
Abstract
Objective
This study examines the psychological well-being of Swiss youths born with a unilateral cleft lip and palate (UCLP), in a multi-dimensional and clinical perspective.
Design
Retrospective cross-sectional study.
Setting
Self-report questionnaires completed by youths born with UCLP, followed at a specialized cleft clinic in Switzerland, and by peers without UCLP, recruited in schools of the Vaud county, Switzerland.
Participants
Youths aged 7.5 to 16, born with UCLP (clinical group, n = 41, 29.2% female) or without UCLP (control group, n = 56, 49.0% female).
Outcome measures
Adverse life events (ALE; Adverse Life Events), behavioral and emotional symptoms (Strengths and Difficulties Questionnaire and Post-Traumatic Checklist Scale), bodily self-esteem (Body Esteem Scale), quality of life (Kidscreen-27), emotion regulation (Cognitive Emotion Regulation Questionnaire), social support (Sarason's Social Support Questionnaire).
Results
Most outcomes showed no significant group-difference. Compared to matched peers, youths with UCLP reported lower psychological quality of life and social support satisfaction, along with positive factors of fewer ALE and lower non-adaptive emotion regulation. In youths with UCLP, higher scores for ALE were associated with higher total scores for behavioral and emotional symptoms. Higher scores for bodily self-esteem were associated with higher scores for satisfaction of social support and adaptive emotion regulation.
Conclusions
Youths with UCLP show globally similar psychological well-being as matched peers. We observed some vulnerabilities but also protective factors, which support the need for psychological perspective within multidisciplinary care. The relationships between dimensions suggest specific targets that may have an impact in context of intervention.
Keywords
Introduction
Psychological Well-Being in Youths Born with a Unilateral Cleft Lip and Palate
Unilateral cleft lip and palate (UCLP) is a condition that affects 1 in 650 infants born in Europe 1 and that requires long-term advanced medical care. Implications may concern various developmental domains (eg, feeding, phonation, dentition, psychological) according to cleft type.2,3 Coordinated care by a multidisciplinary team is therefore essential for the proper follow-up of the child and his or her family, to support an optimal development, by starting at the time it is diagnosed (ideally during pregnancy) and ending when the child is fully grown (ie, reaches skeletal maturity). The team brings together specialists from medical and allied disciplines, trained to manage consequences of UCLP at all developmental stages, within an integrative perspective: esthetic, functional, as well as psychological, and social. This visible condition and the medical interventions needed to treat it may indeed represent a form of early adversity in those children's lives, which they must face, and which can have an impact on their psychological well-being. 4
Psychological well-being is a broad concept that encompasses multiple dimensions. A recent meta-analysis published in 2022 including 41 studies 4 investigated some of those dimensions and showed that most psychological outcomes seem to be similar between children with UCLP and non-affected children, however with a higher incidence of psychological difficulties in certain domains. More specifically, the authors observed inconsistent evidence of increased emotional and behavioral problems in children with UCLP, especially anxiety and depression, and in particular, among girls. These symptoms seem to be associated with cleft visibility. Furthermore, the authors showed that self-concept (ie, internal thoughts about oneself, including self-image, self-esteem and satisfaction with appearance) was affected by the presence of UCLP in half of the studies; in the other half, however, self-concept did not differ between participants with and without UCLP. 4 Finally, they highlighted that children born with UCLP show good resilience and coping, which constitute a protective mechanism and may improve their outcomes. 4
This meta-analysis 4 highlighted an important heterogeneity among studies regarding psychological dimensions in children with UCLP, making it hard to have an accurate image of difficulties encountered by them. Psychological well-being is indeed a complex and multi-dimensional concept that needs to be dissected to be assessed in full. However, previous studies addressed only one or a few dimensions at a time, leaving the relationships between them largely unexamined. The current study therefore considers a broader range of dimensions of the psychological well-being than those described in the recent meta-analysis (ie, emotional and behavioral problems, bodily self-esteem and emotion regulation), 4 that we found appropriate for a comprehensive assessment.
First, a comprehensive dimension of the psychological well-being is the quality of life, as it is defined by the World Health Organization (WHO) as a multi-dimensional concept, encompassing physical and psychological health, level of independence, social relationships, personal beliefs and relationship to the environment. 5 In their review in 2020, Guillén et al. 6 reported the presence of inconsistent results between studies regarding the quality of life of children and adolescents born with UCLP: some studies reported lower quality of life scores, while others revealed a similar or even superior quality of life in children with UCLP compared to a control group. More specifically, some studies in this population suggested a decrease in social and emotional quality of life (especially in late adolescence), as well as lower functional physical quality of life (eg, corresponding to difficulties in eating or making oneself understood when speaking).3,7 However, some studies described that the influence of craniofacial conditions on quality of life is small.8–10
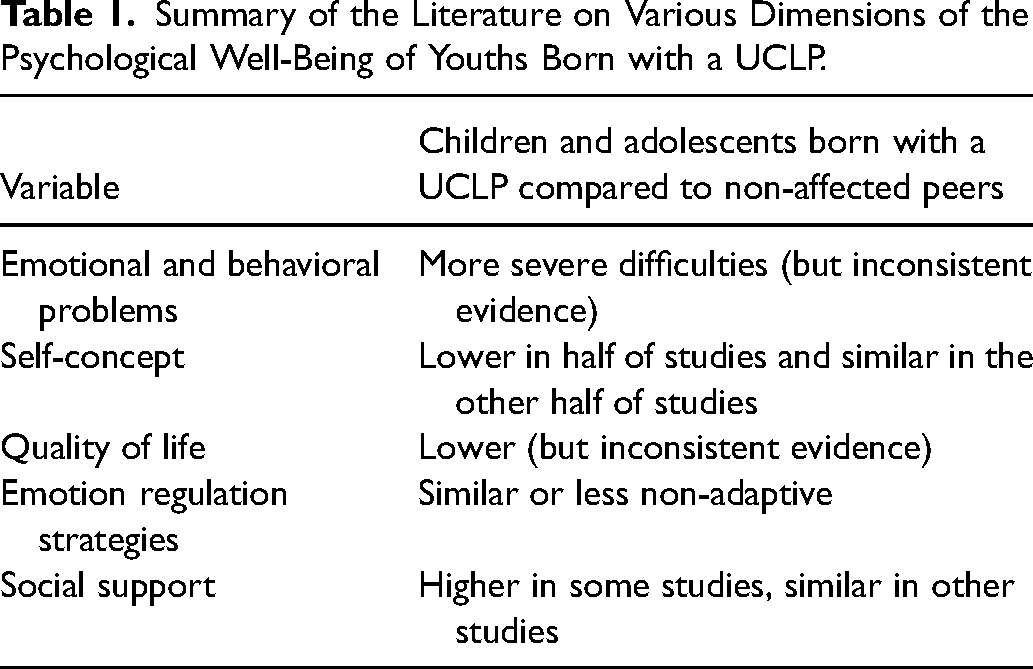
