
Abstract
Objective
The birth of a child with a craniofacial anomaly (CFA) can have a profound psychological impact on the family and the parental relationship. The purpose of this study was to qualitatively investigate how a child's CFA condition affected parents’ couple relationship.
Setting
All patients with a CFA are followed-up by the National Unit for Craniofacial Surgery, a specialized and multidisciplinary team. Hence, participants were recruited within a centralized treatment setting.
Design
We used a qualitative approach to explore the relationship experiences of parents of children with CFAs. The interviews were analysed using a hermeneutic-phenomenological approach.
Participants
The study included 13 parents, nine mothers and four fathers of children with a range of different CFAs. At the time of the interview, 10 participants were married, one was cohabiting, and two were divorced.
Results
Most participants perceived their partners as committed and engaged in caring for their affected child and involved in the family's everyday life, and described a strengthened relationship to their partner after the child with a CFA was born. However, some participants struggled in their relationships with their partners, and did not receive the comfort and support they needed during this critical time, leading to feelings of distance and loneliness.
Conclusions
Craniofacial teams should be mindful of the importance of the environment surrounding the child, such as parental relationship and family function. Therefore, a comprehensive approach should be included in team-based care, and couples and families in need of extra support should be referred to relevant specialists.
Introduction
The transition to parenthood may be challenging for a couple and can intensify pre-existing relationship problems even for couples with healthy babies.1–3 Moreover, research from the general population suggests that parents’ relationships, particularly how parents express and deal with conflicts, can affect children's development. 4 The birth of a child with a chronic condition, such as a craniofacial anomaly (CFA), can be expected to have a profound impact on the parents’ relationship, and these parents face challenges that exceed those of most families. 5
A CFA includes a range of conditions that affect the form and function of the head and neck. Commonly affected areas are the mid-face and jaws, cheekbones, eyes and ears, and the respiratory tract; in severe cases, a restricted growth of the skull is possible. 6 Consequently, many patients with CFAs experience problems with breathing, as well as potential problems with speech, chewing and eating, and symptoms related to intracranial pressure, such as vision loss and headaches. 6 Therefore, multidisciplinary and complex surgical treatment is often necessary throughout childhood, lasting into adulthood for the more severe cases.6–8 This situation undoubtedly places a great burden on the parents, as they have to deal with their children undergoing multiple treatments and, in some cases, experiencing complications or life-threatening situations, such as acute respiratory difficulties. 7 Understandably, these stressors may be emotionally demanding for parents.9–12
Although there is a body of research on how having a child with a chronic condition affects couple relationship, the results have been inconsistent. Two reviews of the literature13,14 included studies with parents who had children with chronic conditions and disabilities, including some rare diseases, such as CFAs. Some studies have found a decrease in marital stability when having a child with a chronic condition, while other studies have found a small but significant increase in divorce rates. However, studies have also reported the opposite – namely, that some parents experienced increased closeness to their partners and a strengthened relationship after having a child with a chronic condition.13,14 Qualitative studies from various medical populations, including childhood cancer, autism and rare diseases, have also explored parents’ experiences of having a child with a chronical illness.15–17 Similarly, the findings indicate that some parents struggle in their relationships, while others feel that their relationship has grown stronger.
In the CFA field, research on this topic is scarce. A study of the siblings of children with CFAs found a strong association between parental relationships and the children's behavior problems and social competence. 18 A recent qualitative study has explored how a child's cleft lip and/or palate affected couples’ relational adjustments, 19 finding that most couples experienced both challenges and growth in their relationships. St. John et al. 5 asked 275 parents of children with CFAs how their children's conditions affected their marriages. The major finding was that the type and severity of CFA were not central in relation to divorce rates. Instead, the quality of the relationship before the child's birth was important for long-term outcomes.
It seems that great variability exists in how parents’ relationships are affected by a child's chronic condition. However, this does not contradict the fact that having a child with a chronic condition may be stressful and challenging, putting some couples’ relationships through an ordeal, 14 and that there are reasons to believe that parents of children with CFAs may experience challenges affecting the quality or the stability of their relationships. Existing research is mostly based on quantitative investigations of marital adjustments among parents of children with other chronic conditions.5,13,14 In the CFA field, relevant studies are scarce, and qualitative research that explores parents’ experiences in this regard is lacking, and therefore needed.
We aimed to approach arising issues with as few preconceptions as possible and did therefore not build the study design on any particular theory. Qualitative enquiry aims to understand, capture and represent the experiences and actions of individuals as they encounter, engage and live through specific situations, 20 which may provide valuable insights into a phenomenon, informing, in turn, both research and clinical practice.21,22 Therefore, the aim of our study was to gain a deeper understanding of how parents experience the birth of a child with a CFA in terms of their couple relationship.
