
Abstract
The COVID-19 pandemic placed unprecedented strain on healthcare professionals around the globe, particularly those working in intensive care units. It was reported that instances of moral injury – a betrayal of what is ethically right by those in positions of power – were widespread in these organizational settings. In this paper, we explore these emerging findings to ask: What are the experiences and implications of moral injury in critical care nursing during the pandemic? Drawing on 103 interviews with 54 critical care nurses, we offer insights into the experience of moral injury in a workplace experiencing crisis, focusing on (i) unsafe staffing levels, (ii) inadequate equipment, and (iii) inability to provide patients with a dignified death. We provide accounts of the implications of moral injury ranging from debilitating anxiety to post-traumatic stress disorder and sectioning, as well as widespread feelings of anger and guilt leading to an intention to leave the profession.
I mean we’re all broken, we’re all beyond broken. There's not a staff member that isn’t. (Critical Care Nurse (CCN) 14)
The COVID-19 pandemic has left indelible marks on us all – psychological and physiological scars that run deep, some that might never heal. For those working on the frontline, particularly in healthcare, life has been especially challenging (Maben & Bridges, 2020). Witnessing suffering during crisis in an organizational setting can be a traumatic experience (Powley, 2009), and we all owe a massive debt to those that, when called to do so, ran ‘towards the bullets’ and risked not only their own lives but their psychological well-being so that those infected with the virus might have a better chance at survival. During this period, the pandemic has put unprecedented strain on healthcare professionals around the globe (WHO, 2020) – in particular, in intensive care units (ICUs), where the very sickest patients were sedated, intubated, and often ventilated as doctors and nurses fought to wrestle each individual from the grip of a deadly virus with a high mortality rate, no known cure, and no known reliable course of treatment (Harris et al., 2021).
The working environment in an ICU ward was made especially challenging due to a variety of factors, including a lack of adequate personal protection equipment (PPE), a shortage of medicines, the reduction of the staff-to-patient ratio from 1:1 to as low as 1:6, and the subsequent need to redeploy staff from other parts of the hospital often with no experience of ICU care (Arnetz et al., 2020). Patients died without loved ones at their bedsides, and nurses struggled to communicate in restrictive PPE and toiled for 12-h shifts in unbearable heat, fearing infection as hospitals were ravaged by a surging virus. In these circumstances, it was often impossible to deliver a normal standard of care, and ICU nurses were faced with the overwhelming responsibilities of care but often without the time, resources, or skill mix to do so in a way that felt adequate or safe (Crowe et al., 2021).
The toll on ICU staff was extensive. A 2021 survey in the UK found ‘substantial rates of probable mental health disorders, and thoughts of self-harm, amongst ICU staff’ with ‘nearly one in five nurses … working in ICU report[ing] thoughts of self-harm or suicide’ (Greenberg et al., 2021, p. 1). It was also found that ‘these difficulties were especially prevalent in nurses’ (Greenberg et al., 2021), and for reasons yet unknown, they were substantially more likely to suffer (than doctors or other health workers) from serious mental health problems during the pandemic. Indeed, high levels of anxiety, depression, and post-traumatic stress disorder (PTSD) in nurses on the frontline have also been found within similar studies in China (Pan et al., 2021), Italy (Di Tella et al., 2021), France (Caillet et al., 2020), Turkey (Şanlıtürk, 2021), and Canada (Crowe et al., 2021). Efforts are now underway to understand the deleterious psychological effects on ICU nurses, starting with the root cause but extending to the implications and the potential ways of helping nurses both now and in the future (Williamson et al., 2020).
One way of understanding ICU nurses’ experiences is through the concept of moral injury. Originally used within clinical psychiatry to understand the experience of war veterans (Shay, 1995), moral injury is described by Williamson et al. (2021, p. 453) as ‘the strong cognitive and emotional response that can occur following events that violate a person’s moral or ethical code’ that occurs due to ‘a betrayal by a trusted person in a high-stakes situation’. It leaves ‘a deep emotional wound’ (Čartolovni et al., 2021, p. 590) that can profoundly affect an individual. Concerns about moral injury in ICU nursing during the pandemic have been highlighted in the media (Alexander, 2021), professional bodies (RCN, 2021), and academic commentaries (Borges et al., 2020) as an urgent emerging problem requiring investigation. A lack of PPE, low staffing levels, and poor planning by those in positions of power are all potential sources of moral injury. And yet, very little is known about how nurses have made sense of experiences associated with moral injury in an organizational setting or how they have attempted to work towards moral repair (Goodstein et al., 2016). Indeed, there are ‘limited empirical studies on moral injury’, including in the area of healthcare, meaning that now is a ‘timely moment to speak about moral injury amongst healthcare professionals’ (Čartolovni et al., 2021, p. 590).
With this in mind, and building upon the recent introduction of moral injury to organizational studies in this journal (Kalkman & Molendijk, 2021), we ask: What are the experiences and implications of moral injury in critical care nursing during the pandemic? In our paper, we argue that the cumulative and repetitive nature of moral injury over this period has been devastating for critical care nurses (CCNs). To show this, we reflect upon how they made sense of their experiences during the pandemic, including their assessment of general levels of support and how this challenged their own internalized standards of professional ideals and values. To do so, we adopt a ‘writing differently’ approach within our work, endorsing the claim that too often ‘scientific writing excises much of what it is to be human’ (Gilmore et al., 2019, p. 4), sacrificing a deeper understanding of issues on the altar of feigned disinterestedness and objectivity. We, instead, embrace an emotional writing style that invites the reader into the world of critical care nursing, exploring experiences of intense suffering in an organizational context without foregoing the centrality of academic rigour.
Our article has three core theoretical and corresponding practical contributions. First, we provide a novel insight into the repetitive and cumulative nature of moral injury in an extreme, underexplored organizational setting, the ICU. We do so by providing a voice to an essential but largely unheard (and in some cases, silenced) group of workers during the pandemic: ICU nurses – amplifying their experiences of cumulative moral injury in an organizational context, focusing on the emotional and psychological consequences in the workplace. In doing so, we respond to calls within this journal to speak out against social injustices that the pandemic has brought into focus, telling the stories of an overworked and underpaid profession within the modern workforce (Peredo et al., 2022).
Second, we highlight the tendency to individualize responses to moral injury by pushing the burden of moral repair back on to workers, here the ICU nurses. In doing so, we emphasize the collective and intersubjective dimensions of moral injury and the need to take these more seriously to address them in the workplace. Finally, our exploration of nurses’ experiences in the ICU reveals the centrality of power relations to the concept of moral injury and shows how essential it is for institutions to take a systemic approach to tackling moral injury. That is, they must also consider both political and structural dimensions if they are going to minimize occurrences of moral injury in the workplace and collectively help workers to repair and recover from it over time.
In the remainder of the article, we first discuss the context of ICU nursing and explore how moral injury is a productive theoretical frame to understand their experiences. We then outline the methodological approach, focusing on 103 interviews with 54 CCNs over a 12-month period at the height of the pandemic in the UK. We then present our findings, focusing on experiences, implications, coping mechanisms, and required action for reducing moral injury, and then discuss the broader relevance of these. Finally, we conclude by suggesting that the experiences of CCNs must be listened to and learnt from by senior healthcare managers and government officials if we are to avoid the horrors of moral injury and its implications in the future.
In 2009, approximately 30 million people were treated worldwide within ICUs (Vincent et al., 2009). Despite this, public knowledge of what goes on within an ICU ward is still limited (García-Labattut, 2006), and as a workplace, it remains somewhat shrouded in mystery. According to Adam and Osborne (2001, p. 1), the purpose of the ICU is to ‘to provide care for severely ill patients with potentially reversible conditions’ usually ‘with potential or established organ failure’ with the intention of ‘reduc[ing] avoidable mortality in critically ill patients’. The ICU nurse – and the principle of one-to-one patient care – is central to ICU provision. Indeed, for the patient and their families, the ICU nurse is their primary contact, providing a depth and duration of interaction that far exceeds that of many other occupations attending ICU. ICU nursing involves not only high levels of skill development, qualifications, and enhancement (Leiter et al., 1994), which has contributed to its increasing professionalization (McMurray, 2011), but also an emotional component of communicating with dying patients and supporting scared and often grieving families. The need to make complex decisions and choices within ambiguous care scenarios around holding or withdrawing treatment and securing a ‘good’ death for their patient when required places a huge burden on these nurses (Hoy et al., 2007).
The ICU can, as a result, be an extremely stressful working environment. The emotional and psychological strain of being an ICU nurse requires of them constant self-regulation (Hayward & Tuckey, 2011) and resilience (Powley, 2009). The regularity and close proximity of grief and a range of intense emotional experiences have been shown to lead to compassion fatigue and nurses wanting to leave the profession (Dashtipour et al., 2021). Not surprisingly, studies have found that a significant number of CCNs experience severe burnout, including the main symptoms of exhaustion, depersonalization, and reduced personal accomplishment (Moss et al., 2016). It is an extremely difficult profession, and the ICU nurse is susceptible to a range of negative outcomes – a speciality in which nurses have a high degree of commitment but in which psychological and emotional pressures were already at extremely high levels leading to calls for action within the critical care community (Poncet et al., 2007).
And then, in March 2020, the pandemic arrived.
