
Abstract
Objective
To compare cleft lip and palate management between the USA and Guatemala, focusing on surgical timing, secondary procedures, and multidisciplinary access.
Design
Multicenter, retrospective cohort study (2011–2024); nonrandomized, with anonymized clinical and surgical data.
Setting
Vanderbilt University Medical Center (USA) and Moore Pediatric Surgery Center (Guatemala). U.S. care was continuous; care in Guatemala was provided through short-term surgical missions.
Patients
1693 patients aged 0–21 years with cleft lip and/or palate (790 Guatemala; 903 USA). Patients with Tessier clefts or non-Guatemalan residency (for the Guatemalan cohort) were excluded.
Interventions
Primary and secondary cleft surgeries and multidisciplinary interventions.
Main Outcome Measure
Age at primary surgery, cleft type, sex, secondary procedures, palatal fistula, velopharyngeal insufficiency, dental/ear interventions, and sociodemographics (Guatemala).
Results
Guatemalan patients underwent primary cleft lip and palate repairs at significantly older ages (p < .001) and had higher rates of palate fistula (24% vs. 7%), fistula repair (13% vs. 7%), and lip revision (15% vs. 8%) (p < .001). Access to multidisciplinary care was greater in the USA (myringotomy tubes: 70% vs. 10%; dental restoration: 24% vs. 17%; p < .001). Among Guatemalan patients, 53% lived in rural regions and traveled a mean 3.3 h to access care.
Conclusions
Significant disparities exist in cleft lip and palate management between Guatemala and the USA, marked by delayed surgical intervention beyond the optimal developmental window. Overcoming systemic, geographic, and socioeconomic barriers through integrated, sustainable, locally supported care models is critical to enhancing outcomes in resource-limited settings.
Keywords
Introduction
Escalating global health challenges have driven a surge in initiatives aimed at addressing the burden of untreated surgical conditions. Approximately three-fifths of the world's population lacks access to adequate surgical care, with the most affected communities residing in low- and middle-income countries (LMICs). 1 Although these countries account for 33% of the global population, they receive less than 10% of all surgical procedures annually. 1 Government health expenditure plays a critical role in shaping access to care, with higher spending consistently associated with reductions in mortality and morbidity. 2
In Guatemala, public health expenditure remains among the lowest in the Americas.3,4 As a result, healthcare access, particularly surgical care, is severely limited, especially in rural and indigenous regions where infrastructure deficiencies, socioeconomic disparities, and geographic isolation contribute to delayed diagnosis and treatment. 5 Although Guatemala is classified as a middle-income country, 6 nearly 60% of its people live in poverty, 5 many of whom face a daily struggle to access even basic health care. This disparity extends to congenital conditions such as cleft lip and/or palate (CL/P), which is sometimes left untreated due to these limitations.
In response to those gaps in Guatemala and other LMICs, numerous non-governmental organizations (NGOs) have emerged to help bridge the surgical care gap by providing targeted interventions where public systems fall short. 7 These efforts play a crucial role in addressing health inequities, reducing the burden of disease, and expanding access to essential surgical services. 8 Since its establishment in 2011, the Moore Pediatric Surgery Center (MPSC) has facilitated access to surgical care for underserved communities in Guatemala by coordinating short-term missions with U.S. surgical teams. 9 These missions provide essential procedures, such as CL/P repair, for children who would otherwise lack access to care. 10
CL/P is among the most common congenital anomalies worldwide, with an incidence of approximately 1 in 700 live births. 11 The prevalence of untreated CL/P is substantially higher in low- and middle-income regions, with rates in Latin America exceeding twice those reported in North America. 12 In Guatemala, where access to healthcare and surveillance systems are limited, reliable prevalence data are scarce. 13 As a result, up to two-thirds of congenital anomaly cases may go unreported. 13 One regional study documented cleft prevalence ranging from 4.7 to 18.9 per 10,000 live births, 14 but systemic underreporting and the absence of centralized data collection likely result in underestimation of the true national burden.
In LMICs, many children with CL/P do not receive surgical repair or multidisciplinary follow-up within optimal developmental windows. Barriers, such as limited access to medical care, financial constraints, low awareness of the condition, and insufficient knowledge of available treatments, compromise their outcomes.15–17 In contrast, CL/P management in the United States often follows well-established, evidence-based guidelines such as those developed by the American Cleft Palate–Craniofacial Association (ACPA). These protocols emphasize early surgical intervention, often with primary lip repair by 6 months and palate repair by 12–18 months. 18 Care is coordinated by multidisciplinary teams, including surgeons, speech therapists, otolaryngologists, and geneticists, who provide longitudinal support across childhood.18,19 This model has been shown to improve both functional and aesthetic outcomes, minimize complications, and reduce the need for secondary surgeries.18,20–22
Card et al. compared surgical timelines between Guatemalan and U.S. children with CL/P, revealing significantly longer delays in Guatemala. 23 However, the authors acknowledged limitations in their methodology, including a non-representative sample and a small sample size (n = 115). The disparity between care delivery models in the USA and Guatemala is evident. While institutional, year-round care is the standard in the USA, Guatemala often relies on intermittent, mission-based models provided by international NGOs. Although these missions play a critical role in expanding access to surgical care, their capacity for long-term patient follow-up, secondary corrections, and multidisciplinary care may be limited.
Despite well-documented disparities in cleft care between high-income and low-resource settings, few studies have systematically compared treatment outcomes using multicenter clinical data across these contexts. A recent scientometric analysis underscored the persistent inequalities in healthcare access, research funding, and policy implementation faced by low-resource countries, 24 and highlighted the ongoing lack of reliable, up-to-date data, driven largely by underreporting and weak health information systems. This absence of robust data continues to hinder the development of evidence-based protocols and sustainable health policies. The present study addresses this gap by contributing a large, multicenter dataset comparing cleft care in Guatemala and the USA and provides a more comprehensive overview of cleft management across economic settings. By evaluating differences in surgical timing, rates of secondary interventions, and access to multidisciplinary health services, this research aims to inform global cleft care strategies, support the development of adaptable treatment protocols in low-resource settings, and ultimately improve outcomes for children with CL/P.
Materials and Methods
Study Setting and Design
A multicenter, retrospective cohort observational study was conducted to compare the management of patients with CL/P across two populations. Data was obtained from the electronic medical records of Vanderbilt University Medical Center (VUMC), a tertiary care academic pediatric hospital in Nashville, Tennessee, USA, and from the physical medical records of the MPSC, a nonprofit surgical facility operated by the Shalom Foundation in Guatemala City, from 2011 to 2024. The MPSC was founded with the goal of providing free surgical care to pediatric patients with congenital deformities and general surgical needs. Short-term medical missions typically last one week, with three surgical missions scheduled annually for CL/P among other pediatric surgical needs, which Richard et al. have previously detailed. 25 Initial screenings at MPSC are conducted by a local maxillofacial surgeon, after which patients are scheduled for evaluation and surgery by U.S. surgeons who travel to Guatemala as part of nonprofit foundations. Follow-up care is provided by a Guatemalan surgeon with availability and discussions with the U.S. surgeons that previously operated on the patients.
Data Collection
Patients were excluded if they presented for initial evaluation but did not return for treatment or if they were diagnosed with Tessier clefts. To ensure accurate representation of the Guatemalan CL/P population and minimize characterization bias, individuals residing outside Guatemala who sought care at MPSC were excluded from the Guatemalan cohort, as they may differ demographically, socioeconomically, or clinically from the local population.