Secondly, as Branson et al. 4 pointed out, children with UCLP present good resilience, which has been defined as the capacity for positive adaptation in significant adversity (eg, adverse life events - ALE). 4 We identified one study that examined ALE in children born with a UCLP, which found that 60% of participants reported zero to one ALE and 11% reported four or more ALE. 11 To deal with adversity, adaptive ways of coping include good emotion regulation and capacities to rely on social support.12,13 Emotion regulation was described as conscious or unconscious processes by which individuals modulate the intensity and/or duration of their emotions in response to environmental demands.13,14 One study observed normal emotion regulation in adults with UCLP 15 and another found less non-adaptive emotion regulation in children and adolescents with UCLP than in non-affected children. 16 Studies of social support in patients with UCLP have shown conflicting results: some observing that adolescents with craniofacial conditions report higher perceived social support,10,17 while another found no difference in social support between a UCLP group and a control group. 18 The Table 1 presents a summary of the literature on various dimensions of the psychological well-being of youths born with a UCLP compared to non-affected peers.
Relationships between Dimensions Encompassed in Psychological Well-Being
As described above, psychological well-being integrates multiple dimensions that interact with each other. For example, Branson et al. 4 reported that low satisfaction with facial appearance is the factor most commonly associated with poorer psychosocial outcomes in children born with UCLP. Perception and acceptance of physical appearance are associated with various aspects of psychological well-being (ie, quality of life, social experiences, psychopathological symptoms and overall mental health) in the general population as well as in children with craniofacial conditions.8,9,19,20 Another example is behavioral and emotional symptoms having shown associations with quality of life, in youths with UCLP as well as in the general population.6,21
Concerning emotion regulation, mostly studied in the general population, Aldao et al.13,14 found that strategies theoretically defined as maladaptive (ie, rumination, avoidance, suppression) were associated with more psychopathology and adaptive strategies (ie, acceptance, reappraisal, problem solving) with less psychopathology. Regarding social support, positive relationships and support from family members have been identified as key factors associated with better health and reduced psychological difficulties in young people with UCLP,4,22,23 whereas troubled interactions with peers negatively affect the quality of life of affected and non-affected children.2,6,19
Aims of This Study
Previous studies examining the psychological well-being of youths with UCLP sometimes showed contradictory results. As psychological well-being is a complex construct resulting from the interactions of many factors, our study aimed to assess the psychological well-being of young people born with a UCLP by considering multiple dimensions, in order to gain a more comprehensive understanding, and with the strength of including a control group. The clinical perspective chosen for this study may add to the current literature. Indeed, a multi-dimensional approach can be useful for clinical practice, as it is more representative of the reality of the person in their wholeness. Exploring relationships between these dimensions may allow to identify children and adolescents who are at higher risk of difficulties and provide clues for targeted and specific interventions.
The first aim of this study was to assess differences in psychological well-being and its dimensions (ie, behavioral and emotional symptoms, bodily self-esteem, quality of life, emotion regulation and social support) between a group of children and adolescents born with a UCLP and a group of typically-developing children and adolescents. The second objective was to assess the relationships between these dimensions within the UCLP group, to focus on a clinical approach that may be applicable to the care of these youths.
Hypotheses
Regarding the first aim, we hypothesized that several dimensions would be affected in the clinical group, such as quality of life and bodily self-esteem, as described in the existing literature,4,6 as well as increased behavioral and emotional symptoms, as observed in previous studies. 4 In the second part of the study, numerous hypotheses can be put forward based on the existing literature. However, certain relationships between variables that have already been mentioned in previous studies would seem to be clinically relevant. For example, we expected to find links between non-adaptive emotion regulation and the presence of psychopathology,13,14 which would appear, in our measures, in the form of behavioral and emotional symptoms. In addition, an association between ALE and behavioral and emotional difficulties was expected, as it was already described in the non-affected population.24–26 Higher bodily self-esteem was also expected to show associations with higher quality of life 8 or with potential protective elements such as good social support. 8 Likewise, we expected a relationship between good social support and higher quality of life.6,8
Methods
Procedure
This study is embedded in a more global project (see 27 about bullying in youths born with a UCLP, where only the participants’ socio-demographic data overlap with the present data) that aimed to assess various psychosocial factors in young people born with a UCLP compared to the general population. The study has been approved by the local ethical committee (#2016-02019).
For the clinical group, we selected children and adolescents between 7.5 and 16 years old born with a UCLP, followed in the multidisciplinary cleft consultation at the University Hospital of Lausanne (CHUV: Centre Hospitalier Universitaire Vaudois), Switzerland. Exclusion criteria included the following: a comorbid diagnosed intellectual developmental disorder and/or the presence of a UCLP-associated syndrome. Children who met the inclusion criteria and their parents were approached by a member of the research team during an appointment of their usual follow-up at the consultation. For the control group, we recruited children of the same age, in schools of the Vaud county (Switzerland), who did not have a UCLP.