As COVID-19 cases rose in the initial months of the pandemic, the UK was considered especially vulnerable. The country possessed a low number of critical care beds relative to its population, ‘with just 7.3 critical care beds per 100,000 people, more than half the average in OECD EU nations’, compared to 29.2 beds per 100,000 in Germany (BMA, 2022). The immediate reaction was to postpone non-urgent planned operations, increase the number of beds in ICU (often through expansion into areas conventionally used for other purposes), and redeploy staff from elsewhere in the National Health Service (NHS) to boost staff numbers.
Despite these measures, numerous studies point towards problems within hospitals during this period. In a survey of frontline doctors, Harris et al. (2021, p. 6) highlight an ‘overwhelmed system’ reflected by the reduced nurse-to-patient ratio in which medics felt like ‘cannon fodder … exposed and unprotected’ not least by a lack of PPE. Meanwhile, one Canadian survey of ICU nurses in the pandemic highlighted a fear of ‘staying safe’ within the hospital (Crowe et al., 2021, p. 7) due to worries of contracting the virus and passing it to family. Finally, a Turkish survey of ICU nurses identified ‘high working hours … and failure in patient treatment’ leading to abnormally high death rates as additionally difficult for staff in trying to adjust in the first year of the pandemic (Şanlıtürk, 2021, p. 1).
The psychological implications on ICU nurses were significant. Multiple studies conducted during the pandemic have reflected this. One UK survey of 709 staff in ICU suggests that ‘45% [of surveyed staff] met the threshold for probable clinical significance on at least one of the following measures: severe depression (6%), PTSD (40%), severe anxiety (11%), or problem drinking (7%)’. They go on to add that ‘more than one in seven clinicians (and nearly one in five nurses) in our sample working in ICU reported thoughts of self-harm or suicide [which] is also highly concerning’ (Greenberg et al., 2021, p. 4). This has been supported by surveys conducted in other health systems, which show, for example, that 14% of healthcare workers in a study conducted in Wuhan, China, were suffering from PTSD (Pan et al., 2021); ICU nurses in Italy were showing signs of post-traumatic stress (Di Tella et al., 2021); and in French ICUs, ‘the incidence of anxiety and depression were 48% and 16%, respectively … [with] … PTSD symptoms … present in 27% of respondents’ (Caillet et al., 2020).
The current state of psychological distress in ICUs has led to calls by World Health Organization (WHO) (2022) and others (Greenberg & Tracy, 2020) to provide a deeper and more layered understanding of ICU nurses’ experiences during the pandemic in order to protect them in the future. At present, however, whilst multiple quantitative surveys exist, there is a lack of a deeper qualitative and longitudinal understanding of the experiences of ICU nurses over this period. It is important, we argue, to try to explore more deeply the ways that their expectations about care have been challenged in the workplace and the consequences of doing so.
Moral Injury: The Theoretical Frame
Conventionally, there are a variety of organizational approaches that could explore the psychological experiences of nurses during a time of crisis, encountering the competing demands of their organization and their own values and ethical beliefs. We might focus, for instance, on breaches of trust (Sama & Shoaf, 2008) or of the psychological contract (Zacher & Rudolph, 2021). Alternatively, we might try to capture the deleterious effect on stress and well-being of staff in morally taxing situations (Guest, 2017), including implications of psychological injury (De Rond & Lok, 2016) or of resistance and deviance that staff might engage in to push back against the imposition of what they feel is wrong or unsound (Pelly, 2017). Whilst accepting the benefits of potential studies through these perspectives, we believe that another much less explored concept in organizational studies can offer more in this context. A concept that captures not only the moral and ethical component of the organizational situation but also the affective internal experience of the worker: moral injury.
Moral injury involves a ‘deep emotional wound and is unique to those who bear witness to intense human suffering and cruelty’ (Čartolovni et al., 2021, p. 590). It involves experiencing what Litz et al. (2009, p. 700) call a potentially morally injurious event (PMIE), that is, ‘perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations’. Importantly, according to Shay (2014, p. 182), moral injury is felt as ‘a betrayal of what's right, by someone who holds legitimate authority … in a high-stakes situation’. All three components must be present. Originally, and until quite recently, moral injury was used to explain the lingering psychological injuries suffered by military personnel (Richardson et al., 2020; Shay, 1995), such as being sent into warzones without adequate weaponry or support. Over the past few years, however, moral injury has been applied to a wider range of professions, including police officers (Komarovskaya et al., 2011) and child protection officers (Haight et al., 2017).
More recently, in this journal, moral injury was introduced to the organizational studies literature for the first time (Kalkman & Molendijk, 2021, p. 221), exploring how border guards as ‘lower level organizational members face moral challenges because their personal values conflict with organizational directions’. The authors suggest that strategic ambiguity within an organization (encouraged by senior leaders) can contribute to the experiences of moral injury, particularly for those who are more vulnerable (not in leadership positions) within an organization. Carucci and Praslova (2022) meanwhile suggest that the experience of moral injury – being asked to make moral decisions within jobs that contravene deeply held values and beliefs – might be a more acute reason for employee distress and resignation than burnout and other commonly used concepts in organizational studies. As they argue, drawing directly on the concept of moral injury, ‘the mass exodus from our workplaces is, in part, a proclamation that people can’t – and won’t – tolerate mistreatment, injustice, and incompetence from their leaders anymore, particularly at the expense of their dignity and values’ (Carucci & Praslova, 2022).
We know from previous studies on health professionals that an increase in moral injury is linked directly to an increase in serious mental health problems ranging from depression (Nash et al., 2013) to PTSD (Gibbons et al., 2013), although it is distinct from the latter insofar as its deeper engagement with our moral and ethical core. In a recent systematic review, Williamson et al. (2021, p. 453) found that moral injury leads to ‘profound feelings of shame and guilt, and alterations in cognitions and beliefs (e.g. “I am a failure”, “colleagues don’t care about me”), as well as maladaptive coping responses (e.g. substance misuse, social withdrawal, or self-destructive acts)’. The experience of moral injury in healthcare settings has also been linked to suicidal thoughts that ‘include social withdrawal, self-depreciating emotions, and a loss of meaning’ (Williamson et al., 2018, p. 344). Other studies show feelings of alienation by healthcare workers following experiences of moral injury in the workplace (Gibbons et al., 2013) and even of physical pain (Koenig et al., 2018).
There have been indications during the pandemic that healthcare workers might have been suffering from moral injury. In the USA, Mantri et al. (2021) show through a large survey of health professionals that moral injury was prevalent within the workforce, particularly for those who had direct experience of caring for COVID-19 patients. In addition to this, Borges et al. (2020) and Williamson et al. (2020, p. 318) both wrote short commentaries with the latter warning of the dangers of an ‘exposure to traumatic events’ warning of an ‘increased risk of moral injury if staff feel unaware or unprepared for emotional/psychological consequences of decisions’, especially ‘if leaders are perceived to not take responsibility for the event(s) and are unsupportive of staff’. In a US survey of healthcare workers during the pandemic, Litam and Balkin (2021, p. 3) also found a link between the experience of moral injury and negative outcomes such as ‘difficulty sleeping, feeling on edge, and avoidance of activities that remind healthcare workers of frightening experiences of their patients’.
There have, nevertheless, been a limited number of qualitative studies into moral injury of NHS staff during the pandemic. In their study, French et al. (2021) found that ‘abandonment as betrayal … dishonesty and lack of accountability … and fractured relationship to management or the NHS’ were all central experiences for staff during this period. The 16 staff from across the NHS that were interviewed ‘voiced feelings that their death would be meaningless to the leadership … and that … [n]ot only had leaders failed to live up to the trust placed in them, they had failed to place well-earned trust in their employees by not acknowledging the reality of the situation’ (French et al., 2021, p. 517, 520). The study, whilst limited in size, duration, and focus on ICU nurses, calls for greater moral repair – attempting to heal the emotional wounds of the pandemic – whilst also asking for greater accountability. It is upon this work that we wish to build, providing a deeper understanding of ICU nurses’ experiences on the frontline during the pandemic.
It is increasingly recognized that the concept of moral injury has relevance to healthcare and a ‘multidisciplinary appeal’ (Griffin et al., 2019, p. 350) that can integrate perspectives from healthcare to psychology and sociology (see also Molendijk et al., 2022). Yet it is also understood that it is thus far underresearched as an emerging concept (Williamson et al., 2018, p. 345). Until very recently, organizational scholars, in particular, have failed to engage with this term to understand its relevance to people within their working lives. Instead, there has been a tendency either to rely upon legalistic approaches to understanding the breaches of expectations in the workplace or to portray these situations as failures of a leader–follower relationship. Whilst these concepts have been productive elsewhere, we argue that the concept of moral injury can help retrain a focus on the lived experience of the ethically and morally transgressed, helping us as organizational scholars to see and understand the emotional wounds of those that work in difficult circumstances.
We argue that it is important, therefore, to focus on exploring these issues of moral injury with a wider disciplinary lens but with a qualitative focus on ICU nurses in order to understand the experiences and the implications of moral injury in depth. Consequently, this leads us to ask within our study: What are the experiences and implications of moral injury in critical care nursing during the pandemic? It is to answer this question that we now turn.
Methodology
Data Collection
Early in the pandemic, the research team decided to conduct longitudinal semi-structured interviews to gain insight into the experiences of CCNs (Hermanowicz, 2013). After a recruitment campaign with the support of the British Association of Critical Care Nurses (BACCN), we recruited 54 CCNs who worked in ICU prior to and during the pandemic. All recruits were band five or six nurses (i.e. not in management roles), reflecting our intention to focus primarily on the experiences of those at the coalface during the pandemic. This purposive selection strategy was not to ignore or downplay the complex difficulties that faced leaders within the NHS throughout the pandemic; they indeed have their own story to tell. With a focus on moral injury, though, this study chose to concentrate on non-managerial staff and the experiences that they faced on the frontline during this period.
