
Abstract
Objective
To identify different cost categories incurred by the parent and child born with an orofacial cleft from birth to 20 years of age in the United Kingdom.
Design
Focus groups were used to explore different cost categories associated with cleft care based on participants' personal experiences at different stages of the cleft care pathway.
Setting: Conducted online using Microsoft Teams.
Participants
Parents of children born with unilateral cleft lip and palate, bilateral cleft lip and palate, and cleft palate were recruited from the Cleft Collective UK and the Cleft Lip and Palate Association support group.
Interventions
Two focus groups were used to identify cost categories within the ages 0–10 years (n = 5) and 11–20 years (n = 4) of the cleft care pathway.
Main Outcome Measure: Qualitative assessment identified hierarchical direct and indirect cost categories for each focus group.
Results
The main direct costs incurred originated from travel, overnight accommodation, childcare, food, equipment, private treatment, and costs originating from encouraging inclusivity for the child. The main indirect costs originated from the loss of earnings due to time out of work, and time out of school for the child. Similar cost categories were identified in both focus groups.
Conclusion
Families incur numerous direct and indirect costs for cleft care from birth to adulthood. The different categories of costs identified will inform the development of quantitative instruments that will allow a better understanding of the true financial burden of cleft care for the parent and child in the United Kingdom.
Introduction
Orofacial clefts occur in 1 in every 700 live births in the United Kingdom, making it the most common craniofacial abnormality. 1 A child born with a cleft requires long-term multidisciplinary treatment, including input from surgeons, speech and language therapists, audiologists, pediatric dentists, orthodontists, prosthodontists, social care workers, and psychologists. The main aims of the numerous surgical and non-surgical treatment interventions are to establish good function during speech, eating, and swallowing; good facial appearance; a functional, stable, and aesthetic occlusion; and good hearing. These interventions from birth through to adulthood entail costs for the healthcare system, the affected child, and their parents.
In the United Kingdom, the National Health Service (NHS) is the universal system of healthcare delivery, where the state covers the costs of treatment at the point of accessing that care. Resources and expertise for cleft care are concentrated at national “hub” centers, with operators that carry out cleft-related procedures routinely. Smaller local hospitals or primary care settings that provide outpatient appointments related to cleft care are termed “spoke” centers. A summary of the cleft care pathway, including the appropriate locality for care at various stages within the “hub” and “spoke” settings within the United Kingdom, is demonstrated in Figure 1. (adapted from NHSEngland 2013)
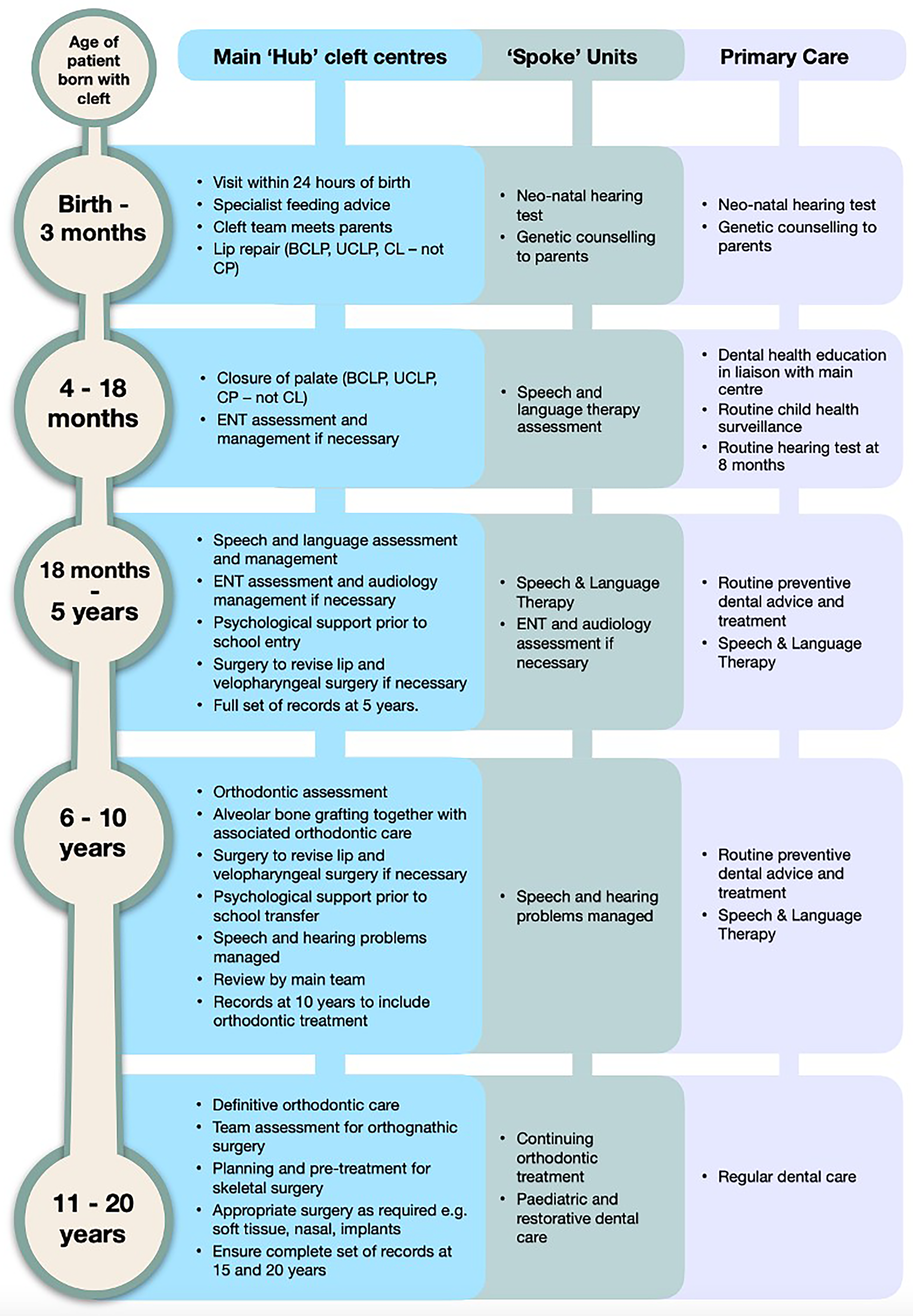
Care pathway flow diagram.
