
Abstract
Objective
To determine a baseline of anticipated change in nasolabial appearance following primary repair of unilateral cleft lip/palate and evaluate the degree to which revision surgery improves nasolabial appearance.
Design
Retrospective chart review.
Setting
Patients treated at the Lancaster Cleft Palate Clinic interdisciplinary clinic.
Patients
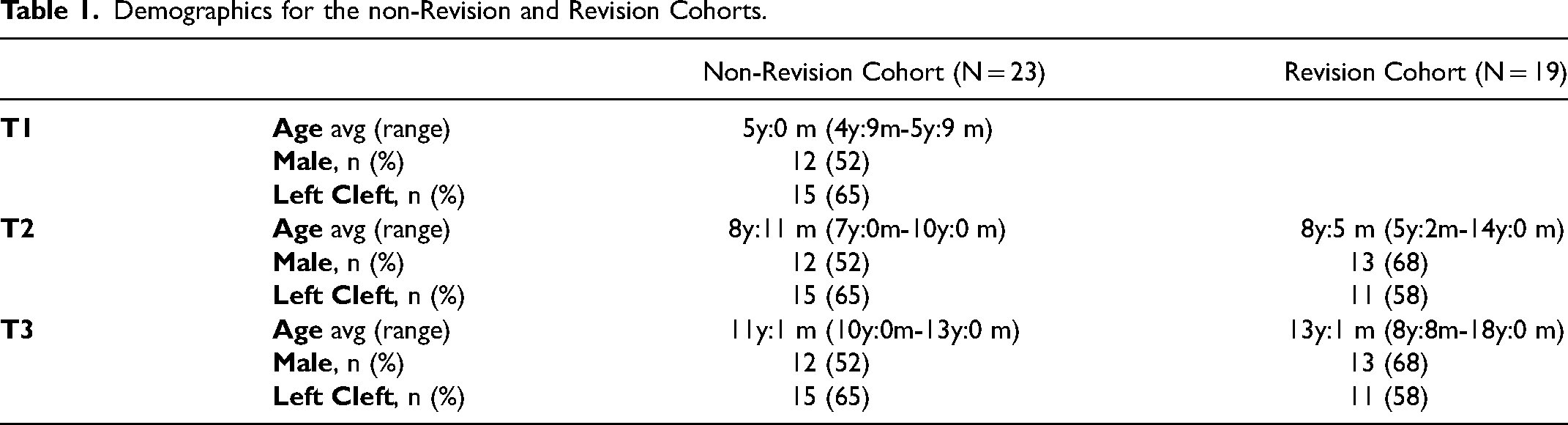
Twenty-three patients with complete unilateral cleft lip and palate who underwent primary surgical repair and 19 additional patients who underwent subsequent revision surgery were included.
Interventions
Patients in the non-revision group underwent a Tennison-Randall triangular flap lip repair at 3mo. Patients in the revision group underwent a modification of the Nakajima straight-line repair after primary Tennison-Randall triangular flap lip repair at an average age of 141mo.
Main Outcome Measures
A modification of the Asher-McDade Aesthetic Index was utilized to evaluate Nasolabial Frontal (NLF), Nasolabial Profile (NLP), Vermillion Border (VB), and total change in appearance. Scores for patients in the revision group were evaluated before and after revision while appearance for patients without revision was evaluated at 3 distinct ages. Scores were averaged across time-points and inter-rater reliability was assessed.
Results
Nasolabial appearance in the non-revision sample did not change significantly over time, except for nasal profile. Scores improved after revision surgery – NLP: 3.48 to 2.97, (p = 0.001); NLF: 3.50 to 2.95 (p = 0.001); and Total Nasolabial Score: 3.29 to 3.01 (p = 0.004), with no significant change in VB.
Conclusion
Decisions regarding need for nasolabial revision surgery may be made as early as 5yo with successful outcomes following secondary surgery improving appearance except for vermillion border appearance.