Data from the MPSC cohort were manually extracted from paper medical records by two researchers. One researcher reviewed the records, and the other entered the data into Microsoft Excel to ensure accuracy and consistency. Patient information was deidentified prior to analysis. Data from the VUMC cohort were extracted from the REDCap database. Using REDCap's data export querying tool, the dataset was exported to Excel with all identifying fields removed. Data fields were standardized and matched across both cohorts prior to analysis.
Data collected included patients’ clinical and demographic characteristics, surgical history, and multidisciplinary interventions. For the MPSC cohort only, parental sociodemographic data were also recorded. Cleft type was classified using the Veau classification system. 26 Isolated cleft lip (iCL) and submucous cleft palate (SMCP) were recorded separately. Patients with atypical presentations were categorized as Other/Indeterminate within their respective cleft type: those with iCL variants (e.g., median cleft lip or other non-classical lip phenotypes) were grouped as Other/Indeterminate iCL, while those with atypical cleft palate with or without cleft lip (CP ± L) presentations (e.g., cleft lip with contralateral cleft palate, non-continuous cleft phenotypes, unilateral cleft with variable palatal extension) were classified as Other/Indeterminate CP ± L.
Age at primary CL/P surgery was recorded in months to assess treatment timing. Surgical outcomes included documentation of velopharyngeal insufficiency (VPI) and palatal fistula. VPI was diagnosed through speech assessment and perceptual speech evaluation conducted by a speech-language pathologist (SLP). Secondary surgical procedures, including lip revision, pharyngeal flap, rhinoplasty, fistula repair, and other revision palatoplasties, were recorded if performed after the initial repair. Other revision palatoplasties refer to procedures performed for indications beyond fistula repair, such as VPI correction or palate re-repair.
Multidisciplinary interventions included dental restoration and myringotomy tube placement, with the latter's timing relative to primary palatoplasty documented.
Parental education was categorized as none, elementary, middle school, high school, or post-secondary education; parental occupation was also recorded. Monthly household income was documented in quetzales (Q) and converted to U.S. dollars (USD) using an exchange rate of 7.8 Q per 1 USD, which approximates the average rate during the study period. Access to care was assessed based on mode of transportation (public, private, or walking) and the time required (in hours) to reach the hospital. Patient residence was classified as either rural or urban. However, some variables had incomplete reporting due to changes in social work documentation forms over time. These gaps resulted from differences in documentation structure rather than selective omission and were therefore classified as missing at random. Analyses were conducted using the available data.
Statistical Analysis
Descriptive statistics were calculated for all variables, including frequencies and percentages for categorical variables, and means ± standard deviations (SD) or medians with interquartile ranges (IQR) for continuous variables, depending on the distribution. For continuous variables with non-normal distributions, medians and IQRs were reported, while normally distributed variables were summarized using means and SDs.
The Wilcoxon rank-sum test was used to evaluate differences in age at primary surgical intervention for CL/P. Categorical variables were compared between the Guatemalan and U.S. cohorts using chi-square (χ2) tests, including comparisons of secondary surgical intervention rates and multidisciplinary care. Fisher's exact test was applied when expected cell counts were insufficient for chi-square testing.
Differences in clinical and demographic characteristics, such as sex and cleft type, were also assessed using chi-square tests; the Pearson chi-square test was used for most comparisons. For all statistical tests, a p value of <.05 was considered statistically significant. All analyses were performed using R (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 1693 patients aged 0‒21 years with a diagnosis of CL/P who consulted or received surgical treatment, whether primary or secondary interventions, were included in this study. Among these, 790 patients were treated at the MPSC in Guatemala, and 903 patients were treated at VUMC in the USA. Of the 790 patients treated at MPSC, 31% (n = 246) had previously received care at another institution. Of these, 33% (n = 82) underwent primary cleft lip repair, and 67% (n = 165) received repair for both cleft lip and palate (CLP). In contrast, only 5% (n = 43) of the sample from VUMC had been treated outside the center; 98% (n = 42) underwent surgery for cleft lip, and only one patient (2%) received treatment for both CLP.
Demographics and Clinical Characteristics
A summary of the demographic and clinical characteristics of the MPSC and VUMC cohorts is presented in Table 1. Male sex predominated in both cohorts, with no statistically significant difference between the two populations (p = .147). In the MPSC cohort, 40% (n = 319) of participants were female and 60% (n = 471) male, with a similar distribution observed in the VUMC cohort, including 44% females (n = 397) and 56% males (n = 506).
Demographic and Clinical Characteristics of Patients with Cleft Lip and/or Palate at MPSC and VUMC.
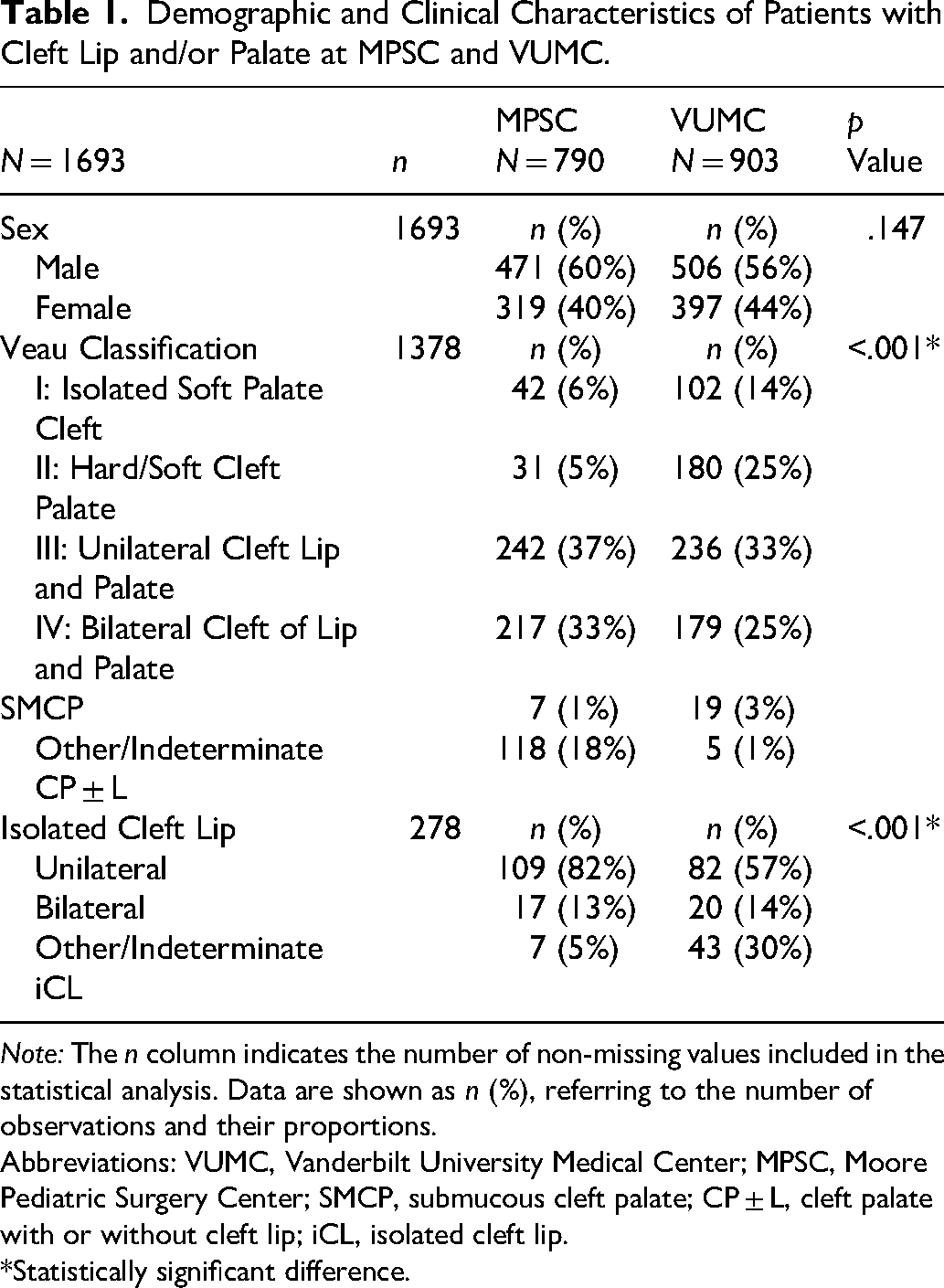
Note: The n column indicates the number of non-missing values included in the statistical analysis. Data are shown as n (%), referring to the number of observations and their proportions.