Recent studies within the United Kingdom have assessed the costs of cleft care to the NHS for children born with unilateral cleft lip and palate (UCLP), bilateral cleft lip and palate (BCLP), and cleft palate (CP) only across various age ranges.2,3 These studies provide a retrospective understanding of the main financial costs incurred by the healthcare system for cleft care for the above three phenotypes, from birth to 20 years of age. The biggest cost drivers found are the overheads associated with theatres and outpatient appointments, staff costs, the need for repeat surgery, and the cost of overnight stays in hospital.
Souster 3 estimated the basic financial costs to the families of a child with a UCLP from birth to 5 years, travel costs, and costs due to loss of earnings. Recommendations for further research included that “a study to assess the true cost to the families with input from patient/public involvement would benefit our understanding and potentially make the burden of care easier.”
Previous health economic studies have investigated the cost of cleft care from the perspective of the healthcare system extensively.3–5 Yet, despite the prevalence of CLP, a paucity of information exists on the cost of cleft care from a personal perspective, for the patients and parents/carers. Cost-of-illness studies with a personal perspective highlight a range of direct and indirect costs that are frequently incurred throughout the treatment journey of other childhood conditions. 6
To date, there has been no prior study within the United Kingdom that has reported on the different categories of costs of cleft care incurred by the patient and parents/guardians as a child progresses from birth through to adulthood. Identifying these categories is important for understanding the financial burdens of families and allowing for accurate investigations into quantifying the actual costs incurred over the cleft care pathway.
Aims and Objectives
To identify the different cost categories experienced by the patient/parent of children born in the United Kingdom with orofacial cleft from birth to 20 years of age.
Methods
The initial plans for this study were informed through patient and public involvement (PPI), and the study was undertaken during the period of the COVID-19 pandemic. The project proposal was presented at the CLAPA Cleft Collective Patient Consultation Group Meeting in July 2021.
The Cleft Collective Study is “a large prospective cohort study of children born with cleft lip and/or palate (CL/P), investigating causes of cleft, the best treatments, and the impact of cleft on those affected and their families. The resource comprises biological samples, speech audio recordings, medical and educational records and parent and child completed questionnaires. The resource is available for clinical and academic communities to access and use to address a range of cleft related research questions”. 7 The Cleft Collective currently has data available for patients aged 0–13 years.
The Cleft Lip and Palate Association (CLAPA) is a UK-wide voluntary organization that provides support to individuals and families affected by orofacial clefts from birth through to adulthood. Set up in 1979, CLAPA provides information and advice to affected families and plays a role in advising and encouraging further cleft research through patient and public involvement. Some of the services provided include a vibrant social media network for the cleft community, online support groups, and community social events. 8 Members of CLAPA represent all age ranges, from birth through to adulthood. Both the Cleft Collective and CLAPA allow potential access to a large dataset of families in the United Kingdom affected with an orofacial cleft.
A qualitative focus group method was employed to investigate the different cost categories associated with cleft care based on participants’ personal experiences at different stages of the cleft care pathway. The qualitative method of research was used to gain a deep understanding of certain human beliefs, behaviors, or attitudes, including people's personal perspectives. 9 The focus group method used group dynamics to gather information on collective views and provided depth and insight into specific beliefs and experiences. 10
The aim of this qualitative work was to understand individuals’ lived experiences of the costs incurred in relation to their or their child's cleft care, for these findings to later enable the development of a quantitative instrument (online questionnaire), to be used to accurately capture actual expenditure related to the identified cost categories.
Ethical approval of the study was granted by the Faculty of Health Sciences Research Ethics Committee at the University of Bristol 04.11.2021 (Reference Number: 0128).
Inclusion/Exclusion Criteria
Inclusion criteria:
Parents of children (0–20 years), and adults aged 16–20 years, born with either UCLP, BCLP, or CP by diagnosis in the United Kingdom, and Parents of children (0–20 years), and adults aged 16–20 years registered in the Cleft Collective (0–13 years) and/or CLAPA (0–20 years).