Introduction
Cleft lip and/or palate is the most common congenital craniofacial anomaly, with an incidence ranging from 1:500 to 1:700 live births, internationally. 1 Patients with clefts present with an array of facial abnormalities including facial asymmetry due to deviation of nasal tip, nasal flattening, premaxilla prominence in addition to a short columella, wide philtrum, and a deformed orbicularis oris ending at the cleft margins. 2 Surgical correction is the primary treatment for patients with clefts.3,4 Lip repair is normally performed when the child is 3-6 months old aligning with the “rule of tens”: 10 weeks old, 10lbs and a hemoglobin of 10 mg/dL.5,6 The primary goal of surgical repair is to reinstate facial movement and establish normal aesthetics of the deformed lip and nose, however, the final aesthetic outcome is usually not determined until patients are in their twenties due to the physical changes that occur with growth.3,4 As a result, secondary surgeries are often required to correct for these changes with estimates of 30-40% of patients requiring revision surgeries. 7 Despite the high prevalence of revision, there is a lack of consensus regarding the utility and timing of these surgeries. There are also few studies reporting changes in aesthetic outcomes following these secondary surgeries. In order to evaluate the potential benefits of lip/nose revision surgery, it is necessary to understand the natural changes in lip/nose appearance that occur with growth in the absence of revision. Accordingly, the purpose of this investigation is twofold: (1) to determine a baseline of anticipated change in nasolabial appearance without revision; and (2) to evaluate the degree to which revision surgery improves nasolabial appearance.
Methods
Cohorts
A retrospective chart review was conducted following institutional review board approval. Identifying information, such as names, images, and specific locations, were anonymized to ensure participant safety and privacy. Cropping of patient images was approved by the institution's IRB to eliminate features that could enable potential identification of individual patients. Data was collected from medical records for patients with nonsyndromic complete unilateral cleft lip and palate (CUCLP) treated at Lancaster Cleft Palate Clinic (LCPC), a major interdisciplinary cleft-craniofacial clinic in central Pennsylvania.
Patients were categorized into two cohorts: non-revision and revision. Twenty three patients who underwent primary lip and palate repair with no revision surgery comprised the non-revision cohort. Outcomes for these patients were evaluated at 3 time points: T1 at 5y:0 m, T2 at 8y:11 m and T3 at 11y:1 m for a total of 69 ratings between all patients and time points. Patients in this cohort were treated in the 1970's and underwent a Tennison-Randall triangular flap lip repair at 3 month-old all performed by one surgeon. None of these children underwent revision surgeries as standard of care at this period of time indicated performing soft tissue revision surgeries after skeletal maturity was attained.
In comparison, the revision cohort was comprised of 19 patients who underwent secondary surgery during childhood to address abnormalities in nasolabial appearance. All patients in this cohort underwent a Tennison-Randall triangular flap for primary lip repair at 3 months-old by one of 2 experienced surgeons followed by a modification of the Nakajima straight-line repair for revisions. Outcomes were assessed at two time points, before revision at an average age of 8y:5 m and after revision at an average age of 13y:1y for a total of 38 ratings. Since these time points coincided most closely with the second and third time points for the non-revision group, they were called T2 and T3 respectively.
Outcomes of Interest
Nasolabial outcomes were evaluated using frontal and profile 2D photographs and rated by 6 providers using a modification of the Asher-McDade methodology. 8 For the non-revision group, all profile photographs were taken from the right side, which was the non-cleft side for 15 of the 23 patients. Since no cleft-side profiles were available for those 15 patients, the cleft side and non-cleft side groups were kept separate in the analysis. The revision group had both right and left profile views available. To ensure blinding of the groups, the left cleft side in the revision group was flipped to be facing right so that all profile views in this group were cleft-side and facing right. Photographs were scanned, cropped to reveal only the nasolabial region and rescaled with uniform backgrounds similar to the protocol used in the original Americleft Study. 9 These images were randomized, numbered, and printed on 4 X 5 3⁄4 inch cards (Figure 2).
Nasolabial frontal (NLF), Nasolabial profile (NLP), Vermillion Border (VB), and total nasolabial changes were assessed using the Stoutland et al. Q-Sort method. This process is a modification of the Asher-McDade method which uses a 5-point rating scale with 1 indicating the best outcome and 5 being the worst.8,10 Additionally, a full nasolabial reference yardstick providing examples in each category was utilized as a reference per guidelines described by Mercado et al. (Figures 1-4). 11 Photographs were rank-ordered into five piles indicative of the five potential scores described previously. The ratings were performed twice over two separate days and the mean at each age was used as the final score.