Participants received oral and written information. If they agreed to participate, they signed an informed consent form. Depending on the age of the youth, the agreement of the legal representative was needed (until age 13) or not (from age 14). Participants of the clinical group completed the anonymous questionnaires individually in the presence of caregivers and members of the research team in order to answer any of their questions or concerns. Completing the battery of questionnaires usually took around 45 min. Completing of the questionnaires was done anonymously and was not checked by the team, making it difficult to avoid missing data. Participants of the control group received information in their classroom and a letter was sent home to inform the parents/caregivers about the study and to obtain their consent if needed. Youths of the control group had around 45 to 60 min to fill the questionnaires at the same time during class. Two members of the research team were present for the whole class, to answer any question or concern. There was no financial compensation for study participation.
The Specialized Cleft Consultation at the Lausanne University Hospital (CHUV)
In the Vaud county (Switzerland), all children born with a cleft have public access to multidisciplinary care, in a specialized pediatric surgery consultation at the CHUV. All children and their parents are carefully followed from the diagnosis (usually prenatal) by the pediatric surgeon and the psychologist, and from the age of three, by the multidisciplinary cleft team which consists of a pediatric surgeon, two pediatric ENT specialists, a craniofacial surgeon, an orthodontist, a speech therapist and a psychologist, the latter being available until the youth is 20 years of age. The child and parents are seen according to the child's needs, usually once or twice a year.
Measures
French versions were used for all questionnaires.
Socio-Demographic Data
In the clinical group, the socio-demographic data were reported by the children and their parents in an additional questionnaire, asking about the child's age, gender and nationality, the parents’ living situation (married/living together or separated/divorced), both parents’ level of studies and profession, and the home environment (urban or rural). We chose to keep only parents-reported socio-demographic data, as there were fewer missing answers than in the children-reported data. In the control group, socio-demographic data were reported by children and adolescents. Three types of socio-economic status were derived from the parents’ level of studies and profession based on the Schedule for Affective Disorders and Schizophrenia - Present and Lifetime (Kiddie-SADS-PL) classification 28 : low (specialized workers and laborers), middle (artisans and skilled trades, agricultural or forestry and fishing occupations, service occupations, technicians, salespeople, administrators) and high (executives and self-employed).
Adverse Life Events
The questionnaire Adverse Life Events (ALE) 29 probes for the occurrence of 25 potentially stressing events (eg, death of a loved one, moving, burglary, parents being frequently away from home, changing school) during the last year. Items are scored 0 (“no”) or 1 (“yes”), according to whether or not the event has occurred, and a sum score is obtained.
Behavioral and Emotional Symptoms
To assess the presence of behavioral and emotional symptoms, we used two scales. First, the Strengths and Difficulties Questionnaire (SDQ), 30 which consists of 25 items, covering four domains of difficulties (emotional symptoms – eg, “I am often unhappy, down-hearted or tearful”, conduct problems – eg, “I fight a lot. I can make other people do what I want”, hyperactivity/inattention – eg, “I am easily distracted, I find it difficult to concentrate”, peer relationship problems – eg, “I am usually on my own. I generally play alone or keep to myself”) and one domain of strength (prosocial behavior – eg, “I try to be nice to other people. I care about their feelings”). Each item is rated on a 3-point scale: not true (=0), somewhat true (=1), certainly true (=2), referring to the last six months. A sum score is calculated for each domain (with reversed points for some items) and a total difficulty score is obtained by summing the scores of all four domains of difficulties. Higher scores mean a higher proportion of difficulties (or prosocial behavior in the strength domain). This questionnaire shows satisfactory reliability and validity. 31
We also used the Post-Traumatic Checklist Scale (PCL-S or PTQ), 32 which investigates symptoms of post-traumatic stress. In this questionnaire, the participant describes the most stressful event in their life and then answers 17 questions about symptoms that may result from it (eg, “I am bothered by repeated memories, thoughts, or images of the stressful experience”), on a scale from 1 “not at all” to 5 “extremely”, during the last month. Item scores are summed to obtain a total score. The PCL-S has good empirical and discriminant validity. 32
Bodily Self-Esteem
In the area of self-concept, we chose to assess specifically bodily self-esteem, given the predominantly physical difference implied by the UCLP. We used the Body Esteem Scale for Adolescents and Adults (BES), 33 which is a 23-item questionnaire assessing the participant's attitudes and feelings about their body and appearance, with no specified time frame. Each item is scored on a Likert-type scale with five responses from “never” (=0) to “always” (=4). Some negative items are recoded for scoring by reversing the scale. The items scores are then summed within three subscales: Appearance (eg, “I like what I see when I look in the mirror”), Weight (eg, “I am satisfied with my weight”) and Attribution (eg, “Other people consider me good looking”). A total score is also obtained by summing all three subscales. Higher scores mean a higher bodily self-esteem. This instrument has good psychometric qualities.34,35
