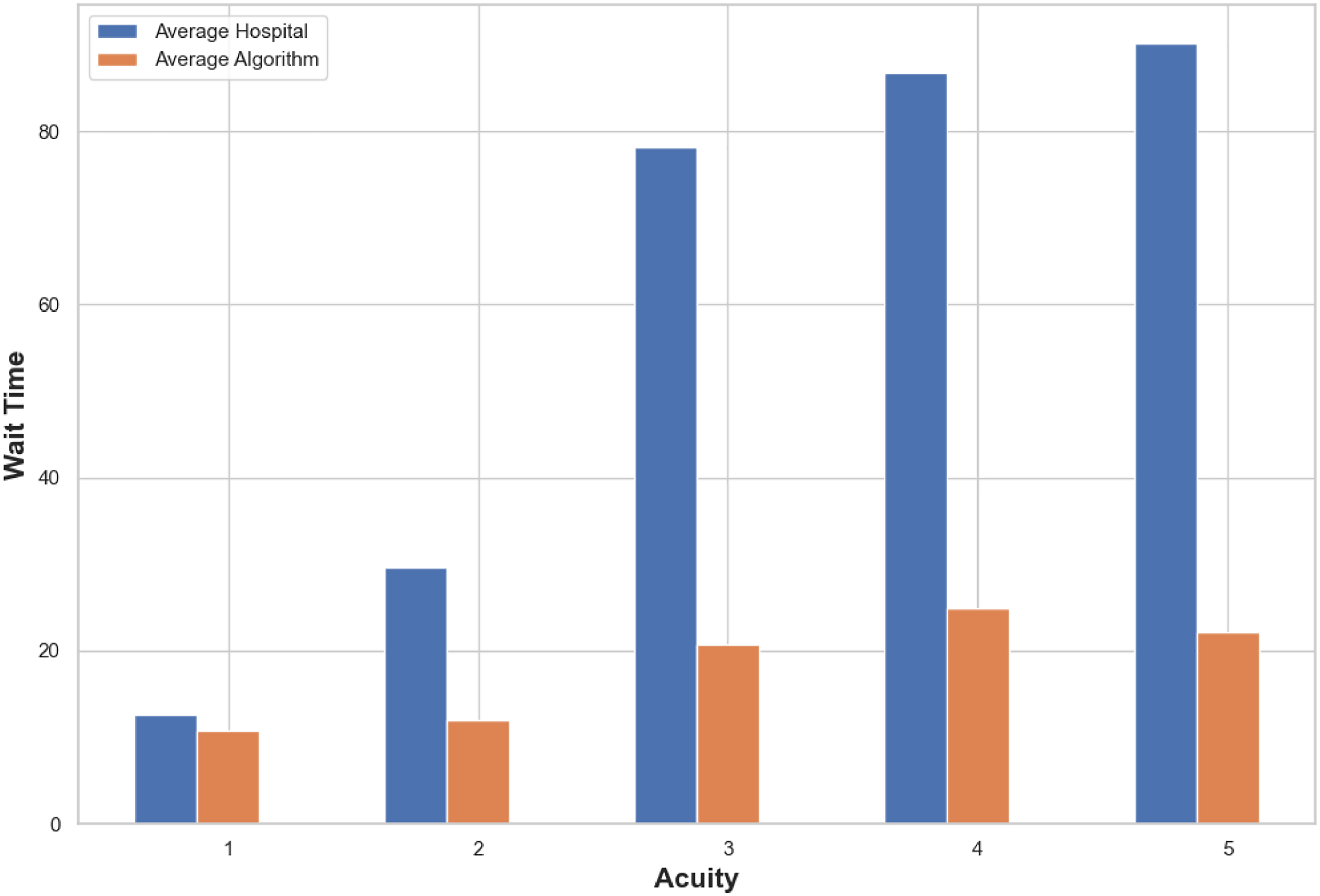
Average wait times (in minutes) realized for each acuity level based on our algorithm’s recommendations (in orange) compared to the hospital (in blue).
Our algorithm also preserves the prioritization of patients within NHAMCS categories (CDC 2022) while substantially reducing average wait times across all NHAMCS categories (Figure 4).
