
Abstract
Alveolar bone grafting (ABG) in bilateral cleft lip and palate (BCLP) patients provides a reconstructive challenge. We present a novel technique of combining autologous iliac crest bone graft (ICBG) with recombinant human bone morphogenic protein 2 (rhBMP-2) and cellular bone matrix (CBM) for ABG in BCLP patients. Complete bone fill occurred in 90% of patients, with 100% having bilateral canine eruption. No patients required repeat ABG, and no significant complications were reported. The alveolar cleft gap volume significantly decreased with an improvement of 75.87%. ABG with autologous ICBG with rhBMP-2 and CBM is an effective technique for patients with BCLP.
Introduction
The revision rate of alveolar bone grafting (ABG) in bilateral cleft lip and palate (BCLP), utilizing autologous iliac crest bone graft (ICBG), has been reported to be 20-46%.1-3 Patients needing revisions commonly undergo an average of two additional surgeries. 4 The relatively higher revision rate, compared to patients with a unilateral cleft, can be attributed to increased pre-maxilla mobility and a wider alveolar cleft.3,5 The high rate of ABG failure leads to increased stress for the patient and their family, confounded by increased operative risk, exposure to anesthesia, and financial cost.
While most cleft surgeons still utilize ICBG for ABG, the tendency to employ non-autologous materials to replace or supplement reconstruction is increasing. 6 Recombinant human bone morphogenic protein 2 (rhBMP-2) is a transforming growth factor with osteoinductive properties. Using rhBMP-2 with a de-cellularized scaffold in UCLP ABG is an acceptable alternative to ICBG.7-10 Cellular bone matrix (CBM) provides a similar osteoconductive scaffold with the additional benefit of seeded mesenchymal stem cells (MSC) capable of osteoblastic differentiation.11-13 These matrices have primarily been used for spinal fusion and have shown successful outcomes in limited studies. 13
This study reports our technique's clinical and volumetric outcomes for BCLP ABG using autologous ICBG combined with rhBMP-2 and CBM. Our technique aims to improve bone fill to allow for maxillary arch stability, closure of the oro-nasal fistula, and dental eruption. Additionally, we aim to decrease the re-operation rate to prevent the excess burden on patients and their families and the risks and cost associated with revision ABG.
Methods
A retrospective review of patients with BCLP who underwent ABG with autologous ICBG with rhBMP-2 and CBM was performed following institutional review board approval by the University of Texas Southwestern Medical Center. All patients indicated for alveolar bone grafting, and the diagnosis of bilateral cleft lip and palate were selected. The 20 patients included were sequential, and all were treated with the combination of ICBG with rhBMP-2 and CBM between 2018 and 2022. All patients had adequate records and were included in the study.
Medical records were reviewed to collect demographic, operative, and post-operative information. Senior author YJP completed a comprehensive physical exam and reviewed dental radiographs and cone beam computed tomography (CBCT) for an orthodontic evaluation. Cleft alveolus volume was evaluated using CBCT performed pre-operatively and six months post-operatively. Manual CBCT segmentation of the empty alveolar gap was performed using Mimics 25.0 (Materialise, Belgium), and volume calculations were performed using 3-Matic 17.0 (Materialise, Belgium). The segmentation borders encompassed the pyriform aperture superiorly, the alveolar margin inferiorly, and the adjacent teeth alveolus (Figure 1). The volume occupied by dental eruption into the alveolar cleft was not included. The alveolar cleft width was measured using pre-operative CBCT.