Methods
To ensure methodological integrity, we used a hermeneutic- phenomenological approach that supported our research goal of getting close to the participants’ lived experiences.23–25 It is phenomenological through its concern with the subjective experiences of individuals, and hermeneutic through its recognition of how observations are always interpretative.26,27 As we wanted to approach the data with as few preconceptions as possible, we performed an inductive analysis, though acknowledging the inevitable influence of researchers’ own positions when interpreting the data.22,28
Setting and Norwegian Context
The participants recruited in this study were part of a larger study that investigated experiences of treatment among parents of and adults with CFAs. Forty-eight parents of children with CFAs were recruited for the larger study. In Norway, the National Unit for Craniofacial Surgery, a specialised and multidisciplinary treatment team, is in charge of coordinating all follow-up of patients.
Giving birth to a child with a CFA is not associated with socioeconomic status. In Norway, craniofacial treatment is given free of charge, being covered by the national health insurance provided to all residents in Norway. Also, gender- equal parenting has become increasingly common. This development reflects active fathering practises, combined with an increased frequency of mothers within the labor market, as well as policies promoting more equal parental roles. 29
Participants
Parents of children with single suture craniosynostoses (n = 5) were excluded from the present study because the condition implies early surgical intervention only during infancy and most children are not severely functionally or esthetically affected. 30 Thus, 43 parents of children with CFAs who were included in the larger study, were eligible for the present study. In qualitative studies, the adequacy of data depends more on the quality and sufficiency of information, and not so much on the number of participants. 31 Hence, samples of 8–15 participants are often recommended. 32 To ensure a sample of 12–15 participants, we invited 20 participants into this study. To avoid a potential bias in which participants among the 43 eligible parents would be asked for a second interview, 20 participants were randomly selected and invited to participate in the present study. Three declined participation and four could not be reached. Therefore, 13 participants were included: four fathers and nine mothers. At the time of the interview, 10 participants were married, one was cohabiting and two were divorced. All participants were in heterosexual relationships, and mainly represented white middle- class families. The mean age of the participants was 43.5 years (ranging between 34 and 60 years). The participants’ children ranged from 2 to 18 years (mean age of 9 years), with one exception, an adult child with a severe developmental disorder whose parents still had custody. We interviewed one parent of each affected child. The included diagnoses were Pierre Robin sequence, Pfeiffer syndrome, oral-facial-digital syndrome, Crouzon syndrome, oculo-auriculo-vertebral spectrum and Treacher Collins syndrome, in addition to some very rare genetic conditions (not specified to protect anonymity).
Researchers