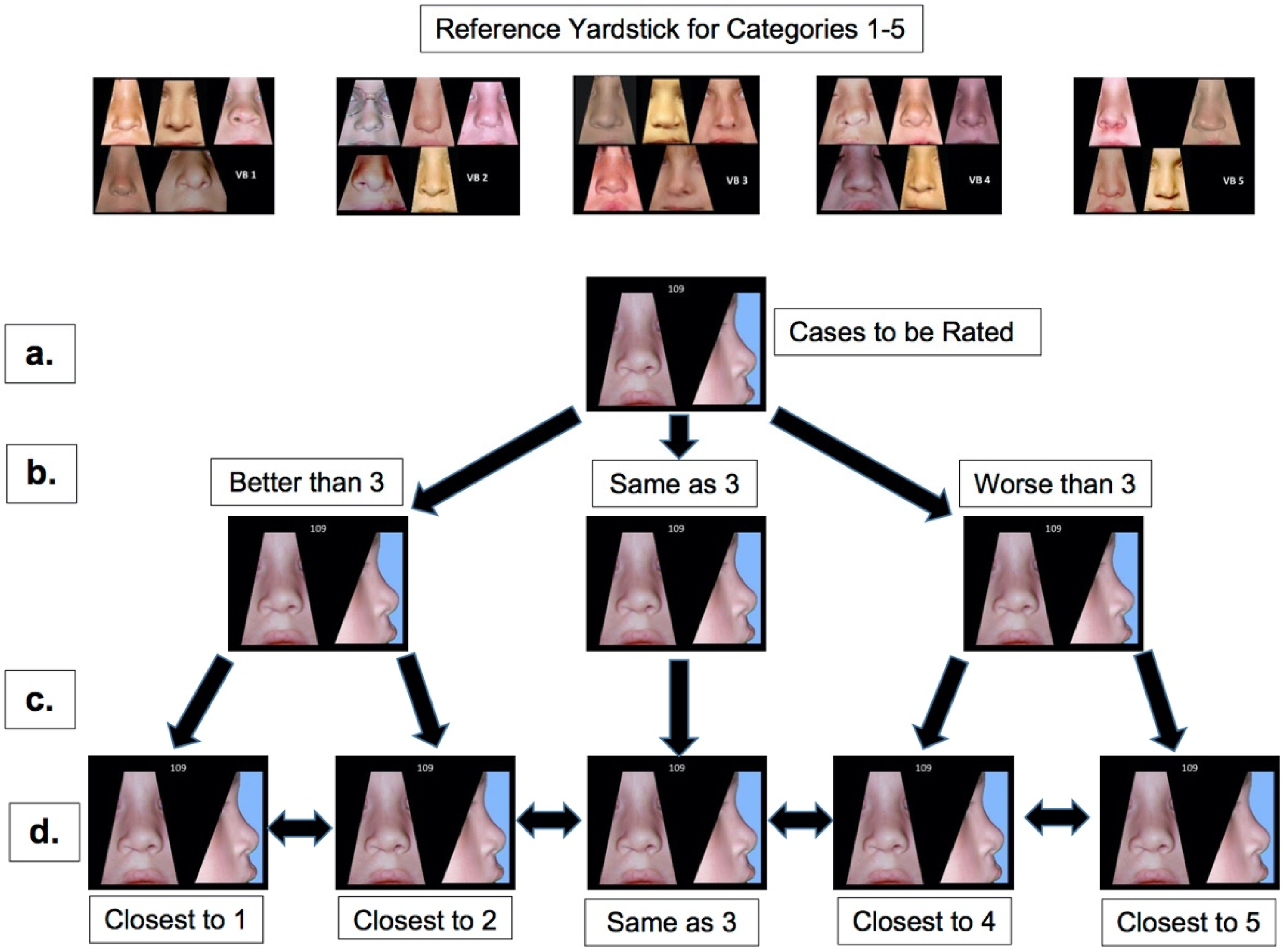
Nasolabial appearance evaluation 10 with Expanded Nasolabial Yardstick 11 . The method utilized was the same method implemented by Stoutland with progressive winnowing for cases to be rated into 5 categories, where for example (a.) is the case to be rated which is compared to the yardstick at the top (and Figures 2-4 below), and then, as is seen in (b.), it is placed into one of three piles: equal to a 3, or better or worse than a 3. (c.) the better-than-3 and worse-than-3 pile are then reviewed and separated into a 1 or 2 (for the better pile) and 4 or 5 (for the worse pile) (d.) The raters could now re-examine their ranking and make any necessary changes.