Exclusion criteria:
Individuals who presented with a diagnosed or suspected syndrome associated with the orofacial clefting, or Individuals who have moved away from or into the United Kingdom and whose care has been transferred to or from another Cleft Team outside of the National Health Service.
Participant Sampling and Recruitment
Purposive quota sampling was used to recruit participants at different stages of the cleft care pathway (children of different ages) and with different cleft phenotypes. This approach was employed to deliberately select individuals with characteristics of interest from the population to contribute to the investigation. 11 The target population for participation in the focus groups was parents with a child born with UCLP, BCLP, or CP, and adults aged 16–20 years born with a cleft. Participants were recruited from the Cleft Collective UK and from the Cleft Lip and Palate Association support group, CLAPA. The age range of participants accessible through the Cleft Collective was parents of children born with a cleft from 0 to 13 years of age. The age range of participants accessible through CLAPA included parents of children born with a cleft aged 0–20 years, and adults aged 16–20 years born with a cleft. The rationale for recruiting participants via both the Cleft Collective and CLAPA was to gain access to a wide range of participants who fell into our inclusion criteria for participant selection. The Cleft Collective and CLAPA agreed to share the research recruitment advertisement via their social media networks.
The participants were recruited to form distinct groups that were defined by age:
Parents of children born with a cleft aged under 10, Parents of children born with cleft aged 10–20 and individuals themselves aged 16–20
It was important to recruit participants in these groups to reflect very different stages of treatment experience and identify any differences in the types of costs across the different age ranges. Participants were selected to ensure that a mix of the cleft phenotypes and ages of children born with clefts were represented within each group. These groups then formed separate focus groups during the data collection phase to facilitate the emergence of potentially different cost categories across the groups. The selected participants were sent an invitation to the online Microsoft Teams meeting and an “e-consent” form to complete and return via email prior to the meeting date.
Data Collection
Focus groups were conducted online using the University of Bristol Microsoft Teams (Version 1.4.00.35562). A distress protocol and topic guide were prepared for the focus group discussions. The topic guide was developed using the direct and indirect costs of childhood illness that were commonly identified through the literature review. The direct costs (which are expenses directly tied to the need for medical care) were travel costs, childcare, foodstuffs, overnight stays, and any other direct costs. The indirect costs (which are a consequence of a health condition, but not directly tied to medical care) identified were loss of earnings for parents, less time in education for the child, and any other indirect costs. The topic guide was used to guide the conversation and allow the conversation to go beyond the topics from the literature review.
With permission from the participants, data were collected via video-recorded focus group interviews and subsequently uploaded to the secure, encrypted University server.
Data Transcription and Qualitative Analysis
The focus groups were initially transcribed via the automated transcription function on Microsoft Teams (Version 1.4.00.35562) and uploaded to the secure University of Bristol server. The lead researcher edited the transcript on Microsoft Word 2016 (Microsoft, Redmond, Washington, USA) cross-referencing and checking the focus group audio against the automated transcription. Each participant was given an individual participant identification for anonymization (ie, P1, P2, P3 etc) prior to data analysis. Inductive thematic analysis was carried out using the Braun and Clarke approach 12 as subsequently described. Firstly, the transcripts were read individually by the lead researcher and co-supervisor, to allow familiarization with the data. The transcribed data were imported into QSR NVivo 12 Software (QSR International) and independently coded to reduce single researcher bias. The coding was then reviewed between the lead researcher and co-supervisor to strengthen validity. Through reviewing collections of codes relevant to the research question, overarching themes were subsequently generated. Themes were evaluated by reviewing the themes against the coded data and reviewing the themes for clarity with the research co-supervisor. Coding structures were constructed for each focus group; a helpful visualization technique that allows clear visualization of the various hierarchical categories and overlapping codes within the data on a single page.