Sample Path Analysis
To gain deeper insights into the allocation decisions, in Section EC.6 we present three actual scenarios when bed utilization is lowest, median, and highest (Tables EC.6, EC.7 and EC.8, respectively), and summarize the actions of the hospital and the algorithm for the first ten patients on the corresponding day in more detail. The main insight from the scenario analysis is that our algorithm expedites bed allocation substantially; however, it is sometimes difficult to account for human factors that may cause the actual delays. The example of Patient 1 (ESI-4, 45, M, general symptoms—leg swelling) on the lowest bed utilization day from Table EC.6 is informative. Patient 1 had to wait for an hour, despite the availability of
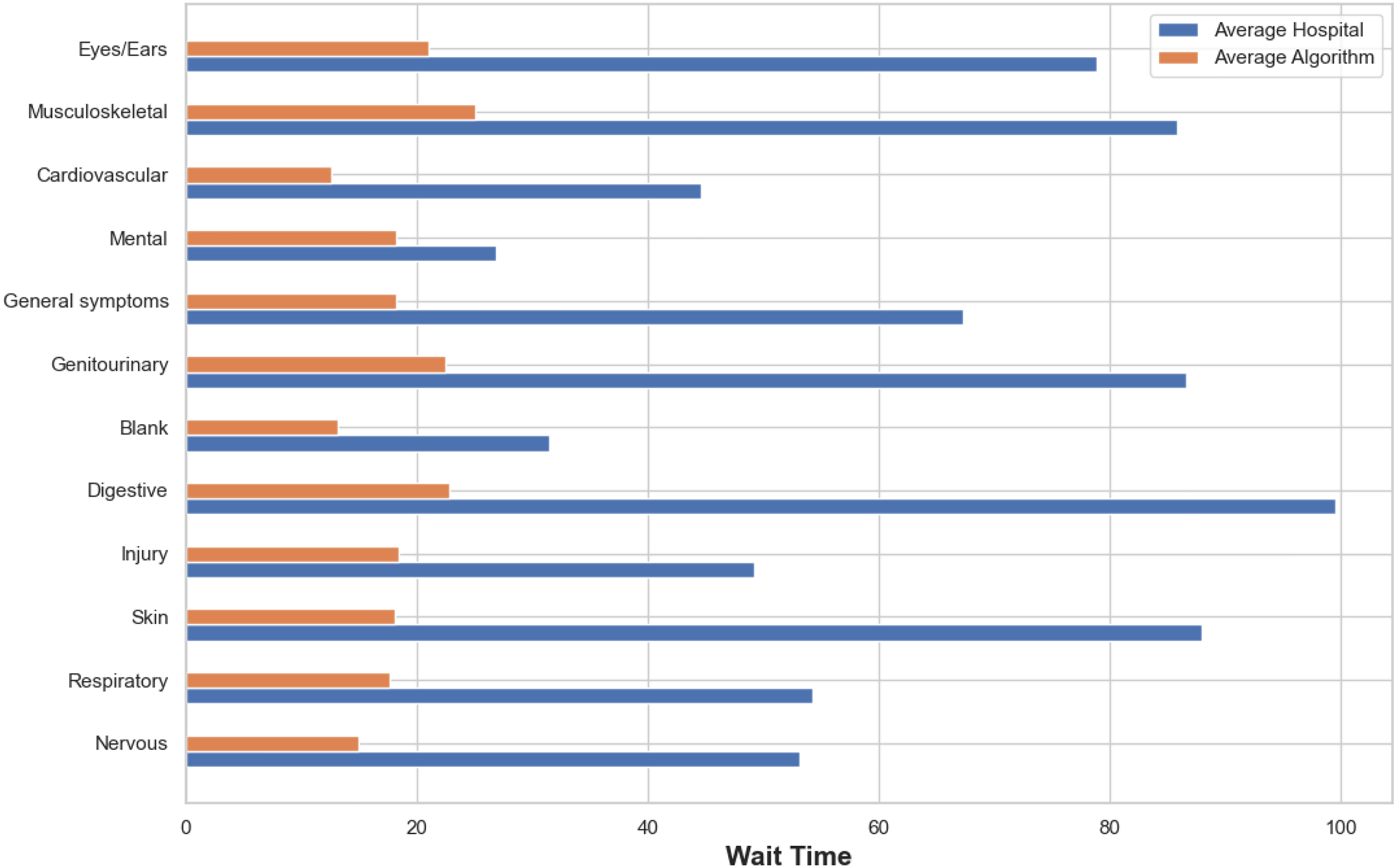
Average wait times (in minutes) realized for each National Hospital Ambulatory Medical Care Survey (NHAMCS) based on our algorithm’s recommendations (in orange) compared to the hospital (in blue).
