
Abstract
The aesthetic management of a case involving a high smile line in a patient with a cleft lip and palate can be difficult. In this report, we look at a complex case of a patient with a unilateral cleft lip and palate which required a multidisciplinary approach involving crown lengthening, extraction of a maxillary right central incisor and fabrication of a 4-unit fixed partial denture to replace this tooth and the adjacent absent maxillary right lateral incisor with use of gingival porcelain in order to improve the aesthetics of the patient's smile.
Introduction
Cleft lip and/or palate (CL/P) is a range of genetic disorders of unknown aetiology 1 affecting approximately 1 in 700 live births.2,3 It has a three-dimensional effect on the growth of the alveolus with the lesser segment rotated superiorly and medially during development. 4 Even when surgically repaired the scar tissue can have long term effects on the alveolus. 5 One or more anterior teeth may be congenitally absent, malformed or malpositioned; maxillary lateral incisors are the most commonly affected teeth. 6 These anomalies and their effect on facial aesthetics can psychologically impact patients. 3 Multidisciplinary teams can provide a wide range of treatment options appropriate to patient needs.1,3,7 Sometimes surgical and orthodontic treatment alone be insufficient to improve the patient's smile and advanced prosthodontic treatment may be indicated; however, prolonged orthodontic and surgical treatment times may cause patient fatigue before prosthodontics can be commenced. 8 In this clinical report, we review a complex case involving the multidisciplinary restorative management of a patient with CL/P presenting for further treatment to address aesthetic concerns.
Clinical Report
A 24 year old woman was referred to the Prosthodontic Cleft Lip and Palate Unit to address her aesthetic concerns. About to complete a second course of orthodontic treatment to correct lower incisor crowding, she had previously undergone multiple corrective surgeries, including placement of an iliac crest bone graft to the cleft site and multiple lip revisions, speech and language therapy, and one previous course of orthodontic treatment lasting three years. Her chief complaint was she was unhappy with the appearance of her teeth, particularly when smiling. A resin-bonded prosthesis had been placed to restore the missing maxillary right lateral incisor.
On examination, there was no active caries or periodontal disease evident. There was no mobility to any of teeth and all teeth were vital to sensitivity testing. The patient's profile was good and there was a Class I orthodontic relationship and there was no mobility between maxillary segments. An aesthetic analysis revealed a number of issues. There was asymmetry of the occlusal plane with the teeth on the right side being higher than those on the left, as well as asymmetry of the gingival margin line, distortion of the gingival zenith architecture and asymmetry of gingiva on smiling. The maxillary teeth did not follow the curvature of the lower lip, and the buccal corridor was wider on the left side than on the right side. Finally, the midline was off-center and canted inferiorly towards the right; the maxillary right central incisor displayed 3 mm gingival recession and the maxillary right lateral incisor was