Results
Participant Characteristics
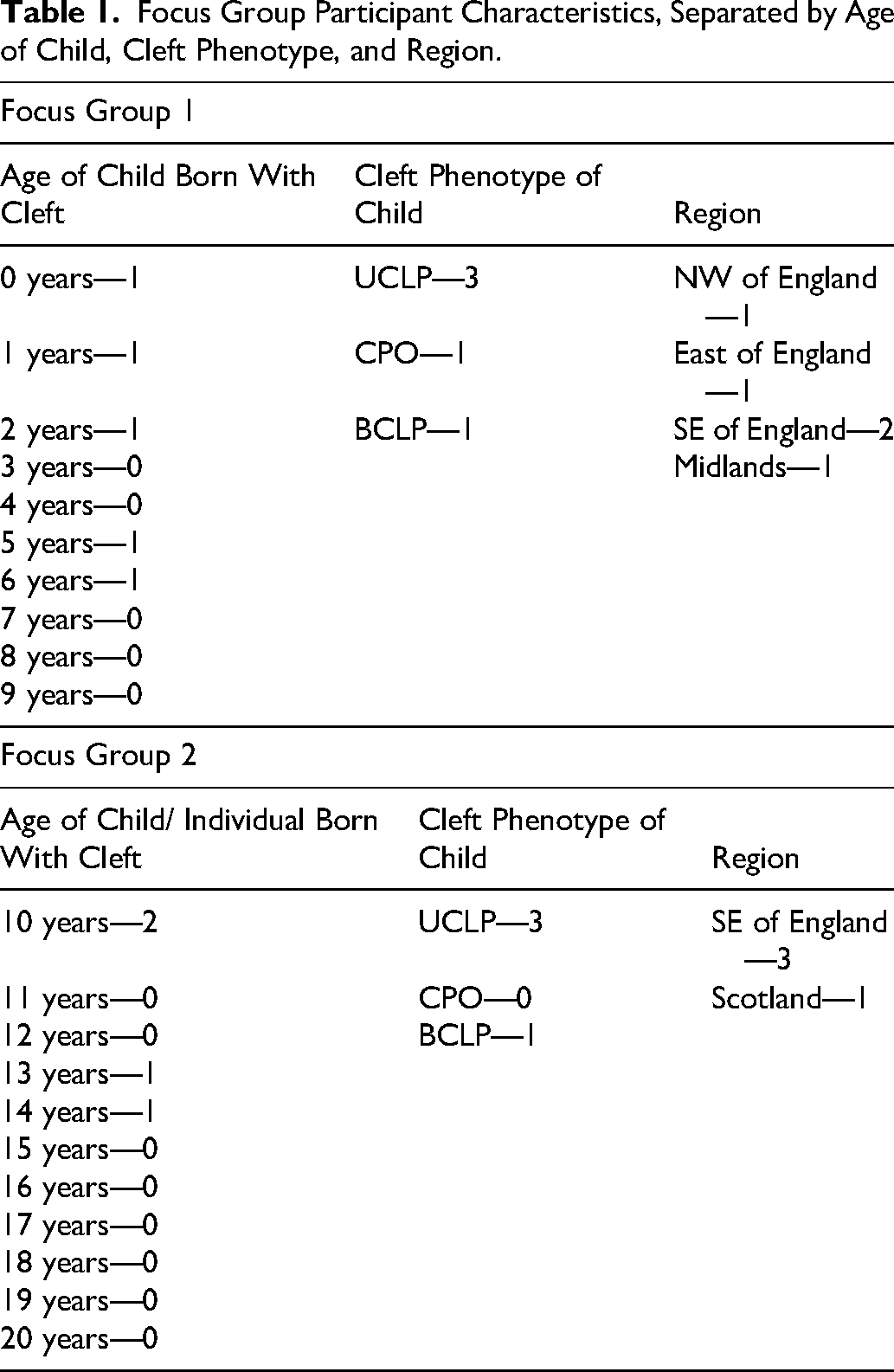
Two focus groups were conducted, with five participants in each. The participants in focus group 1 were all mothers of children born with cleft lip and/or palate under 10 years of age. The participants recruited were purposely selected such that the mix of focus group participants would represent all three cleft phenotypes: UCLP, BCLP, and CP. The participants in focus group 2 were all mothers of children born with cleft lip and/or palate aged 10 years or over and represented two of the three phenotypes: UCLP and BCLP. One participant who had a child born with CP was unable to attend on the day. The participants were purposely recruited nationally, and as such, they are located from a mix of regions across the country (see Table 1).
Focus Group Participant Characteristics, Separated by Age of Child, Cleft Phenotype, and Region.
Coding Structures of Different Categories of Cost Divided into Direct and Indirect Costs
The participants in both focus groups discussed the costs that they had incurred in relation to the cleft care for their child. The coding structure of costs discussed in focus group 1 has been summarized in Figure 2, and those discussed in focus group 2 are summarized in Figure 3. The costs that had been amplified because of the COVID-19 pandemic have been highlighted in the pink box within Figure 2.