Quality of Life
We used The Kidscreen-27 (KS-27),36–39 which investigates the quality of life of children through 27 questions, grouped into five dimensions: Physical (eg, “Have you felt fit and well ?”), Psychological (eg, “Have you been in a good mood ?” or “Have you felt sad ?”), Autonomy & Parents (eg, “Have your parents enough time for you ?” or “Have you had enough money to do the same things as your friends ?”), Peers & Social support (eg, “Have you had fun with your friends ?”), and School environment (eg, “Have you been happy at school ?”). The questions ask about the frequency or intensity of various hypotheses during the last week, reported on a Likert-type scale with five responses ranging from “never” (=1) to “always” (=5) or from “not at all” (=1) to “extremely” (=5). A score is then obtained for each dimension, and a total score summing all dimensions, considering that some negatively formulated items are scored reversely. Higher scores mean a higher quality of life. This questionnaire shows good psychometric properties. 38
Emotion Regulation
To investigate emotion regulation, we used the Cognitive Emotion Regulation Questionnaire (CERQ),40,41 which asks what the participant generally thinks when he or she goes through negative or uncomfortable events (no time frame is specified). It consists of 36 questions on the use of various emotion regulation strategies, with five possible responses on a Likert-type scale ranging from “almost never” (=1) to “almost always” (=5). There are nine emotion regulation strategies assessed (with four items each), grouped into adaptive (Acceptance, Positive Refocusing, Refocus on Planning, Positive Reappraisal, Putting into Perspective) and non-adaptive (Self-Blame, Rumination, Catastrophizing, Blaming others) strategies. Total scores are obtained by summing separately all adaptive and all non-adaptive strategies, higher scores representing a more frequent/preferential use of the strategies. This questionnaire has good psychometric properties. 42
Social Support
The Sarason's Social Support Questionnaire (SSQ) 43 is composed of six items measuring the availability and satisfaction of perceived social support. In six different situations (eg, “Who can you really count on and who is reliable when you need help ?” or “Who accepts you as you are, with your qualities and faults ?”), the participant indicates the number of persons they can count on and evaluates, on a Likert-type scale with six answers ranging from “very satisfied” (=6) to “very dissatisfied” (=1), their level of satisfaction with the social support received. A sum score is calculated by adding up all the items, with higher scores representing a better satisfaction of social support. This instrument shows good psychometric properties. 43
Data Analyses
For statistical analyses, we used the SPSS®, version 27.0 (IBM Corporation, Armonk NY; USA). The data suit Gaussian-like distribution, allowing for parametric testing. For all the statistical tests, we used only proportions of valid data, without considering missing answers. First to assess the differences between the two groups, we computed independent sample tests of Students (for continuous variables) or Chi-square (for categorical variables). For questionnaires with multiple dimensions, we used multivariate analyses of variance (MANOVA). To assess the magnitude of differences (ie, effect size), we computed Cohen's d for t-tests, partial eta square (pη2) for MANOVA. Cohen's d of 0.2 refers to small effect, Cohen's d of 0.5 refers to moderate effect and Cohen's d of 0.8 refers to large effect. Whereas pη2 of .01 indicates a small effect, pη2 of .06 indicates a medium effect and pη2 of .14 indicates a large effect.44–46 To assess our second aim regarding the relationships between the dimensions, we computed Bravais-Pearson coefficients of correlation, only on the clinical group's data. Notice that as sex is a categorical variable, we computed Eta (η) coefficient. 47 Coefficients of correlation of .10 is considered a small effect, of .30 a medium effect and of .50 refers to a large effect. Data of the control group was run as a supplementary analysis and is, thus, presented in Supplementary File. Significance of the P-value was set by convention at P < .05.
Results
Socio-Demographic Data
The clinical group of children and adolescents born with UCLP included 41 participants (17 boys, 7 girls and 17 uninformed gender/missing data), with a mean age of 12.4 years old (missing data in 9 participants). Most of these children and adolescents had a Swiss nationality and lived in a rural environment. The socio-economic status was middle to high. The control group included 56 participants (27 boys, 26 girls and 3 uninformed gender/missing data), with the same mean age as the control group (12.4 years old; missing data in 3 participants). They were also mostly Swiss but there were more other nationalities represented, as for example French, Italian, Albanian, Belgian and others. The distribution of living in rural and urban area was almost the same as in the clinical group, most participants living in rural areas. They also reported middle to high socio-economic status.
Table 2 describes and compares the socio-demographic data of both groups.
Summary of the Literature on Various Dimensions of the Psychological Well-Being of Youths Born with a UCLP.
Socio-Demographic Characteristics.
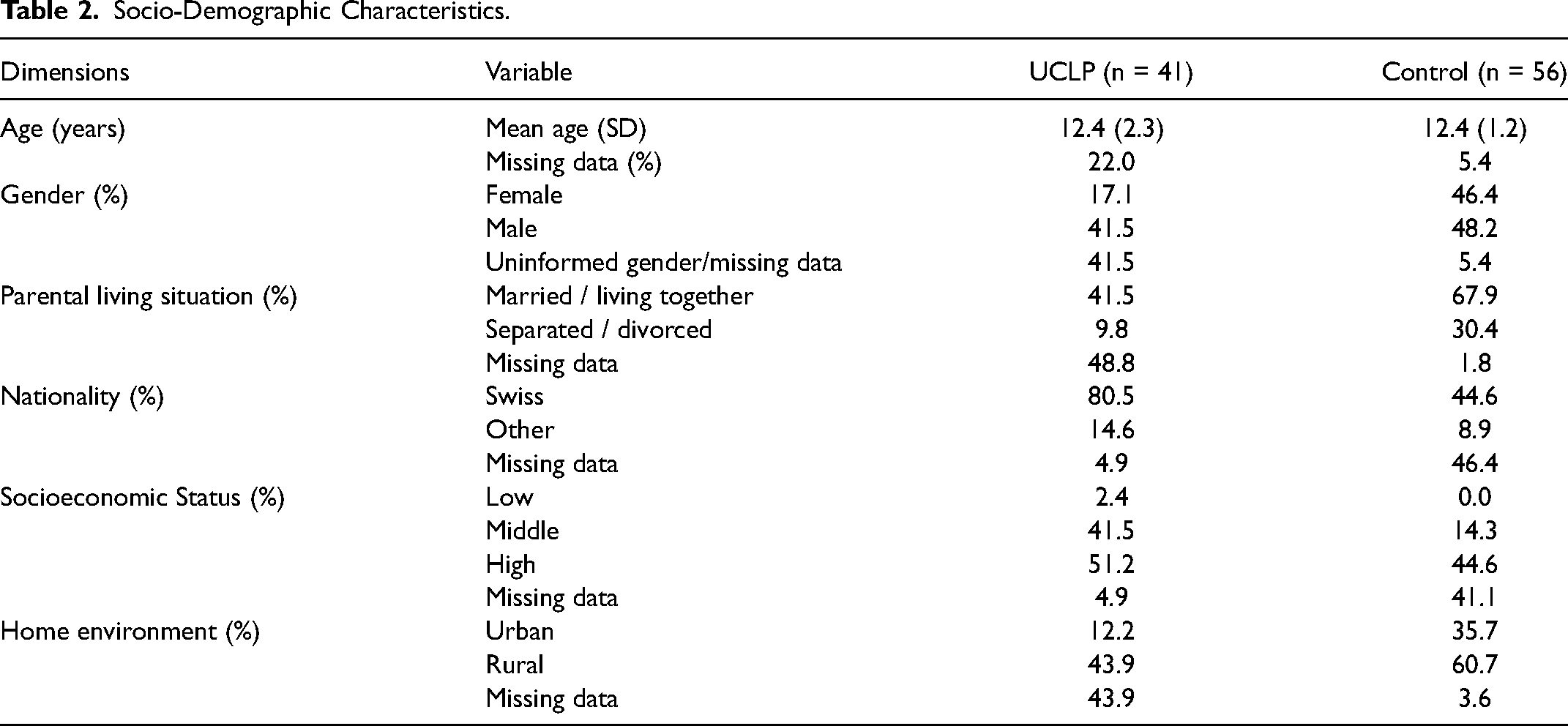
Given the high proportion of missing data, it is not possible to assess precisely the socio-demographic composition of the groups. However, statistical analyses run on valid data revealed no significant differences between the groups. Although the absolute difference in gender ratio between the two groups may be striking, the statistical difference did not reach significance. Consequently, we will not discuss potential implications on results.