The experience of the nurses ranged from just under 2 years to over 30 years, and all but two of the participants worked in ICU wards in UK hospitals (the other two worked in Ireland). There were 38 different hospitals/ICU wards represented within the study, providing geographical diversity. In terms of gender, whilst NMC (2023) reports that 11% of nurses are male, only three participants were male representing approximately 6% of the participants. Likewise, in relation to ethnicity, there was a lack of representation as it proved difficult to recruit from minority groups, and here again, the sample was unrepresentative as only one ethnic minority CCN was interviewed. The recruitment of ethnic minorities has been identified as a wider problem for studies of this kind (Brown et al., 2014).
There were three rounds of interviews in September/October 2020, January/February 2021, and May/June 2021. The value of interviewing over time was allowing us to ‘capture critical moments of change and transitions’, enabling participants to describe how feelings and situations changed during a highly disruptive and fluid time in their working lives (Vogl et al., 2018, p. 178). There was an expected attrition in nurses from phase one (54 nurses) to phase three (24) due to the emotional and difficult nature of the interviews and the complexities of timetabling meetings with exhausted nurses. A total of 103 interviews were ultimately conducted. These lasted on average 75 min in phase one (where we asked 54 nurses more broadly about ICU nursing and experiences during the pandemic), 55 min in phase 2 (reinterviewing 29 nurses), and 30 min in phase 3 (follow-up interviews with 24 nurses).
Whilst there was an interview guide (decided deliberatively by the research team in between phases), the overall intention of the interviews was to enable the CCNs to voice whatever issues they were facing in ICUs during the pandemic. Many of the interviews, conducted by all members of the research team, were emotional for both participants and interviewers. We met weekly to debrief from what were (at times) disturbing and uncomfortable interviews that stayed with many of us long after they had ended. Given the subject matter, interviews unintentionally but somewhat unavoidably took on a therapeutic component, with nurses able to offload experiences and memories to interviewers (Birch & Miller, 2000). This had unintended consequences on the interviewers who used their debrief sessions to vocalize their own emotional reactions to stories that they heard. Free counselling sessions were offered to the nurses participating through a trained psychotherapist who was also part of the wider research team, with a number of them taking up this opportunity in between phases and after the study had been completed.
Data Analysis
We sought to avoid an overtly ‘mechanistic’ analysis of the data, seeking instead a more organic approach in which we sought to bring the voices and stories of the CCNs to life. That is, to embrace an analytical approach that enabled us to amplify the voices of the nurses to explore the experience of moral injury by this group of people in the pandemic. The interviews were transcribed by a professional transcription service and analysed through NVivo. Inspired by the principle of developing analytic themes from template analysis (King, 2012), the data were coded following Locke et al.'s (2020) ‘delimiting the field’ approach. In what was a highly iterative and team approach to coding (Giesen & Roeser, 2020), we began with the calls from multiple sources that moral injury is a problem requiring urgent investigation in critical care organizational settings (Alexander, 2021; Borges et al., 2020; RCN, 2021). We therefore used the existing literature on moral injury to discuss and produce four template questions to answer whilst analysing the data (which are displayed in Figures 1 to 3). Following Pratt (2009), Figures 1 to 3 also include ‘proof quotes’ not included in the main analysis to show the depth and generalizability of the data whilst clearly indicating how we reached our codes and categories of analysis.
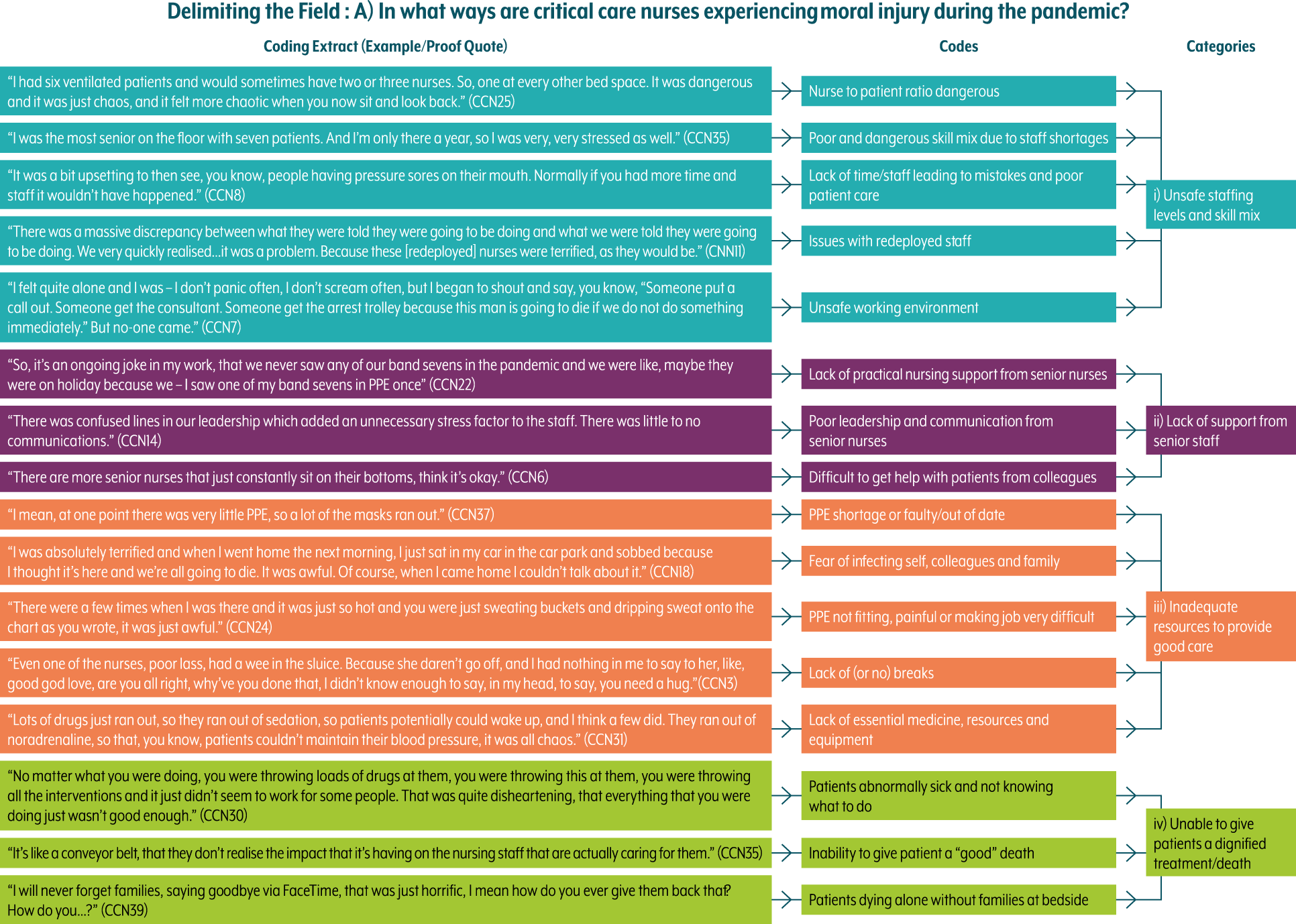
Coding architecture (experiences).
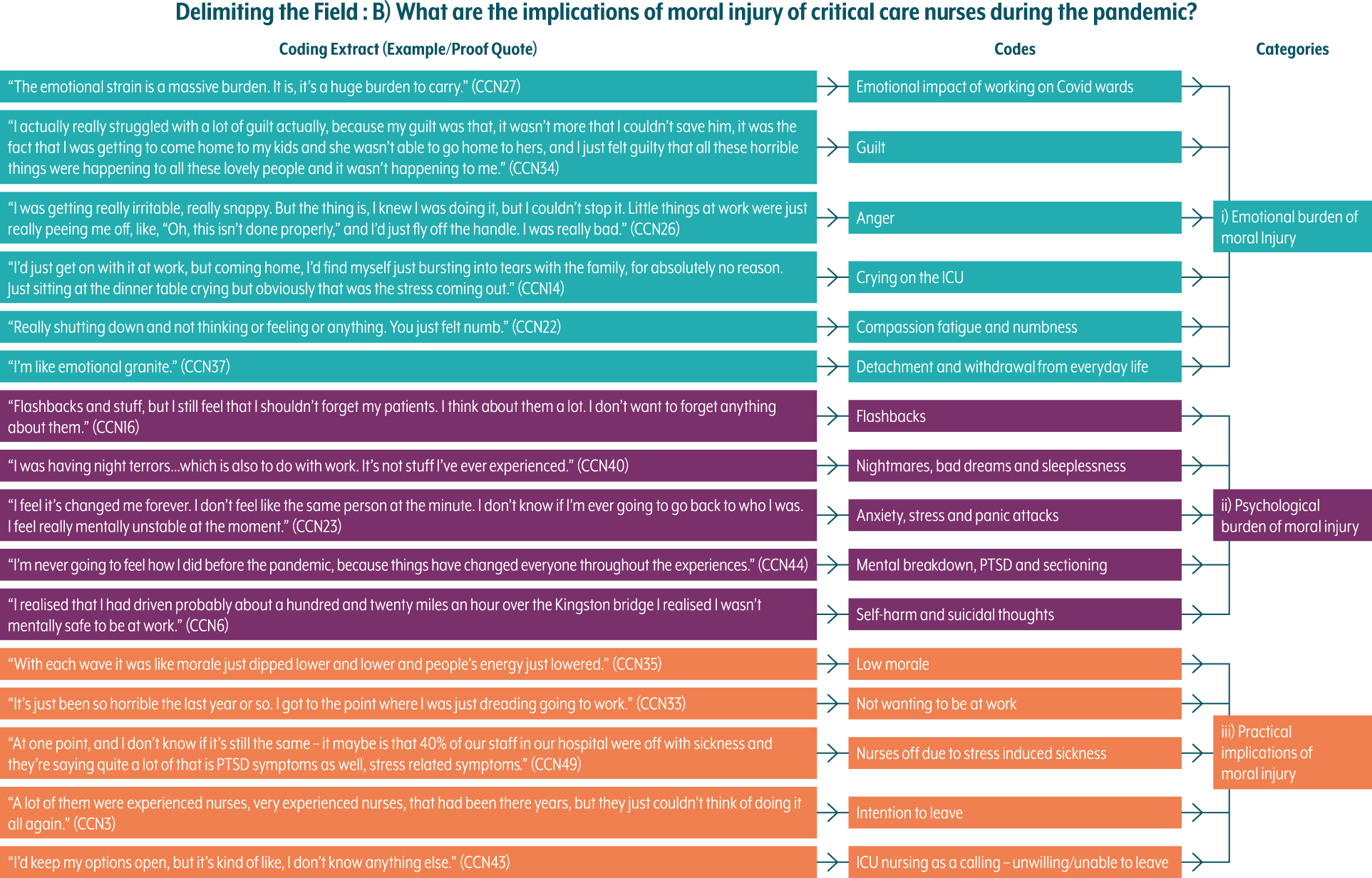
Coding architecture (implications).