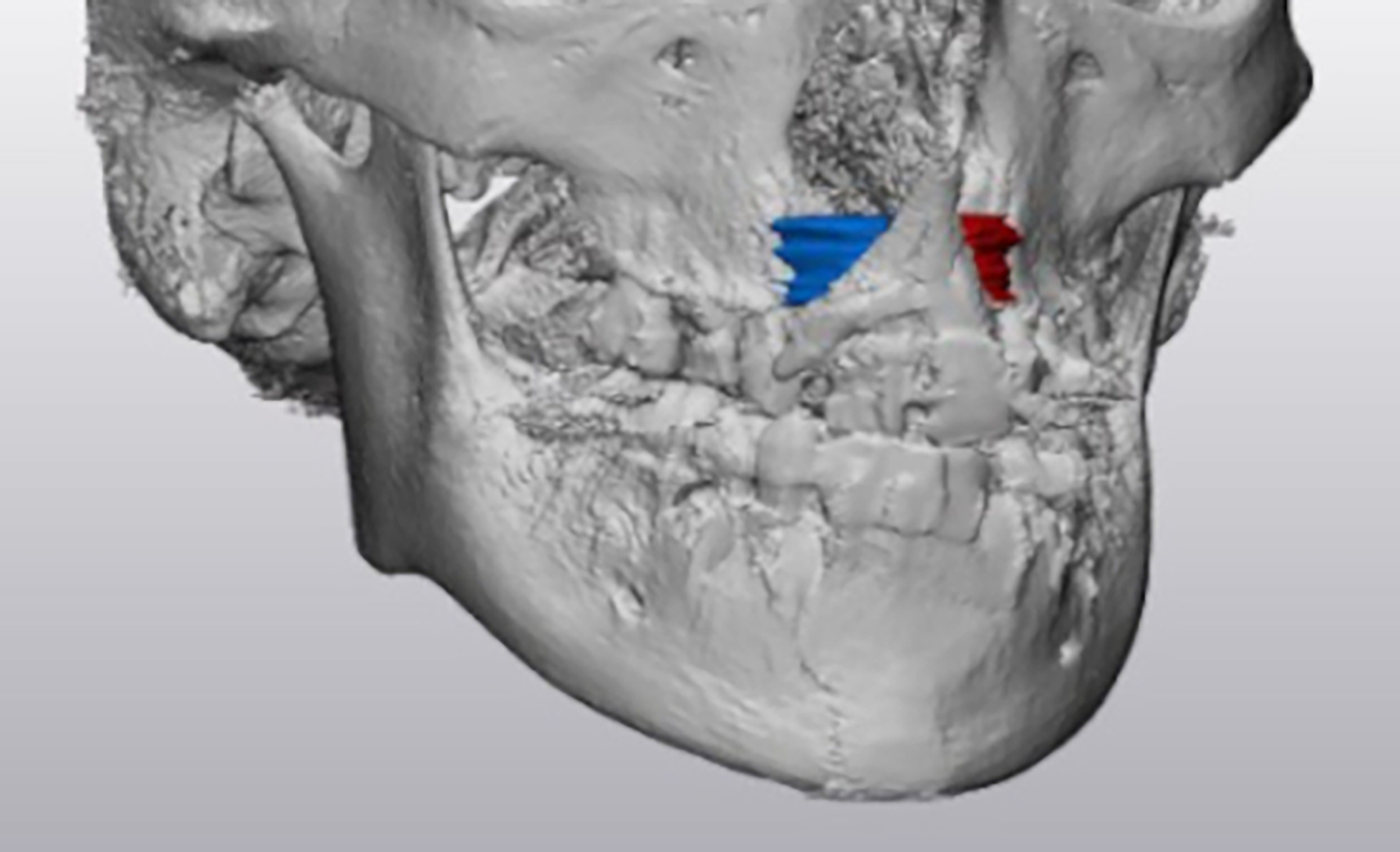
Alveolar cleft gap volume segmentation boards with pyriform aperture superiorly, alveolar margin inferiorly, and adjacent teeth alveolus.
Operative Technique
All patients were treated with simultaneous bilateral procedures. The ICBG was harvested through a three-centimeter incision, inferolateral to the anterior superior iliac spine. Monopolar electrocautery was used through the fascial and muscle layers down to the cartilage cap, which was removed temporarily, revealing the underlying bone. A six-millimeter trephine was used to create three cores, and curettage was used between the cores to harvest cancellous bone. The bony donor site was filled with gelfoam, the cartilage cap was replaced, and muscle, fascia, and skin were closed in layers. In the mouth, the mucoperiosteum at both edges of the alveolar cleft margins was incised and elevated up to the level of the pyriform, and the incision was continued laterally to the cleft along the gingival margin. A superiorly based mucoperiosteum flap and gingiva were raised and mobilized to cover the cleft through a lateral back cut and periosteal scoring. The premaxilla is minimally dissected to minimize the risk of ischemia. Teeth in the cleft were extracted per the orthodontic plan. If present, the fistula running through the cleft was divided, and the edges of the fistula were brought together cranially to reconstruct the nasal floor and caudally to reconstruct the palate. A watertight pocket is created centrally to place the ICBG with rhBMP-2 (Infuse Bone Graft, Medtronic) and CBM (Trinity Elite, MTF Biologics). An average of 2.32 cc: 1 cm3 of iliac crest, 1.75 cc:1 cm3, and 1.50 cc: 1 cm3 CBM was utilized. The proportion of product utilized was based on pre-portioned volumes commercially available and gap volume requirements. Patients know that recombinant BMP is an off-label use in skeletally immature patients, and product brochures are given and discussed in advance.
