
Abstract
Objective
Evidence suggests that cleft lip and/or palate can have significant psychosocial impacts on adults’ lives beyond the end of the standard treatment pathway. Although some studies indicate gender differences, no research has specifically explored the experiences of women with cleft. This study aimed to explore the stories told by women about their adult experiences of cleft, for discussion informed by intersectionality theory.
Design
Participants were interviewed using a narrative, photo elicitation approach. Each participant brought photos they felt represented their story to an unstructured interview, which was recorded and transcribed verbatim. Data were subject to narrative analysis.
Setting
Interviews took place on Microsoft Teams video call, with photos shared on-screen throughout, and lasted an average of 94 min.
Participants
Fourteen women born with cleft aged 20 to 72 living in the United States or United Kingdom took part.
Results
Six overarching discourses were identified and presented alongside 14 individual narrative synopses, depicting converging stories told by each participant throughout their interview. These were (1) enduring, (2) hiding, (3) striving, (4) healing, (5) reclaiming, and (6) reconciling.
Conclusions
Viewing cleft through an intersectional lens offers important insights into the lived and living experiences of adults navigating treatment and the ongoing psychosocial impact of cleft. The findings suggest that expectations and pressures placed on women by society are compounded by, rather than exist in parallel with, the ongoing impact of cleft.
Keywords
Introduction
Treatment of cleft lip and/or palate (“cleft”) is primarily surgical, with procedures carried out during infancy commonly referred to in medical and public discourse as lip and/or palate repairs 1 (italics added). Cleft can impact an individual's speech, hearing, and physical appearance and requires multidisciplinary team treatment. The past decade has seen increased focus and attention on the residual emotional needs of adults within the cleft community, who perhaps do not feel as “repaired” as the medicalized lens might suggest. Adults have reported low mood, 2 dissatisfaction with appearance, 3 treatment anxiety and difficulties accessing further treatment, 4 symptoms of traumatic stress, 5 social anxiety, and challenges in intimate relationships.6,7 Recommendations to support adults with cleft have included greater access to psychology support, 8 routine and early screening for emotional distress in clinic settings, 2 targeted support and resources for individuals experiencing bullying or discrimination, 6 and awareness among teams of the burden of invasive and often appearance-altering treatment. 4
Many studies of the psychosocial impact of cleft on adults are quantitative and conducted within preset parameters such as life satisfaction and treatment outcomes, providing helpful foundations for understanding the potential needs of this previously understudied population.9–11 One study highlighted that for a group of adults, talking positively about their difference in childhood, the presence of close friends, feeling confident in talking about cleft, and the ability to feel comfortable in public places all positively impacted on their psychological adjustment. 11 These latter associations illustrate a link between cleft and shame and sense of social safety. Indeed, results of other studies indicate the presence of shameful feelings among adults with cleft, with participants reporting a need to develop strategies to minimize their cleft in social spaces such as by controlling the angles from which they are seen by others, 3 emphasizing other aspects of their public personas (such as being funny or working on their physical fitness) 12 or by avoiding engaging with others altogether. 7 Gilbert's 13 conceptualization of shame posits that shame is an internal state that can arise from external pressures to conform, leading to direct attacks by others and the self if one cannot meet the prescribed social standards.
Some groups who are typically afforded less power in society and are often under more pressure to conform, such as women, are more prone to shame and internalized negative ideas about themselves. 14 Furthermore, when one's need to be seen as socially attractive cannot be met, such as in the case of an individual who has been taught by their social context that their appearance and/or speech is unacceptable, shame persists and can lead to the types of avoidance and self-doubt already described in the cleft literature. 13
As more qualitative research is conducted, a complex and often dynamic picture of coping, adjusting, distress, and the impact of societal expectations on cleft-affected individuals emerges.15–17 This highlights that differences within the adult cleft population are important, and moving toward more holistic, intersectional considerations of adults navigating their contexts, including but not limited to their cleft, could yield important insights for clinicians supporting individuals with cleft.
Intersectionality Theory and Cleft
Intersectionality is the idea that characteristics that afford an individual a level of dis/advantage in society do not exist in isolation and can be compounded in a way which “creates obstacles that often are not understood among conventional ways of thinking.” 18 Applying this to disability, Wickenden 19 highlighted the gendered experiences of disabled individuals, whereby disabled women must contend not only with the stigma and objectification that so often comes with living in a body that looks “different” or disabled but also with oppressive assumptions about women's roles in society. Some women feel they have been denied credibility as women, given their disability which is the more prevalent identity, due to societal views on what constitutes femininity and these intersecting identities not being compatible.20,21
The impact that cleft can have on one's speech and appearance, coupled with evidence for cleft-related appearance dissatisfaction and longer-term psychological impact on adults indicate that these insights from intersectionality theory and research could be useful in understanding differences within the cleft community. In a study exploring a variety of visible differences, women reported finding it difficult to overcome a negative self-concept because of societal expectations and norms surrounding “attractiveness” and “femininity” 12 ; their appearance delegitimized their claim to a female identity. Although research exploring explicit gender differences in the psychosocial impact of cleft is scarce, women with cleft have reported more appearance-related social anxiety and avoidance than men with cleft. 16
Gender and Cleft in Existing Research
Some quantitative studies have reported lower life satisfaction and higher distress in women with cleft than in men.9,22 Similarly, in a qualitative study of adults’ experiences with cleft, themes around being attractive and of needing to conform to what someone of their gender “should” look like were more prevalent in female participants than male. Women in this study also made more comments about the burdensome nature of their cleft throughout their lives, whereas men spoke more of being “better off” or “lucky” to have a cleft than women. 17 Together, these findings may partially explain the finding that women with cleft have been reported to request and undergo more aesthetic lip and nose revision surgeries than men,23–25 possibly demonstrating a stark and tangible consequence of these gendered narratives. To date, qualitative research has not specifically studied adult women's narratives of cleft, such that these inferences about the roles of shame and intersectional identities might be explored further.