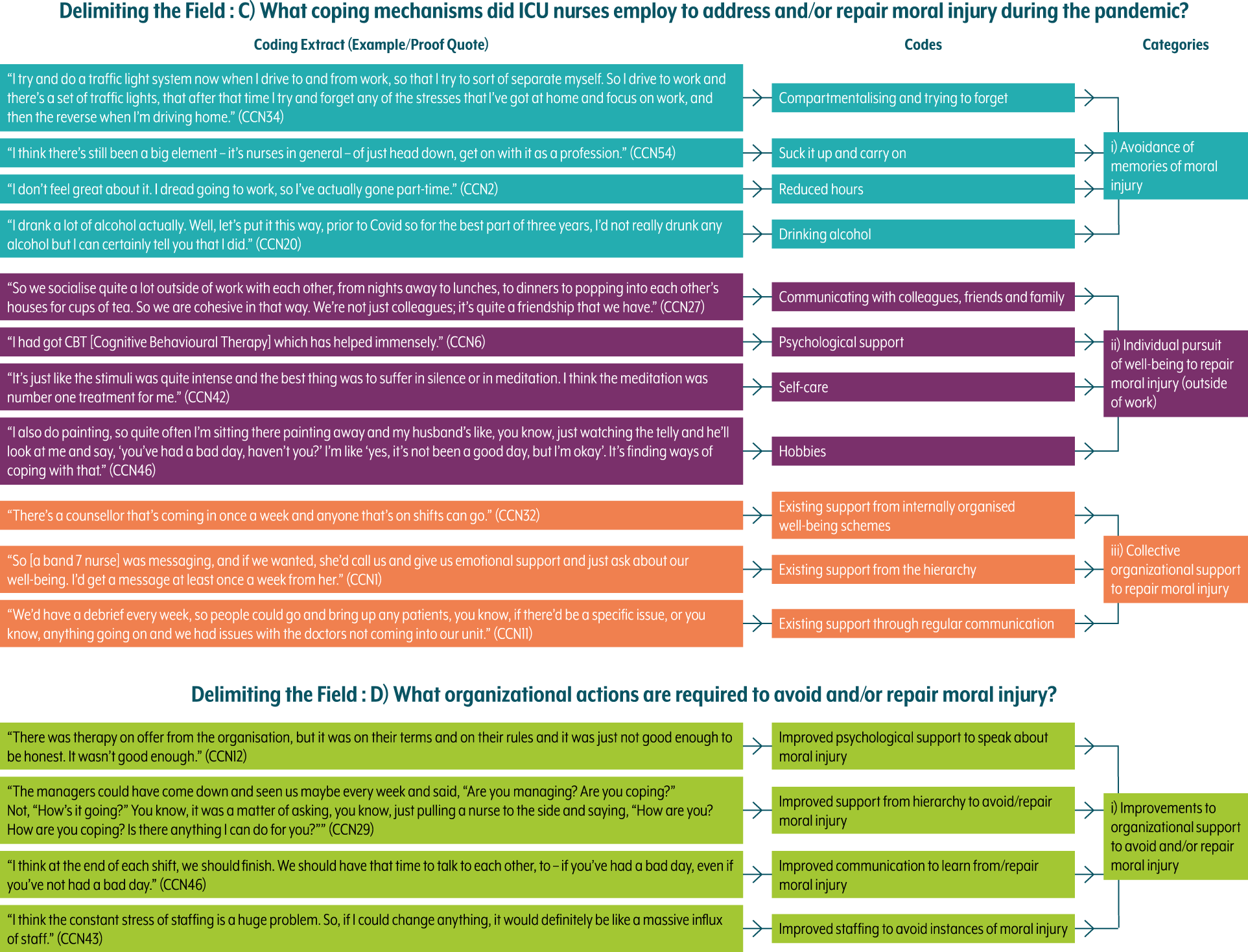
Coding architecture (coping mechanisms and required actions).
The analysis therefore asked: (a) ‘In what ways are critical care nurses experiencing moral injury during the pandemic?’ Following the literature on moral injury, specifically Litz et al. (2009, p. 700), we looked for PMIEs that involved ‘perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held beliefs and expectations’ in the critical care working environment. Following Čartolovni et al. (2021, p. 590), we also looked for instances of ‘deep emotional wounds’ that (as with Shay's (2014) definition of moral injury) included a ‘betrayal of what's right by someone who holds legitimate authority … in a high-stakes situation’. Author One's analysis of the data led to the creation of 16 codes that, following discussion and cross-checking within the team, were then grouped into 4 categories that best reflect the sources of moral injury during this period.
In keeping with this pattern, during the analysis, we also asked: (b) ‘What are the implications of moral injury of critical care nurses during the pandemic?’, reflecting the personal consequences of these experiences of CCNs who endured moral injury. This led to the creation of 16 codes and then 3 categories. In addition to this, we explored the following: (c) ‘What coping mechanisms did ICU nurses employ to address and/or repair moral injury during the pandemic?’ – an effort to understand how CCNs had tried to work through these experiences of moral injury, which led to the creation of 11 codes and 3 categories – and, finally, (d) ‘What organizational actions are required to avoid and/or repair moral injury?’, which reflected on the collective organizational response to moral injury, leading to the creation of 4 codes and 1 category. This analysis enabled us to construct a narrative around the experience of moral injury by CCNs during the pandemic whilst drawing out lessons learnt about how moral injury might be better avoided and repaired.
Findings
Our findings focus on the experience of moral injury by ICU nurses during the pandemic. We concentrate initially on exploring the kinds of situations that nurses experienced on the frontline (Litam & Balkin, 2021; Williamson et al., 2020), which challenged their deeply held moral beliefs and expectations about care (Litz et al., 2009). There are four broad kinds of experiences we consider in turn, reflecting the repetitive and thereby cumulative nature of moral injury when working in the ICU. We then consider the implications of these experiences of moral injury and the extent to which coping mechanisms and institutional responses were used to pursue moral repair (Paul et al., 2014).
Experiences of Moral Injury in the ICU
Unsafe Staffing Levels and Skill Mix
As the pandemic began and the influx of patients requiring critical care increased exponentially, the exceptional nature of the crisis became more apparent. CCN2 recalls, ‘it was like some kind of warzone, it was incredibly dangerous and incredibly stressful.’ One source of danger was the sudden shift in the ratio of nurses to patients away from 1-to-1 nursing (Şanlıtürk, 2021). Two nurses recalled: We were taking one to five, one to six patients per nurse. So obviously having six patients on a ventilator … when we’re only supposed to have one, just completely throws you off guard … you feel like ‘how could I possibly provide the same level of care to one patient that I normally do to six people?’ To do that … every day. You were constantly worried that you were making mistakes. (CCN30)
We were looking after far too many patients. We were doubling up, tripling up … it was just absolute, absolute madness. (CCN38)
These exceptional circumstances were the primary breeding ground for the experience of moral injury in the ICU (Čartolovni et al., 2021). They led to instances where basic care was, at times, impossible to deliver (Harris et al., 2021): ‘I mean honestly, just getting through the day and everyone still being alive; that was like all we could ask for. Like we couldn’t do a lot of the things we normally do’ (CCN28). There was a widespread feeling that basics around care were being compromised and that the ethical standards of care were being transgressed, leading to an unsafe working environment (French et al., 2021): ‘It was just unsafe, that place was unsafe, so working there was actually quite stressful’ (CCN42).