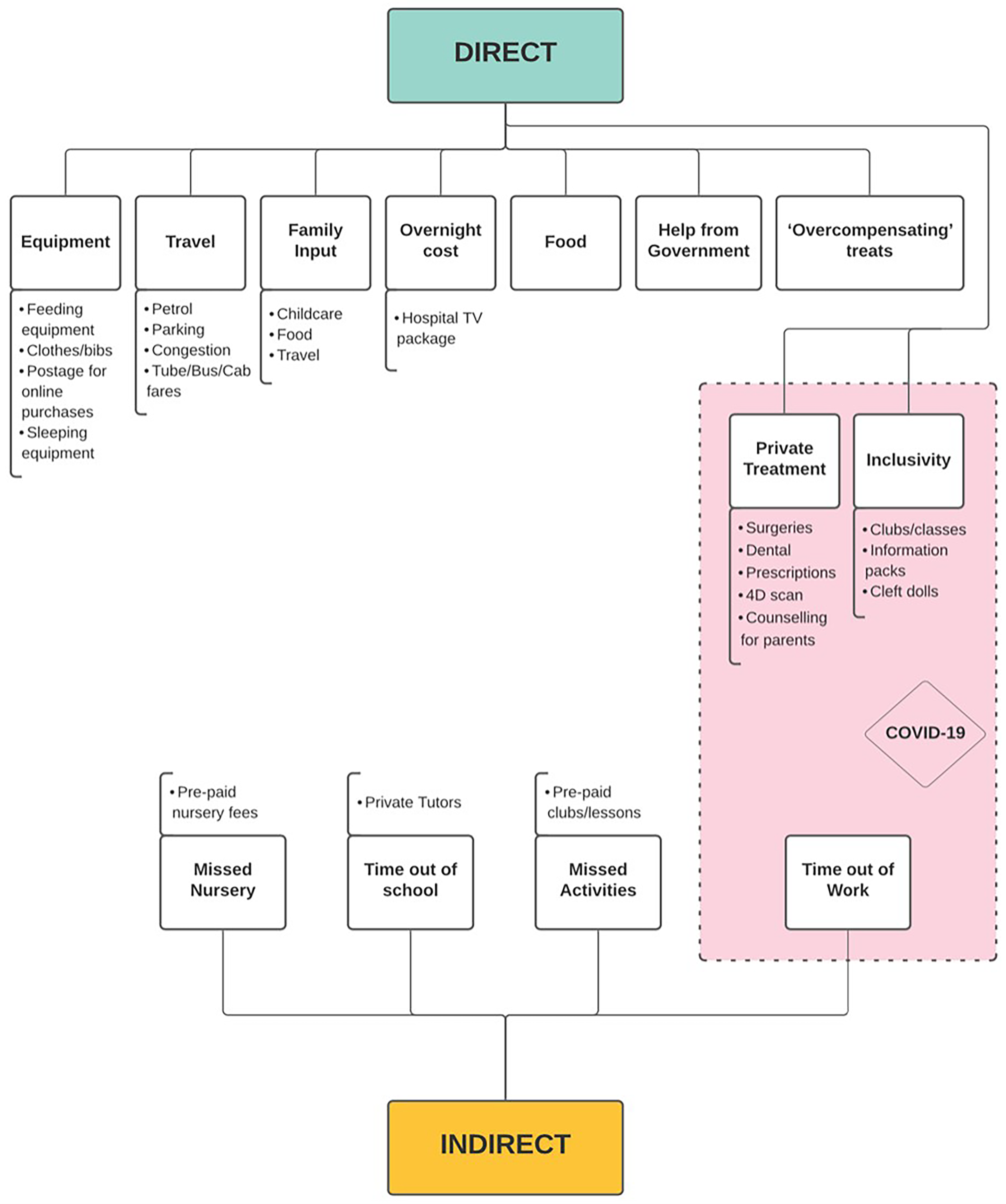
Focus group 1 (0–10 years) coding structure of costs.
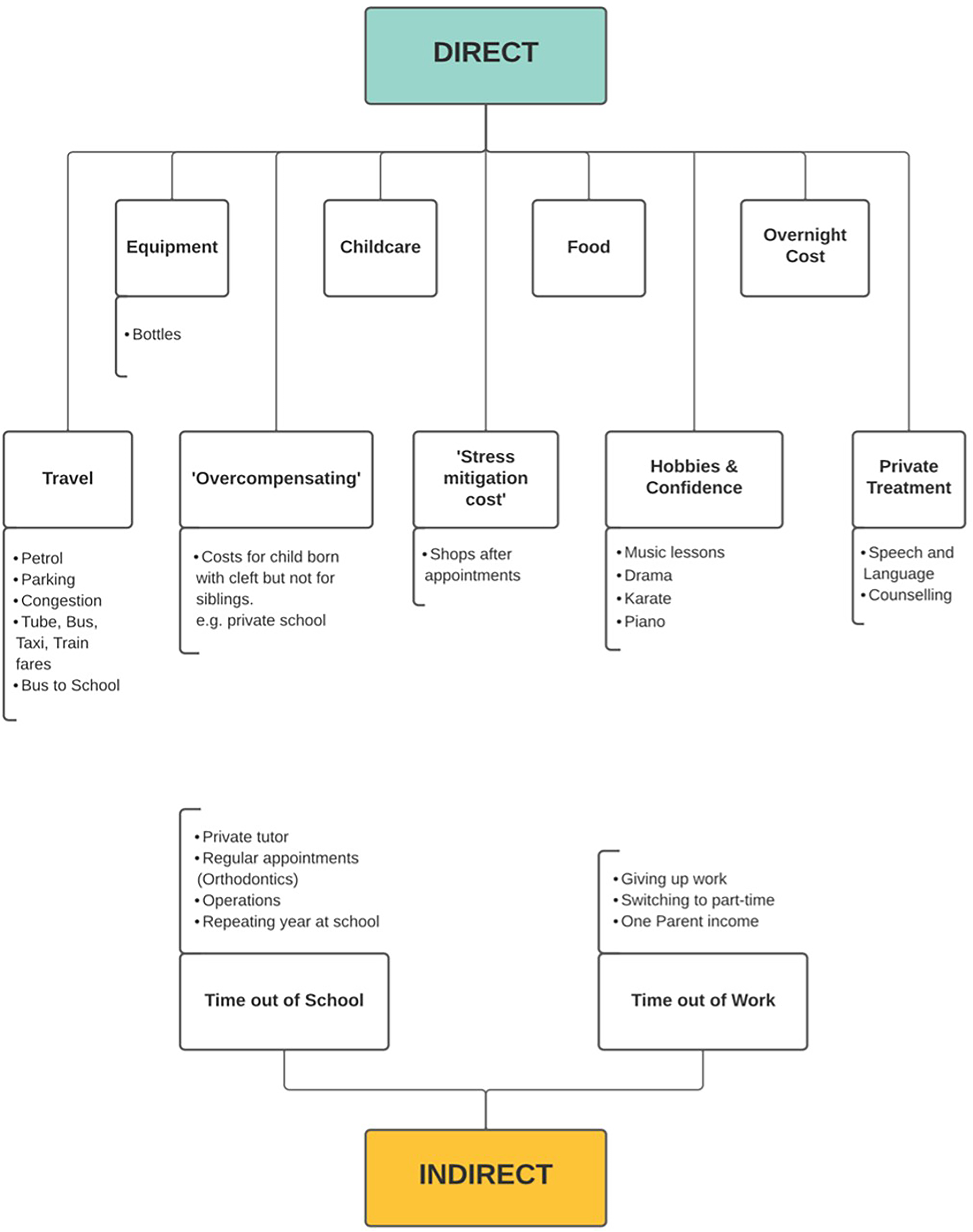
Focus group 2 (11–20 years) coding structure of costs.