missing and replaced by a resin-bonded prosthesis. The pontic was longer than ideal due to a deficient alveolus in the cleft area. (Figure 1) Radiographically, there was about 25-30% bone loss around the distal of the maxillary right central incisor and the root of this tooth was angled distally and was shorter compared to the adjacent maxillary left central incisor (Figure 2a). There was no bone loss evident, however, around the maxillary left central incisor and maxillary right canine and the roots of these teeth featured favourable crown to root ratio (Figure 2a and b).

Preoperative appearance. Extraoral preoperative smile. Dentition is asymmetrical.
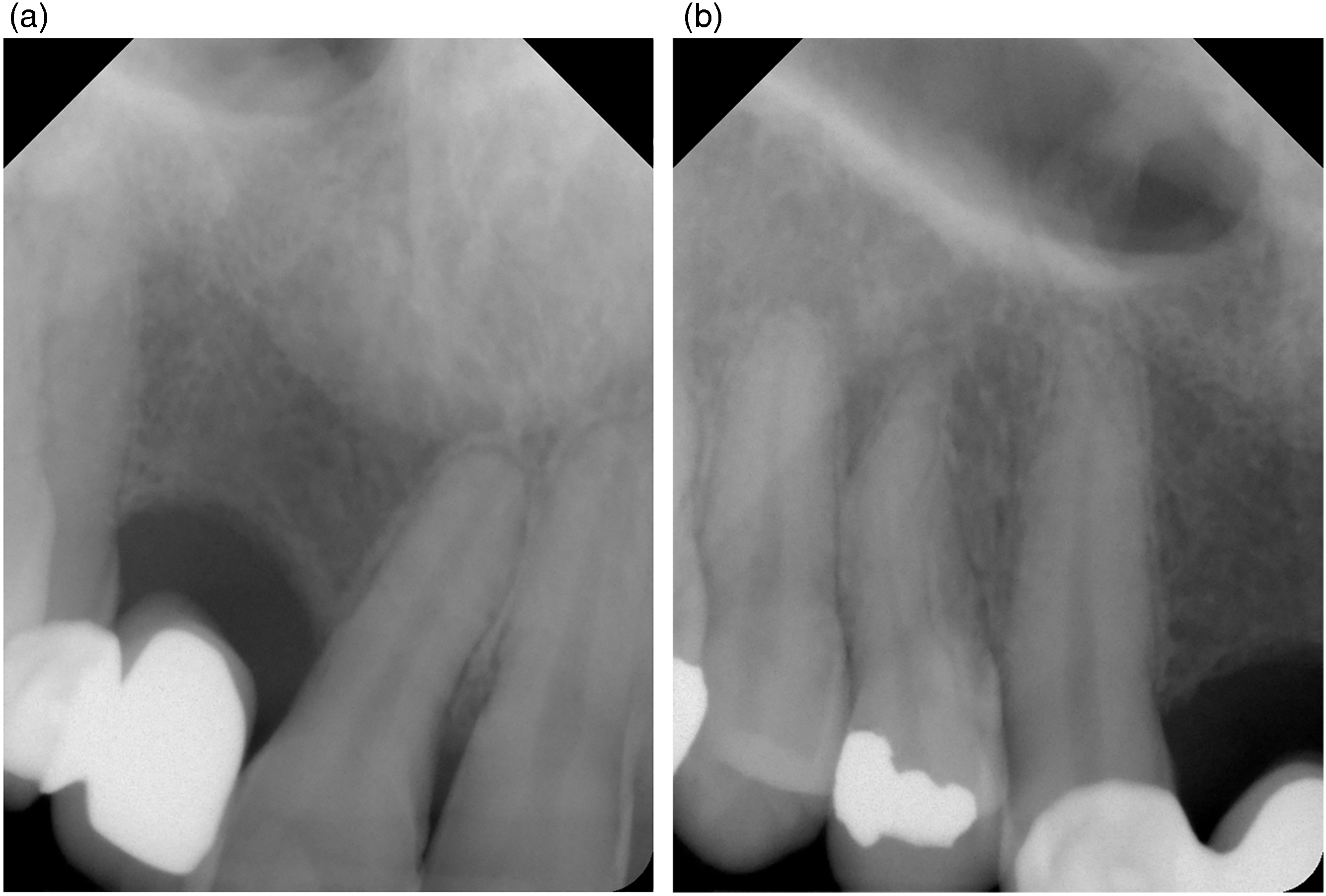
(a) Pre-operative periapical radiograph of maxillary right central incisor. Of note is approximately 20-30% bone loss on the distal aspect of the maxillary right central incisor; the mesial aspect, and the adjacent maxillary left central incisor, have minimal bone loss. The root of the right central incisor is also shorter than that of the left central incisor, and is angled distally towards the site of the repaired cleft palate. (b) Pre-operative periapical radiograph of maxillary right canine. Note no bone loss evident.
The advantages and disadvantages of maxillary orthodontic retreatment followed by restorative treatment versus restorative treatment alone were discussed with the patient. Keen to have the shortest and simplest treatment with a predictable outcome, the restorative-only solution was agreed on and completed. Treatment commenced with crown lengthening of the teeth in the maxillary left quadrant (from maxillary left central incisor to maxillary left second premolar): this involved the raising of a full thickness mucoperiosteal flap, removal of about 2 mm of alveolar bone around the teeth and closure with an apically positioned flap. This reduced gingival show on the right while smiling and minimized the discrepancy between right and left gingival margin heights. This was allowed to heal for six weeks, with a periodontal dressing (Coe-Pak, GC Europe) in situ for one week post-operatively. (Figure 3)

Post-crown lengthening to achieve symmetric gingival lines of zenith. Periodontal dressing in situ.
As the maxillary right canine and maxillary left central incisor were of favourable crown to root ratio, were unrestored and featured no periodontal involvement, a 4-unit conventional fixed partial denture, extending from the maxillary right canine to the maxillary left central incisor, was planned to correct the occlusal plane asymmetry. This required removal of the existing resin-bonded prosthesis and the maxillary right central incisor was extracted as its position compromised the aesthetic result. A provisional Rochette resin-bonded prosthesis to replace the maxillary right central and lateral incisors was placed during the healing process.
One month later the maxillary right canine and maxillary left central incisor were prepared for a definitive 4-unit zirconia fixed partial denture; a provisional acrylic fixed partial denture was used as an interim restoration. Following a course of night-time vital tooth bleaching using 10% carbamide, definitive impressions were taken 8 weeks later for the 4-unit zirconia fixed partial denture, with gingival porcelain cervically to correct the gingival margin line discrepancy.