Aim of Current Research
Considering the evidence that there may be a gendered experience of cleft, this project invited women to share their lived and living experiences of being a woman with a cleft. In doing this, it aimed to lay foundations for understanding if and how intersecting gender and disability/appearance identities, along with narratives of shame, may be present among this population. This information is intended to inform care within and beyond cleft teams.
Research Question
What stories do women born with a cleft lip and/or palate tell about their lives and experiences of cleft?
Methods
Design
A qualitative design was employed, utilizing both photo elicitation and narrative interview methods of data collection. Participants were asked to collate photographs which told their story of living as a woman with cleft and were subsequently asked to relay this story in a life-story interview.
The researcher chose to combine narrative interviews with photo-elicitation methods to create a more holistic inquiry into women's lived experience of cleft. Narrative interviews offered an open platform for participants to share what felt most pertinent to their lives, 26 rather than restricting discussion to predetermined topics such as surgery, 27 emotional adjustment, 8 treatment satisfaction, 4 or appearance concern, 16 which might have felt limiting or irrelevant. In this way, the approach encompassed the breadth of lived and living experiences and sought to approach challenges without imposing frames such as resilience or coping, in line with trauma-informed principles. Photo-elicitation complemented this by encouraging emotional and detailed storytelling, 28 supporting memory, fostering dialogue, 29 and disrupting researcher-participant power dynamics. By collating photographs, the participant can prepare, ask questions of their lives and develop ideas about their narrative before the interview begins,30,31 thus making participants the “experts.” Importantly, the researchers acknowledged that many participants’ prior experiences of photography may be in medicalized contexts,32,33 or avoidance of photographs due to appearance concerns. 3 Using a visual methodology without necessitating pictures of the participants themselves was considered a counterweight to these possible prior experiences.
Researcher Reflexivity
The lead researcher and first author, a woman with a cleft (disclosed in participant materials), was motivated to conduct this study not only by professional interest and knowledge, but by lived experience and engagement with the cleft community. Together, these highlighted gaps in trauma-informed, holistic care which took characteristics such as gender into account. Insider status shaped recruitment, rapport, and data generation: disclosure and shared language sometimes facilitated access and richer accounts, and brief self-referential anecdotes were used to build trust and connection. 34 The researcher attended to the importance of balancing her own position as a facilitatory tool with privileging the unique stories of each participant, ensuring her position was a strength, rather than a limiter, to the project.
Epistemological Position
Photographs and stories provide access to lived experiences and individual truths, which are shaped by their beliefs and unique contexts. The researchers take a social constructionist view of knowledge: participants’ accounts are coconstructed through interaction between participant, their experiences, and the researcher, with meaning produced relationally and interpretively with respect to situational factors, rather than discovered as objective fact or absolute truth. 35
Expert by Experience Involvement
Health research that actively involves Expert by Experiences (EBEs) is generally acknowledged to be more relevant and sensitive to the needs of those who are most likely to be directly impacted by the work. 36 Within cleft research, calls to advance the field include an emphasis on engaging with EBEs at all stages of research. 37 The researcher worked with an EBE, a woman with a cleft living in the United States, to review materials, design the protocol, support recruitment and discussing this manuscript, conference presentations, and other dissemination efforts. This was facilitated using MS Teams calls approximately every 8 weeks.
Ethics
Ethical approval was granted by the Canterbury Christ Church University ethics committee (approval #ETH2324-0081). Written consent including permission to use images was obtained from all participants. Pseudonyms are used throughout this report. A debrief sheet including well-being advice was sent via email to each participant immediately after their interview.
Procedure
Recruitment
Participants were recruited via social media advertisements which were promoted by the Cleft Lip and Palate Association (CLAPA) 38 and Face Equality International. 39 An information sheet was provided via email to eligible participants detailing the methods, protocol, and framing of the project (see Table 1 for inclusion and exclusion criteria).
Inclusion and Exclusion Criteria.
Photography Period
After the initial call, participants were given 1 to 3 weeks to collate photographs which they could use to tell their story during their interview. This was deemed appropriate in leaving enough time to consider and produce the images while maintaining interest and engagement. Participants were not limited on how many photographs they should send or on whether they used preexisting or new photographs. The researcher did not look at photographs in the folders prior to the interview to avoid forming preconceptions of the data and to ensure the same procedure was followed for all participants.