Cost Categories
Overall, the different categories of costs identified were divided into two costs:
Direct Costs
Participants from both focus groups mentioned the following
All participants across both focus groups discussed travel costs associated with their child's cleft care. The different types of travel costs identified included fuel, parking, congestion fees, and tube/bus/taxi/train fares. One participant shared their experience of unforeseen parking costs associated with a prolonged stay in hospital. P2 (focus group 1): “… our car was in the car park for two weeks and you can imagine what the price was. I think about £100, £200, £300 ….” P1 (focus group 1): “It's like an hour on a good day, but before now we've had appointments at like 9:00 o'clock in the morning. So, because it's been rush hour, it's taking like 2 h to get there so that's the petrol….” P3 (focus group 1): “I do have the help of his grandmother. She lives a good hour and 15 min away, so she has driven around the motorway to come and look after him and stay overnight with operations and things ….” P4 (focus group 1): “we now do overnight hotel stays …. 'Cause if you've got to be there at 7:00 AM, you're not going to get up at 3:00 in the morning and drive - early morning operations, they usually are, and that's a bit of a distance.” P4 (focus group 1): “when we did the operations, I do remember just eating the hospital food in, and it was quite pricey. But yeah, now we just try and take as much with us.” P2 (focus group 1): “We have gone through about one hundred teats in two years and then again you do have to get the different flow ones, from flow 1, 2 and 3 […] I paid £60 for an expressing machine at home.” P3 (focus group 1): “So when we go out and about, because people look at her, I make sure she wears nicer clothes or I feel like I need to spend a little bit more on her to make sure her appearance is right.” P6 (focus group 2): “He [son born with cleft] got a private school for three years and the other two [children] went to the state school. So, you know, financially and emotionally, you're sort of almost taking stuff away from the other children, aren't you?” P7 (focus group 2): “You know, I'm sure some of you will get this, to try and mitigate that by saying ‘well after we go, we’ll go to the bookshop, or we’ll do something’ and so there isn't just that - the travel cost. There's the kind of stress mitigation cost. And that is, that is huge.” P6 (focus group 2): “We've had this private speech therapy for [son born with cleft] ….” P7 (focus group 2): “I pay £360 a month on counselling, I pay £60 a session because we don’t have any access to any at [hospital] and she started self-harming, my daughter…..” P3 (focus group 1): “I bought a lot of books basically for the children at school.” P7 (focus group 2): “So we paid hundreds and hundreds and hundreds of music lessons …. They told us to get her to do two handed tasks so we did the karate, we've done the piano …. And to find really good extracurricular clubs that are inclusive, they cost money where the teachers are going to be interested in how to support your child, and making sure they're not easily isolated … because she does look different …. And all these things cost money.” P1 (focus group 1): “when I was in hospital, we was in for five days so I bought the TV as well. Um, ‘cause I think as well, you can go a bit stir crazy if you sit there.”
Indirect Costs
Participants from both focus groups mentioned the same
Two participants in focus group 1 explained they felt their money seemed to be wasted on nursery fees because of their child missing nursery for hospital appointments, for surgery, and also due to cancelled hospital visits. P2 (focus group 1): “That's a loss of £600 because you pay upfront [for nursery] and it gets me and my boyfriend down so much that I know we can't help that he's been ill … we don't get it back so it's money, literally down the loo.” P4 (focus group 1): “But I am very concerned about his education. […] Well it's still early days, but if this continues in this way you know, am I going to have to hire a private tutor to just to make sure that we're staying on top, ‘cause I don't want him suffering ‘cause he's in and out so much, you know?” P7 (focus group 2): “My daughter had to repeat a year at school, so a lot of time has been spent catching her up with her education. She doesn't come home from school and do nothing, she comes home from school and she has to work to keep up with and to not fall behind ….” P4 (focus group 1): “You know, we've got to usually take 1/2 day or whole day off work to do it [go to a hospital appointment]. P3 (focus group 1): “you can't rearrange those appointments around your working hours. So, I made the decision to go part time and so I try and get all of her appointments on the days I do, and if I can't, my husband takes the time off work to go.” P4 (focus group 1): “But it's more of an impact on … my potential for growth and development any way in my role, because I then become known as this person that's gonna constantly be going off for medical appointments with my son and therefore people aren't very keen on promoting you or pushing you up the chain or putting you in for other roles, because you'll be known as someone that needs you know, extra time off, and that's not very popular usually in companies ….” P9 (focus group 2): “… there's no way we could have both worked full time and managed all those appointments. Just ‘cause we don't have any family support.” P7 (focus group 2): “I have to be there for emotional support when she comes home from school, because sometimes she's had stuff that's not been very kind towards her.”