Abbreviations: VUMC, Vanderbilt University Medical Center; MPSC, Moore Pediatric Surgery Center; SMCP, submucous cleft palate; CP ± L, cleft palate with or without cleft lip; iCL, isolated cleft lip.
*Statistically significant difference.
Although the overall proportion of iCL was similar between cohorts (MPSC: 17%, n = 133; VUMC: 16%, n = 145; p = .667), the distribution of cleft types within the iCL subgroup differed markedly (p < .001). In the MPSC cohort, 82% (n = 109) of cases were unilateral and 13% (n = 17) bilateral. In contrast, the VUMC cohort showed a lower proportion of unilateral cases (57%, n = 82) and a similarly low proportion of bilateral cases (14%, n = 20), with 30% (n = 43) classified as other or indeterminate, compared to only 5% (n = 7) in Guatemala.
Significant differences were observed in the distribution of cleft palate types according to the Veau classification (p < .001). The MPSC cohort had higher proportions of Veau III and Veau IV, accounting for 37% (n = 242) and 33% (n = 217), respectively, compared to 33% (n = 236) and 25% (n = 179) in the VUMC cohort. In contrast, Veau I clefts were more frequent in the VUMC cohort (14%, n = 102) than in MPSC (6%, n = 42). Similarly, Veau II clefts were reported in 25% (n = 180) of VUMC patients compared to 5% (n = 31) in the MPSC cohort. SMCP was rare in both cohorts, accounting for 1% (n = 7) of cases in the MPSC cohort and 3% (n = 19) in the VUMC cohort. Other/indeterminate CP ± L accounted for 18% (n = 118) of cases in MPSC but only 1% (n = 5) in the VUMC cohort.
Timing of Primary Cleft Repair
Figure 1 illustrates the age at primary CL/P repair surgeries at VUMC and MPSC. The differences in age at primary repair between cohorts were all statistically significant (p < .001), indicating that patients at MPSC underwent cleft surgeries at older ages compared to those at VUMC.
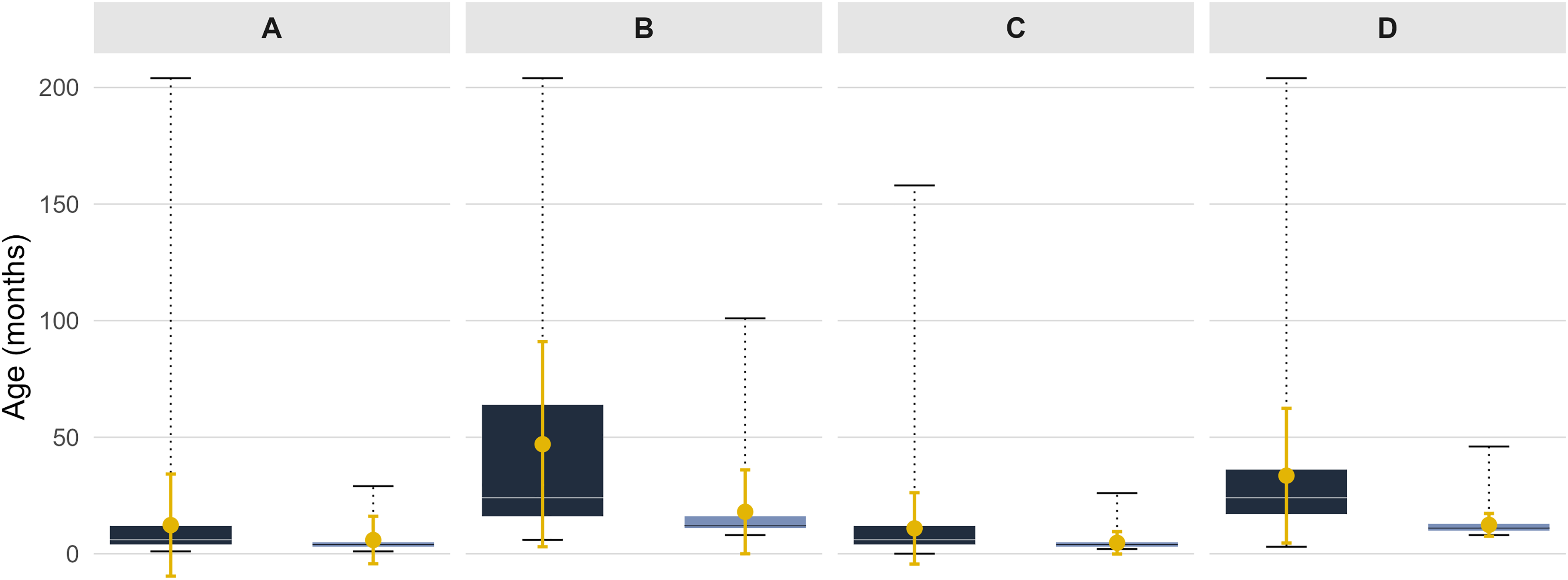
Comparison of age at surgical repair between the Moore Pediatric Surgery Center (MPSC) and Vanderbilt University Medical Center (VUMC) for primary cleft lip and palate repair: A. Isolated cleft lip repair, B. Isolated cleft palate repair, C. Cleft lip repair in patients with cleft lip and palate (CLP), and D. Cleft palate repair in patients with CLP. In each panel, the left box plot represents the MPSC and the right box plot represents VUMC. Each box plot shows the interquartile range (25th–75th percentiles), with the horizontal line indicating the median and whiskers representing the minimum and maximum reported ages. The mean age is shown as a solid dot, with vertical error bars representing ± 1 standard deviation (SD).
At VUMC, the median age at lip repair was 4 months (mean ± SD, 5.3 ± 7.6 months), and the median age at palate repair was 12 months (16 ± 15 months). In contrast, MPSC patients underwent lip repair at a median age of 6 months (11.4 ± 17.8 months) and palate repair at a median age of 24 months (36 ± 32 months), reflecting a significant delay.
Specifically, the median age for iCL repair was 6 months (12.3 ± 21.9 months) at MPSC versus 4 months (5.9 ± 10.2 months) at VUMC. For isolated cleft palate (iCP), the median age was 24 months (47 ± 44 months) at MPSC, compared to 12 months (18 ± 18 months) at VUMC.