Psychological Well-Being in Youths Born with a UCLP Compared to Control Group
Descriptive and Between-Group Comparisons in Psychological Well-Being.
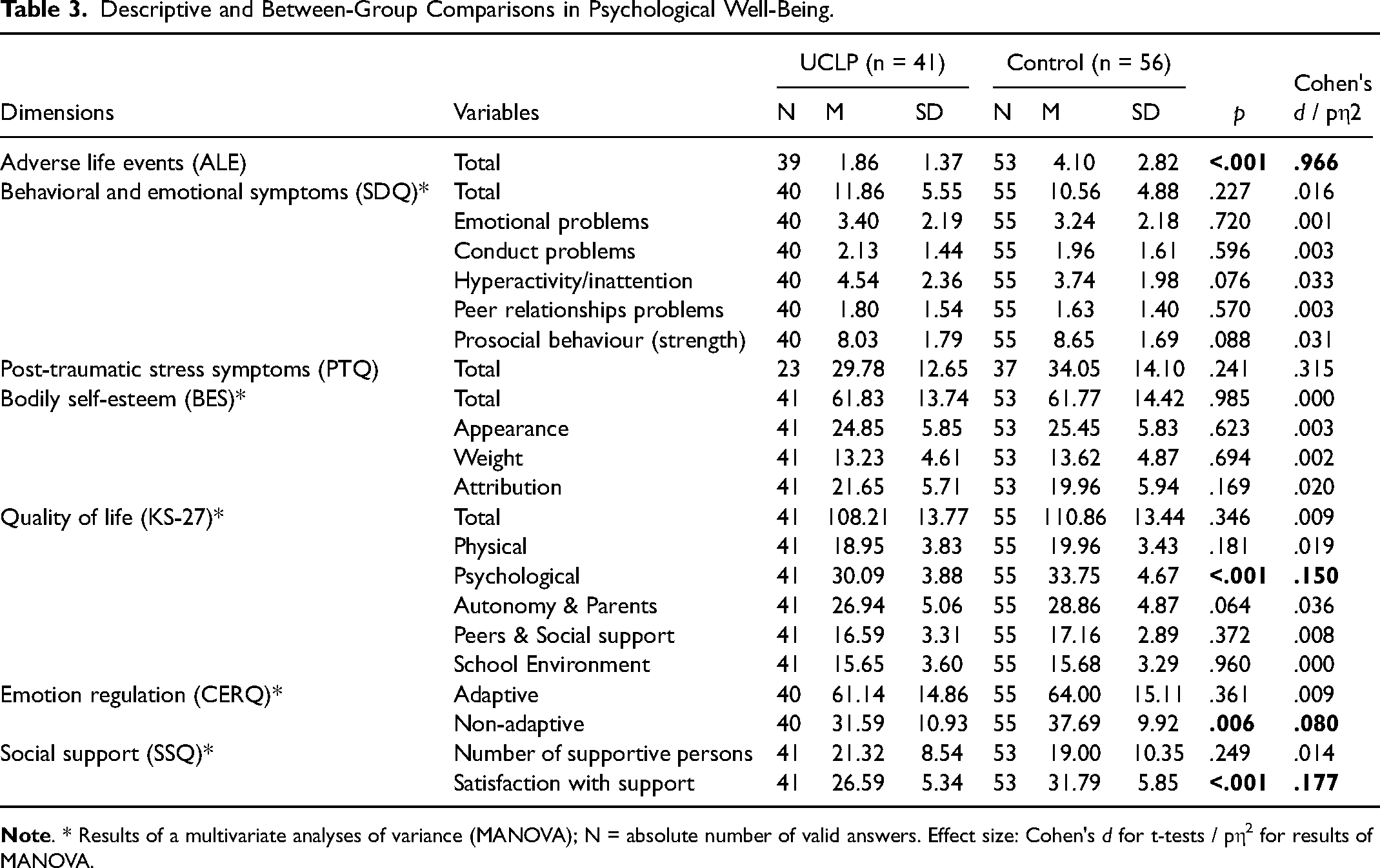
We observed significant lower scores for ALE (t(90) = 4.58, P < .001, Cohen's d = .966), lower scores for the psychological subscale of quality of life (F(1,96) = 16.63, P < .001, pη2 = .150), lower scores for non-adaptive emotion regulation (F(1,95) = 8.05, P = .006, pη2 = .080) and lower scores for satisfaction regarding social support (F(1,94) = 19.75, P < .001, pη2 = .177) reported by youths born with a UCLP compared to their matched peers (see Table 3).