Interviews
Interviews took place on Microsoft Teams video call, lasting between 61 and 118 min, with an average length of 94 min. The interview schedule allowed for open storytelling, conversation, and discussion (eg, “tell me the story behind this photo”). 40 Where participants indicated that they wanted further support to start or explain an element of their story, the researcher asked open questions about elements of what had already been said, thus not introducing any material that had not been provided by the participant. Interviews were recorded and transcribed verbatim.
Participants
Information was initially emailed to 37 women with a cleft who expressed an interest in participating, with reminder emails sent after 5 days if no response was received. Fourteen responded and opted to take part. Participant characteristics are outlined in Table 2.
Participant Characteristics.
Data Analysis
This project employed narrative analysis41,42 with analytic attention paid to both personal and sociocultural levels of meaning. This approach places an emphasis on coconstruction of stories and their meaning, with an assumption that neutrality is neither possible nor the aim in storytelling and hearing. 42
Analysis aimed to understand how participants made sense of their lived experience and how their voices converged and differed as a group. Thus, the method also allowed for the identification of shared narrative forms: broader discourses that emerged across multiple accounts.
Attention was paid to the meaning participants attached to their images and how they used them to punctuate their stories. The project prioritized experiential narratives, valuing content and tone over adherence to form. 43 To this end, the definition of “narrative” was held loosely, constituting an account shared by a participant which held personal meaning to them in relation to their cleft. The “discourses” were the ways in which these individual narratives could be seen within and across each other; shared stories.
The analytic process (Table 3) involved iterative readings and movement between individual and collective stories.
Step-by-Step Process of Data Analysis.a
Although this is presented as a linear process, earlier steps were continually revisited to consolidate understanding and add observations.
Results
The results below are supplemented by direct quotations from participants (denoted with “”, with ‘…’ to indicate shortening, [–] to indicate context. A narrative synopsis for each participant is provided first in Table 4, with the intention of preserving each individual's story in context, such that it can be interpreted alongside the proceeding overarching discourses below.
Narrative Synopses.
Six overarching discourses were identified in the stories the participants told of being a woman with cleft. These constitute stories of Enduring, Hiding, Striving, Healing, Reclaiming, and Reconciling and are presented with examples of individual narratives that scaffold them. These discourses are presented in sequence out of necessity, but all were present throughout almost every interview, and the ordering of this section does not depict a linear process.
Enduring
Twelve participants explicitly talked about the pervasive impact of childhood and ongoing medical experiences, sometimes decades later. For Claire, who describes herself as “quite outgoing, I’m quite bolshy, I’m quite outspoken and…not afraid to be so,” she struggles to make sense of her response to being in a dentist chair: “I really regress…I go really like a little girl, like I cry and go all like meek. It's not me at all. And I hate it…I hate the person I am when I'm in the dentist chair.” Mary reflects on the uncomfortable power imbalance between a dentist and their patient and how her dentist “keeps saying ‘Your mouth's so small’ as if it's my fault…anatomically, we are a bit different. And we’ve been through horrible things in the past…she showed the student my mouth and didn’t even ask…you're made to feel like you’re some sort of freak. And most of the time they ask you to take your glasses off. And I know it sounds silly, but that makes me feel even more vulnerable.” As the site of so much cleft treatment, dentists and dental work appeared as a source of discomfort in all but one (Taniya) of the participants’ stories (see Figure 1A). Anna describes that, even when treatment is less obviously invasive, being invalidated by professionals is exhausting and has had a lasting impact on the trust that individuals with cleft have to be able to place in their cleft teams “I actually thought I had a chromosome deletion…the surgeon was just flicking through my notes and he laughed at me…literally no-one was interested…it definitely does make you lose trust in medical professionals. They make you doubt yourself too because like ‘surely, doctors know best.’”

Participant quotations and accompanying images of (A) Barbed wire, (B) Tartan handkerchiefs, (C) work desk.
For Taniya, her recent surgery had highlighted the impact of her appearance changing so frequently throughout her life: “you look in the mirror for so long and it looks a certain way…you get used to it. And then when it is repeatedly and drastically and in a span of 6 hours changed and you wake up and now like this is like your new normal…but it's not normal. It's not me. I don't hate it, but I am also like ‘I feel like Mr Potato Head with parts that don't belong to me.’ My nose doesn't feel like it's mine. It feels like I can whip it off and put another one on” which she later added is a more difficult process to recover from each time.
Enduring others’ reactions to cleft seemed often more distressing than treatment itself. Narratives of being “not conventionally attractive” women were commonplace, and Sophia described missing out on “milestones of femininity” such as being flirted with or cat-called by men, which she recognizes as “negative…but as someone who would never have that happen, it’d be novel. It's an aspect of womanhood which has never been accessible to me.” For Sassie, her view of herself as unattractive is substantiated by other women's responses to her, which she explains is a direct result of dominant societal narratives about the roles women are expected to serve: “[other women are like] “don't come near us, because if you're near us, then no men will want to approach us.” …because, you know, “we are fertile and beautiful and you are an anathema.””