Among patients with CLP, the interval between lip and palate repair was longer at MPSC (10.9 ± 15.3 and 33.5 ± 28.9 months, respectively) than at VUMC (4.7 ± 4.8 and12.4 ± 4.9 months, respectively). The age distributions for MPSC were highly right skewed, indicating that some patients received surgery at substantially older ages.
VPI and Palate Fistula
Palate fistula occurred at a significantly higher rate in the MPSC cohort (24%, n = 186) compared with the VUMC cohort (7%, n = 64; p < .001). VPI rates also differed between sites, occurring in 6% (n = 45) of MPSC patients and 13% (n = 117) of VUMC patients (p = <.001).
Secondary Surgical Interventions
Figure 2 presents rates of secondary surgical interventions in the two cohorts, with comparisons made using Pearson's chi-square test. Lip revision was more common in the MPSC cohort, occurring in 15% (n = 120) of patients, compared with 8% (n = 71) at VUMC. Palate revision rates were lower in the Guatemalan cohort (9%, n = 70) than in the U.S. cohort (14%, n = 125); both differences were statistically significant (p < .001 and p = .001, respectively).
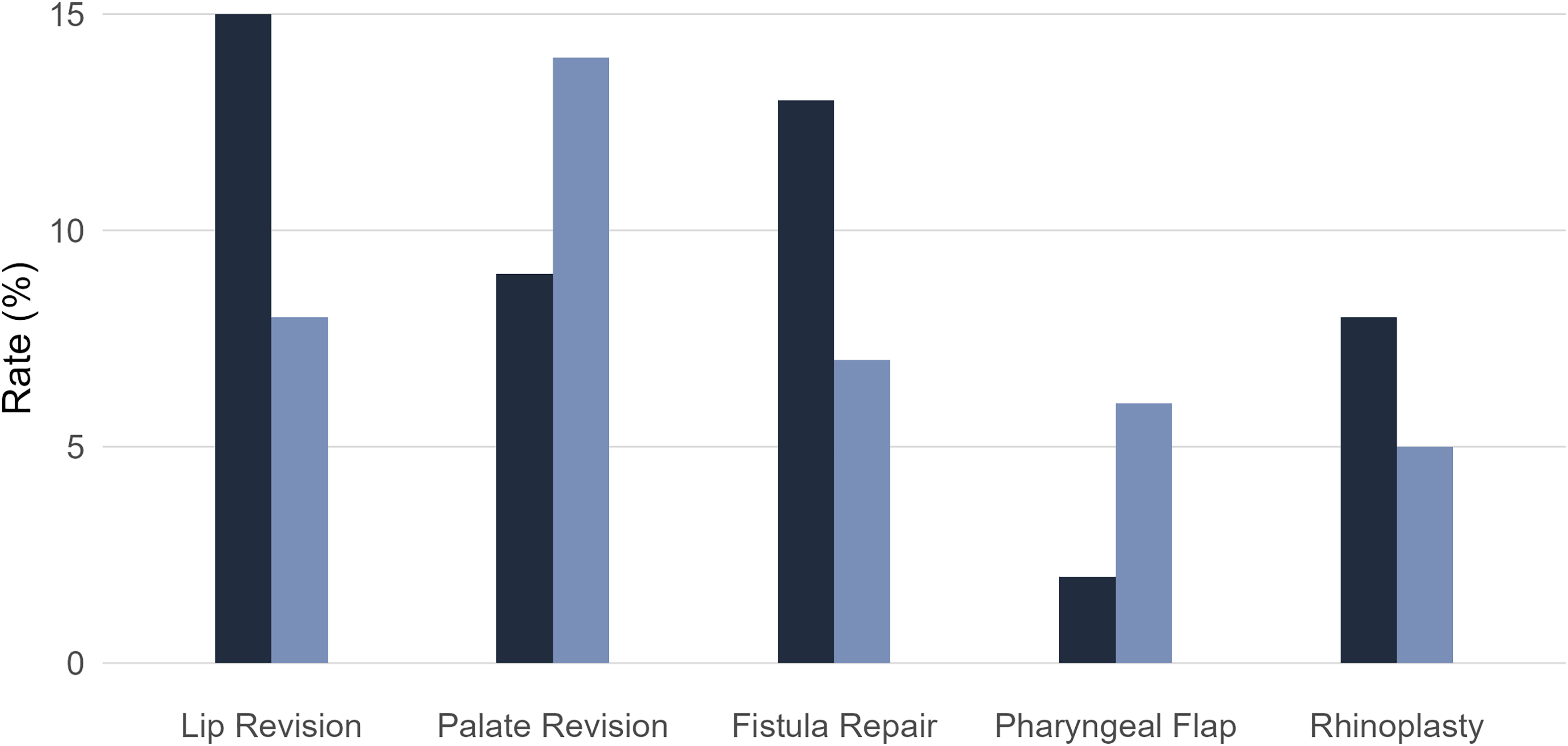
Comparison of secondary surgery rates between the Moore Pediatric Surgery Center (MPSC) and Vanderbilt University Medical Center (VUMC). In each category, the left bar represents the MPSC and the right bar represents VUMC. Each bar represents the proportion of patients who underwent the corresponding secondary procedure at each site.
Fistula repair was analyzed separately from revision palatoplasty. The fistula repair rate was higher in Guatemala (13%, n = 102) compared with VUMC (7%, n = 64, p < .001). Notably, 84 patients in the Guatemalan cohort had unrepaired palatal fistulas, whereas all identified fistulas at VUMC were surgically repaired.
Rhinoplasty rates differed significantly between cohorts (p = .006), with higher rates in Guatemala (8%, n = 63) compared to VUMC (5%, n = 43). Pharyngeal flap pharyngoplasty rates between groups showed significant difference (p < .001), occurring in 2% (n = 16) of MPSC patients and 6% (n = 56) of VUMC patients.
Multidisciplinary Team Approach
Among patients with palate involvement, there was a statistically significant difference in myringotomy tube placement rates between cohorts (p < .001; Table 2). At MPSC, out of 657 patients with palate involvement, 90% (n = 594) did not receive tube placement in the first year of life or at the time of cleft palate repair. Among those who did, 4% (n = 26) had tubes placed prior to primary palatoplasty, and 6% (n = 37) had tubes placed at the time of palate repair. In contrast, at VUMC, 70% (n = 528) of the 758 patients with palate involvement underwent tube placement, with 19% (n = 143) receiving tubes before palatoplasty and 51% (n = 385) at the time of repair.
Rates of Myringotomy Tube Placement and Dental Restoration Among Patients at MPSC and VUMC.