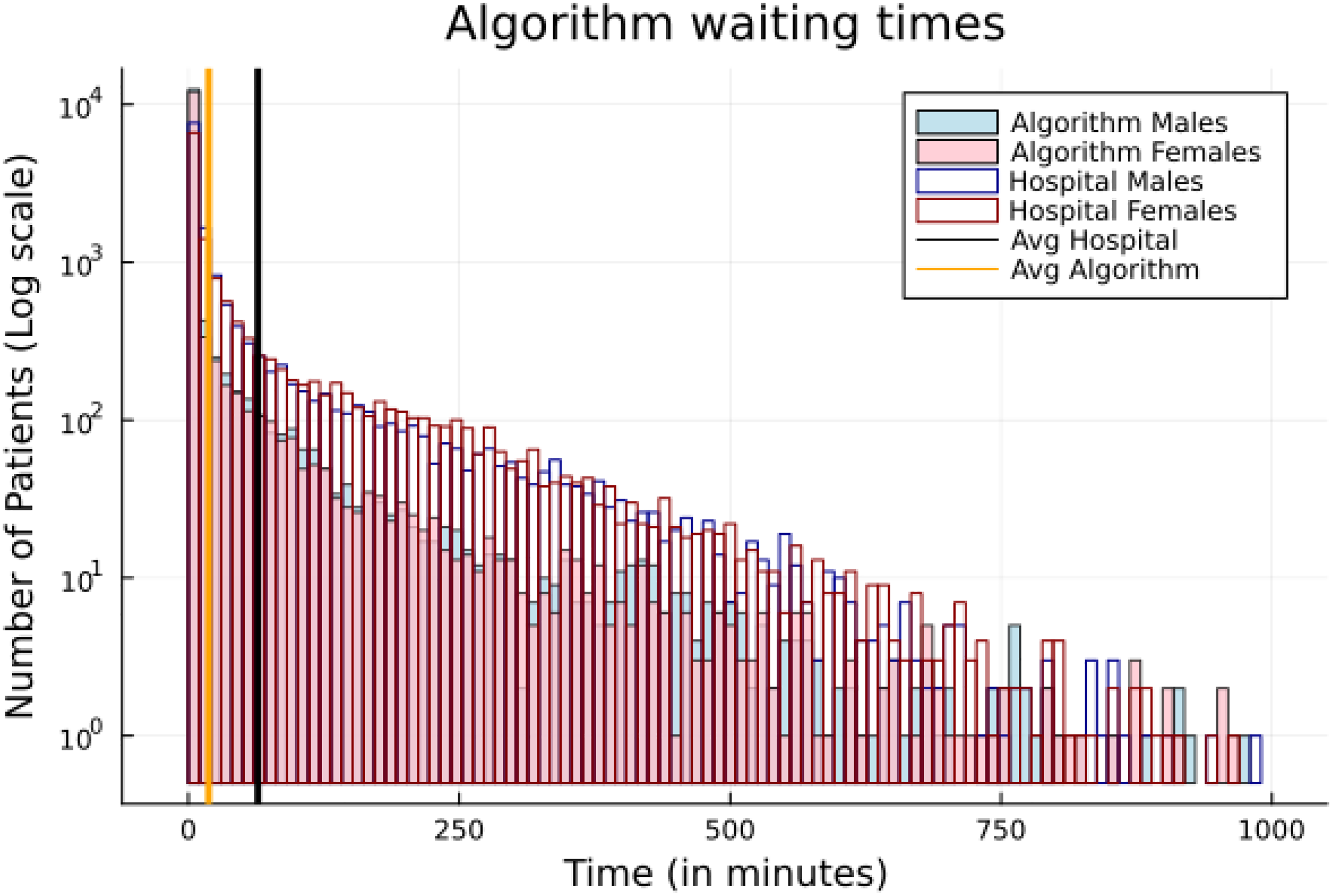
Overall, our algorithm reduced wait times by an average of
ESI-5 Patient Prioritization
ESI-5 patients wait much longer than other patients (see Figure 3), sometimes even exceeding 4 hours. There is a logical reason for this: they are prioritized last given their stable condition. This is confirmed also by our detailed scenario analysis summarized in Sections EC.6-EC.7. However, it is also evident that human factors may be contributing to some of the delays in allocating ESI-5 patients, because the delays often happen even when the ED is not busy. Anecdotally, there is deprioritization and even avoidance of ESI-5 patients who are in the ED for prescription refills and other tasks that should not be performed in the ED. In addition, ED physicians need to catch up on paperwork and do not have designated meal breaks. They cannot do it when there are truly urgent patients waiting but may do it while low-severity patients are waiting, extending the wait times for those patients. In contrast, our algorithm schedules such patients more quickly.