The research team comprised three researchers. The first author, a clinical psychologist and a PhD candidate in health psychology, has, over the past five years, conducted research and clinical work in the field of CFAs and visible differences. The second author is a professor of clinical psychology at the Department of Psychology, University of Oslo. She is an experienced researcher in studies of process and outcome in psychotherapies and an expert in qualitative methods, with nonspecific prior knowledge in the field of CFA. The third author is a clinical psychologist with a PhD, working at the Centre for Rare Disorders, Oslo University Hospital, and has 20 years of research and clinical experience in appearance psychology and congenital conditions, such as CFAs. Our different perspectives and areas of expertise helped us reflect on our pre-understandings as professionals and individuals and on how such pre- understanding might have affected the data analysis. 31 The first author led the data analysis, while the second and third authors facilitated the analytic process.
Interviews
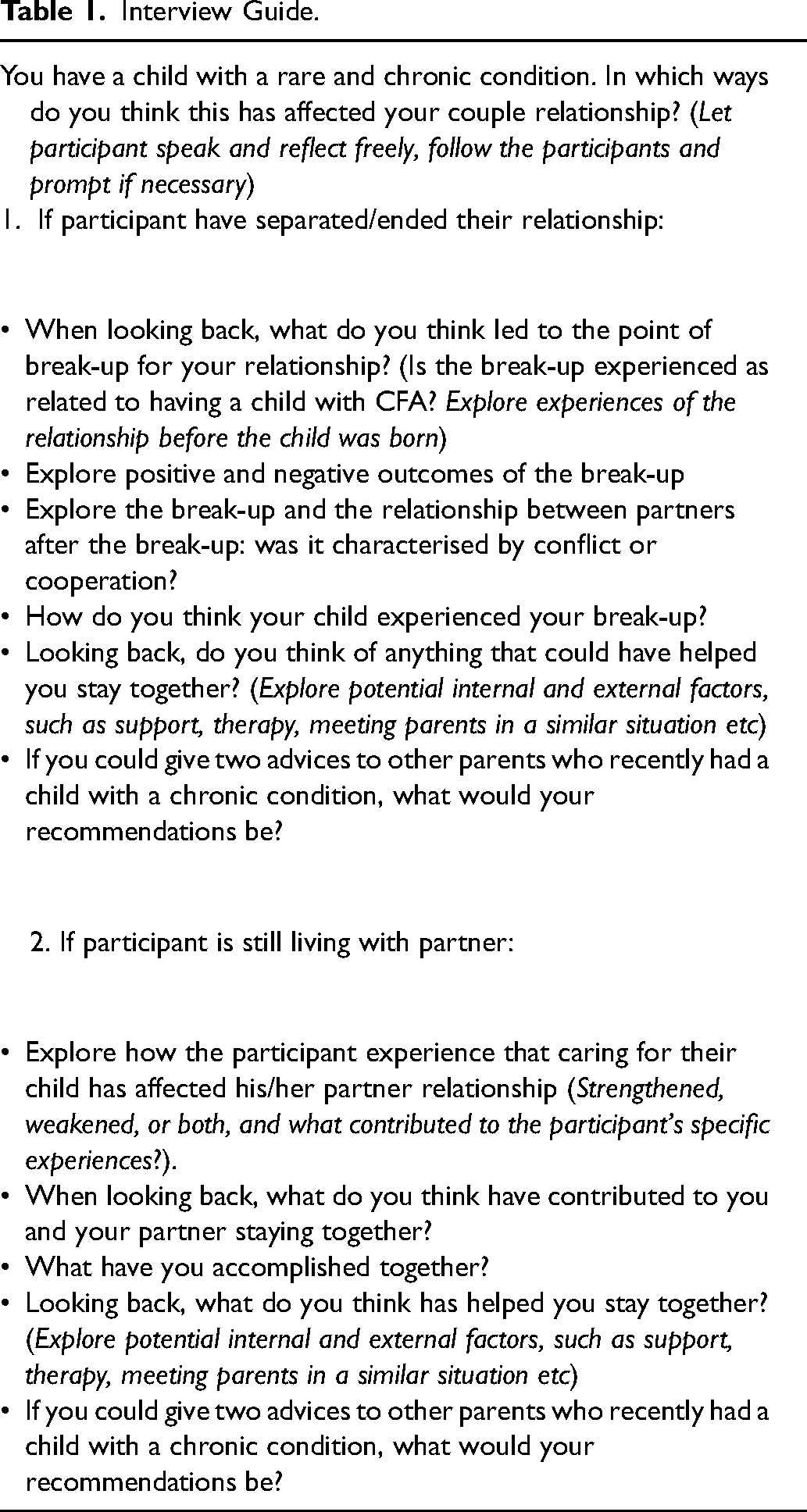
The first and third authors developed a semi-structured interview guide (see Table 1) to explore how having a child with a CFA affected the parents’ relationship. Parents’ relationships were an issue that appeared in the data from the larger study. Since this issue has not previously been explored in depth within this population, we aimed to approach the research question with as few preconceptions as possible. An interview guide including broad questions on relationship experiences was therefore developed, based on general psychological and clinical knowledge, with the aim of exploring positive as well as negative experiences. We contacted each family and asked couples to choose which parent would participate in the study. Due to large geographical distances, all interviews but one were carried out over the telephone. The first author conducted the interviews.
Interview Guide.
Data Analysis
First, the first author transcribed all interviews verbatim and read the full material closely to familiarize with the data. Second, the first author created a document with all the extracted data. Third, the second and third authors carefully read through the extracted data. Fourth, all authors separately identified units of meaning relevant to the research question, and subsequently met to discuss the main tendencies within the dataset. Fifth, the first author carried out the initial coding and categorization of the themes. Sixth, all authors held several meetings in which themes were critically reviewed and revised. Finally, condensed descriptions were developed based on the process of the sixth step. Throughout the analysis, the first author went back to the data several times, to make sure the themes and descriptions were grounded in the data. No issues of disagreement on coding were experienced, and discussions around findings were mostly related to data structure, rather than content. The process was very tentative and open for an extended period.
Inspired by Hill et al. 32 we used the frequency labels ‘general’, ‘typical’ and ‘variant’ to indicate the representativeness of findings. The label ‘general’ covers all but one case and is referred as ‘all’ participants. ‘Typical’ included more than half of the cases and is referred to as ‘most’ participants. ‘Variant’ included at least two cases and is referred to as ‘some’ participants.
Ethical Considerations
The study was approved by the Data Protection Office at Oslo University Hospital. (Reference number: 18/17336). Identifying details, such as names and places, were omitted from the transcriptions, and participant details were changed to provide anonymity.
Results
The participants appeared to be eager to reflect on how having a child with a CFA had impacted their relationships. This process of reflection drew together subjective experiences loaded with emotional tensions from the first years after their children were born.