Hiding
Concealing oneself in some way was a narrative across all participants’ stories. For some, this was hiding the physical features of cleft itself, such as Lindsay, Rose, Sophia, and Gemma, who cited the COVID-19 mask-wearing mandate as a way to hide their faces and to make them feel equal to those around them for the first time. While Morag and Rebecca both described feeling more confident in their appearance in adulthood, having a palatal fistula results in nasal regurgitation, which they find embarrassing and socially obstructive: “after I've had some chocolate, I'll find myself getting a runny nose and its brown chocolate residue…it sounds absolutely disgusting and people go ‘eeeurgh.’” Morag manages this by always carrying patterned handkerchiefs (see Figure 1B).
Employment presents unique challenges and triggers relating to navigating adulthood with a cleft for most participants. Following distressing childhood medical photography experiences as part of her cleft treatment and feeling ashamed of her appearance, Rose describes how she manages needing profile pictures for work opportunities: “I just think for me black and white is not as unattractive. I think that a reader would just take a look at a black and white photo and not spend as much time studying it. I mean, I should have a professional headshot, but I want nothing to do with it.” For Sophia, who is due to graduate soon and will be seeking employment, having a cleft means constantly minimizing her need for adjustments and concealing as much difference from her peers as possible: “You're seen as a liability. They don't want to hire you because you're not going to be at work as often as a typical employee…you don’t talk about it, because you will end up disadvantaging yourself.” This introduces the prevalent idea from many participants that cleft itself is not their primary concern, but the shame that they feel because of dominant narratives which disempowers individuals with cleft, is far more impactful. This is further explored by Anna regarding avoiding needing to explain to her work that she was taking time away for “plastic surgery”: “When I was growing up, plastic surgery was a taboo…people don’t realize it's a medical specialty and plastic surgeons don’t just do people's boobs or whatever…in my old job, I had to put off surgery…I just didn't want to have that conversation with my managers.”
Finally, for Annmarie, her story of hiding was one of feeling that her needs were being hidden as part of a wider social discriminatory practice of ageism. As an older adult with a cleft, Annmarie reflects on how invisible she feels that her cleft-related medical needs are, despite continually advocating for herself and others in her situation: “it's like we're lost…I mean, it's really sad. I love what they're doing for children, but we need to look at all age groups.”
Striving
The pervasive feeling of needing to “measure up” to others, and perhaps to sociocultural expectations of women was described by most participants. Claire described carefully planning her outfits for each day because “beauty bias is a real thing. People make assumptions about unattractive people, that they’re less likely to be intelligent…I think I give people a leg up by looking ‘the part’ and then they’re more likely to overlook my face.” Similarly, some participants, such as Anna, described feeling a need to prove that they could have worthwhile qualities to employers, despite their cleft: “with surgery…I need to work extra hard before and after to make up for it.” For many, this was true in social spaces too. Sassie used an example of racial bias as a powerful parallel to how she feels entering a room and immediately feeling at a disadvantage, “my stepson says that his blackness always enters the room before he does. And it's the same…my cleft is in the room, and if I'm really lucky…and I make people laugh, people start seeing me shortly afterwards.” Sometimes, Sassie's striving to meet expectations of how women should be was even apologetic (see Figure 1C).
On a practical level, all participants described the effort that they have needed to continually invest in their cleft and/or dental treatment, far beyond the cessation of their original discharge from their cleft team. Fighting for adequate care of obturators was a source of particular stress for 6 participants, with Gemma stating “if I couldn't wear it, I couldn't eat. I couldn't speak. I couldn't do anything…[dentists have] got no comprehension of how major that is” and Sassie highlighting the trust that dentists demand regarding them “The other thing about an obturator…what an absolute bloody ball-ache it is getting a new one…I don't like handing it over because people put it on the tissue on the side. I don't know where it is. It's so hard to get another.” For Iris, the fight is simply trying to be seen by a cleft team: “I don’t know what they do or what they don’t do but they’re rubbish at it so referrals got bounced every time…they don’t seem to know how…I need more help and I’ve tried so many times.”
For most, a general sense of trying and fighting was present, across multiple themes. Taniya reflected on how cleft cannot and should not be held in isolation from other intersectionalities if people's stories of striving to overcome are to be fully appreciated: “one of my college admissions questions was: tell us how you've overcome an adversity. And now I think like, “sure, but from what aspect? Being cleft affected? Being a woman? Being a black woman? Being a black woman who is also plus size?””
Healing
By way of reprieve from emotionally- or labor-intensive aspects of coping with their cleft, all participants described aspects of their lives in which they sought refuge (see Figure 2A). Within these refuges of choice were stories of honoring and healing painful past experiences or beliefs relating to living with “difference.” Some of these were explicitly relating to treatment, such as Gemma always scheduling time to go to a café after appointments for cake in honor of a routine she had with her parents over 40 years prior, or Sophia's collection of photos of medical equipment or environments that were once a source of great stress, but she now looks at them to motivate herself as a reminder of how far she has come. For Rebecca, learning to ground herself and gain the perspective that “‘my cleft doesn't have an impact on whether my train is going to be delayed…I'm just going to work like a normal person would…I do things the same way any other human being would’” has been comforting.