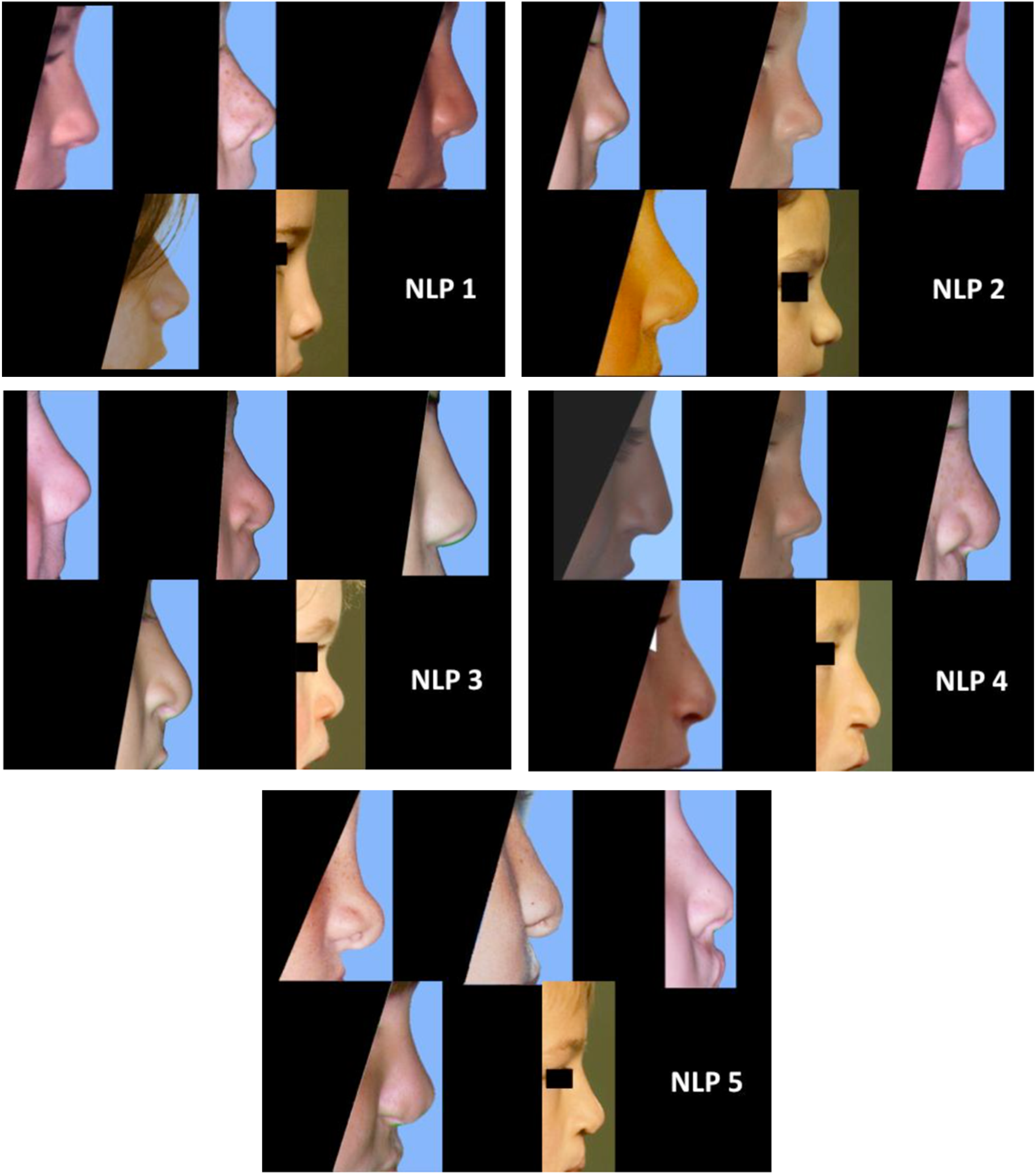
Nasolabial profile yardstick.
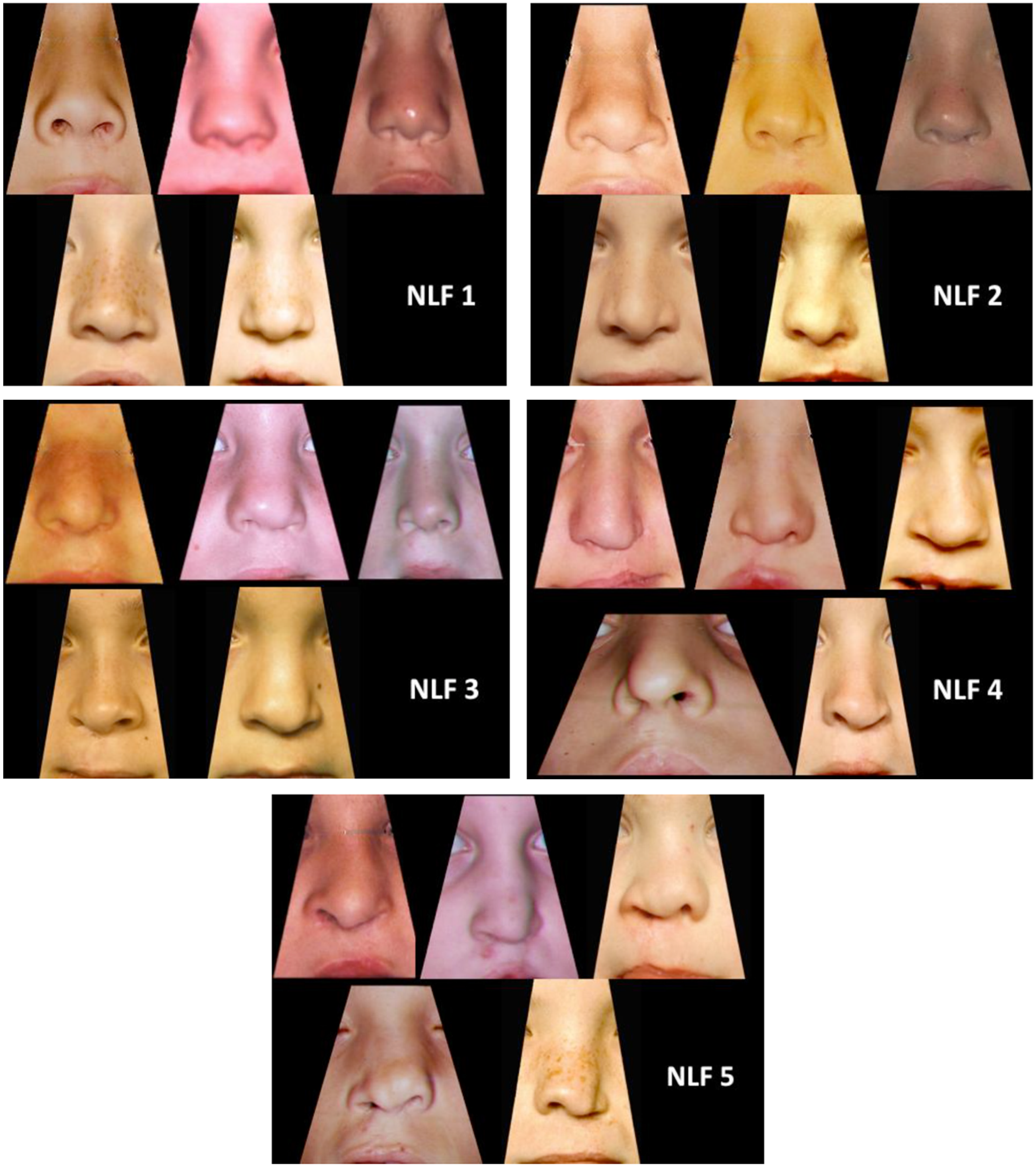
Nasolabial frontal yardstick.
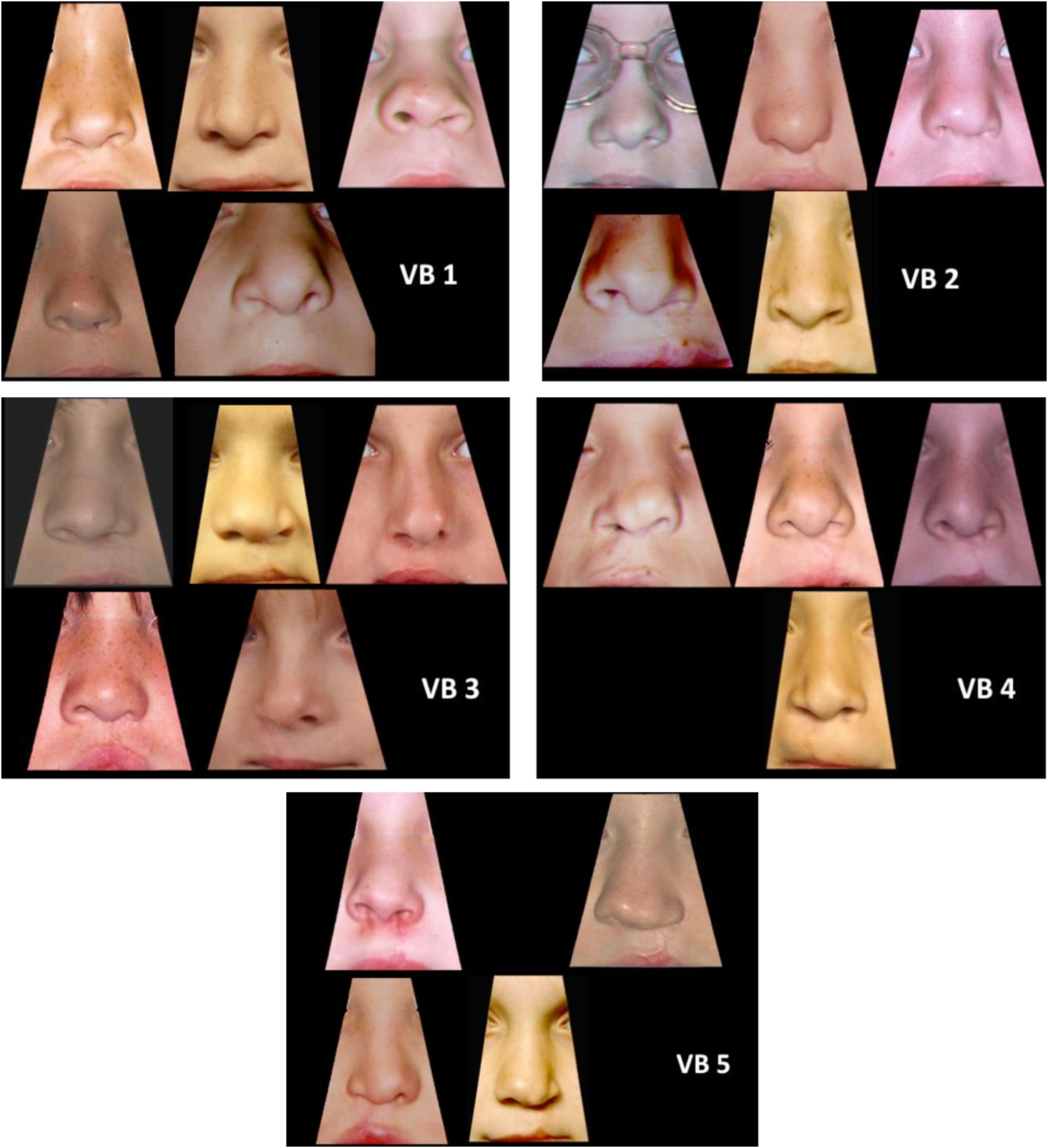
Vermillion border yardstick.
In the non-revision cohort, the three time points were rated as part of the Americleft Outcomes Comparisons Project (www.americleft.org). For T1, the photographs of the 23 patients from 4 centers were rated by 6 experienced cleft orthodontists. T2 and T3 photos were rated by 5 orthodontists and 1 oral maxillofacial surgeon for 119 and 144 patients from 4 centers, respectively. For the revision group assessments, the before and after photographs for the 19 patients were rated along with the patients in the non-revision group for the T2 and T3 rating sessions. All ratings were completed by members of the Americleft Team following training and calibration between raters.
Statistical Analysis
Patient characteristics were summarized using mean and standard deviation or frequency and percentage for continuous and categorical measures, respectively. A Mixed Effects Model and Multiple Linear Regression were utilized to test for significance in changes over time. Values of p < 0.05 were considered statistically