The redeployment of non-ICU nurses to the ICU during the early months of the pandemic was intended to help with rebalancing the nurse-to-patient ratio. However, the vast majority of the redeployed nurses had little-to-no experience of ICU nursing, leading to reduced skill mix on wards and, with this, added pressure. CCN2 explained: ‘It was correcting all of their mistakes, basically, and also looking after them in the sense that some of them were really, really helpful and really got on with it, and some of them were outright dangerous. They wouldn’t listen to you and just kind of did their own thing. That was incredibly stressful.’ Whilst there was a widespread appreciation by the ICU nurses of those who had offered (or been forced) to come and support, there was also a feeling that this amounted to a danger within the ward and the creation of an unsafe working environment: ‘I’m just like, this is dangerous – this is my PIN number [unique nurse registration code] and my career, this is someone's life more, than that, this is somebody's relative and you’re asking me to supervise [an untrained member of staff], I can’t do that when I’ve got nine other patients to supervise with two other untrained members of staff at the same time’ (CCN11).
Lack of Support from Senior Staff
This imposition of untrained staff during a period of unsafe staffing levels was felt by ICU nurses as a moral injury that they carried with them throughout the pandemic. These effects were, indeed, cumulative as nurses (particularly in the third phase of interviews) expressed anger towards those in positions of power who were deemed responsible for these ethical transgressions. Many ICU nurses blamed management within the NHS, highlighting the lack of senior nurses in visible patient-facing roles. CCN47 stated: ‘I think one of the band sevens, I think I saw her on there once, and that was because she was showing the chief exec. Around. It caused a bit of bitterness really.’ Other nurses highlighted institutional powers: ‘So people are pissed off and they don’t know if they’re pissed off with COVID or the actual Trust. Because we feel let down by the Trust, just as we feel let down by the government. The Trust is doing exactly the same thing as the government to be honest. So, it's a massive shortage of staff. They knew this was going to happen, nothing was in place to prevent that, they just said get on with it’ (CCN42). Each of these contributions to staff shortage (repeated by nurses across the interviews) – and subsequent inability to get the right assistance with patients – was felt as a moral injury insofar that it was fundamentally ‘a betrayal of what's right, by someone who holds legitimate authority’ (Shay, 2014, p. 182). There was a sense of betrayal by ICU nurses that a systemic weakness in staffing and historical lack of preparedness had placed them in morally painful situations in which delivering normal levels of safe and effective care was at times impossible.
Inadequate Resources to Provide Good Care
The widespread reports of a lack of PPE in hospitals also played a significant role in engendering a sense of moral injury for the CCNs. It echoes findings from studies on doctors during the pandemic who felt the lack of appropriate equipment left them ‘exposed’ and was ‘a kick in the teeth’ (Harris et al., 2021, p. 1367). CCN3 explained: ‘We started to get really upset because … they couldn’t get [PPE] fast enough. We hadn’t got enough masks, or if you’d got your mask, you hadn’t got enough suits.’ When PPE was being delivered, it was sometimes substandard or unsuitable: We normally wear the big surgical gowns, but we ran out of those. So, you were literally being taped into ten different aprons. It was like wearing ten bin bags. It was a joke. You literally went in, and this is supposed to be your protective equipment, and then someone with a bit of tape was literally taping you together. (CCN37)
Nurses also reported being asked to reuse PPE between breaks and ‘to double our risk, pretty much, by putting contaminated gowns back on’ (CCN1). All of these (and similar) instances left ICU nurses in a constant state of vulnerability to infection and the fear of taking the virus home to their families (Crowe et al., 2021). One nurse (CCN18) recalled: ‘There were quite a few shifts after that, that I would just sit my car and cry before going home. It was just out of sheer exhaustion and fear. I was worried that I would bring it home.’ Other nurses directly evoked the sense of a warzone in which they and their colleagues were poorly equipped and vulnerable to attack: ‘It was sort of that horrible feeling of going, oh actually could I die … a lot of my friends are nurses and doctors and I think that was the sadness … we’re fighting this war and not all of us may not be here at the end of it’ (CCN32).
Where PPE was available, and nurses felt more secure from infection, it was an incredibly uncomfortable physical experience to endure wearing it for 12-h shifts (Koenig, 2018). The nurses explained: ‘We’ve got nurses that have had scarring from just pressure damage’ (CCN22) and ‘A lot of the girls … have still got scars on their noses’ (CCN10). Others described ‘wearing PPE for 13 h is like, it's like being in a desert with no water’ (CCN39), an issue that was made worse by the fact that ICU nurses could not in any case drink too much fluid (as they could not afford to lose PPE for regular toilet breaks). The resulting moral dilemmas, influenced by what was felt to be a lack of political planning and institutional care, all contributed to the experience of moral injury. One nurse explained: ‘A human right to be able to go and get a drink or go and have a wee isn’t it? Yeah. But nurses hold their bladders until they can’t do it anymore’ (CCN41).
In the midst of this daily endurance, the shortage of medical equipment and medicines due to the sheer volume of patients and workload was particularly distressing to nurses in their efforts to maintain patient care. CCN23 described a situation in which ‘we didn’t even have piped in oxygen at some of the bed spaces [within the ICU]. So, we were having to use portables. Four months we were down there, and we still didn’t know where anything was. It was ridiculously dangerous and everybody was out of their comfort zone and everything we’d known was normal, was gone.’ Many nurses reported running out of medication so that they were having to make choices that felt unethical insofar that they contravened what they had been taught about the best care: We were running out of sedation … so basically like everything we’ve been taught [went out of the window] I feel like, it went back like 20 years where people were giving benzos because they didn’t realize … [negative patient outcomes] … like delirium and PTSD. So, I felt like I was going against what I should be doing by doing that. Kind of, it goes against best practice doesn’t it? All the things that you know you should be doing, but all of a sudden you can’t do anymore. (CCN16)
This situation experienced by ICU nurses was reflective of an overwhelmed system exacerbated by COVID-19 (Harris et al., 2021). It led to feelings of moral injury in which nurses knowing what care was required were not able to give it due to a lack of basic resources. The sense of betrayal by their workplace and the wider mis-management of a government response created emotional wounds that were felt deeply. One nurse (CCN31) stated: ‘So I think for me that was really challenging, because like, how can you give care when you haven’t even got the basic stuff to keep your patients sedated and safe, let alone anything else.’ The resulting damage to professional standards and expectations, as well as nurses’ professional commitment to offer care and prevent harm, had a knock-on effect of causing feelings of ethical transgression, which manifested as a major source of moral injury.
Unable to Give Patients a Dignified Treatment/Death
The novel nature of the virus during the pandemic also contributed to the experience of moral injury. As medical staff sought ways of slowing down the progress of the virus and reversing its effects, it led to situations where every viable treatment was being applied to a patient in an effort to save them despite the improbability of survival – a term that many nurses referred to as ‘flogging’: You flog people and then you’re ultimately looking after them, thinking, we all know they’re not going to manage, they’re not going to survive this but they’re not quite at that stage yet, that on paper we can withdraw [let them die] but we know that we are going to ultimately do it. There's no real satisfaction. You know, it's not a very satisfying job to just know that you’re keeping somebody going and that ultimately, you’ll be withdrawing treatment on them in a few days. (CCN47)
Many nurses felt that this came at the expense of the patient, leading to situations in which care might be considered inhumane (Harris et al., 2021). CCN39 explains: I think a lot of people that aren’t nurses or doctors maybe don’t realize there's a huge dignity and a privilege in giving a good death. That's part of nursing, certainly, that you give dignity and compassion and empathy, and you can give somebody a good death. Even attached to a ventilator, on a filter machine, it's that ability to go, we’ve got as far as we can, this patient isn’t going to survive, let's give them a good death. What's happening is, I think we’ve lost the ability to give a good death.
On a daily (or even hourly) basis therefore, ICU nurses were being asked to be complicit with what they often considered an inhumane death – professionally speaking perhaps the most serious of ethical transgressions – that was for all intents and purposes avoidable through different choices by those in positions of power. This contributed further to feelings of moral injury that as we shall see stayed with these nurses in a variety of different ways.
One of the most distressing aspects of patient care during this period was the added indignity of patients dying alone without families at the bedsides. Normally, patients – sometimes sedated and intubated but other times not – would be allowed close family members in with them to say goodbye, with nurses playing a central role in facilitating this process, which enabled what they might consider a ‘good’ death. In this situation, however, given the lack of time available, the requirement for families to use already scarce PPE, and hospital and government guidelines blocking them from doing so in any case, end-of-life care became a traumatic experience. CCN14 explained: Not having the families at the bedside for end of life, that was really difficult. So, it was, for all intents and purposes, it was the nurse holding the hand and stroking the forehead … we facilitated a virtual end of life if the family wanted that, or we would have rang the family, ‘what do you want us to tell your loved one? What is the most important message that you want to give them?’ And we would be whispering that into the patient's ears.
Other nurses such as CCN16 spoke about a patient's wife: ‘She just gave me a load of, like [audio] WhatsApp messages for me to play to his ear, which I did for like 3 days before he died. I feel like that really affected me.’ It was this somewhat unnatural situation with patient care that CCNs most regularly stated as the most upsetting, with nurses describing it as ‘heart-wrenching’ (CCN30), ‘horrific’ (CCN39), ‘horrendous’ (CNN47), and ‘morally wrong’ (CCN40), which reflected the ethical transgressions they felt complicit with, completely in opposition to the usual provision of a good death. CCN6 explained her frustrations and sympathies with the families: ‘I could imagine if it was me being kept in a room away from my person, I got really annoyed. Because where did they think that this was a good decision? Bring that woman in, let her say goodbye to her husband with the dignity that he deserves and the love that he deserves. So, I was really annoyed.’