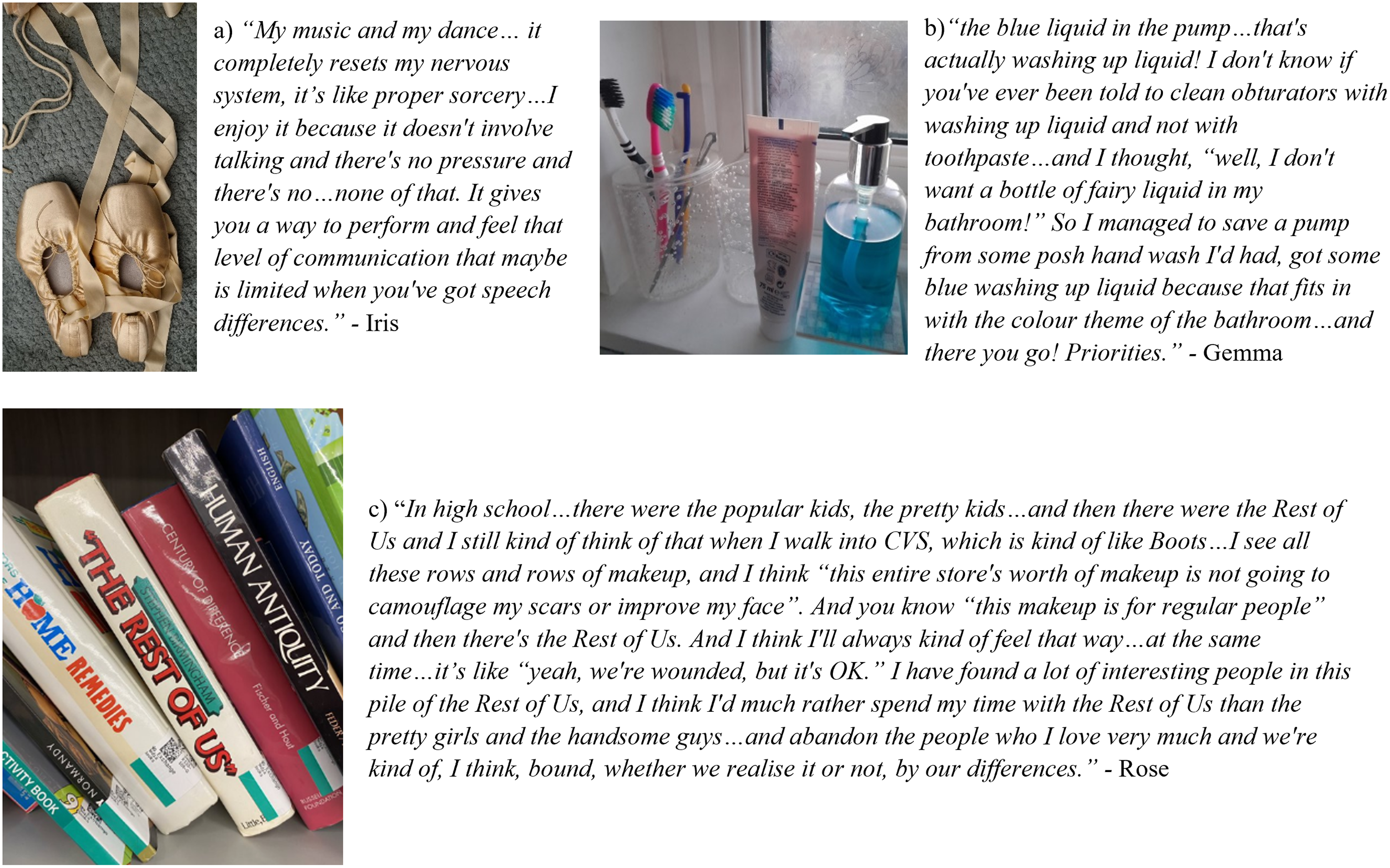
Participant quotations and accompanying images of (A) Ballet shoes, (B) bathroom shelf, (C) books.
For all participants, having close social bonds and feeling at peace with one's place among their social context were described as healing. Taniya reflects “I am mummy to my children. I am my husband's wife. I don’t need anything else,” having told stories of never believing she would be able to have a family of her own. However, some participants felt that the presence of loved ones conveyed a sense of normality to onlookers, such as for Sassie: “Having the combination of dog and partner makes a massive difference when we go out and about. It's a normalizing thing, ‘Oh, she has a partner and a dog. She must be alright then.’” This being seen as desirable as part of being “normal” manifested frequently when participants spoke about their relationships, specifically with intimate partners.