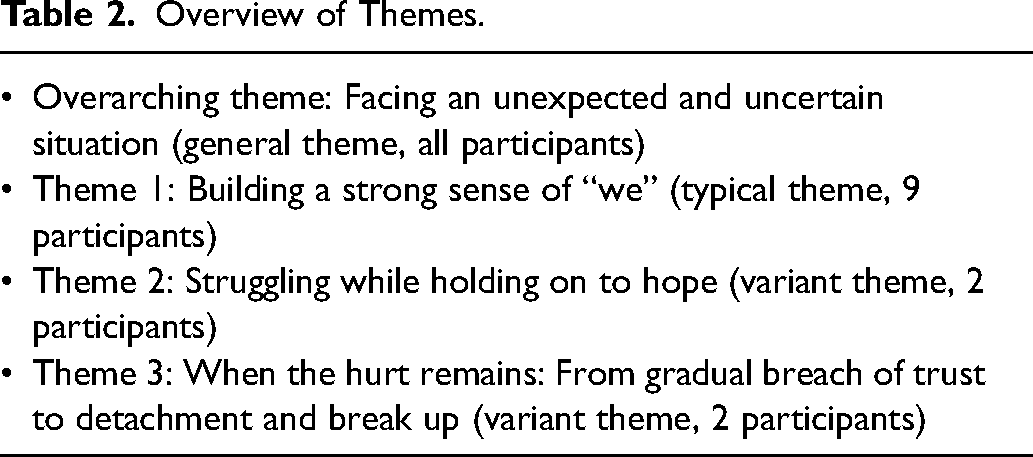
The participants’ experiences and context during the initial time period after their child with a CFA was born is described by the overarching theme of ‘facing an unexpected and uncertain situation’. Most participants described having mastered a difficult life event together with their partner in a way that strengthened their couple relationships. Two participants experienced an ongoing struggle in their relationships, and two participants had ended their marriages after years of striving to make it work. In order to gain insights from participants who identified themselves as being in stable relationships, as well as from participants who experienced struggles and those who ended their relationships, results were categorized into three themes that reflected these groups experiences (for an overview, see Table 2). Types of craniofacial conditions seemed to be evenly distributed across themes.
Overview of Themes.
Facing an Unexpected and Uncertain Situation
This theme included all participants’ experiences during the initial time period after their children were born, which was marked by intense worry and uncertainty about the future. The participants described this period as having the most significant impact on their relationships. Most participants needed to spend time in hospitals separated from the rest of their family, deliver home-based interventions, monitor their child's health and symptoms and maintain vigilance despite experiencing fatigue. For some participants, the experience of living with uncertainty became prolonged, as it took time before they received a diagnosis providing them with answers. As some participants had children with extremely rare conditions, health professionals could offer little knowledge about the prognosis, which intensified the participants’ experiences of uncertainty. Some participants feared for their children's lives and were unsure if their babies were going to survive. Moreover, caring for children had to be balanced with domestic responsibilities and caring for siblings. All participants described the children's first years as life altering. Their worlds became unpredictable, as positive expectations regarding postnatal time were transformed into an uncertain reality. Most participants described going into survival mode and had no capacity other than attempting to go from one day to the next.
Building a Strong Sense of ‘we’
When looking back and reflecting, most participants expressed that having a child with a CFA strengthened their relationships. However, some participants described that being each other's support was a process that took time and was hard work.
Most participants spoke of their relationships in terms of a strong sense of ‘we’ and appeared eager to reflect on what they had done to achieve this feeling of togetherness. As a result, they felt deeply attached to each other, both practically and emotionally.
The most important contributor to building a strong relationship seemed to be the experience of sharing the care for their affected child, siblings, and domestic responsibilities, as well as managing to be emotionally supportive of each other:
‘All the appointments, doctors, trainings, x-rays (…) it wasn't like one of us did it. We were both equally engaged. And that gave an immense strength to our relationship’.
The participants emphasized the importance of handling health- related situations regarding their child, as a team. Most participants described that shared responsibilities was a process that had found its way between them, often without the need to discuss it: ‘Delegating tasks between us went without saying’. Some participants also described how tasks were allocated based on each partner's strengths and preferences:
‘For instance, I couldn’t deal with anesthesia, so when our son needed it, my husband knew that was his job. And that was not something we had a written agreement on, that's just the way it was’.
Hence, participants described how they took on different roles in caring for their child, and highlighted their experience of togetherness as essential for managing the heavy task of caring for their affected child: It became a mutual project for us (..) We rarely argued about division of labor because we both wanted to be involved and take responsibility. With time, we developed different roles in the project. Since I’m a language person, I have taken care of things such as the speech therapy, and my wife is much better than me at technical gadgets, so it was natural that she took care of that stuff, such as the hearing aids (..). Also, there has never been a word said between us that one has taken more or less responsibility, than the other. So I think we both have felt very united in this.
They described that their partners had the same sense of engagement and commitment as themselves, working hard to enable the best possible everyday life for their families, particularly for their affected children.
In addition, the participants described that they also managed to comfort and support each other in their relationships, in dealing with powerful emotions, such as fear, anger and grief. Some participants described the importance of sharing vulnerable feelings with their partners, which made them feel safe and connected. This openness also allowed them to get to know their partners well, and they seemed capable of tolerating difficult feelings in themselves and their spouses. We have such strong feelings for each other. We're both so dependent on each other, at the same time, very autonomous. We know each other very well at an emotional level. To experience a thing like this shapes your feelings, you're high, and you're low. And we have learned to talk about it, that's what makes us so strong. (…) In the beginning, we sat together in the evenings and just talked. And we came to an agreement that we must share all our feelings with each other because we must spend our energy on our daughter and not on misunderstandings and us not being friends.