Relationships between Dimensions Encompassed in Psychological Well-Being
Bravais-Pearson Coefficient of Correlations Between Dimensions Encompassed in Psychological Well-Being, in the UCLP Group.
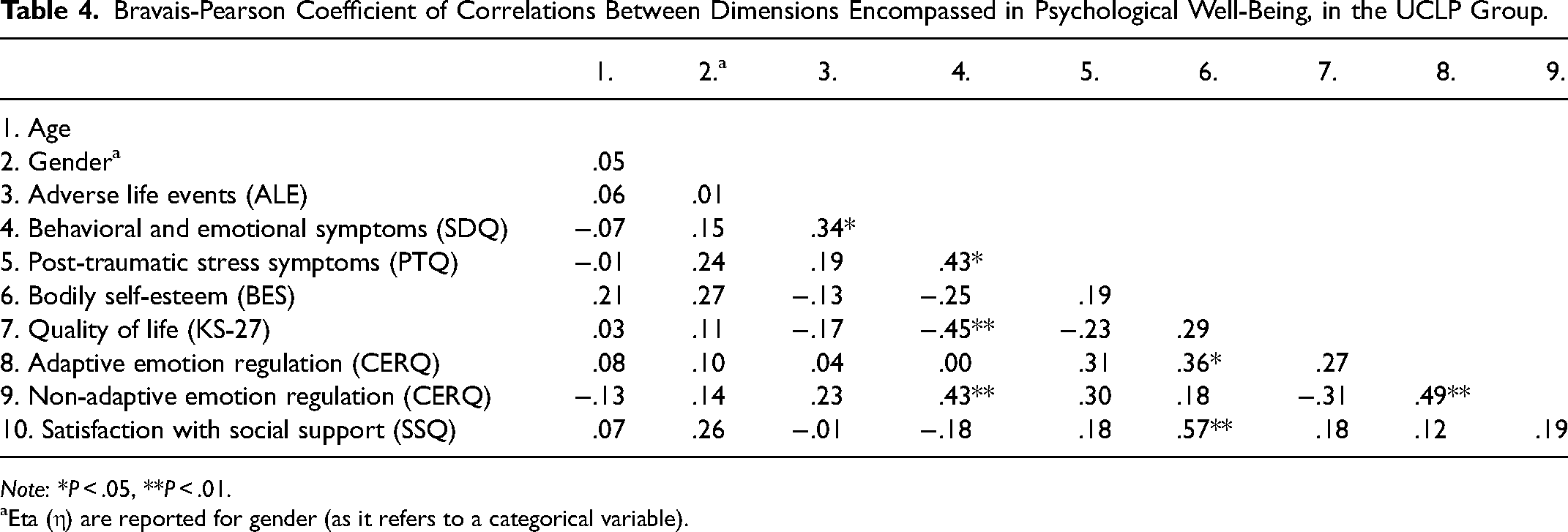
Note: *P < .05, **P < .01.
Eta (η) are reported for gender (as it refers to a categorical variable).
No dimension showed an association with age nor gender. We observed that higher scores for behavioral and emotional symptoms were significantly associated with higher scores for post-traumatic stress symptoms (r = .43, P = .048), with higher scores for non-adaptive emotion regulation (r = .43, P = .007) and with a higher number of ALE (r = .34, P = .038). Higher scores for behavioral and emotional symptoms were correlated to lower scores for quality of life (r = −.45, P = .004). Moreover, we found that higher scores for bodily self-esteem were significantly associated with higher scores for adaptive emotion regulation (r = .36, P = .023) and with higher scores for satisfaction with social support (r = .57, P < .001). Finally, we observed that higher scores for adaptive emotion regulation were associated with higher scores for non-adaptive emotion regulation (r = .49, P = .001). Table 4 reports the Bravais-Pearson correlation coefficients between dimensions encompassed in psychological well-being, in the UCLP group (for the control group see Table S1).
Discussion
Our study, which aimed firstly to compare different dimensions of psychological well-being between the two groups, found only four measures to be significantly different in youths born with a UCLP compared to typically-developing children and adolescents: less ALE, lower psychological quality of life, less non-adaptive emotion regulation and lower satisfaction regarding social support. The findings did not fit with our prior hypotheses, since some factors we expected to be affected were not (eg, bodily self-esteem, most dimensions of quality of life, behavioral and emotional difficulties).
The second aim of our study was to assess the relationships between the dimensions encompassed in psychological well-being in youths with UCLP. Several findings were consistent with our hypotheses, including associations of behavioral and emotional difficulties with non-adaptive emotion regulation, as well as with ALE, and of bodily self-esteem with social support satisfaction. Other associations were not as we predicted, such as behavioral and emotional difficulties with lower quality of life and bodily self-esteem with adaptive emotion regulation.
Psychological Well-Being in Youths Born with a UCLP Compared to Control Group
Adverse Life Events
First, participants with UCLP reported fewer ALE compared to the control group. The average number of ALE reported by youths born with a UCLP was between one and two. This result is difficult to compare to those of the study of Ponton et al. 11 (in which there was no comparison with a control group), because the items (life events) assessed in their questionnaires are different than those of our questionnaire, and because their questionnaire covered adverse childhood experiences that occurred at any point during the child's life, whereas our questionnaire focused on the last year. Nevertheless, the low number of ALE reported by our clinical group (on average 1.86 out of 25 items) seems aligned to what they reported as a low number of ALE (0 or 1 for the majority of children). It is difficult to explain the group-difference for ALE, given the measures included in this study and the lack of consistent literature on this topic. Further specific studies are needed to confirm the presence of a difference between the two groups and to better understand the underlying mechanisms.
Psychological Quality of Life
As with previous literature reporting inconsistent evidence of lower quality of life in youths born with UCLP,3,6,7 we observed a significant difference between the two groups only in the psychological dimension of the quality of life, which the UCLP group reported to be lower. This confirms a possible vulnerability in children and adolescents born with a UCLP, although it should not be over-interpreted, since the other four dimensions of quality of life (physical, autonomy & parents, peers & social support, school environment) showed no group-difference. A decreased psychological quality of life may be explained by the fact that being born with a UCLP implies various physical and functional differences with others, which can be difficult to manage and be the source of some psychological discomfort in daily life.