Finally, half of the participants told positive stories of meeting and befriending others with cleft, which for Beth, started reluctantly in adolescence where she remembers thinking “why on earth would you want to sit in a room with everyone with the same problems as you…we don’t look good!” but later embracing the community and reflecting “If I was looking for support…my first port of call would be my friends that also have clefts…they understand and are open to listening and sharing on another level.” However, while all participants mentioned encountering others with cleft, some, like Rose, felt less comforted about the idea “I don't know if emotionally I can take a roomful of us!” but later recognized that perhaps this was part of her journey toward healing, which could run parallel to Beth's story.
Reclaiming
For most participants, finding ways to reclaim parts of their lives they feel less autonomous over, such as their medical care or others’ responses to their cleft, was important (see Figure 2B).
For Morag, who learned to ride a bike as a child to circumvent bullies on the school-bus, being a commuter cyclist is now a treasured part of her private and social identity which represents freedom, rather than escape. All but 2 participants discussed makeup as a route to reclaiming and somewhat sculpting what others would see of their lips and scars, but through different mechanisms. Lindsay's characteristic red lipstick holds the meaning that “you know, if people are gonna look…I'm gonna give them something to look at,” whereas for Sassie, her designer lipstick is “just my private little thing…it's little private moment of ‘Here we go. It's OK to be out there.’” For Iris, repeated surgery represented other people and processes claiming control over her face, compromising her feeling of connectedness to her own body. Piercings were a way of gaining “control over what I looked like and who went in my headspace” while acknowledging a wider sociocultural context that there is “pressure on females about looking a certain way” and that the approach of “we’re not gonna look normal so lets not bother,” allows Iris to claim ownership of her appearance beyond what others believe it should be. For others, reclaiming narratives were found in stories of proving wrong others’ limiting beliefs about their cleft. Annmarie, having been told she would never be a nurse due to her cleft, recalls realizing her worth by rejecting those who she felt rejected by: “they equated…my appearance with a lower intelligence…once I got my [nursing] degree, I was asked to come back and teach…and I said ‘no thank you!’” This reclaiming seemed to be of power and autonomy over one's ability, in a similar way to Sophia, who, in her 20s, taught herself to play the flute after being told as a child that she never could. Accepting and realizing that she must “play flute differently than somebody else because of the shape of my top lip but I'm able to do it” depicts a flexibility, as well as determinedness, in reclaiming previously denied experiences.
Reconciling
For Rebecca, Beth, Taniya, Morag, Sophia, and Annmarie, publicly advocating for others with cleft represented a turning point in their lives, wherein a desire to hide was overridden by a calling to inspire, inform, and instil hope. Finding community and genuine allyship catalysed this shift, and for Beth there was a sense of choosing and being proud to declare her difference: “I noticed a pride almost in my cleft, which I hadn't really felt before in that like, I'd always felt pride of being part of the CLAPA community but never…pride in my own cleft journey and kind of own it as, like, something actually really quite badass and cool.” Morag, who only reports acknowledging her cleft in her 60s after meeting a compassionate dentist, says “I can't be private if we’re going to achieve proper dental care and all the rest of it for other people like…us” signifying being motivated by campaigning for change and finding community. In terms of treatment, Taniya concludes that there could always be more surgery, but her pursuit of more cosmetic work is now over, saying “I have to ask myself who I’m doing this for. My children are not going to see me any different. My husband isn’t going to see me any different…I’m happy with where I am. How the rest of the world feels, its not my business. I don’t care.” Among all participants, there was a sense of catharsis in the interviews whereby it was acknowledged that cleft remains “in the room” and its impacts will be sustained for as long as care remains a battle and dominant social narratives on what is it to be “attractive” and “normal” are prevalent. However, each individual had strategies of reconciling themselves with their difference in personally meaningful and emotive ways. Summarizing, Rose describes her journey to developing understanding and acceptance of her cleft and where she believes she “fits” in the world (Figure 2C).
Discussion
This study aimed to explore the stories of adult women born with a cleft to better understand cleft from a gendered perspective. Within cleft, as a condition for which the primary treatment is medical and all treatment is managed within medical MDTs, little space has been made within research and practice for considering the intersectionality of living as an adult navigating cleft alongside living as a woman within a society holding established appearance and gender norms. Operations of shame can be inferred from broader literature suggesting that external pressures may become internalized, such that those who are or feel “othered” risk self- and other-attacks, reinforcing emotional distress and societal disadvantage.13,14
Qualitative research has identified that the factors impacting the psychological well-being of adults with cleft include social support,7,11,44 satisfaction with treatment outcomes,11,44 appearance-satisfaction,7,11 and tendency toward optimism. 11 Furthermore, a comprehensive narrative review suggested the lifelong impact of cleft is “low,” though findings are complex and firm conclusions difficult. 45 Within this study, the 6 discourses identified in participants’ stories depicted ongoing processes that appeared to be dynamic and constantly co-occurring rather than linear, which perhaps goes some way in explaining this complexity. Establishing a neat overall conclusion on “well-being” may be unreasonable when shame and enduring trauma coexist with healing and reconciling with cleft. These processes likely reflect systemic and sociocultural norms and power beyond individual control, and the ways that these are internalized and triggered in different ways. The current study builds on previous research findings that highlight that while distress is present in men and women with cleft, it is more prevalent and acute among women.16,22 It may indicate where dominant social narratives may be operating to maintain this distress, in addition to the ongoing adverse impacts of both relational and medical trauma. This was particularly prevalent within the “hiding” and “striving” narratives, where participants spoke of assumptions others make about their intelligence or desirability and their constant efforts to anticipate and overcome these.