significant. Gender, orthodontic treatment, and cleft-side were evaluated as potential co-factors with only cleft laterality having significance for the profile view. Therefore, in the final analysis cleft side profile in the non-revision group was included in the profile comparison and for combined total nasolabial score. Reliability was assessed using the weighted Kappa statistics for inter and intra-rater reliability. 12
Results
A total of 42 patients were included in this study, 23 in the non-revision cohort and 19 in the revision cohort. Table 1 reports a summary of demographics for the two groups. For the non-revision cohort, the mean intra-rater agreement for all three ratings (NLF, NLP, and VB) was good with a mean weighted Kappa for VB = 0.779, NLF = 0.775, NLP = 0.758. The mean inter-rater agreement for this cohort was also good for VB (0.628) and NLF (0.619) and moderate for NLP (0.567). For the revision sample, intra-rater agreement was good to very good for all views (mean weighted Kappa for VB = 0.794, NLF = 0.800, NLP = 0.794). Inter-rater agreement was also good in this cohort for VB (0.623) and NLF (0.661) and moderate for NLP (0.529). There were no significant effects related to gender and orthodontic treatment.
Demographics for the non-Revision and Revision Cohorts.
For the non-revision group, NLP worsened (scores increased) over time from 3.26 to 3.75 on the cleft side but improved on the noncleft side from 3.26 to 2.97. NLF also worsened slightly over time from 3.37 to 3.44 as did total NL appearance with the cleft side changing from 3.30 to 3.37 and the non-cleft side changing from 3.19 to 3.26. VB remained constant from 3.23 to 3.25.
Mean scores in the revision group improved (scores decreased) from before revision (T2) to after revision surgery (T3) for all angles: NLP 3.48 to 2.97; NLF 3.50 to 2.95; VB 3.09 to 3.05, and Total NL score from 3.29 to 3.01. Although all aesthetics improved, these changes were not significant for VB (p = 0.953) as measured by the interaction effect when compared to the changes in the non-revision control group over a similar age range (T2-T3). On the other hand, the improvements in NLP, NLF and total nasolabial scores were significant as measured by the interaction effect when compared to the longitudinal control group without revisions (p = 0.001, p = 0.001 and p = 0.004 respectively). The changes in appearance ratings for the non-revision and revision groups are illustrated in Figure 5.