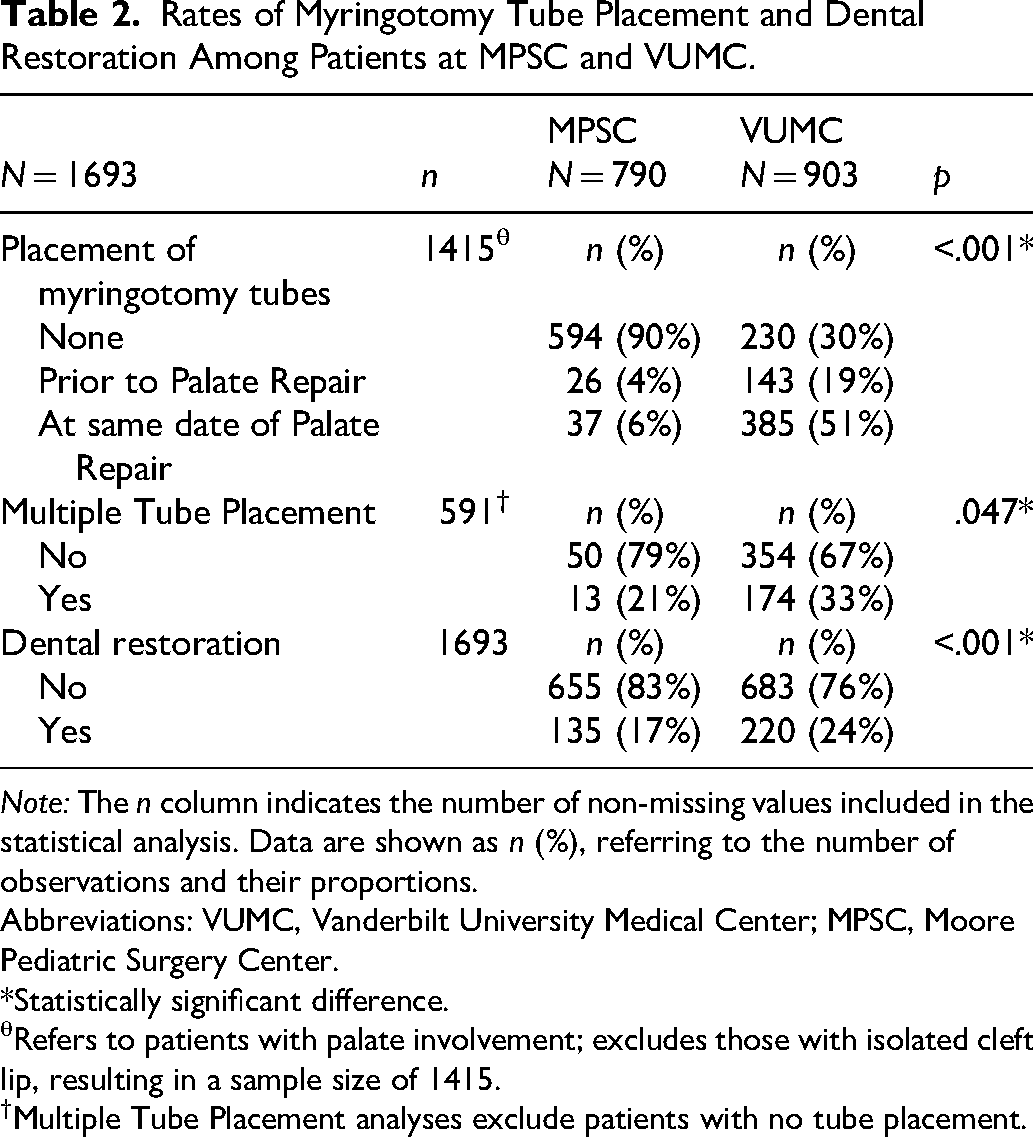
Note: The n column indicates the number of non-missing values included in the statistical analysis. Data are shown as n (%), referring to the number of observations and their proportions.
Abbreviations: VUMC, Vanderbilt University Medical Center; MPSC, Moore Pediatric Surgery Center.
*Statistically significant difference.
θRefers to patients with palate involvement; excludes those with isolated cleft lip, resulting in a sample size of 1415.
†Multiple Tube Placement analyses exclude patients with no tube placement.
Among patients who received tubes, multiple ear tube placements were more frequent in the U.S. cohort (33%, n = 174 of 528) compared to Guatemala (21%, n = 13 of 63; p < .047).
Dental restoration was performed in 17% (n = 135) of MPSC patients and 24% (n = 220) of VUMC patients (p < .001).
Regional Context: Guatemala
In the Guatemalan cohort, sociodemographic characteristics, including parental profiles, were analyzed using measures of central tendency and dispersion. Over half of the patients resided in rural areas (53%, n = 419), while 46% (n = 365) lived in urban settings. Mode of transportation to the MPSC was recorded for 421 patients: 73% (n = 308) used public transportation, 26% (n = 109) private transportation, and four traveled on foot. Travel time to the center was documented for 422 individuals, with a mean duration of 3.26 ± 3.49 h (see Table 3).
Parental Socioeconomic Characteristics at MPSC.
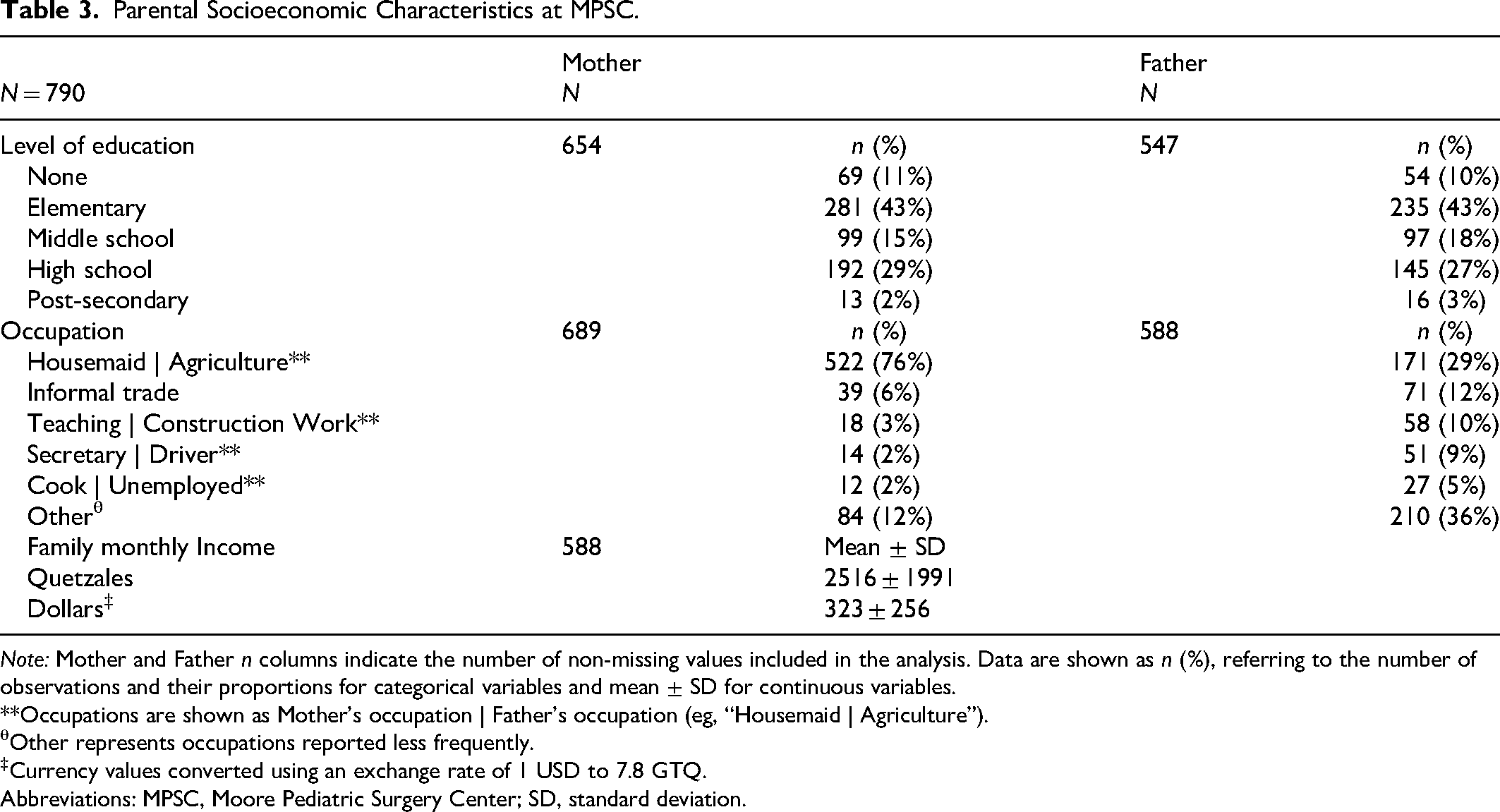
Note: Mother and Father n columns indicate the number of non-missing values included in the analysis. Data are shown as n (%), referring to the number of observations and their proportions for categorical variables and mean ± SD for continuous variables.
