
Abstract
Objective
This study examined the posttraumatic growth (PTG) about parents of children with cleft lip and/or palate (CL/P) and the correlates of PTG.
Design
A cross-sectional study.
Participants and Setting
Parents (N = 388) of children with isolated CL/P (ages 3 months-18 years) who had at least one cleft surgery within an oral and maxillofacial surgery department of a university-affiliated tertiary hospital in a provincial capital in southwest China.
Main Measures
Demographic information questionnaire, The Posttraumatic Growth Inventory, Simplified Coping Style Questionnaire, and Social Support Rating Scale were used for data collection.
Results
Parents’ mean PTG score was in the moderate range (M = 65.7, SD = 13.73). PTG differed regarding the participants’ sex, ethnicity, and educational background. Pearson's correlation analysis revealed that positive coping (r = 0.43, P < .01), negative coping (r = 0.13, P < .01), and social support (r = 0.26, P < .01) were positively correlated with PTG. Multiple regression model showed that 20.6% (P < .001) of the variance in PTG was explained by higher positive coping (β = 0.35, P < .001), greater social support (β = 0.13, P = .01), and for cleft lip compared to cleft palate (β = −0.14, P ≤ .01), with no variance difference for cleft lip and palate.
Conclusions
Parents of children with CL/P had moderate PTG. Potentially modifiable correlates of PTG suggest interventions to enhance parental positive coping and social support may increase PTG. Further studies are needed to confirm the PTG level and its affecting factors of parents of children with CL/P.
Introduction
Cleft lip and/or palate (CL/P) are the most common craniofacial diagnoses, with a worldwide prevalence of 1 in 700 live births. 1 In China, the overall prevalence of orofacial clefts was 1.4 per 1000 live births. 2 CL/P can be divided into 3 main subgroups: cleft lip only, cleft lip and palate, and cleft palate only. People with CL/P need multidisciplinary interventions, including nutritional support, surgical repair, speech and language therapy, orthodontic care, hearing intervention, and psychological counseling. The initial diagnosis, repeated hospitalizations for surgeries, and intermittent clinic visits cause psychological distress and economic burden for children as well as their families.3–5
The concept of child health includes both the child and the family because of children's dependence on their caregivers and family. 6 Studies have shown that the sociodemographic characteristics and the health status of mothers are associated with parent–child interactions, which as a result may influence the children's health outcomes. 7 Hence, the psychological adjustment of parents of children with CL/P is an important research subject. The majority of studies have focused on negative adjustment in parents of children with CL/P and revealed that some parents experienced psychological shock, feelings of guilt, stress, depression, and sorrow.3,8,9 Moreover, some researchers have found that having a child with CL/P impacts the parental quality of life.4,10,11
Although some parents of children with CL/P have experienced negative emotions and psychological distress, studies have shown that certain positive effects can emerge through the struggle with traumatic events and treatment-related experiences.5,12 The positive psychological changes gained through experiencing challenging life circumstances are referred to as posttraumatic growth (PTG). 13 Researchers have investigated the PTG of bereaved parents, parents of children who have undergone hematopoietic stem cell transplantation, and parents of children with autism, intellectual disability, schizophrenia, cystic fibrosis, and pediatric cancer.14–19 In general, parents of children with illnesses had a moderate PTG level.17,18,20 The correlates of parental PTG in these studies varied, including parental and children demographics, resilience, family function, coping, and social support.17–19,21 It was reported that PTG was associated with coping style and social support among caregivers.22,23 Social support is an important factor that directly influences the PTG of mothers of children with cancer and chronic illnesses and bereaved parents.19,20,24
To date, studies focusing on the positive psychological changes of parents of children with CL/P are scarce. O'Hanlon et al investigated whether a parental diagnosis of CL/P affects the adaptation (including PTG) to having a child with CL/P and revealed a relatively low PTG level. 25 In Feragen et al's 5 qualitative study, parents of children with a congenital craniofacial anomaly experienced stressful and potentially traumatic symptoms, but they also experienced increased confidence, and their perspectives of life changed. Omiya and Yamazaki 26 conducted a survey on 293 mothers of children with CL/P and found that many of them experienced positive change through child-rearing. In the study of Baker et al., parents of children with CL/P reported better self-understanding, greater personal strength, and optimism. 27 This study set out to explore the status of PTG in parents of children with CL/P and its potentially related factors.
Methods
Design and Participants
This cross-sectional survey aimed to explore the posttraumatic growth of parents of children with CL/P who had at least one surgery and its potential relationship with social support and coping style.