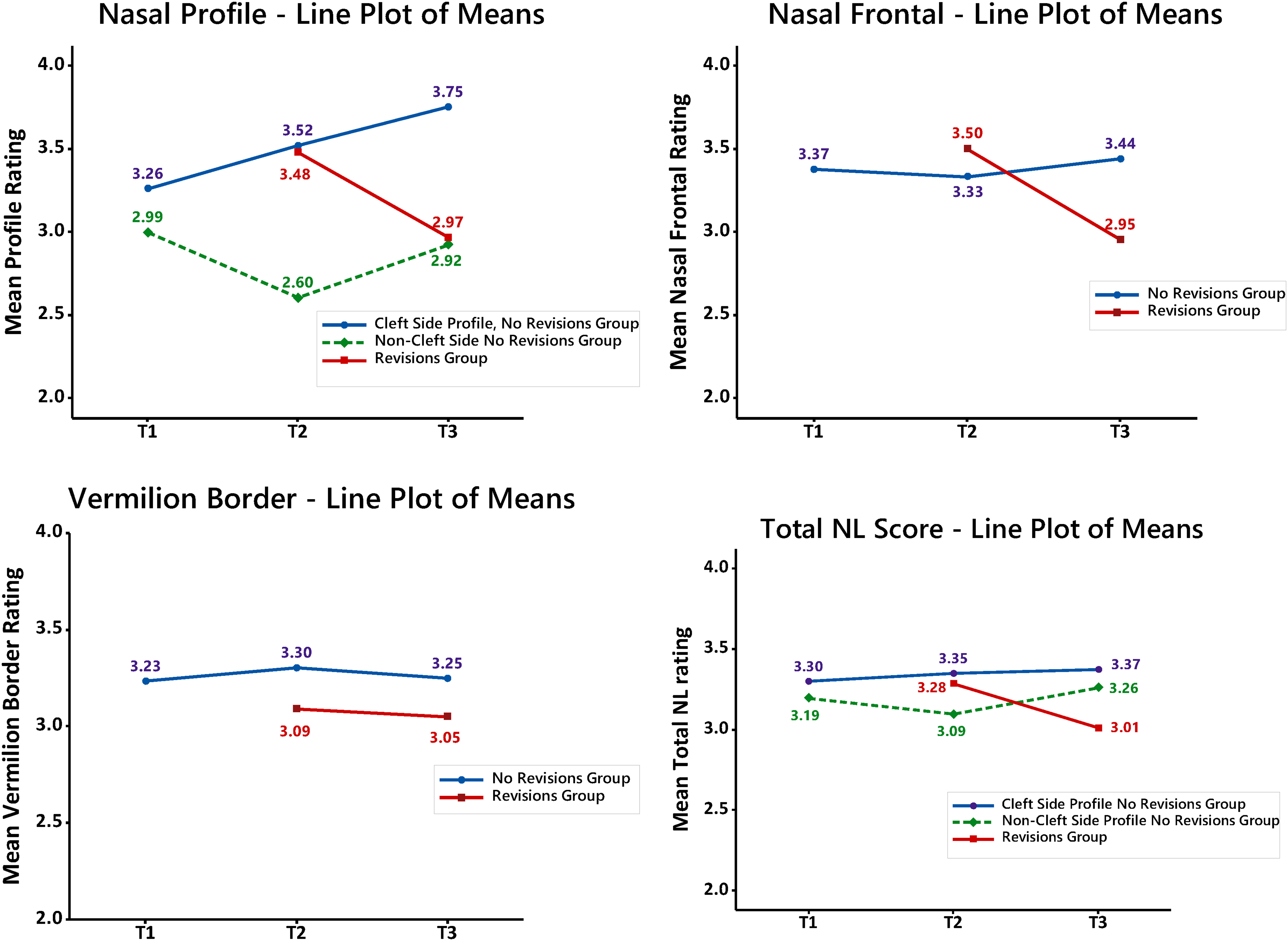
Line plot of score means.
Discussion
Results from this study suggest that nasolabial appearance remains predominantly stable between the ages of 5 and 11 years old after primary repair except for nasal profile appearance which tends to worsen with age on the cleft-side. Children who undergo revision surgery around this age have improved outcomes in frontal, profile, and total nasolabial appearance compared to before surgery. Gender and history of orthodontic treatment have no effect on these outcomes.