Some participants seemed to be somewhat compatible to their partners in their ways of approaching challenges in life, such as the need to openly share their feelings with each other: “I’ve always been open, and my husband is also very sensitive and open, so that felt very natural for us”. Other participants felt different from their partners in this respect, yet still managed to be emotionally supportive towards one another, possibly because the participants perceived their differences as a resource: My husband didn’t worry about the things I worried about, which was nice (..) Sometimes it felt frustrating, but I also appreciated those differences. I tend to get preoccupied and worried, and in a way, he didn’t allow me to, and that's been really nice. (..) I think he has such clear thoughts. I am more driven by my emotions.
The participants thus felt that they could lean on their partners for comfort and support, working as a team.
Most participants described their relationships as being on solid ground when their affected child was born. They knew their partners well, which felt reassuring when facing the crisis. Some participants explained that they had previously overcome difficult times with their partners, such as losing loved ones, which helped them believe that they could also manage this ordeal together.
Most of these participants had close family members to support them in caring for their affected child. The experience of support from close family provided the participants with a sense of belonging and protection, an opportunity to take a break from the intensity of everyday life and a chance to spend quality time with their partners. The participants spoke of these breaks as a priority in taking care of their relationships.
Most participants stated that they and their partners had found shared meaning and purpose in the situation they were facing. Some participants described that sharing a sense of humor with their partners eased the tension in the most serious situations. We have both laughed during the most absurd situations (…) and it felt like a wonderful break in the midst of this seriousness, so lovely, like a pause from the drama. (…) We have shared a sense of humour throughout this time. (…) I think that is vitalising.
Shared humour seemed to enable the participants to perceive the situation from a new perspective: ‘Sometimes, it gets too difficult and serious, and [when traveling] we can laugh and giggle with the kids and say things such as, “We are mutants on vacation”. Sharing a sense of humour seemed to strengthen the bond with the partner and the rest of the family.
Some participants described seeing their child as their central task in life and feeling chosen to be the parents of their affected children. Some spoke of a new presence in life, which helped them feel like better parents and find relief from getting lost in worries about their child's future. Others described a shared attitude of determination with their partners and the ability to accept the way life had turned out for them. It might sound like I am telling you this success story, and in many ways, it is. In the sense that my wife's attitude of, ‘Ok, we can handle this, let's do this’, combined with my own philosophical-religious approach to why I became my daughter's father. That combination helped us finish grieving the normality that we had lost from an early point.
They described the importance of letting the idea of ‘normality’ go and the sense of relief when they managed to do so. For some participants, the process of achieving acceptance for their new ‘normal’ was hard and took time and effort. Other participants described that they accepted the situation from an early point.
For some participants, reaching a strong sense of ‘we’ was not a straightforward process. These participants described differing from their partners in what they needed and in how they reacted to having a seriously ill child. Such differences made them struggle to understand and support each other, which created a distance between them. It took time and effort to rebuild an emotionally safe connection: I was very persistent, and preoccupied with the kids, and I wanted to get as much information as I could. And my husband pulled away, he got quiet, he didn't share what he was thinking. We were on different planets.
However, these participants and their partners managed to work through their crises together. They described that a willingness to work on and have faith in their relationships helped them stay together: ‘We had a strong and good relationship before our child was born (…) and luckily, we both had determination and faith that we would manage to get that back’. Others needed some distance and time apart from their partners, which provided them with a new perspective that the burden they were experiencing came from the crisis and not from their partners. When reflecting, the participants spoke gently about their relationships and their partners’ intentions. They highlighted that they and their partners did their best given the circumstances: ‘The thing was, neither of us did something wrong (…) or intentionally said or did things to hurt each other’.
The participants described being proud of managing to get through the most vulnerable time in their lives while gaining new knowledge about each other and their relationships. They learned to set boundaries for themselves and respect their partners’ boundaries. As the participants and their partners were committed, they found the courage to let their guard down and share feelings that felt shameful and difficult while working on unresolved issues from the initial period after their child arrived. We're really proud that we managed to resolve our issues and work together. We have learned each other's weaknesses and strengths, which gave us the courage to ask each other questions and to talk and share, which we didn't dare to before. So, we became very good at knowing what went wrong, what I had to change, what he had to change (…) and to build on the good stuff, to be more aware of our typical ways of reacting.
These participants experienced their relationships growing stronger as a result of overcoming difficulties together.
Struggling While Holding on to Hope
The participants included in this theme seemed to be in an ongoing process whereby they were struggling with their relationships. When the interviews were conducted, their affected children were still young. At the same time, the participants were holding on to the hope that with time, their relationships would recover.