Although all 6 narratives were identified across stories, developmental context may shape how they are emphasized. For example, Erikson 46 posited that younger adulthood is characterized by identity and intimacy, midlife by caregiving or self-definition, and later life by reflection and legacy, evidence of which is seen within the stories in this project. Lifespan perspectives, such as Erikson's psychosocial stages, highlight how age-related roles and tasks influence meaning-making. From this view, variation across participants’ stories reflects the interplay between individual experience of cleft lip and palate and broader developmental and social contexts.
(En-)Gendered Norms and Power
Centuries of literature have documented that being female generally affords less advantages than being male in Western societies and beyond. Women deemed attractive are more likely to be employed, 47 succeed financially, 48 and be successful in dating.49–51 “Beauty bias,” wherein physical unattractiveness, particularly in women, affords fewer opportunities, continues to be substantiated.52–54 Multiple studies of what constitutes female attractiveness conclude that visual symmetry and “softness”/femininity are most important and more determining of a woman's likeability than the equivalent in men, for whom nonphysical characteristics such as personality and perceived resources are privileged.50,55 Many participants reported being certain that their appearance altered others’ assumptions and behavior toward them and described themselves as in some way less than their noncleft-affected peers, particularly when speaking about social, intimate, or dating experiences. Indeed, both male and female laypeople rated images of faces with cleft as “less attractive” than those without, but men's responses were more extreme. 56 The narratives “hiding” and “striving” depicted examples of where having a cleft can feel shameful, embarrassing, or isolating. Taking oneself away from others to adjust an obturator or manage nasal regurgitation were examples of this, where an awareness of cleft was egregious and obstructive.
Feminist and broader social justice movements throughout history have given rise to alternative narratives of reclaiming power, including around disability and facial difference. 57 These assume a social model of disability, which rejects medical models of defects and abnormalities and adopts the stance that society, rather than biology, dis-ables individuals physically or mentally through discriminatory practices and norms. 58 The narratives “reclaiming” and “reconciling” suggest a shift, or even rebellion against, oppressive societal messages that participants are “abnormal.” These narratives saw a marked shift away from shame and shaming self-talk. Most participants described an interest in advocating for others with cleft and in becoming involved in the broader cleft community, which may partly explain this omission of shame as individuals feel genuinely understood or equal to those with shared experience and understanding. Participants saw this as a positive part of their lives allowing them to find community, establish new norms, and embrace their cleft.
While most participants reported eventually coming to an acceptance of their cleft, the co-occurring emotional pain associated with being and appearing different was tangible throughout the interviews, as was the distinctly female voice of self-subjugation and bereavement of missed or inaccessible opportunities that not having a cleft may have afforded them.
Recommendations for Clinicians
Considering not only the content, but the function of the stories told within this study could support clinicians in their understanding of their cleft-affected clients. Some existing research has concluded that with age comes self-acceptance and a reduction in care for others’ judgments among adults with cleft.8,15,17 The current study provides some support for this, but the coexistence of trauma, shame and concealment narratives within participants’ current, living experiences could indicate that more positive narratives serve as a protective defence against the emotional pain of the others. According to psychodynamic frameworks, establishing truths to justify adversity is a common mechanism by which people learn to live with uncomfortable or painful realities of their past or present beliefs and experiences.59,60 Therefore, remaining curious about the function of narratives to protect either the client or others could support cleft-affected clients’ stories to be heard and explored more thoroughly.
The presence of “enduring” narratives, particularly relating to dentists, medical care, and experiences of social stigma, indicate that adult cleft care must be trauma-informed, to meet the needs of those who need it. There is extremely limited research support and no guidelines for particular therapeutic models or interventions for individuals with cleft. 61 However, these findings support the use of trauma-informed models that validate experience over diagnosis. 62 Furthermore, they contribute to third-wave cognitive behavioral theories by evidencing the specific role of self-stigma in women with cleft, highlighting the potential for compassion-focused therapy (CFT) interventions to counteract entrenched shame in these individuals.63,64
The inherent power of being a medical professional should also be considered by clinicians in cleft teams. While they can and should be advocates for their patients in appointments and beyond, 65 the environment may not feel approachable or safe for adults with cleft. This may hold truer still for women, for whom medical interactions are more broadly indicated to feature oppressive power relations requiring more active resistance than for men.66,67 Narratives of “enduring” and “striving” within participants stories provided examples of this power in action. Within therapy, his barrier could be acknowledged by explicitly naming what, or whom, the psychologist may represent for the adult client with cleft and taking steps to redistribute power in the therapeutic relationship, such as by meeting outside of the hospital, explicitly recognizing the expert knowledge of the client and/or taking longer to establish rapport before beginning change-orientated work.