In patients affected by cleft lip and palate, appearance of the nasolabial region can be aesthetically and functionally abnormal, even after successful primary surgery. 11 Secondary surgical revision is the primary method utilized to attempt correction of these residual abnormalities. Unfortunately, there is a lack of consensus surrounding the need for and benefits of revision surgery, which may be attributed partially to the subjective nature of nasolabial aesthetic ratings. As a result, past studies attempting to identify potential improvements with secondary revisions have been inconclusive with poor reliability. Moreover, there is a lack of data pertaining to whether the deformity will naturally improve, worsen, or stay the same without additional intervention. Utilizing the Stoutland Q-sort Modification of the Asher-McDade method, comparing to the nasolabial reference yardstick, and including a longitudinal assessment of nasolabial appearance addresses these shortcomings.
This study demonstrates improvements in nasolabial appearance with secondary revision surgery for children with CUCLP for nasolabial frontal and profile aesthetics, however, this secondary surgery comes at the cost of additional burden and risk. As a result, there have been developments in presurgical orthopedic methods to align lip, alveolus and nose prior to primary repair of lip and palate.13-15 These approaches minimize the severity of the initial cleft, using either passive or active appliances, with the goal of precluding the need for secondary revision surgery. 16 One of the most common methods is Nasoalveolar Molding (NAM) during which an external force is applied to shape and mold the nasal cartilage. 15 It is presumed that aligning the alveolus before attempting the primary surgical repair can lead to more favorable outcomes due to reduced tension of the two cleft segments. Unfortunately, in a comparison of nasolabial appearance between children who underwent primary repair relative to children who received pre-surgical orthopedic management, undergoing the orthopedic methods had little to no effect on improved outcome. 17 There is also little evidence available regarding the effect or need for secondary revision surgeries following orthopedic methods to justify their use.
One major shortcoming of previous attempts to evaluate the nasolabial aesthetic benefits of infant presurgical orthopedics or secondary revision surgery is the lack of baseline data surrounding the changes in nasolabial appearance that occur over time without intervention. The non-revision cohort in this study served as a control sample and allowed for documentation of the trends in age-related changes that occur naturally in nasolabial appearance. Outcomes for this cohort showed that vermilion border and nasal frontal appearances do not change significantly between ages 5yo to 11yo, suggesting that the decision regarding need for secondary revision surgeries for these areas can be determined as early as 5yo. On the other hand, caution may be warranted in deciding upon the best age to revise nasal profile as this appearance did worsen with age.
While this study provides invaluable information regarding changes in nasolabial appearance following primary repair of CUCLP and secondary revision surgery, some limitations must be addressed. First, there is debate surrounding potential bias implicit to the Asher-McDade method for evaluating nasolabial aesthetics which may explain why there was significant improvement in nasal frontal and profile scores but no measurable improvement in vermillion border appearance. 18 If the improvements in vermilion border were subtler than the nasal revisions, it is possible that the subjectivity of the Asher-McDade method is not sensitive enough to detect such differences. However, to date, this method is still the primary source utilized to determine need for revision surgery.10,18,19 Moreover, the modifications implemented in this study were employed to reduce subjectivity and improve reliability. Second, the images evaluated were 2D not 3D. Although evaluation of 3-dimensional images has been suggested as a more objective method with improved intra-rater reliability, a recent study comparing rating of 2D versus 3D images showed very similar scores from both methods. 13 Despite these limitations, the results suggest that revision procedures result in positive changes for aspects of nasolabial appearance. This information opens the door to next steps of directly comparing different approaches for optimizing nasolabial appearance outcomes for patients with clefts. Along with this comparison of outcomes, it also becomes essential to understand the potential burden of care the different approaches may place on patients and their families.20-22
Conclusion
After primary repair of complete unilateral cleft lip/palate, appearance of the vermillion border and nasal frontal border does not change significantly between the ages of 5 to 11 years old when secondary revision surgery is not completed. The nasal profile does change during this period. Therefore, decisions regarding need for revision surgery may be made as early as 5 years-old for vermillion border and nasal frontal border correction surgeries but delay may be warranted for nasal profile revision. Meanwhile, patients who undergo secondary revision surgeries have improved ratings of frontal and profile nasal appearance with no measurable change in vermillion border scores after surgery.
Footnotes
Acknowledgements
The authors have no acknowledgements for this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Ethics Committee of Lancaster General Hospital (approval no. 183) in 2008, with the need for written informed consent waived. Identifying information, such as names, images, and specific locations, were anonymized and cropping of patient images was approved by the institution's IRB to ensure participant safety and privacy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Patient Consent
This study was approved by the Ethics Committee of Lancaster General Hospital (approval no. 183) in 2008, with the need for written informed consent waived.