In contrast to the participants who looked back on how their relationships had weathered the stresses during the initial time after their children were born, these participants still seemed to be exhausted and distressed, even though the shock and intensity of the very first time had passed. As a result, none of these participants had the capacity to take care of their relationships or to even think about it. A lack of rest and sleep in addition to the constant experience of uncertainty had marked them: ‘When the evening comes and we have some time to be together, you're so exhausted and drained that you just don't have the energy. You don't have the resources to take care of the relationship’.
These participants described reacting and adjusting differently to the situation compared to their partners: ‘We are very different persons; that became more evident in this situation’. Having a seriously ill child made pre-existing differences within the couples clearer, and they struggled to provide each other with the understanding and comfort needed; thus, the participants described that they still had work to do in their relationships. They seemed to struggle to resolve breaches between them and strove to feel emotionally close. One participant felt disheartened regarding the future of his relationship. To know that their child's condition would not pass felt like a heavy burden: [In the beginning] I thought that if we get through this, we will get through everything together. But, as time passes, that seems to be less evident because after things are a bit normalised, you kind of lower your shoulders, and you're left with just being even more tired.
One participant described how lonely she felt at the very beginning when caring for her affected child. She tried to come to terms with her experience of her partner's lack of engagement and the absence of understanding her endless worry for their child. Such experienced neglect seemed to have produced a wound that still needed healing: We've talked about it, and I've said that it was really tough to feel that he wasn't there for me. But I don't think he understand that he hasn't. I think he feels that he did what he could, in that situation (…) but I've felt that he hasn't been there in ways that he doesn't seem to grasp.
At the same time, the participants expressed hope that over time, their relationships would recover and become stronger: We have so much together, all the children (…) we had a good relationship, and I don't want this to ruin it. There's a few more years ahead of us, where things will be extra tough, and then things will normalise.
In addition to holding on to the hope that their relationship would recover the participants also seemed to have willingness to work on, their relationships with their partners.
When the Hurt Remains: From Gradual Breach of Trust to Detachment and Breakup
Two participants spoke about a process whereby ending their marriage seemed like an inevitable outcome. They expressed that their marital problems had existed for a long time before the birth of their affected children. Some variations in these participants’ accounts will be explored below.
The participants wished for their relationships to be a place in which both parties could express their feelings and experiences and receive emotional support, especially situations of vulnerability. However, they did not experience receiving the comfort and connection that they needed in their relationships, emphasizing this as a major concern. They described their partners as their opposites – that is, as persons who were scared of disclosing and sharing difficult feelings. The participants described various attempts at reaching out to their partners – for example, by initiating conversations, addressing difficult issues and suggesting professional help. However, they experienced failure in their attempts to connect with their partners: [His message was that] we should not change anything and not talk about anything (…) if we just sat there, quietly and did nothing, then everything will just pass and be fine. I think that's how he wanted it to be. If we're silent about a problem long enough, it passes.
It seemed as if the more the participants tried to reach out to connect with their partners, the more they experienced their partners to withdraw by becoming silent or remove physically from the situation. As a result, the participants felt alienated from their partners, which was described as the most painful experience of their marriages: ‘That feeling of standing there by myself and also living with the uncertainty by myself, it's dreadful’.
The decision to leave their partners was not a straightforward process, and the participants struggled for years to make their relationships work. They went through an internal process in which the idea of breaking up gradually developed: ‘[His silence] was the thing that over time made me uncertain about whether he will be there for me when I need it’. The partners’ avoidance of emotional intimacy produced a sense of existential insecurity.
Both participants also described specific events that contributed significantly to the decision to end the relationships. These incidents involved experiences of being let down by their partners, and both participants described these events as turning points in their marriages. It was as if the incidents were final indicators that their partners were not persons on whom they could depend. For one participant, the incident involved witnessing her husband be openly ashamed of their child in front of strangers: It felt as if he spat in my face [cries]. And in that moment, I thought about all those hours in couple's therapy, they felt like a complete waste, we're back at square one. (…) Like he was to pity because he had this child. And that was the turning point. (…) I felt how my marriage broke in that moment. (…) Who am I supposed to support? Him, or should I help and support my child? So, I had a choice, and that choice felt easy.
The participant did not merely experience her husband letting her down; rather, she also experienced that he let their child down, which felt like absolute betrayal. The participants experienced these events, or turning points, as indicating a relationship that was beyond repair, a symbolic manifestation of their lack of trust in their partners.
Discussion
The aim of this study was to explore the relationship experiences of parents who have children with CFAs. The participants provided vivid and powerful descriptions of how their couple relationships were influenced by having children with CFAs. Most participants described themselves as being in happy relationships, with the crisis that they faced strengthening their couple relationship, in spite of relationship difficulties on the way. Others found that the struggles overshadowed their daily lives and experienced distance between themselves and their partners. For two of those participants, their already troubled relationships ended after years of striving to make them work.