**Occupations are shown as Mother's occupation | Father's occupation (eg, “Housemaid | Agriculture”).
θOther represents occupations reported less frequently.
‡Currency values converted using an exchange rate of 1 USD to 7.8 GTQ.
Abbreviations: MPSC, Moore Pediatric Surgery Center; SD, standard deviation.
Among 588 families, the average monthly household income was 2516 ± 1991 quetzales (approximately 323 ± 256 USD; see Table 4). Regarding maternal education, 43% (n = 281) had completed only elementary education, 2% (n = 13) had post-secondary education, and 136 had an unspecified educational level. Most mothers were employed as housemaids (76%, n = 552), followed by informal trade (6%, n = 39) and teaching (3%, n = 18). Among fathers, 43% (n = 235) had elementary education and 3% (n = 16) had post-secondary education. The most common paternal occupations were agriculture (29%, n = 171), informal trade (12%, n = 71), construction (10%, n = 58), driving (9%, n = 51), and 5% (n = 27) were unemployed. A wide range of additional occupations were reported among both maternal and paternal roles, each comprising less than 5% of the sample.
Access to Care at MPSC.
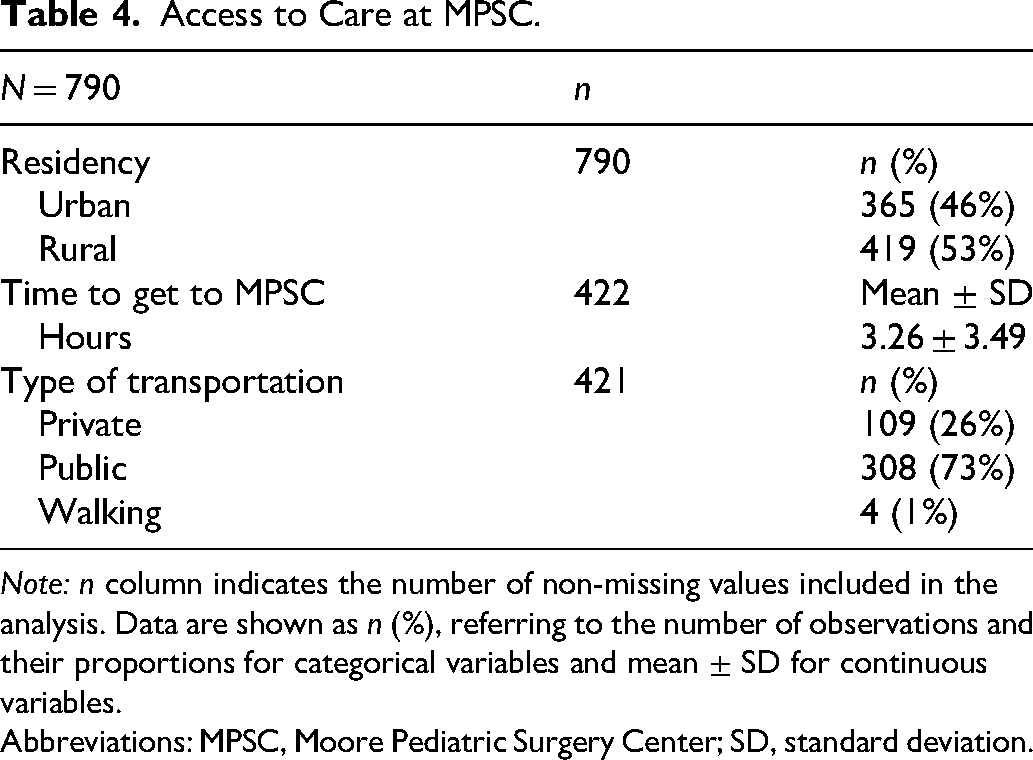
Note: n column indicates the number of non-missing values included in the analysis. Data are shown as n (%), referring to the number of observations and their proportions for categorical variables and mean ± SD for continuous variables.
Abbreviations: MPSC, Moore Pediatric Surgery Center; SD, standard deviation.
Discussion
Comparative studies of cleft care across countries with different economic contexts and healthcare systems are scarce. Our study revealed that Guatemalan patients with CL/P experience significantly delayed primary surgeries compared to U.S. patients and undergo secondary procedures at varying rates. These differences reflect inequities in cleft management between high-income and resource-constrained settings and highlight the need for contextually adaptable care models.
To improve cleft care outcomes in resource-limited settings, it is essential to identify the systemic and contextual factors driving delays and uneven surgical access. Guatemala's healthcare system is divided between public and private sectors, with fewer than 5% of the population covered by private insurance and approximately 18% covered by social security through formal employment. 27 As a result, the vast majority of the population relies on the public health system, which is organized into different levels, including health posts staffed mainly by certified nurses; health centers where general physicians and nurses provide care; and about 45 hospitals nationwide, only seven of which are classified as specialized facilities. 28 However, there are under one hospital bed per 1000 Guatemalans, 4 and the density of surgeons remains under four per 100,000 population, 29 far below the Lancet Commission on Global Surgery 2030 target of at least 20 per 100,000, necessary to provide basic surgical services. 1 These capacity constraints compel the public system to prioritize the most urgent or life-threatening conditions, likely contributing to delayed cleft repairs and inadequate long-term follow-up.
Consistent with prior research, children with cleft conditions in LMICs often receive primary repair well beyond internationally recommended timeframes. 30 One study linked Gross Domestic Product inversely with timely access to primary cleft repair. 31 Retrospective research from Indonesia and Brazil showed that over 60% of patients experienced delayed cleft repair.32,33 Conversely, a U.S. national analysis found that fewer than 15% of patients faced treatment delays overall. 34 In our study, Guatemalan children underwent CL/P repairs at older ages than those at VUMC; lip repairs occurred early in some cases, but on average patients were nearly twice as old at surgery. Palate repairs were delayed even more, often occurring more than twice as late as at VUMC, underscoring significant barriers to timely care.
Our results align closely with those reported by Card et al., 23 allowing direct cohort comparison. Using a substantially larger sample, our analysis shows a meaningful delay in age at repair, highlighting greater disparities in surgical access than previously reported. These delays reflect systemic and structural barriers within the Guatemalan health system. Limited access to surgical specialists and fragmented referral pathways contribute to late cleft repairs, which are associated with speech impairment, hearing loss, psychological distress, and social exclusion.35,36
Card et al. 23 also reported that children in Guatemala presented with more severe anatomical clefts, with CLP being the most common diagnosis. Our findings confirm the predominance of unilateral CLP, followed by bilateral CLP, with iCP being the least frequently observed, whereas at VUMC, iCP was seen in 40% of the patients. Matute and colleagues 14 conducted a survey with midwives who reported the prevalence of craniofacial clefts over one year. Their study found a significantly higher prevalence of cleft lip compared to cleft palate; however, none of the cleft lip cases were in combination with cleft palate.