The situation in the ICU, overall, was one in which nurses felt like they were never able to do enough with the resources that they had. CCN27 described: ‘It was almost like a battlefield. I personally don’t know what that feels like, so I don’t want to be flippant with that term at all, but it felt like a warzone and it felt like we were running to stand still.’ As another nurse described, despite all of these instances of moral injury and emotional wounds being inflicted, they were still ‘running towards the bullets’ (CCN18) and taking them on (in the form of emotional wounds) again and again. The overarching theme in the experience of moral injury in the ICU during this period was having to drop expectations in medical care across multiple areas, which severely impacted nurses’ core ethical codes and values (Čartolovni et al., 2021). There were situations where nurses felt the following: ‘We couldn’t give the same standard of care that we normally could, [and] that it wasn’t enough and that people deserved more than we were giving them’ (CCN28) and, another, ‘It changed the way I view nursing … so many things went on that just you would never, ever, you would just never, ever see or do or accept that went on, you know’ (CCN39). Whilst entirely blameless for the situations they found themselves within then, it was these memories of disappointment in the medical care provided that haunted many of these nurses due to the high professional and ethical standards they held themselves and their colleagues up to.
The cumulative nature of moral injury in a relatively short period of time was perhaps the most damaging aspect to ICU nurses. It became difficult for them to pinpoint that one moment that inflicted an emotional wound. CCN44 explains: ‘My stresses seem to be an accumulation of many things that what's caused it, you can’t pinpoint one thing. And it feels like lots of little things, but actually when I’ve spoken to the psychologist, they’re not lots of little things; they’re lots of very big things.’ The lack of rest and capacity to recover during the peaks and troughs within the waves of the pandemic made it extremely difficult to process what was going on or to begin to heal. There has been little chance for rest and recuperation: ‘I think it's a culmination of everything. It's from not recovering from the first wave, not resting from it, and then the expectation that they have on you is incredible’ (CCN2). There was a sense of an ongoing collective experience of moral injury as a profession in which, according to one nurse, ‘feels like the rest of the world's moving on and they’re all happy, and then the poor ICU nurses are just stuck in this horrible never-ending kind of nightmare’ (CCN33).
Implications of Moral Injury on CCNs
Emotional Burden of Moral Injury
The cumulative nature of moral injury during the pandemic had a variety of implications on CCNs. The emotional impact of working on COVID wards during the pandemic was the most immediate of these, with guilt being one of the foremost outcomes mentioned in the interviews (Williamson et al., 2021) – guilt, that is, in the face of powerful forces being unable to make different moral and ethical decisions in a time of crisis. One nurse, CCN34, explained her own experiences as follows: I went and had a chat with [my therapist] … and he talked about the fact that, there was a lot of cases during the Afghan and Iraq war where there were a lot of military nurses having the same issue, that they were feeling guilty about the fact that they survived … survivor's guilt. He called it a moral injury … that health professionals can go on to experience through the fact that they haven’t been able to save somebody, but they’re getting to carry on and live their life.
Many nurses spoke about their ‘anger’ (CCN8) or ‘rage’ (CCN23) emanating from their own powerlessness in the face of moral injury in the ICU, culminating in instances of being unable to regulate their emotions (Hayward & Tuckey, 2011). This surfaced through nurses either snapping at colleagues in the workplace or (as one of the most commonly coded instances) breaking down in tears in the ICU. CCN3 remarked: ‘You’re seeing [nurses], you’re seeing them falling to bits, you know, people walked off the unit … people just sat and cried.’ And CCN9 remarked: ‘I basically spent the whole nightshift walking round, crying. I just did all my work, fortunately my patients weren’t really conscious enough to see me, but I just spent the whole night walking around doing my jobs, crying.’ Another nurse (CCN14), in a managerial role, noted the broader effect on nurses in her hospital between the second and third waves: A lot of our ICU staff have just collapsed. We have them breaking down during shifts, you know crying, you know at home, crying on shifts, it's, you know, it's almost like the cavalry have arrived, albeit late, and we’ve sort of let our guard down a little bit. It's an emotional rollercoaster at the moment; with no highs, all lows … the hardcore ICU team, you know [are] broken, you know, and we just go off, have a cry, have a cup of tea, have a walk outside, come back in and get at it again.
Other nurses, such as CCN42, spoke about emotional outbursts on days off from the ICU: I went for a run to the park and I was running and I started to feel like a rising pressure in my head, like something was rising, and it was mainly anger, but I don’t know what I was angry of. I felt something very intense rising over a few minutes and I had to stop the run and I went into absolute hysterical mode. I was hysterical. And I don’t even know at the time what the hell is going on with my brain. I thought that I’d lost it, I thought I’d lost my mind. I had to stop running and it was just hysterical crying in the middle of a park and I couldn’t calm it down. It felt like the brain was on fire. It was kind of on fire. And there was like a million thoughts at the time, I don’t even know what was the main theme. I think it was anger.
Interestingly, this type of reaction is consistent with those of many war veterans suffering from moral injury who blame leaders and those in positions of power for placing them in situations where ethical transgressions were impossible to avoid. Shay (2014, p. 185) argues that ‘where leadership malpractice inflicts moral injury, the body codes it as physical attack … and lastingly imprints the physiology every bit as much as if it had been a physical attack’. The reaction of CCN42 to the cumulative experiences in the ICU clearly reflects the trauma of moral injury being felt physically within the body, the effects of an invisible emotional wound made visible.
Conversely, another response to the immense emotional burden of moral injury was to withdraw and feel very little at all. Nurses spoke of ‘really shutting down and not thinking or feeling or anything. You just felt numb’ (CCN22), whilst others spoke of detachment and withdrawal from everyday life and engagements so that they did not have to feign being emotionally in control. CCN44 explained: ‘I didn’t want to speak to anyone and I fell out with a couple of friends, because they kept messaging me and asking me how I was, and I was like, please just don’t talk to me, I don’t want to talk to anyone.’
Psychological Burden of Moral Injury
The psychological burden of cumulative and repetitive moral injury on CCNs was also significant (Litam & Balkin, 2021). Reminiscent of war veterans’ experiences of moral injury, ICU nurses regularly spoke of flashbacks that invaded their working lives. One nurse, CCN25, remarked: ‘You have these visions you can’t even get rid of. I said to my colleagues, how many ghosts can there be in your head? These people are dead, I’m still carrying them around.’ These ghosts manifested in a number of different ways in the home lives of many of the nurses in the form of sleepless nights, ‘being afraid to sleep’ (CCN7) due to nightmares (Stolt et al., 2021), heart palpitations, and debilitating panic attacks resulting from the trauma of repeated moral injury. One nurse described such an instance: ‘A physical reaction of the trauma … [a] situation that I could not leave behind, and it lasted for 3 days, constantly. I was actually shaking for 3 days, constantly having the flashes [of my dying patients]’ (CCN42.) CCN9 added another very common experience during this period: ‘I was waking up in the night, between four and eight times, and I was having nightmares and waking my boyfriend up with shouting. He said it was about work. He could tell. He said I’d cry in my sleep a lot and shout work-related stuff out.’
More broadly, ICU nurses reported widespread experiences of anxiety, stress, and panic attacks as a result of the emotional wounds of moral injury (Williamson et al., 2018). CCN20 explained: ‘Mental health has had a massive, massive impact because of the pressure, because of the amount of people that we’ve seen die. The fact that we were just helpless.’ This was not limited to a few nurses in the ICU either or those that had suffered previously with mental health problems: ‘It definitely feels like, across the board, not just on a personal point of view but my colleagues, everybody's really sort of, at the end of their rope really in terms of being able to cope with the stress’ (CCN38). In addition to this, the effects of the psychological impact on nurses due to moral injury were widely considered to be something that would be long-lasting (Caillet et al., 2020). One nurse (CCN3) put it quite bluntly, signalling the detrimental impact of these experiences: It upset me to see some of the [nurses]. One girl kept tapping her head so strongly. It was so bad. She was in a state with herself, and to watch her, she was looking at me eye-to-eye, just trying to stop crying. You could actually taste the atmosphere. You could slice it. You could just slice it. It was awful. It was awful. Anyway, yeah, the end of my career, love (laughs).
A number of nurses spoke directly about experiencing symptoms of mental breakdown and PTSD, another outcome attributed to the experience of moral injury in war veterans (Currier et al., 2015) and increasingly being found in healthcare settings (Bartzak, 2015), especially since the start of the pandemic (Williamson et al., 2021). Some nurses spoke of being diagnosed through visits to psychotherapists: ‘He diagnosed me with complex trauma PTSD, just because of the events in the past and events at work’ (CCN16), whilst others spoke about nurses on their wards who had been affected in this way: ‘I know lots of my colleagues have been off. They’ve all gone, you know, they’ve all got PTSD’ (CCN37) and ‘I mean we’re all broken, we’re all beyond broken. There's not a staff member that isn’t’ (CCN14). For some nurses, this situation had got so bad that they had suicidal thoughts: ‘I phoned the GP … and I’d said to them, look, I’ve had thoughts that I didn’t want to get up in the morning, didn’t want to exist anymore. Didn’t want to do my job. I’ve had enough. I feel like a number’ (CCN6), whilst another nurse (CCN16), with no previous mental health problems prior to the pandemic, spoke about the severe implications of her own encounters with moral injury: ‘[I experienced] more nightmares and flashbacks about my patients; I was sectioned twice over the summer under a Section 2.’