Finally, despite recognizing significant emotional distress and, for some, a desire to seek mental health support regarding their cleft, most participants had never had contact with their cleft team regarding this. For some, this was because they were not aware of psychologists in cleft teams, others believed it was too late for them to seek help and at least one had a long history of rejected referrals. It is recommended that cleft teams find ways to reach out to adults, perhaps through colleagues in other cleft specialties and via dental and general practitioners in primary care services. Self-referral may also be a positive step in empowering adults to reaccess cleft care.
Research Recommendations
Future research could build upon this study by mirroring the method and approach with men, exploring narratives of masculinity and power in relation to cleft. In addition, other intersectionalities, including but not limited to ethnicity, age, and sexuality, could be investigated in relation to adults born with cleft to promote and build momentum for more holistic understandings outside of the clinic room.
The narratives identified in this study could be used as a foundation for future clinical research. For example, “hiding” could be quantitatively explored further in terms of shame which could inform treatment decision-making and/or therapeutic interventions. Trials of therapies which seek to address shame, such as CFT, could contribute to the lacking evidence base for particular modalities in cleft care.
Finally, the interactions between participants’ stories and the researcher's own lived and living experience of womanhood and cleft was an important feature of the project. While it was not possible to evaluate this entirely within this report, data were collected about participants’ experiences of sharing their stories in this way, and it is hoped that it will inform future research. It would be particularly pertinent to consider the impact and experience of using photo elicitation methods with this group, given the salience of one's “image” in the context of visible difference and the role of photography in visible difference treatment. Future work may wish to explore the possibility of a therapeutic benefit of narrating lived/living experience using self-generated images.
Strengths and Limitations
The open, narrative approach to interviewing and the multilayered data analysis process allowed for rich stories to be told and heard in this project. Given the relative lack of qualitative research conducted in this area, a more structured approach may have necessitated assumptions being made about where priorities for enquiry should lie, resulting in important nuances being missed. However, a limitation of this approach may have been that participants may have focussed more on explicit aspects of femininity had they been given more directive guidance.
A further strength of the project was the diverse age range of participants, which is likely due to the efforts employed to recruit through multiple channels. However, all but one participant was white, indicating that the project advertisement did not reach and/or feel applicable or interesting to those in the cleft community of the global majority. Additionally, many participants were highly educated and/or involved in advocacy, so were possibly more comfortable sharing stories than others less engaged in the community. Further research should aim to diversify participation using targeted recruitment if necessary to maximize the reach beyond those who are already engaged with organizations supporting and advocating for individuals with cleft.
With a shared language of the intricacies of cleft treatment and the ability to share, rather than solely hear experiences, it is likely that the researcher was able to ensure participants felt more comfortable telling elements of their stories than they would with someone who they did not feel could relate to them in this way. However, it was held in mind that participants may feel a need to withhold some aspects of their realities to protect the researcher's emotional well-being. There may have also been an assumption from participants that she already knew parts of their story and therefore did not need to be told, risking individual nuances being omitted. This was mitigated by assuming an open stance, acknowledging that there will be shared experiences which might include some impactful or emotive stories and discussion of thoughts and beliefs which may be different or similar to my own. The researcher reminded participants of their centeredness to their own interviews and was mindful of this when choosing what to share of her own story. With appropriate supervision, a robust reflexive diary, and utilizing prior knowledge and experience practicing self-care during this type of work, this influence served, rather than limited, the project.
Overall, this project employed a relatively novel method with a population primarily studied under a medical lens. It is hoped that by introducing intersectionality to cleft discourse in such an explicit way through the metaphorical and literal lenses of this group of participants will be meaningful in advancing the field further.
Conclusion
Using a narrative analytic approach combined with photo elicitation, this study built on existing literature exploring the lived and living experiences of adults born with a cleft lip and/or palate, specifically focussing on women. Stories of enduring, hiding, striving, healing, reclaiming, and reconciling were shared and heard, converging in ways that defied the establishment of an orderly pattern or trajectory. Participants were clear that cleft remains a part of their life regardless of how much time has passed since the end of their prescribed treatment and emphasized the impact that others’ appraisals of them continue to have. Ongoing difficulties with accessing appropriate medical and dental care, friendships, dating and intimacy, employment, makeup, and living with the lasting impact of invasive medical procedures were all prevalent in the narratives. Being a woman who looks and/or sounds different in a society which often disempowers women and places expectations on their appearance and behavior was discussed as being exhausting by some, and unique ways of compensating and adjusting were explored. Clinicians and researchers should ensure they are aware of the intersections of cleft and gender in the context of adults’ ongoing experiences, such that their clients’ and participants’ realities can be fully heard in a trauma-informed and respectful way.
Footnotes
Acknowledgments
The authors would like to thank all participants, the UK Cleft Psychology Clinical Excellence Network, our patient representative, the Cleft Lip and Palate Association, and Face Equality International for their support. Also to Dr. Susannah Colbert for methodological consultation.
Ethical Considerations
Full ethical approval for the thesis this study constituted was sought and obtained (ETH2324-0081) from Canterbury Christ Church University, Kent, UK.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Salomons Institute for Applied Psychology in line with their postgraduate (DClinPsy) thesis guidelines.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.