A cross-sectional multicenter study in Nigeria aimed to identify factors influencing the timing of primary cleft repair. The study found that less severe clefts were associated with greater delays in treatment, with incomplete cleft palates exhibiting higher rates of delayed repair compared to other cleft presentations, 37 likely because iCPs are less visible and often undiagnosed until speech issues emerge. In our study, the lower prevalence of isolated cleft palates could be due to diagnostic challenges or limited access to specialized evaluation.38,39 This may also explain the markedly longer delays in palate repair observed among MPSC patients with iCP, compared with those patients with CLP.
Few studies have compared rates of secondary cleft interventions across countries with differing economic and healthcare systems. In our analysis, we found higher rates of lip revisions in Guatemala, but lower palate revision rates than in the USA, suggesting challenges in achieving optimal primary outcomes in resource-limited settings, missed surgical optimization, or inconsistent follow-up. This may be further complicated by the fact that 31% of Guatemalan patients received primary repairs outside MPSC, which could contribute to variability in surgical outcomes and reduced follow-up continuity. A study in neighboring El Salvador found that with every additional year of follow-up, the odds of attending a visit decreased by 27%. 40 Makar et al. 41 reported that the need for revision palatoplasty and pharyngoplasty increased with longer follow-up, rising from 4.7% to 21.7%, further underscoring the importance of long-term follow-up.
Beyond these factors, anatomical characteristics such as cleft width and classification have been shown to influence functional outcomes and the need for secondary surgery. Yao et al. 42 conducted a study that demonstrated a positive correlation between palatal cleft width and the occurrence of VPI following primary palatoplasty. Similarly, Okhiria and colleagues 43 reported that greater cleft width was a predictor for secondary surgical interventions. Additional studies have shown that higher Veau classifications, reflecting more extensive cleft involvement, are linked to increased rates of complications and poorer speech and surgical outcomes such as VPI, palate fistulas and suboptimal aesthetic results.44–46
Our study shows a notably higher rate of palate fistulas in the Guatemalan cohort, likely reflecting the higher prevalence of severe anatomical clefts, as demonstrated in the meta-analysis by Bykowski and colleagues. 47 Additional contributing factors may include differences in nutritional status and wound-healing capacity, 48 as well as the itinerant nature of surgical care at MPSC. 49 Among children diagnosed with palate fistula, 11% did not undergo surgical repair at MPSC, in contrast to the VUMC cohort, where all identified fistulas were treated. These findings highlight the significant backlog of unrepaired clefts in Guatemala and the prioritization of initial surgical interventions over secondary procedures. Rousso et al. 50 similarly found that the odds of fistula repair during mission trips were significantly lower than those for primary cleft repair, noting that in settings with limited surgical capacity and mission-based care delivery, providers often prioritize primary repairs, leaving fewer resources for follow-up interventions such as fistula closure.
In contrast, the observed rate of VPI was significantly lower in the Guatemalan cohort, despite the greater severity of cleft phenotypes in this group. This discrepancy likely reflects differences in diagnostic criteria and reporting practices; more severe cases of VPI may be documented in Guatemala, while VUMC records even mild cases through systematic postoperative speech evaluations. A Peruvian study comparing VPI rates between mission-based and referral center models reported rates nearly three times higher at surgical missions. 51 Ideally, VPI should be assessed by a trained SLP, a specialist who may be inconsistently available in resource-limited settings, potentially contributing to underdiagnosis in LMICs. 52 This raises the possibility that VPI is underdiagnosed or underdocumented in the Guatemalan setting. Additionally, the absence of standardized cleft care protocols and variability in surgical techniques across mission settings may contribute to inconsistent outcomes. 53
Our findings also demonstrate significant disparities in multidisciplinary cleft care between Guatemalan and U.S. patients. It is estimated that 97% of the children with CLP will develop otitis media with effusion in the first two years of life, predisposing them to hearing disabilities and consequently speech abnormalities.54,55 The markedly lower rate of tube insertion in Guatemala, alongside fewer repeat procedures, suggests limitations in access to otolaryngology services and challenges in delivering comprehensive, longitudinal care. Studies have shown that early myringotomy tube placement may offer improved early middle ear ventilation and potential speech and hearing benefits.56,57 The earlier and more frequent use of myringotomy tubes in the U.S. cohort likely reflects established protocols to reduce the risk of otitis media and associated hearing loss in children with cleft palate.
Children with CL/P are at increased risk of dental abnormalities compared to those without clefts. 58 The dental restoration rate was also higher in the U.S. cohort. However, this study does not distinguish between general dental care and the specialized interventions often required for patients with CL/P, such as orthodontic, periodontal, or prosthodontic procedures, 59 which can vary significantly in availability.
Beyond structural limitations, geographic, economic, and sociocultural barriers further constrain access to care. An estimated 31% of Guatemalans lack access to healthcare altogether. 60 In many rural and Indigenous communities, traditional healers continue to serve as first points of contact, offering culturally important care alongside the formal health system. 61 These regions often face long travel times, low household income, and language barriers that complicate referrals and continuity of care.62–65
Sociodemographic data from the Guatemalan cohort highlight the multifactorial barriers influencing health outcomes. With over half of patients residing in rural areas and experiencing average travel times exceeding three hours to reach the surgical center, geographic isolation clearly limits timely access to specialized care. Furthermore, the average family income was Q2,516.00 (approximately $323.00), while the cost of the basic food basket as of February 2025, defined as the minimum nutritional intake required to meet the energy and protein needs of a household of 4.77 members, was Q2,188.70.66,67 This narrow margin suggests that many families operate at or just above subsistence level, leaving them economically marginalized and with limited capacity to afford additional healthcare-related expenses.
Numerous studies examining underserved populations have identified barriers to timely and adequate cleft care, including travel costs, limited health literacy, shortages in the medical workforce, and insufficient economic support.68,69 Moreover, parental educational and occupational profiles suggest economic challenges that may affect health-seeking behavior, adherence to treatment plans, and the ability to attend multiple appointments. Plonkowski et al. found that a higher maternal education reduced the odds of delayed primary cleft surgery. 70 In our study, only 2% of mothers had postsecondary education.
In Guatemala, an estimated 2009 cases of unrepaired craniofacial clefts occur annually, according to a model developed by Carlson and colleagues. 71 The burden of cleft care falls largely on public hospitals and NGO interventions. While many NGOs aim to alleviate the immediate surgical backlog by temporarily expanding the healthcare workforce, these efforts often lack integration into long-term, multidisciplinary care systems. To address these gaps, a care model has been developed to promote sustained and coordinated cleft care through locally embedded solutions. This diagonal care model emphasizes the training, education, and mentorship of local surgeons; the development of local infrastructure; securing sustainable financing; establishing an effective referral system; and strengthening academic research capacity. 72 By building comprehensive programs, the goal is to bridge the gap in surgical and rehabilitative outcomes between resource-limited settings and high-income countries, with a focus on long-term cleft care and sustained follow-up. 73
In India, the transition from mission-based interventions to a diagonal care model has been shown to improve the longitudinal management and outcomes of children with facial cleft deformities, primarily through the development of specialized centers.74,75 This shift has led to improvements in surgical outcomes, patient follow-up rates, and access to multidisciplinary services, marking a significant advancement in comprehensive cleft care.76,77 El Salvador has begun to implement a similar diagonal care approach by integrating mission-based support with investments in local capacity, infrastructure, and long-term follow-up. This model has shown promise in improving continuity of care and building sustainable, locally driven solutions, reinforcing the effectiveness of diagonal care systems in addressing the complex needs of patients with craniofacial clefts in resource-limited settings. 78
Taken together, these findings underscore the urgent need for targeted interventions to strengthen cleft care in Guatemala. We propose focusing on four key areas, integrating culturally sensitive community health initiatives:
1. Policy and System Leadership: Governments must recognize cleft care as an essential surgical service and allocate targeted resources, especially in underserved rural regions.