Emotion Regulation
Youths born with UCLP reported lower non-adaptive emotion regulation compared to their matched peers. This result is consistent with those of Guillén et al, 16 who found lower non-adaptive emotion regulation (ie, rumination and catastrophizing) in young people with UCLP. Berger et al., 48 too, observed rather adaptive emotion regulation strategies in children born with a UCLP (with a maximum prevalence of resignation, social support and distraction), in line with Branson et al.'s meta-analysis, 4 showing good emotion regulation skills in this population. The less frequent use of non-adaptive emotion regulation reported by young people born with a UCLP could be explained by a number of factors beyond what was measured in this study, such as increased parental support, access to professional support, increased resilience in response to potential stressors, or other factors.
Social Support
Concerning lower satisfaction with social support as reported by the UCLP group, which has already been observed by Ponton et al., 11 several hypotheses may explain this result, such as experiencing social stigma. Berger and Dalton 48 hypothesized that using avoidant strategies like social withdrawal to cope with difficult situations may be easier for individuals with a cleft. Difficulties with social situations may impact both the formation of friendships and their perceived need for support. This is an important area of study for future research.
Dimensions Showing No Difference Between the Two Groups (ie, Quality of Life, Behavioral and Emotional Symptoms, Bodily Self-Esteem)
Most of the quality of life dimensions (except psychological quality of life) investigated by our questionnaires showed no significant difference between the two groups, as well as bodily self-esteem, behavioral and emotional symptoms and post-traumatic stress symptoms. This is consistent with the findings of the meta-analysis by Branson et al., 4 indicating that the overall psychological outcomes appear to be similar to the non-affected population, and more specifically, similar to their meta-analysis of the SDQ results by self-reports, which revealed similar levels of behavioral and emotional symptoms compared to the non-affected cohorts. As explained by De Oliveira et al., 49 these patients may have good access to interdisciplinary health services and the care received may reduce the magnitude and psychosocial impact of the physical and functional differences that may affect them. Psychological consultation and support offered as part of multidisciplinary team care starting at the time of diagnosis throughout early adulthood may be a protective factor resulting in similar psychosocial adjustment to peers without a cleft.
Relationships Between Dimensions Encompassed in Psychological Well-Being
Factors Associated with Behavioral and Emotional Symptoms
Consistent with previous studies in youths born with UCLP as well as in the general population, we observed an association between higher non-adaptive emotion regulation and more behavioral and emotional symptoms13,50,51 and between more behavioral and emotional symptoms and lower quality of life.6,21 Non-adaptive strategies have, by definition, deleterious effects on psychological functioning, which can lead to the occurrence of behavioral or emotional difficulties. These symptoms obviously have an impact on the child's psychosocial functioning, and therefore probably on his or her overall quality of life, as we also observed.
We also found an association between ALE and behavioral and emotional symptoms. The association between recent negative life events and psychopathological symptoms (eg, emotional or conduct disorders) has already been demonstrated in the general population.24–26 The association was considered transactional by March-Llanes et al., 25 which means that psychopathological symptoms could be a consequence as well as a cause of stressful situations experienced in adolescence, through circular mechanisms. In our specific population of youths with UCLP, this result may be useful to clinical practice (see Clinical Implications below).
Factors Associated with Bodily Self-Esteem
Regarding bodily self-esteem, which was described by some studies as a vulnerability in youths born with UCLP, 4 we identified that it was correlated with adaptive emotion regulation. Through this, we may understand that adaptive emotion regulation strategies are necessary to maintain a positive bodily self-esteem despite the alteration of facial appearance, for example by minimizing the importance of one's appearance. As Guillén et al. 16 have hypothesized, those children's ability to regulate their possible dissatisfaction with appearance may act as a protective factor against the negative effects of stress and help to minimize the internalization of problems. Likewise, Crerand et al. 9 pointed out that adolescents with craniofacial conditions report significantly less investment in their appearance compared to unaffected adolescents and suggested that this may indicate an adaptive or protective strategy of minimizing the importance of appearance.
In our results, bodily self-esteem was also correlated with satisfaction with social support. This suggests that the latter is a protective factor; Stock and Feragen 8 also observed that ratings of physical appearance were significantly associated with social experiences in youths born with UCLP. Nevertheless, these two dimensions have been little studied together in this population, so this remains an area for future research.
Clinical Implications
Our investigations of the dimensions that contribute to the psychological well-being of youths born with a UCLP are overall reassuring. However, as previous literature has already pointed out, children and adolescents born with a UCLP are specifically at risk in terms of the psychological dimension of their quality of life, so this aspect should be seriously investigated by the health professionals who treat them. This investigation could allow to detect the youths most affected by their medical condition and to support them, for example by strengthening or adding professional psychological follow-up. Youths born with a UCLP also show protective factors such as less ALE and lower use of non-adaptive emotion regulation, which should be taken into account.
From a clinical perspective, studying the relationships between dimensions encompassed in psychological well-being may help to identify the youths at greater risk of difficulties, and may also indicate which interventions might help to improve aspects of their well-being. For example, given that ALE are associated with behavioral and emotional symptoms, screening for these life events could allow to identify children and adolescents at risk of developing these difficulties. This is particularly important as anxious children are more likely to be introverted, which may make their symptoms more difficult to detect and treat. 2 Ponton et al. 11 found that families are comfortable and willing to discuss these life events with their healthcare team in an appropriate setting. As children are usually followed for years by the same care team, those who experience multiple ALE such as moving, changing school, death of a relative, parental separation, may benefit from closer attention to identify and treat symptoms at an early stage. The association between ALE and behavioral and emotional symptoms is not limited to youths with UCLP, but the special attention they receive as part of their follow-up could be useful for higher detection of these situations than in the general population.