Our findings are aligned with those of Zeytinoğlu et al.'s 19 study, which examined how having a child with cleft lip and/or palate impacted couples, finding that most couples reported that their experiences had strengthened their relationships and that they managed to be supportive of each other and to work as a team while facing challenges. Furthermore, St. John et al. 5 have investigated marital stability among parents of children with CFAs, finding that most couples with stable relationships before the births of their affected children reported strengthened relationships. By contrast, couples who reported struggling before the child's birth experienced their relationship being destabilized after having children with CFAs. Although the methodological approaches used in our and St. John et al.'s 5 studies were very different, both studies suggest that the stability of the relationship before the birth of a child with a CFA is important in how a couple copes with the challenges involved in having a child with a CFA.
Some studies exploring parents’ experiences of stress in other medical populations have also touched on how the couple relationship is affected by their child's diagnosis. Some parents have reported elevated levels of conflict, blaming each other in times of stress, which leads to experiences of distance and loneliness. Other parents have found that their relationships have grown stronger as they leaned on and helped each other when caring for their children, working together as a team.15–17,33 These reported experiences are in line with our findings. However, our focus on the participants’ relationships with their partners, along with our qualitative approach to the research question, provides a more detailed account of the participants’ relationship experiences – for example, by revealing the motives behind the decision to break up and highlighting the development of a strong sense of ‘we’.
Attachment theory provides a framework for understanding adult romantic relationships, which seems particularly appropriate for understanding our findings.34,35 Attachment theory states that humans have a basic need for relational care and closeness and that emotional dependency is a fundamental part of human nature. 36 Moreover, attachment theory has increasingly been applied to understand adult romantic relationships, claiming that adults, like children, have an increased need for attachment during times of vulnerability.36–38 Particularly vulnerable periods include times of loss, physical illness, uncertainty, fear and transition. 39 Such stressful situations increases attachment needs and behaviors, such as turning to close others for assistance, comfort and support. In our study, the participants described the initial period after the birth of the affected child as a life-altering transition marked by feelings of intense uncertainty and fear about the child's future. Therefore, this period constitutes a vulnerable time for parents of children with CFAs, thus potentially raising attachment needs in both parents.
Securely attached relationships are characterized by interactions between partners in which both are emotionally engaged and respond to each other's needs in ways that build trust, intimacy and closeness. Such bonding interactions provide the foundation of the relationship as a secure base on which a couple can deal with the stress of caring for their affected child. Facing and dealing with stress, such as caring for a child with a CFA, tends to strengthen a couple's relationship and reinforces the attachment bond between the partners, rather than pulling them apart. 40 The experience that one can rely on one's close ones to be there in times of need has been associated with resilience and the ability to deal with stress. 41 Most of our participants described that having a child with a CFA had strengthened and given depth to their relationships, as also described by Zeytinoğlu et al. 19 Our participants highlighted their partners’ engagement, commitment and responsiveness as essential for the feeling of being supported and not feeling alone when facing the new situation. This finding is in line with studies that have investigated marital satisfaction in the parents of children with other disabilities, finding that sharing childcare responsibilities is a strong and significant predictor of marital satisfaction.42–44 In this study, the ability to safely share uncertainties, fears and vulnerabilities was described by the participants as an important contributor to their strong sense of ‘we’. In contrast to the participants who felt distance from their partners, these participants described engaging in what can be understood as bonding interactions: they managed to be mutually responsive to each other's powerful feelings. Thus, they seemed to use their relationships as a secure base from which they could deal with the stress and uncertainty associated with their children's conditions. 40
A couple's experiences of ‘we-ness’ represent each partner's capacity to invest in the other and in their partnership through actions such as having each other's backs, supporting each other through tough times, teamwork and expressions of commitment, trust and loyalty. 45 Moreover, we-ness refers to a sense of shared identity, which is composed of lived relationship experiences and is built up over several events, 46 in addition to being important in the adjustment to illness and disability.46,47 We-ness further includes elements that were described by our participants, such as shared purpose, meaning and a sense for humor, 45 which seemed to bring the participants and their partners closer together, strengthening their sense of ‘we’. A shared sense of humour also enabled our participants to distance themselves from the emotional impact of the serious situation. 48 Some of our participants described caring for their children with CFAs as their central task in life, whereas others described a new presence in life, which enabled them to envision a greater purpose in their lives and to view their relationships as lifelong projects with shared goals, as described in research from the general population. 49
Most of our participants provided vivid and powerful accounts of how they, together with their partners, had handled having children with CFAs. Although most participants’ children were older, the memories from the initial years were easily recalled. It seemed that their accounts of how they and their partners had managed this process were important to their relationship identities and their strong sense of ‘we’. This is in line with research on couples’ storytelling, which has revealed that vivid, positive and well-rehearsed relationship memories are associated with high levels of marital satisfaction.50,51