Practical Implications of Moral Injury
Previous studies on those experiencing moral injury in war settings have shown that individuals often subsequently undergo existential crises in which they question who they are and what they are doing with their lives (Shay, 2014). Similarly, the prevalence of moral injury during the pandemic fostered a sense of alienation (Gibbons et al., 2013) and led to lowering of morale and led many nurses to question the extent to which their employer has their best interests at heart: ‘The NHS would see me in a bloody coffin before, you know, they would stop taking from us, so I have to address myself and be me, look after [my]self’ (CCN41). Indeed, given the extreme nature of the implications of moral injury for ICU nurses during this period, it is perhaps unsurprising that the most commonly coded term in the study was ‘intention to leave’ (Carucci & Praslova, 2022). There is a palpable fear of a ‘mass exodus’ of talented and experienced staff occurring and of traumatized nurses ‘leaving in droves’ (CCN37). For many nurses, the pandemic has shortened their careers dramatically, forcing them to question why they were working for an institution that failed to shield them from cumulative moral injury: ‘I’ve actually handed my notice in. Whereas I probably would have gone on until I was 60, I just think no I’m going to do it now’ (CCN18). And another remarked: ‘I’d say this pandemic alone has probably taken about 5 years off our nursing careers, just (laughs) looking ahead into the future. I was just thinking the other day that, technically, I could still work for 42 years or something. I was like, there's not a hope in hell I’d be able to do that’ (CCN35). For many, the emotional wounds inflicted by the pandemic have meant moving out of nursing altogether: Seven people handed their notice [to my ICU] in within the week. Some people left without an alternative job. Half of them left and didn’t go for nursing positions; people have started their own businesses, like dog-walking businesses and something else. So, one of them is working in a supermarket. (CCN44)
There is a widespread feeling of having had enough with the ongoing nature of moral injury on a daily basis: ‘I’ve seen so many dead people. I’ve seen so many people die and I don’t want to do it anymore. I don’t want to – it's so depressing. There's no light in it at the moment’ (CCN39). However, despite the cumulative experiences of moral injury, many nurses still feel that critical care is their ‘calling’ and that they could not imagine themselves doing anything else: ‘I have been looking for other jobs, but the thing is, if I weren’t in critical care, I don’t know what I would do. It's hard, because what I feel like, I feel like the job that I love has been taken away from me at the moment’ (CCN23). The important thing to ask, therefore, is what is being done in the ICU to help CCNs cope with these experiences of moral injury and their implications and, perhaps even more urgently, what could be done to improve the working lives of CCNs in the future.
Coping Mechanisms and Organizational Action to Avoid and/or Repair Moral Injury
Avoidance of Memories of Moral Injury
Consistent with previous studies in other settings, CCNs relied on ‘cognitive avoidance as a maladaptive coping strategy’ (Williamson et al., 2018, p. 344). This might involve compartmentalizing and trying to forget what happened: ‘It was horrible. Like I’ve got – I feel like I’ve actually blocked parts of it out. There's stuff I can’t remember. I can’t remember all of the patients. I feel like I just blocked it out’ (CCN9). Other nurses spoke about ‘sucking it up’ (CCN1) or ‘burying your head in the sand’ (CCN38) and not having the ‘psychological safety … to say I’m not managing’ (CCN21). Much like a soldier's mentality, it was considered part of being an ICU nurse to be tough enough to cope with moral injury and show resilience in crisis (Powley, 2009). Whilst some nurses spoke about reducing hours to cope, the majority reflected this mindset: ‘It's a pandemic, get on with it’ (CCN39). Many nurses suggested that away from the ICU, they avoided feelings associated with moral injury (anger, guilt, etc.) through drink. Some were light-hearted about this: ‘Thank God for alcohol’ (CCN29), whilst others were more concerned: ‘Alcohol played a big part and then I realized, this is becoming a bit of an issue’ (CCN20).
Individual Pursuit of Well-Being to Repair Moral Injury
Nurses also undertook a variety of restorative activities to try and go through a process of moral repair or healing from the wounds of moral injury (Litz et al., 2009). This ranged from communicating with colleagues and friends and gaining support through family (cf. Mantri et al., 2021) to actively seeking psychological support. CCN12 explained: ‘Towards the end of the first wave, I had to get myself some private counselling because it was just too much.’ Another (CCN16) suggested that they had found an external agency to help with psychological issues she was experiencing: ‘There's a charity called Frontline19 that I found on Facebook. They gave me three counselling sessions for free. I was supposed to only have 12 sessions but he says it's not going to stop until like it needs stopping.’ Nurses also outlined a broad range of hobbies they undertook during the pandemic to either distract from the implications of moral injury endured (painting, walking, and photography, for example) or attempt to heal through self-care (meditation, yoga, and hypnotherapy). In each of these broader coping mechanisms above, however, the solution to moral injury seems to be both one of individualization – the nurse was expected to confront their moral injury alone. It was clear, from the widespread sense of abandonment, that many nurses felt that there was an ongoing abdication of responsibility by those in positions of power in terms of helping them to repair and recover following experiences of moral injury, further compounding its effects.
Collective Organizational Support to Avoid/Repair Moral Injury (and Actions Required)
Our analysis demonstrates the paucity and inconsistency of collective organizational support for ICU nurses. Whilst, for many, there was existing support through internally organized well-being schemes and limited counselling, this was in some cases (especially during the first two phases of interviews) missing entirely and/or slow to arrive. CCN11 suggested: ‘The psychologists? I never saw a psychologist, never met one, never had a phone call, never was given a phone number.’ And CCN43 remarked: ‘It sounds really harsh, but nothing really. Nothing like set-up officially … there was no sort of support for anyone psychologically.’ Most worryingly, nurses like CCN16, who had the most serious signs of moral injury and had, as noted above, been sectioned due to their experiences in the ICU, had found it impossible to receive anything beyond basic counselling: ‘The first time I was sectioned I was put on their waiting list [for Cognitive Behavioural Therapy] and I was took off the second time I was sectioned, so I’m still on the waiting list. I’ve contacted work and I’ve contacted the head of nursing as well who I know quite well. And they can’t like push me up the waiting list at all.’ One might speculate that this further betrayal by those in positions of power could only act to prolong and worsen this nurse's existing wounds of moral injury, conjuring yet more ethical transgressions upon those already committed.
Other nurses suggested that whilst there were a number of nurse-led initiatives and people trained in psychological first aid, it was often a case of a lack of availability of this psychological help: ‘There's this misconception that there's nothing out there, but the stuff that's out there, it's not easily accessible’ (CCN21). It was also reported regularly that nurses were either unable to take breaks to visit psychologists during their shifts or expected to come in at other times, which were inconvenient: They’re only half an hour or 45 min but we aren’t allowed to leave the ward to go to them. You have to be on a roster day off, and in reality, working through a pandemic, no one's going to come into the hospital on a day off for a session. (CCN35)
In many cases, then, rather than being addressed directly and rapidly (Greenberg et al., 2021), the emotional wounds of moral injury were being left to fester, and as seen in the case of war veterans, prolonged exposure to feelings of shame, guilt, and anger can make these wounds all the more difficult to repair (Litz et al., 2009). The ongoing lack of care by those in positions of power could be considered further acts of ethical transgressions that, again, deepen emotional wounds and make attempts at repair (when eventually received) even more difficult.
Whilst there were accounts of support from the hierarchy in terms of dealing with the outcomes of moral injury and the associated emotional and psychological distress, there were many more voices of disappointment and anger at senior staff within the NHS. This was not only for the aforementioned lack of staffing but also for failing to come to the nurses’ aid once moral injury had occurred. CCN9 explained: ‘I’ve been extremely disappointed in … the people higher up within the hospital hierarchy. I’ve felt really, really disappointed in the support or their lack of support that has been given to me.’ And CCN23: ‘I don’t feel that the establishment or the management – I don’t think our management have got any real understanding of what the intensive care nurses have been through, and I don’t feel like we’ve been offered any real support.’ These findings calling for improved support from the hierarchy in regard to moral injury experienced within the ICU echo Kalkman and Molendijk's (2021) suggestion that leaders can be purposefully ambiguous in their strategy, thus contributing to feelings of moral injury and, indeed, compounding the mistakes that they have made. It also points towards the need for a more systemic approach to tackling moral injury in which those in positions of power realize their roles in a healthcare system that allows those who put their bodies and minds at risk to go without the psychological and emotional support that they need.
Finally, in terms of collective organizational responses to moral injury, nurses pointed towards support through improved communication as central to aspects of moral repair. Surprisingly, in addition to obvious calls for increased staffing levels, one of the most called-for activities across the whole study was increased and/or improved debriefing at the end of shifts. On many wards, it simply was not happening: ‘We never debrief in my unit, which I think is not great’ (CCN2), which was seen as detrimental to learning and contributing to either avoiding future moral injury or assisting in moral repair: ‘At the end of each shift, I think we should have a debrief, definitely. I don’t think we should leave it too late to have ‘let's talk sessions’ because I’ve got some powerful feedback, but I do think we left it a bit too late’ (CCN46). In other ICUs where this did occur, it often happened informally. CCN1 stated: ‘Staff took it upon themselves to debrief. But there were no senior members of staff that said, this is what we need to be doing, we need to be having a debriefing session after our shifts. That is what we needed at that time. We needed to all sit there together and chat about our day and our feelings before we went off home. But we didn’t get any of that, really.’ This seems to support Griffin et al.'s (2019, p. 357) suggestion that ‘recovery from moral injury likely involves an affirmative community effort to understand and reintegrate the morally injured, as well as to accept shared responsibility for that injury’.