Results
A total of 20 patients with BCLP who underwent ABG with ICBG with rhBMP-2 and CBM were identified (Table 1). All patients had pre-operative rapid palatal expander, with 30.0% having a face mask. Rapid palatal expander was switched to transpalatal arch after completion of expansion and before ABG. The patients were, on average, 10.57
Bilateral Cleft Demographics and Operative Outcomes.
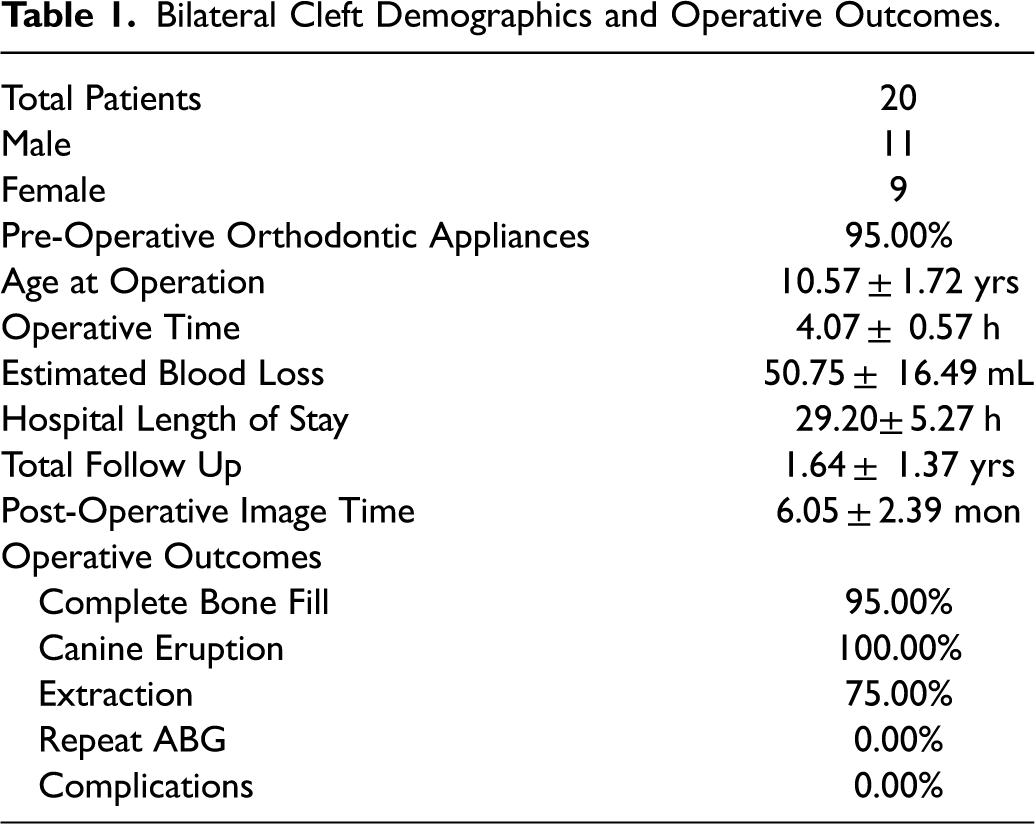
Patients were followed post-operatively for 19.68
Bilateral Cleft Alveolar gap Volume.
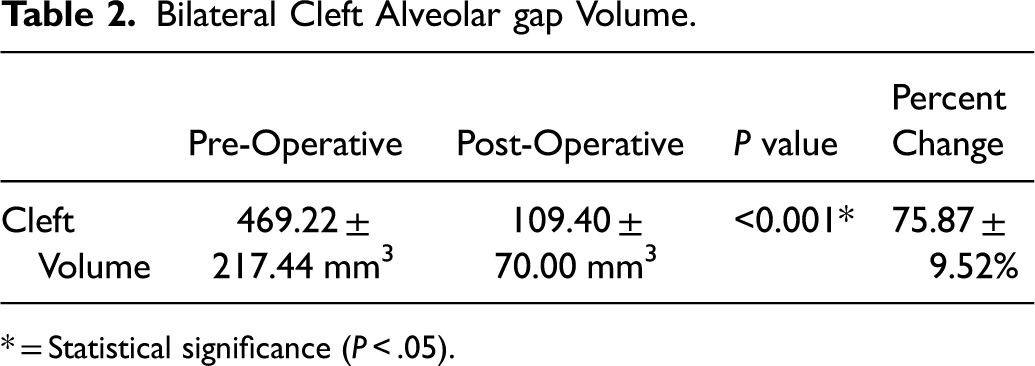
* = Statistical significance (P < .05).