The Impact of COVID-19
All participants in focus group 1 shared that the COVID-19 pandemic had an extra impact on the costs incurred throughout cleft care for their child. The largest cost included parents opting to pay privately for surgery or treatment due to delays or cancellations within the NHS system during the pandemic. Two participants paid for private surgery to avoid the negative impact that delayed surgery would have on their child's speech or hearing. P5: “… because of the pandemic and we were told that he would be sort of 18 months by the time that he would probably have his lip operation - which would then impact the palate operation and so his speech, we did actually opt to go privately for his first operation.”
Discussion
This study provides a unique insight into the identification of different categories of costs associated with cleft care to the parent and child. Focus groups with parents of children aged 0 to 14 born with orofacial cleft were employed to capture families’ lived experiences of the costs of cleft care in the United Kingdom. This method of data collection allowed us to identify a range of costs incurred by families throughout the cleft care pathway. Participants from both focus groups mentioned the following direct costs: private treatment, travel, overnight stays, childcare, food, equipment, and the costs associated with inclusivity/ hobbies and confidence and overcompensating for their child born with a cleft. The indirect costs that the participants from both groups had incurred included time out of work and time out of school for their child. Participants from both groups mentioned paying for or considering paying for a private tutor.
Regarding “overcompensating costs,” such as paying extra for treats or purchases for their child specifically because of their cleft, participants in focus group 1 described this cost in relation to paying for treats, whilst the participants in focus group 2 mentioned the cost of paying for private school for their child born with a cleft but not for the child's other siblings. Whilst the participants in focus group 1 mentioned numerous costs associated with equipment, this was not echoed as strongly in focus group 2 discussion. This is likely a reflection of the difference in treatment experience throughout cleft care between parents of younger children and older children respectively.
Several costs mentioned by focus group 1 participants that were not mentioned in focus group 2 included the cost of the TV package when staying in hospital, missed nursery fees, costs associated with missed activities and the need for financial help from the government. A cost category mentioned solely in focus group 2 was a “stress mitigation cost.” This difference between groups is likely due to participants reporting on their most recent experiences. All of these mentioned costs are new to the parents of younger children, with a new or unforeseen burden leading to these parents mentioning the need for financial help from the government. Parents of older children may not recall costs associated with earlier years, including missed nursery fees or TV package whilst staying in hospital. The stress mitigation cost may be more relevant for the older child affected with a cleft, who has been through more appointments and surgeries, can ask more questions and perhaps requires more reassurance from the parent.
Studies conducted on treatment experiences have highlighted several issues that may indicate inadvertent costs are being encountered by the affected families. A survey led by the CLAPA investigated parents’ experiences and perspectives of their child's cleft care. 13 The survey disclosed that feeding bottles were unavailable on 70% of maternity wards, implying a delay in establishing successful feeding; a cost implication for purchasing feeding bottles and the need for extra stay in hospital. Furthermore, it was found that not all parents had been offered overnight accommodation when their child had to be in hospital for surgery, which they should be entitled to. The Care of Children in Hospital (Health Service Circular (HSC) 1998/238) requires that: “Accommodation is provided for them to remain with their children overnight if they so wish”. 14
A qualitative study assessing the dental treatment experiences of adults born with CL/P in the United Kingdom highlighted certain issues with regard to treatment access. 15 Through focus group discussions with 24 adults with CL/P, the study identified that participants had a limited understanding surrounding their oral health and dental treatment and were also largely unaware of their entitlement to local and specialist NHS-funded dental treatment. As a result, participants felt that “patients with CL/P could be vulnerable to financial exploitation by private dental clinics”. The study's findings may be even more relevant with a recent report indicating that 8 in 10 dental practices across the United Kingdom are not accepting new NHS-funded child patients. 16
Furthermore, a qualitative study exploring the impact of missing school to attend orthodontic appointments described that orthodontic appointments arranged at the end of the school day were associated with additional childcare costs for siblings. 17
A whole life survey published in 2021 investigated treatment experiences of adults born with cleft lip and/or palate in the United Kingdom. A section of this survey explored participants’ awareness of their entitlement to NHS services. From a total of 207 participants included in the survey, 41.4% were unaware that they were eligible for CLP-specific treatment under the NHS. Furthermore, 16.7% participants had paid for private treatment, mostly related to general dentistry, orthodontic, and restorative dental treatment. Almost half of the participants reported ongoing concerns with their dental treatment outcomes, with one of the reported reasons being the cost of future procedures. Additionally, examples of reported reasons for refusing a surgical or dental procedure that was offered to them included time out of work and study, and the costs outweighing the benefits. 18 The results reported from the above surveys highlight a fundamental issue: families are incurring extra costs for cleft care that have not been investigated and could be avoided.