At each point in time, the ED may face practical constraints that are not visible in the data. For example, because the ED with which we collaborated has a trauma, stroke, and heart attack center, there are sometimes delays with non-trauma patient placement when the police are called in. Although there is additional nursing staff specifically dedicated to trauma patients, sometimes nursing staff from the ED gets pulled to respond to particularly difficult cases.
In addition, there is often “bed hoarding”, where the utilization staff always reserves at least some beds for “true” emergencies, so the full number of available beds is never used, effectively reducing the capacity of the ED during normal operations.
Finally, there are operational considerations, such as the need to clean ED beds after a patient leaves as well as compliance with regulations that an ED nurse should not handle more than approximately
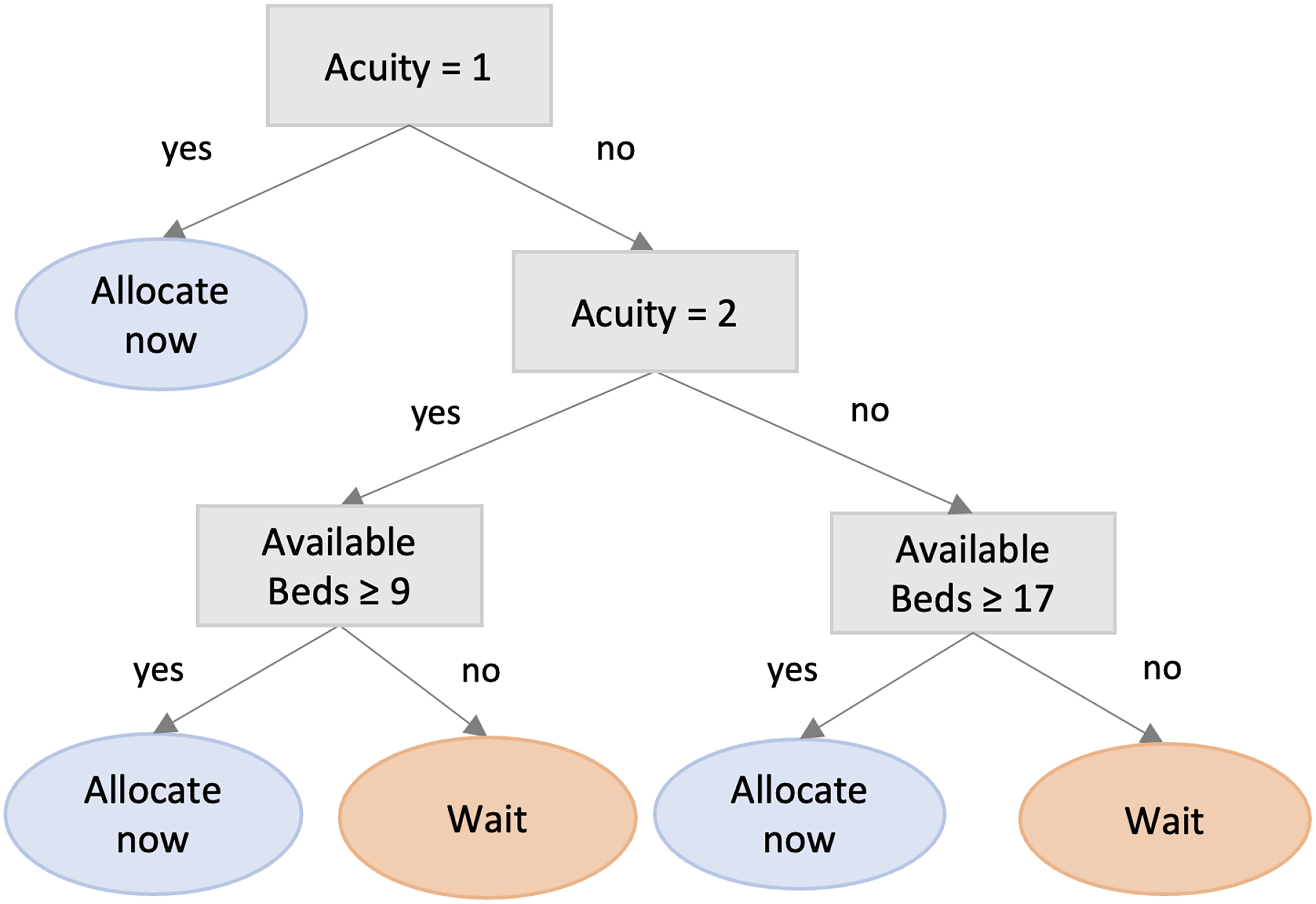
Interpretable decision tree metamodel of our algorithm’s recommendations.