Another practical example, concerning the association between bodily self-esteem and adaptive emotion regulation, would be to develop a specific intervention for children and adolescents born with a UCLP who have low bodily self-esteem, which could focus on developing and strengthening adaptive emotion regulation strategies. No study has examined the effect of emotion regulation on bodily self-esteem but interventions based on teaching emotion regulation skills have shown good results in treating psychopathological disorders, 14 that's why the authors of this study suggest that some large-scale prevention efforts could target emotion regulation strategies. Some psychotherapeutic approaches already incorporate some form of emotion regulation training, as for example dialectical behavioral therapy, emotion focused therapy, acceptance and mindfulness-based therapy, and emotion-regulation therapy. 13
As we also observed a correlation between bodily self-esteem and satisfaction with social support, we imagine that training strategies based on children's social network (eg, parents, extended family, friends) could help them gain confidence in their appearance, as already mentioned by Feragen et al. 17 For example, psychological interventions could focus on working on the youth's social skills to enable them to make more friends and seek more help in others. Similarly, McMahon et al. 52 suggested that developing appropriate strategies to improve relationships can help counteract the negative effects of life stressors. For some families, offering family therapy to work on the social environment and adaptive coping strategies could also be effective.
Limitations
First, our results may be altered by recruitment bias. It is conceivable that children and adolescents born with UCLP who have the most difficult experiences of their condition may have refused to participate in the study, for example those with post-traumatic stress symptoms, who may tend to seek avoidance. Such a bias could make our results falsely reassuring. However, this bias may also be present in the control group (ie, avoidance of completing the questionnaire in case of negative psychosocial experiences), which would reduce the bias in the results.
On the other hand, children in the clinical group individually completed the questionnaires with the help of a member of the research team, which was not the case for the control group (two psychologists were present to answer questions in a whole class). Young people born with UCLP may therefore have felt less comfortable in openly confiding their psychological difficulties to someone they did not know and we may not have had access to the full extent of their psychosocial problems. Finally, between the parents’ and the child's perspective, we chose the child's, thinking that parents might not be aware of all their child's thoughts and perceptions. The inclusion of a dual perspective in future studies could thus make the assessment of the psychological well-being more complete.
Concerning socio-demographic data, the number of missing answers was very high, making it impossible to assess precisely the equivalence between the groups. Missing data could not be retrieved due to the anonymous nature of the data collection. Moreover, the fact that these data were parent-reported in the clinical group and child-reported in the control group generates a potential bias. However, all participants belong to the same geographical area and are within an inclusion age range, which can limit the variability. Likewise, we cannot state that there is no relationship between the socio-demographic variables and the psychological well-being dimensions, even though our results do not show any. For example, age impact on certain variables such as adverse life events (which were investigated only in the last year) might exist.
The questionnaire used to assess bodily self-esteem was not cleft-specific, in order for the results to be comparable to the control group. Nevertheless, a cleft-specific measure of bodily self-esteem might have been more accurate in understanding the relationships among variables in the clinical group. In addition, results for bodily self-esteem may be biased by concerns about weight (which is one of the three subscales in the BES questionnaire), so low scores may not be a consequence of facial scarring.
Regarding the correlations identified between the dimensions, it should be noted that we cannot know the direction of the associations. Longitudinal studies could help to better understand the possible causal relationships and the psychological well-being dimensions.
Finally, there are so many variables involved in psychological well-being (ie, environmental, personal, systemic) that it is impossible to consider them all at once. We chose a part of them that we found appropriate, but some of our results may be biased by factors that we have not considered. Further research including even more variables than here (eg, other dimensions of self-concept than just bodily self-esteem) could help to better understand the psychological well-being of children and adolescents born with UCLP. These findings concur with those of Bous et al., 22 suggesting that future studies may explore additional factors that could explain more of the variance, or use qualitative interviews.
Conclusions
This study provides a clinical perspective on the psychological well-being of children and adolescents born with a UCLP, by considering and analyzing together several closely related dimensions. Our results align with evidence from previous studies, showing that most of these outcomes are comparable to the general population. Nevertheless, our findings highlight the need for clinicians to pay attention to the psychological dimension of the quality of life of these youths, which may represent a vulnerability, supporting the need to include mental health specialists within the offered multidisciplinary care. Importantly, we also identify some protective factors in this population (ie, lower use of non-adaptive emotion regulation, less ALE). Secondly, our multi-dimensional perspective provides clues for a more detailed understanding of the interactions between dimensions encompassed in their psychological well-being. The highlighted correlations between dimensions could allow clinicians to identify small groups of children and adolescents who are at higher risk of difficulties and provide clues for targeted, specific and early interventions, as also suggested by Feragen and Stock. 23
Implications for Future Research
The disparities observed in the previous literature regarding several dimensions of psychological well-being of youths born with a UCLP suggest that further research is needed, with a multi-dimensional perspective such as ours, to clarify the extent of the psychological, social and functional impacts of being born with a UCLP. Such a multi-dimensional understanding of the psychological well-being of these youths would allow for the identification of more applicable avenues of clinical practice, that take into account the complexity of the individual person.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231219418 - Supplemental material for Assessment of Multiple Dimensions of Psychological Well-Being in Swiss Youth Born with a Unilateral Cleft Lip and Palate
Supplemental material, sj-docx-1-cpc-10.1177_10556656231219418 for Assessment of Multiple Dimensions of Psychological Well-Being in Swiss Youth Born with a Unilateral Cleft Lip and Palate by Solène Lecommandeur, MSc, Anthony de Buys Roessingh, MD, PhD, Lisa Dumont, MSc, Lucia Camenzind, MSc, Stéphanie Habersaat, PhD, Daniel S. Schechter, MD, Christelle Jung, BSc, Josée Despars, PhD, Sébastien Urben, MD, PhD, and Mathilde Morisod Harari, MD, MER in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
We would like to thank the youths and their families who took part to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.