In this study, both groups mentioned private treatment costs they had incurred. However, the specific types of treatments paid for were different between the groups, and there were different reasons for why private treatments were sought. Focus group 1 participants mentioned paying privately for surgeries, dental care, prescriptions, a 4D scan, and counselling for the parents, whilst focus group 2 participants mentioned paying privately for counselling for their child and for speech and language therapy. Private dental care and counselling were sought because these participants were not aware of the availability of this service under the NHS, and another participant found it difficult to obtain access to these services via the NHS. It is possible that parents with younger children may not be aware of the NHS dental services available to them.
Recently, the COVID-19 pandemic in 2020 caused disruption to the provision of healthcare services globally and placed significant pressure on NHS services in the United Kingdom. The impact of the pandemic on routine cleft services in the United Kingdom included delays to surgery, the suspension of outpatient appointments, and introduction of telehealth. A qualitative study on the impact of the pandemic on cleft service delivery in the United Kingdom reported that some families had decided to pay privately for their child's primary CL/P operation(s). 19 A recent systematic review on the effect of telehealth on the cost of health care during the COVID-19 pandemic reported decreased patient health care costs, but this was variable dependent upon the telehealth service and further research is required to determine long-term cost savings. 20 In this study, the COVID-19 pandemic appeared to impact participants with younger children (focus group 1) more heavily than those participants with older children (focus group 2) in terms of the types of costs incurred. This is most likely because these families were in the earlier stages of their cleft care journey, managing with establishing feeding and the numerous initial operations. One participant explained that delays to their child's surgeries could result in a negative knock-on effect on other aspects of their child's life, such as issues with hearing impacting progression in education for the child. Delays in the NHS system, specifically as a result of the pandemic, meant that these families had to incur more private costs to access surgery in a timely manner. Furthermore, participants in focus group 1 mentioned increased time out of work. This time out of work is likely to have had an impact on reduced income either through reduced hours or longer maternity leave. Participants in focus group 1 also mentioned the lost money that had been spent on activities related to inclusivity for their child due to the pandemic, such as clubs and classes. However, the only mention of the pandemic within the focus group 2 discussion was surrounding themes of isolation and loneliness for their child, but this was not directly attributed to any specific costs incurred in this group. However, these costs might also have been true of children without a cleft.
Strengths and Limitations
This study has highlighted the importance of considering the patient perspective in economic evaluations of interventions within cleft care pathways. Firstly, the study has been strengthened by consulting patient and public involvement from the outset in this research. Obtaining insights from cleft representatives, who have lived experiences of cleft care in the United Kingdom, has allowed the research to be more relevant to the experiences and needs of patients. Secondly, recruitment via both CLAPA and the Cleft Collective has allowed access to a wide pool of participants representing different cleft phenotypes and ages across the United Kingdom. Additionally, the use of online focus groups allowed data to be captured from a geographically diverse range of families and age groups affected by cleft care across the country. The qualitative approach and examination of both direct and indirect costs through focus groups is relevant to families’ lived experiences and allowed a comprehensive capture of different cost categories.
However, a limitation associated with the recruitment of participants from the Cleft Collective and CLAPA has meant that the population who have responded to the study are families that already engage in cleft-related research and the cleft community. The respondents were primarily female, and it is unknown if their perspectives were similar to those of their partners. Furthermore, there were no respondents from individuals aged 16–20 years born with orofacial clefts themselves, as all respondents were parents of a child born with a cleft. According to the External Engagement Coordinator at CLAPA, survey responses from members often have a bias toward white females. CLAPA are currently looking at how to increase the diversity of those who engage with CLAPA, but this is not at the stage of reporting yet. The Cleft Collective sample is broadly representative of the proportions of cleft subtypes in the United Kingdom cleft population and according to unpublished work by the Cleft Collective “has a uniform distribution when describing deprivation levels of participants using the Index of Multiple Deprivation”. Perhaps the perceived financial “costs” might vary based on the financial status of the parental respondents; however, this information was not collected. Additionally, the impact of the COVID-19 pandemic possibly makes interpretation of the different types of cleft care costs more difficult.
Future Work
This study has identified the different categories of costs incurred throughout the cleft care journey from the perspective of the parent and child. The findings from the focus group interviews will inform the development of a quantitative survey to accurately capture the actual expenditure of both the direct and indirect costs of cleft care to the patient and parent, from 0 to 20 years of age.
Conclusions
This study has identified different cost categories which can be divided into direct and indirect costs for cleft care from birth through to adulthood in the United Kingdom, enabling future investigations to accurately quantitively capture expenditure of the patient and parent at different stages of the United Kingdom cleft care pathway.
Footnotes
Acknowledgments
We wish to acknowledge the Cleft Collective and Cleft Lip and Palate Association for their assistance with study feedback and participant recruitment.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.