We stress-tested our algorithm against these constraints. First, we reran the algorithm under the assumption of some bed hoarding, i.e., when the number of beds in the ED is 3 fewer than the available beds at every point in time. Under this scenario, our algorithm still exhibited a substantial improvement over current hospital placement policies. We also tested the performance of the algorithm assuming that the number of available beds is
To operationalize our algorithm, it would have to be executed every time a patient arrives in the ED. The algorithm’s operation involves predicting the patient’s expected LOS and then simulating multiple scenarios considering multiple future patient arrivals. Based on these scenarios and the availability of ED beds at the moment, the algorithm would decide whether the patient should be allocated directly or wait for the next time period to be considered again. (Those decisions are denoted
To understand how our predictive-prescriptive algorithm affects the actual processes in the ED at a more granular level, we developed an interpretable metamodel that finds rules consistent with the algorithm’s recommendations. After applying the original predictive-prescriptive algorithm, we have not only the test (
Based on the decision tree metamodel, the optimal ED allocation policy is as follows: If an incoming patient is ESI-1, the patient gets allocated immediately. If the patient is ESI-2 and there are at least
The metamodel in Figure 5 is closely aligned with our predictive-prescriptive algorithm: Its fidelity (i.e., the percentage of times its recommendations agree with the recommendations of our algorithm) is
The operationalization of such metamodels in practice can be very beneficial. For example, in Section 4.2.3 we mentioned anecdotally the issue of “bed hoarding” in EDs, which is a source of many inefficiencies, and has been reported also in the literature (McLarty and Jeffers, 2008). Metamodels such as the ones suggested in this section are consistent with the inherent human inclination to save resources for “true emergencies,” but they can provide ED staff with realistic estimates of the number of necessary beds to “hoard” to have sufficient capacity for incoming patients given a particular ED’s historical patient arrival trends.
Concluding Remarks
This work addressed the problem of prolonged ED LOS by proposing a novel approach for improving the patient prioritization and placement aspect of ED operations that also contains mechanisms for outcome and process fairness. In particular, we presented a novel MILP predictive-prescriptive formulation that incorporates a breakdown of predicted patient ED LOS into actionable pieces and allows for a more granular model of ED operations. We also suggested a de-biasing scheme for patient allocation through the selection of weights in the objective function. We developed our approach in collaboration with a large US AMC and used real data from more than
Supplemental Material
sj-pdf-1-pao-10.1177_10591478241240390 - Supplemental material for A Granular Approach to Optimal and Fair Patient Placement in Hospital Emergency Departments
Supplemental material, sj-pdf-1-pao-10.1177_10591478241240390 for A Granular Approach to Optimal and Fair Patient Placement in Hospital Emergency Departments by Maureen M Canellas, Dessislava A Pachamanova, Georgia Perakis, Omar Skali Lami and Asterios Tsiourvas in Production and Operations Management
Footnotes
Acknowledgements
The authors would like to thank the dedicated staff at the hospital with which we collaborated. The authors are also very grateful to the Special Issue Editors, Professors Charles Corbett and Sriram Narayanan, the Senior Editor, and two anonymous referees, for their thoughtful comments and constructive suggestions on previous versions of this manuscript. GP, DP and AT gratefully acknowledge support from the MIT Sloan Health Systems Initiative.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GP, DP and AT gratefully acknowledge financial support for this project from the MIT Sloan Health Systems Initiative.
How to cite this article
Canellas MM, Pachamanova DA, Perakis G, Lami OS and Tsiourvas A (2024) A Granular Approach to Optimal and Fair Patient Placement in Hospital Emergency Departments. Production and Operations Management 34(4): 574–588.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.