Discussion and Conclusion
We set out in this article to respond to recent calls to explore the experience of ICU nurses during the pandemic (Greenberg & Tracy, 2020; WHO, 2020). We took up the challenge to do so through the lens of moral injury (Čartolovni et al., 2021) and to do so empirically by giving a voice to the nurses who have given so much in recent years but have, for the most part, been unheard victims of a health system that takes advantage of people's willingness to do difficult and traumatizing labour for relatively low wages (Peredo et al., 2022) – exploiting nurses as ‘Willing Slaves’ (Bunting, 2004). We now offer theoretical and practical contributions of our study that we believe further the debate and deepen understanding of moral injury in frontline healthcare specifically and relation to work that traumatizes or injures more generally. In sum, our study offers a deepened theoretical understanding of moral injury as cumulative, intersubjective, and systemic in such a way that it invites a more collectivist approach to moral injury. The practical implication of this broader understanding of moral injury is that in professional contexts such as critical care, organizations can and should better understand how, where possible, to minimize instances of moral injury and when necessary speed up the process of moral repair.
Theoretical Implications: Moral Injury Reformulated
This study set out to investigate moral injury beyond its traditional psychological context, considering it through an interdisciplinary approach – by also embracing health, nursing, and organizational studies – which has, in turn, helped shift the theoretical understanding of the concept (Molendijk, 2018). First, our study has shown that whilst moral injury is often portrayed as a singular experience (‘a betrayal of what's right, by someone who holds legitimate authority’ (Shay, 2014, p. 182)), it can become multifarious and repetitive. Within the context of ICU, ethical transgressions were experienced by nurses on a daily basis in a multiplicity of different ways that deeply challenged their expectations about what constituted good and safe care. The moral injury was cumulative in nature (spanning more than a year) and expands our understanding of the ways in which moral injury can materialize and embed itself as an outcome of both previously routine activities in the workplace and the disruption of those routines. Our study shows that in extreme organizational settings or crises such as the pandemic, the emotional wounds of moral injury can be layered and experienced concurrently rather than just intermittently. The vast array of mental health conditions experienced in our study ranging from debilitating panic attacks to sectioning, coupled with the widespread intention to leave the profession, reflects how particularly devastating cumulative moral injuries can be.
Second, our study shifts the conceptual understanding of moral injury as a phenomenon experienced solely by an individual. One of the central reasons for the lack of collective action when it comes to repairing moral injury is that it tends to be approached as what Griffin et al. (2019, p. 357) call a ‘product of intrapsychic conflict’ – something experienced by the individual and thereby to be given meaning and solved by the individual alone (Currier et al., 2015). This has the effect of passing much of the responsibility for repair (and even the moral injury itself) onto the individual. Our data show that individualization of meaning-making and responsibility for moral injury inhibited the process of moral repair. Indeed, it served to heighten a sense of isolation and despair. In contrast, we emphasize the intersubjective dimensions of moral injury in organizational settings and the desire of nurses to communicate, share, and work through the emotional wounds that have occurred as part of shared occupational experiences. This is also supported through emerging research on repairing moral injury. Shay (2014, p. 189), for instance, argues that ‘you don’t get recovery without social connection … recovery happens only in the community’.
Third, our consideration of moral injury in the context of the ICU has also enabled us to show the systemic nature of moral injury. Building on previous research, our study showed ethical transgressions and omissions by those in positions of power, whether in government or hospitals, translated into a sense of powerlessness and betrayal by ICU nurses (French et al., 2021; Kalkman & Molendijk, 2021). This powerlessness was a result not only of the lack of support and planning in the moment of crisis but also of the systemic failure to plan for and resource in the years preceding the pandemic (e.g. understaffing and paucity of critical care beds resulting from a programme welfare state retrenchment and underinvestment). Our conceptualization of moral injury thus highlights its systemic and political components that go beyond but nonetheless impact the individual (Wiinikka-Lydon, 2017, p. 221). In this respect, moral injury, as a theoretical concept, should be understood as part of organizational systems and processes that sustain and fuel its very continuation, often stymying change from occurring or making it more difficult to contest and challenge established orders on a daily basis.
Practical Contributions: Moral Injury as a Catalyst for Organizational Change
The practical contributions of our study involve spreading awareness and deeper understanding of the experiences of moral injury as they relate to CCNs specifically whilst also encouraging consideration of the implications for workers vulnerable to moral injury more broadly. The point is to call on those in power, from government ministers to organizational leaders, to acknowledge the extent to which the tasks they require may emotionally wound workers and, just as importantly, to take steps to promote repair. It points to the need to give voice to the experiences – the moral injuries – of those working on our frontlines so that pain can be addressed and repair enacted through individual attention, collective care, and organizational change. This paper is one mechanism for voicing the moral injury experienced by CCNs.
The first step is to give voice to injuries. Perhaps one of the most important impacts of this paper has been to help ICU nurses understand they are not alone. On reading early drafts of the paper, much of the feedback from nurses was one of relief that they were not alone in feeling the emotions and psychological distress that they did during the pandemic. There was relief at being heard individually and collectively. Such relief points to the absence of voice within their own workplaces, communities, and national health systems. Bearing isolated witness to a clap for carers is no substitute for informal support over coffee, formal offloading at the shift's end, leader presence, or systemic emotional support from crisis beginning to end. We would argue that employers, leaders, and organizations they represent have a responsibility to give voice – to seek out, actively listen to, and respond to – the moral injury that arises in the course of work, whether that be the labour of the CCNs, public servants, private employees, or organized volunteers.
The study also provides a deeper awareness of the kinds of moral and ethical transgressions that can take place (Williamson et al., 2021). This is especially important, as Litz et al. (2009) identify, in the first steps towards moral repair. In their work with war veterans, the first steps of learning to deal with moral injury was ‘to have patients verbalize what they did or saw, how it has affected them … to disclose the transgression, articulate their attributions and how they have been feeling about themselves since the experience’ (Litz et al., 2009, p. 704). This study is valuable for the critical care community, therefore, insofar as it begins to collectively name the sources of moral injury so that they can be repaired. It is also an important precursor to considering the organizational change required to minimize recurrence.
Our exploration of the implications of moral injury on ICU nurses provided deeper evidence of its deleterious effects on mental health and well-being (Borges et al., 2020; Williamson et al., 2020). Our study provides a qualitative exploration of the emotional and psychological effects of moral injury that show widespread instances of resulting anxiety, PTSD, self-harming, and even sectioning. The practical contribution here is that the widespread experience of moral injury requires drastically improved psychological support for ICU nurses to work through feelings of guilt, shame, and anger. Whilst forms of cognitive therapies have been successfully used on war veterans suffering from moral injury that might also help ICU nurses, other studies suggest that ‘no validated treatment for moral injury currently exists … and [instead] approaches that focus on self-forgiveness, acceptance, self-compassion, and (if possible) making amends might hold more promise’ (Williamson et al., 2021, p. 454). This will, in any case, require vastly improved access to emotional and psychological help for ICU nurses and, indeed, other occupations on the frontline of the pandemic and other extreme settings. Whilst by the final phase of our study this was improving, too many nurses had been left to deal with the emotional wounds of moral injury for far too long and many remain in situations where they simply are not getting the support that they require. Beyond the pandemic, these findings invite us to consider how and when the work of other occupations might invite injury, the nature of that injury, and its effects and treatment (Litz et al., 2009). Treatment is likely to vary according to the specifics of the industry, occupation, individual, task, and context in question such that one-size-fits-all remedies are unlikely to be viable. Giving greater voice to the type and impact of moral injury faced by different occupations will however afford a sharing of experiences and a greater range of repair approaches (Goodstein et al., 2016).
Finally, our study provides a more practical understanding of what needs to occur organizationally to begin to minimize instances of moral injury in extreme workplaces such as critical care. Our findings suggest that significant improvement in organizational communication and learning will need to be central to this process. Prior to the pandemic, interventions showed the power of nurses talking within their communities about the emotional impact of healthcare work (‘coping together collectively through dialogue’) to reduce the psychological distress of healthcare (Taylor et al., 2018). This desire for a more collectivist approach here was confirmed further through the very high number of ICU nurses in the study who spoke about their desire for much more regular debriefs as part of a team that might, in turn, be able to apply early pressure to any emotional wounds of moral injury that had occurred on shift. In this sense, employers might usefully learn from the debriefing, sharing, and similar offload practices of voluntary organizations such as Samaritans (see McMurray, 2022).
In practical terms, stopping the occurrence of moral injury in an ICU ward entirely is, more or less, impossible. Nevertheless, through proper organizational responses to the causes of moral injury, such as (according to our data) tackling chronic understaffing in ICU wards, providing better support to staff, and resourcing the ward with appropriate medicines and equipment, the worst excesses of moral injury would be reduced and the impact ameliorated. Studies also point towards better training for senior staff in which ‘leadership at all levels should be trained to be aware of betrayal-based moral injury and to engage in moral repair to reduce staff intent to leave and encourage mutual trust’ (French et al., 2021, p. 516). Beyond this, we argue that it is also important to understand the practical experience and implications of moral injury as a societal responsibility and the result of decisions taken on a political level as to how we decide to fund and support our healthcare systems and those that work within them.
Our study suggests that more must be done to support ICU nurses (and healthcare professionals more broadly) from the emotional and psychological implications of moral injury in their working lives. This paper calls into question the levels of support offered to those who were caught ‘running towards the bullets’ and encourages a deeper reflection on what we owe to those who suffer deep emotional wounds so we, our families, and members of our community might receive care when we need it most.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.