Discussion
The high revision rate of ABG in patients with a bilateral cleft is hypothesized to be due to the mobility of the pre-maxilla segment and often increased width of the alveolar cleft.3,5 The reported rate of ABG revision with ICBG is between 20-46%.1-3 Zubovic et al. demonstrated that the use of CT has significantly increased the revision rate of ABG compared to traditional clinical and dental radiographic assessment. 2 In their patients with BCLP, 69% had revision following CT evaluation, while only 11% had revision following traditional evaluation. These findings indicate that the already high revision rate in older reports may have been artificially low before the implementation of CT evaluation. These previously reported radiographic evaluated only the vertical dimension of grafting without providing information of the transverse dimension.14-17 Patients with BCLP undergo multiple operations over the course of cleft care, and an additional revision surgery increases the stress burden to the patient and their family, operative risk, anesthesia exposure, and financial cost. This study combines ICBG with rhBMP-2 and CBM for ABG to address the high revision rate in patients with BCLP.
ICBG remains the most commonly utilized technique for ABG in BCLP; however, the use of non-autologous materials to replace or supplement reconstruction is increasing. 6 Qamar et al., in a survey of cleft surgeons, found that 23% reported using allograft bone products, and 31% employed rhBMP-2. 6 We believe the synergistic effects of combing iliac crest bone graft with these non-autologous products may provide a substrate due to the osteoinductive, osteoconductive, and osteogenic properties.
Recombinant human bone morphogenic protein 2 (rhBMP-2) is a transforming growth factor with osteoinductive properties that promotes bone growth and repair.7-10 CBM is composed of an extracellular bone matrix with osteoconductive potential and provides volume to prevent the collapse of the alveolar pocket.11-13 The CBM is also seeded with osteogenic mesenchymal stem cells (MSC) capable of osteoblastic differentiation. The volumetric benefit combined osteogenic properties provide a valuable adjunct for ABG. Overall, we believe our combination provides the ideal environment for promotion of bone graft fill within the alveolar gap.
Our cohort of 20 patients treated with ICBG with rhBMP-2 and CBM for ABG in BCLP found clinical success in all patients with canine eruption, and 95% of alveolar clefts had a complete bone fill. The volume of the bilateral cleft was significantly reduced, with decreased volume by 75.9%. The remaining volume was occupied by dental eruption into the alveolar gap. The two patients who had unilateral incomplete bone fill had 63.32% and 58.11% non-dental eruption fill respectively. Liang et al. evaluated volumetric bone fill in a combined cohort of UCLP and BCLP patients using CBCT and found only 32.5% fill in the group who underwent ICBG only. 10 While no patients in our cohort received repeat ABG, two patients did not have complete alveolar cleft fill on a single side. The possible revision rate of 10% is well below the high rates of revision reported in the literature.1-3 Additionally, no complications occurred following ABG, a decrease compared to ICBG results previously reported. Goudy et al., in a review of 42 patients with BCLP, found a post-operative infection rate of 20%. 3
The major limitation of this technique is the cost of non-autologous products. The cost of the rhBMP-2 and CBM will differ by institution, but if the approach prevents a revision operation, the overall cost is offset by the reduction in anesthesia, pharmacy, and operating room costs. The current case series is not able to differentiate between the individual effects of rhBMP-2, CBM, and ICBG. Future studies should differentiate the individual effects of each component to understand the most efficacious and cost-efficient option for ABG. Another limitation is the small sample size, as the results are preliminary data collection, which limits the power of statistical analysis. Our average follow-up was 1.6 years; long-term evaluation should be completed in future studies.
Conclusion
This study presents a novel effective technique using ICBG combined with rhBMP-2 and CBM for ABG in BCLP patients. Alveolar cleft gap fill was successful clinically with canine eruption and volumetrically with 75.9% improvement. No patients underwent revision ABG operation or had post-operative complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.