In contrast, relationship distress is often a consequence of couples’ failures to communicate their feelings and cope with experiences of uncertainty. Moreover, a partner's unresponsiveness or inaccessibility often leads to insecure attachments.37,39 As mentioned earlier, times of vulnerability increase attachment needs and behaviours, such as seeking comfort and support, and can highlight attachment insecurities in a relationship. Some of our participants and their partners seemed unable to meet each other's attachment needs, thus putting their attachment bonds at risk. A typical pattern in insecure relationships is that during conflicts, one partner tends to reach out in various ways to connect, often by criticism, anger and complaints, while the other partner tends to increasingly withdraw, adopting a defensive stance. Overwhelming negative emotions combined with inflexible interactional patterns impede the process of working through conflicts and bringing closure to negative events. 52 Some of our participants’ accounts of trying to connect to their partners for years, which resulted in increased emotional avoidance, illustrate a typically rigid pattern that, for distressed couples, may become reinforced over time. 52
The participants who decided to end their relationships described specific incidents that significantly contributed to their decisions. Attachment theory conceptualizes such incidents as ‘attachment injuries’, which is a particular type of betrayal experienced in romantic relationships that is characterised by a violation of trust and rejection by one partner. Attachment injuries goes beyond a general trust issue in a relationship, as it concerns a specific event whereby one partner fails to provide the support and care expected from an attachment figure in times of need. For the participants, such incidents seemed to be particularly devastating, as their partners’ inability to support and cooperate affected not only themselves but also their children with CFAs. The sense of basic trust, which is the cornerstone of an attachment relationship, was suddenly destroyed. Such violations may rupture the relationship bond in significant ways. 52 Under normal circumstances, a violation of expectations for one's partner to be responsive and supportive would not necessarily harm the attachment bond. 52 However, our participants described what can be understood as a pre-existing frayed attachment bond, 52 which had developed over years as a result of their perceptions of their partners’ inadequacy in providing emotional closeness and disclosure.
Clinical Implications
The environment surrounding a child is essential for the child's opportunities for optimal development. Treating a child with a CFA therefore requires a comprehensive perspective that also should include family function and parental relationships. The parents of a child with a CFA may face a crisis, particularly in the initial period after their baby is born.5,19 To support their child in the subsequent challenges of having been born with a CFA, parents need each other's support and comfort, with both individuals needing to share the responsibilities associated with their affected child's care. Therefore, members of craniofacial teams should be aware of the possible impact of the child´s condition on the couple, and the advantage for the child of a strong couple relationship in caring for their child. In countries providing longitudinal and multidisciplinary care, families often see the same physicians over long periods of time, which can provide a basis for a trustful doctor/patient relationship. 53 Members of craniofacial teams should see this as an opportunity to highlight this issue by providing the parents information about how caring for a child with a CFA can put a strain on the couple relationship and some couples therefore is in need for extra support or counseling. Being aware of this issue creates an opportunity to ask parents directly about their relationship and how they are coping, referring them to a relevant couple and/or family specialist, if needed. Preferably, clinical psychologists or other mental health professionals should be included in all craniofacial teams, to assess the couple and family as a whole and to offer or secure support for families and couples in need of assistance.
Limitations
This study has some important limitations that needs to be addressed. This study explored the accounts from a single parent's perspective, as the resources to travel long- distances to interview couples exceeded those available for this study. We are well aware of couples not necessarily having corresponding stories regarding their relationship. However, the present study's aim was not primarily to conduct an in-depth analysis of couple dynamics, but to explore how parents experienced that their relationship was affected by caring for a child with a CFA. Nevertheless, interviewing both parents would have strengthened the study, and should be considered in future research.
The present study involved a large variation in the children's ages, which may have led to differences in parents’ perspectives. Some parents had quite young children at the time of the interviews and were thus in the middle of the adjustment process. However, most parents had older children, which enabled them to consider retrospectively how they managed to cope. Both of these outlooks are useful because they enable us to draw knowledge from two different perspectives: the experiences of parents who are still undergoing the challenges imposed by caring for their affected child and those of parents looking back and reflecting on how they handled this crisis together.
In Norway, craniofacial treatment is available free of charge for affected individuals. This is far from the case in all countries. Financial burdens and limited access to treatment may be a significant strain for families with chronically ill children, which most likely puts additional strain on parents’ relationships. Moreover, this sample consists of mostly white- middle class parents.
Conclusion
In our study, most participants experienced their relationships strengthened after their child with CFA was born, in spite of challenges, and they perceived their partners as engaged in the care of their children and family life. Some participants struggled in their relationships, finding it difficult to receive the needed practical and emotional support from their partners. Therefore, a comprehensive approach should be included in team based care, and couples and families in need for assistance should be referred to relevant specialists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the EkstraStiftelsen Helse og Rehabilitering (Stiftelsen Dam), (grant number 2018/FO203158)