It has been established that children with CL/P demonstrate lower academic achievement.
79
Integrating national cleft care programs into public health strategies, alongside investments in surgical infrastructure and workforce training, could significantly improve outcomes for children in Guatemala and similar settings.
1
Moreover, such investments may contribute to broader economic development.
80
Partnerships between NGOs and municipalities can reduce transportation barriers through subsidies that improve follow-up rates.
81
Timely communication about missions and available surgical services would further support continuity of care beyond the initial point of contact.
2. Humanitarian Models: NGOs must prioritize long-term health system strengthening over short-term surgical volume, emphasizing training, integration, and continuity of care.
The goal should be to transition from a mission-based model to capacity-building and integrated care, fostering partnerships with local providers to ensure sustainable training, educational development, and global collaboration. Research must be prioritized within the diagonal model. Collaborative research and dedicated funding for comprehensive follow-up data can improve the integration of NGO-collected information into national health systems. This, in turn, can inform clinical protocol development and strengthen public health strategies in similar resource-limited settings.82,83
The Moore Center conducts missions across multiple surgical subspecialties, including otolaryngology. Enhancing interdisciplinary management, encouraging open communication among surgical teams, and investing in non-surgical services such as speech-language therapy and psychology would help advance comprehensive care. Telemedicine for follow-up, including evaluations and virtual speech therapy, can further expand services and improve continuity of care.
84
The MPSC has the potential to become a national referral center for children with clefts, as regionalization typically offers greater resource allocation and access to concentrated expertise.
85
3. Local Clinical Capacity: Provider-level innovation, including task-sharing is key to improving outcomes within constrained systems.
Task-sharing in cleft care, such as nurse-led speech therapy and the training of local surgeons through affordable and feasible models like virtual-reality workshops and exchange programs, 86 has the potential to improve surgical skills and reduce the cleft care backlog.
Furthermore, training midwives, certified nurses at health posts, and other first-contact health providers to recognize diagnostically challenging cases can strengthen the referral system and ensure timely access to specialized care.87,88 Despite being a crucial part of the health system, these frontline providers have often been marginalized and overlooked. 89 A national congress dedicated to this essential workforce has yet to be held in Guatemala. Recognizing and fully integrating them into the healthcare framework is vital for building a more effective and inclusive care system.
Improved documentation of complications and follow-up through standardized forms and digitalization would provide the reliable data needed to develop national cleft protocols tailored to local realities. This ensures that care is both evidence-based and adapted to the specific needs of the health system.
4. Patients and Communities: Culturally sensitive community engagement is essential to improve early presentation and sustained follow-up.
With a range of different ethnic groups, Guatemala is a culturally diverse country. Addressing cultural barriers, including beliefs about surgery and the role of traditional medicine, is essential to improving access to cleft care. Enhancing health literacy through culturally sensitive education and multilingual materials can promote early intervention and informed decision-making. Furthermore, recognizing the opportunity costs families face, such as lost income, travel, and lodging, can inform the design of financial support strategies that reduce barriers to accessing timely and continuous care.
Limitations
As with any retrospective cohort study, several limitations must be acknowledged, including potential selection bias, incomplete records, and unmeasured confounding. Patients in the Guatemalan cohort were treated through a mission-based surgical center, which may disproportionately represent individuals with access to outreach services or those prioritized by external providers; those without access to such systems may be underrepresented.
Differences in healthcare delivery models introduce additional sources of bias in outcome assessment. Variables such as VPI and fistula presence rely on consistent follow-up and access to specialized diagnostic services, which vary significantly across settings. The absence of standardized outcome measurement tools and limited availability of speech or audiologic evaluations, particularly in Guatemala, may contribute to differential misclassification and underreporting. Additionally, sociodemographic data were not uniformly collected between cohorts, limiting the ability to adjust for contextual factors that may influence care and outcomes. Furthermore, the Veau classification system, while widely used, does not account for iCL or alveolus involvement, or the morphological severity of palatal clefts, potentially oversimplifying anatomical differences.
Conclusion
This comparative study highlights marked disparities in the timing and quality of CLP care, with Guatemalan patients experiencing substantial delays in primary repair. These differences appear rooted in constraints within the health system, including surgeon scarcity, fragmented referral systems, and reliance on episodic NGO interventions. To reduce these disparities, we propose a diagonal care model that integrates sustainable capacity-building, infrastructure investment, and locally adapted referral protocols. By emphasizing policy commitment, provider training, task-sharing, and culturally responsive patient engagement, this model aims to improve access, quality, and continuity of cleft care in Guatemala.
Future research should prioritize prospective, multicenter studies with standardized outcome measures, including functional assessments of speech, hearing, and psychosocial development. Longitudinal data collection will strengthen outcome monitoring and guide quality improvement. To enhance generalizability and address current limitations, future studies should include patient populations from multiple NGOs and outreach programs across Guatemala, particularly in rural and Indigenous communities, to ensure broader representation of children with orofacial clefts. Ultimately, establishing nationally integrated, multidisciplinary cleft programs is essential for achieving equitable and sustainable care. These efforts must engage local patients, providers, and policymakers to ensure that interventions are culturally relevant, context-sensitive, and designed for long-term impact in resource-limited settings.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr. Liping Du, PhD, from the Department of Biostatistics, Vanderbilt University Medical Center, for her valuable support in data analysis.
Ethical Approval and Informed Consent Statements
This study was approved by the Institutional Review Board at Vanderbilt University Medical Center (VUMC) (Approval No. 250048), which granted a waiver of informed consent due to the nature of the study. Patient data was de-identified to ensure confidentiality. Data was handled and stored in accordance with ethical standards, with oversight from the Principal Investigator and a trained clinical research coordinator to ensure study quality and safety.
Contributions
E. Tuchez and J.D. Rojas contributed equally to this study, leading conceptualization, design, and data curation including extraction, cleaning, and coding. They performed formal statistical analyses using R, managed project administration, coordinated data collection across Vanderbilt University Medical Center and Moore Pediatric Surgery Center, and contributed to methodology development. Both supervised, validated data accuracy, created visualizations for data presentation in R, and drafted and edited the manuscript.
K. Patel, as the research coordinator, coordinated manual and electronic data review, supported investigation and methodology, managed logistics and resources between sites, supervised data collection, and reviewed and edited the manuscript.
S. Zhao executed data preprocessing and coding procedures, carried out statistical analyses in R, verified data integrity, and developed visual representations of the findings using R.
R. Sanchez contributed to conceptual framing, supervised and validated research activities, and reviewed the manuscript.
R. Belcher provided guidance on the conceptual direction of the study, ensured the rigor of data analytic methods, and contributed to the revision of the manuscript.
J. Phillips, as the senior author, provided overarching conceptual guidance and methodological oversight, secured and managed key resources across both institutions, supervised study execution, ensured validation of analytic methods, and contributed to critical revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.