Postoperatively, the patient received oral hygiene instruction and maxillary and mandibular Essix retainers were fabricated to prevent relapse. The patient subsequently had Botox and micropigmentation of the upper left lip completed outside of the clinic to further enhance her aesthetic result. She was reviewed annually for 2 years post-treatment before discontinuing due to family circumstances. 3 years later (5 years post-completion of treatment), she re-presented. She had not worn her retainers and there was orthodontic relapse on the maxillary and mandibular arches; the maxillary premolars had moved palatally and there was a crossbite on the right-side. (Figure 4) She elected for further prosthodontic treatment to further improve posterior arch aesthetics. She was counselled on the risk of further orthodontic relapse and need to continue wearing her Essix retainers daily.

Post-initial treatment view. Note crossbite has developed due to relapse of maxillary right premolars.
The treatment goal of making the arches as symmetrical as possible was achieved. The occlusal plane and the gingival margin line of the maxillary arch were improved and made as symmetrical as possible. The maxillary dentition follows the curvature of the lower lip, the buccal corridors are more symmetrical, the midline more vertical – albeit with a subtle cant towards the left - and the teeth whiter. Overall, the resulting smile is more attractive. While the subsequent relapse is disappointing, the patient is happy with the aesthetic outcome of the treatment. (Figure 5)

Final appearance. Extraoral postoperative smile.
Discussion
The aesthetic management of this patient was complex due to the issues present. The management can be categorised into three targets of treatment: gingival, dental, and facial.
Gingival
When smiling, an “aesthetic smile” is when the full crown of the tooth and between 1-2 mm of gingival margin is visible. 9 In an aesthetic smile, the gingival zenith point (GZP) of both maxillary central and lateral incisors lie distal to the vertical midline of the tooth itself while the GZP of the maxillary canine will coincide with the tooth's vertical midline. 10 Crown lengthening surgery can increase the clinical crown height, symmetrize the GZPs and reduce the gingival bulk that can characterize an unaesthetic high smile. 11
Dental
The dental component of an aesthetic smile has a number of features. The maxillary dental midline should coincide with the facial midline. When assessing this, one should extend an imaginary line from nasion to the cupid's bow of the philtrum; the dental midline should coincide with this. 12 Canting of the maxillary midline is considered to compromise dental aesthetics. Angulation of this midline by more than 10 degrees, or 2 mm, can be perceived as unattractive by laypersons, dentists and orthodontists.13,14 The curvature of the maxillary incisal edges should parallel the lower lip line on smiling, creating a “consonant” smile.15,16 Mesial inclination of maxillary incisors is seen as harmonious to an aesthetic smile.12,17
The shade of porcelain used in the upper dentition is important. The maxillary central incisors tend to be the lightest maxillary teeth by shade, the maxillary lateral incisors are of a similar hue but a lower value and the canines of an even lower value but increased chroma. 15 Gingival porcelain is an oft-neglected tool in the dentist's armamentarium but can be incredibly useful in a case, such as this; it was added cervically to the pontic of the prosthesis to camouflage the existing bony defect and avoid excessively long crowns. The buccal corridor is the area between the commissure of the lips and the buccal surface of the posterior teeth when smiling. 18 A smaller buccal corridor, or a broader smile, is viewed as more aesthetic than a wider buccal corridor. 19
Retainers, such as Essix or Hawley, are used to retain teeth in their corrected positions post-orthodontic and prosthodontic treatment. Relapse has a higher incidence in patients with CL/P and is often due to the contraction of palatal scar tissue. 5 All patients with CL/P should wear retainers nightly to avoid relapse which can occur at any stage, as evidence in this patient, and is a lifelong issue faced by this cohort of patients.
Facial
To further improve the “gummy smile,” botulinum toxin (Botox) was used. This causes paralysis to the administered muscles and lasts up to 3 months before its effects subside, requiring further administration. 20 Asymmetric administration, often to the levator labii superioris alaeque nasi muscle, can induce a more symmetrical upper lip on smiling. 21 Micropigmentation can be a useful adjunct to improve the asymmetrical upper lip. The pigment used should be nontoxic, nonallergenic and stable, and is injected between the superficial and middle dermis under aseptic conditions.22,23
Summary
Aesthetic management of patients with CL/P is often challenging due to the long phasic course of care in managing such patients from childhood, and is further compromised by facial, gingival, and local dental factors. In this case, a combination of crown lengthening on one side and the use of gingival porcelain on the other created a symmetrical smile; the final result was aided by use of micropigmentation and botulinum toxin use to further aid this symmetric appearance. The use of a conventional fixed partial denture allowed for the correction of the occlusal plane. The necessity for the continuous wearing of retainers is clearly illustrated in this case as there is a tendency for scar tissue from corrective childhood surgeries to cause arch constriction and subsequent relapse.
Footnotes
Author Contributions
Daniel Dilworth: writing – original draft. Emily Lordan: writing – original draft. Sittana Elfadil: writing – review and editing. Aisling O’Mahony: writing – review and editing; conceptualization; supervision.
Consent for Publication
Written informed consent for publication was obtained from the patient whose details and images were used in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.