Parents of children with CL/P were recruited from an oral and maxillofacial surgery department of a tertiary hospital located in Southwest China. The sample consisted of parents of CL/P children recruited from 2 approaches. One part of the participants were parents of CL/P children hospitalized during the period of the survey, which was June to September 2021. The rest of the participants were parents of CL/P children who underwent surgeries between January 2020 and May 2021. The latter group was recruited from preestablished WeChat (the most popular social media in China) groups that were used for routine follow-ups. The WeChat groups contained cleft lip and palate surgeons, nurses, parents of CL/P children, and adolescent and adult CL/P patients. Parents of children with nonsyndromic CL/P were included. The exclusion criteria of parents of hospitalized children with CL/P were parents of children with other comorbid medical conditions, parents who were experiencing other traumatic events, and parents with a mental illness history. There were no exclusion criteria for parents of children with CL/P recruited from WeChat groups.
The sample size was calculated as 5 to 10 times the number of independent variables. 28 In this study, there were 19 predictors, including sociodemographic characteristics and 2 main predictors, that is, social support and coping style. Thus, the minimum sample size was 190. At the end of the survey, 388 questionnaires were collected.
Measures
Sociodemographic Questionnaire
A sociodemographic questionnaire was designed based on literature review and clinical experience.17,26,29 The questionnaire included information on parental sex, age, education level, religion, ethnicity, marital status, employment status, monthly family income and the children's sex, age, cleft type, operations received, whether the only child of the family, family residence, and payment method of medical expenses.
Posttraumatic Growth Inventory
The Posttraumatic Growth Inventory (PTGI) was first developed by Tedeschi and Calhoun 12 to measure the positive outcomes resulting from traumatic or negative events. Wang 30 translated and revised the PTGI into the Chinese-Posttraumatic Growth Inventory (C-PTGI) to suit the Chinese population. The C-PTGI has been proven to be a valid measurement and has been used among bereaved parents and parents of children with autism spectrum and congenital conditions.14,17,31 The 20-item scale consists of 5 dimensions, including relating to others, new possibilities, personal strength, spiritual change, and appreciation of life. The scale was scored on a 6-point Likert scale ranging from 0 (no change) to 5 (very large change), and the total score of the scale ranges from 0 to 100. According to the classification criteria of Forinder and Noberg, 32 total PTG scores less than 52 were considered low, scores between 52 and 74 were considered moderate, and scores greater than 74 were high. The internal consistency coefficient of the scale was 0.874, and the Cronbach's α of the 5 dimensions ranged from 0.611 to 0.796.
Social Support
The Social Support Rating Scale (SSRS) was developed by Xiao 33 for a Chinese population to measure perceived social support. The scale included 3 subscales: objective support (3 items), subjective support (4 items), and support utilization (3 items). Objective support refers to tangible and direct support, such as financial and concrete resources. Subjective support refers to perceived social support such as emotional support. Support utilization reflects the extent of social support that the respondents used. Item 1 to item 4 and item 8 to item 10 are multiple-choice questions, and the item score ranged from 1 to 4. Item 5 has 5 subsections and the score ranged from 5 to 20. The score of item 6 and item 7 ranged from 0 to 9 each. The total score of the scale ranges from 12 to 66 points, with higher scores indicating stronger social support. The internal consistency coefficient of the scale was 0.896, and the Cronbach's α of the dimension ranged between 0.83 and 0.86. 33
Coping
The Simplified Coping Style Questionnaire (SCSQ) was used to determine the coping style tendency of the participants. It was developed by Xie 34 based on a previous questionnaire (Ways of Coping) developed by Folkman. 35 The SCSQ includes 2 subscales and 20 items: positive coping (items 1-12; eg, seeking support, talking about problems for help) and negative coping (items 13-20; eg, avoidance, trying to forget, and substance use). The questionnaire was rated using a 4-point Likert-style scale (0 = never, 1 = seldom, 2 = sometimes, and 3 = often). The total scores of the positive coping subscale range from 0 to 36, and the total scores of the negative coping subscale range from 0 to 24. People may utilize a mixture of positive and negative coping, such as seeking support and trying to forget at the same time. A higher total score of the positive subscale indicates that the participants are inclined to a positive coping style, while a higher negative coping score indicates an inclination of a negative coping style. The Cronbach's α of the scale was .90, and the Cronbach's α of positive and negative coping were .89 and .78, respectively. 34
Data Collection
The study was approved by the Biomedical Ethics Review Committee of the hospital (Approval number: WCHSIRB-CT-2020-438). Data were collected through the on-site and online distribution of questionnaires. On-site distribution took place at the Oral and Maxillofacial Surgery Department of a tertiary dental hospital. Researchers explained the purposes of the survey to parents of hospitalized CL/P children. If the subject was eligible, informed consent was obtained, and the participants were given a QR code of the questionnaires that was automatically generated from the Wenjuanxing website (https://www.wjx.cn, a widely used Chinese online survey tool). Simultaneously, the QR code of the questionnaire was distributed through preestablished WeChat groups. The submission of the electronic questionnaire requires the completion of all questions; hence, all collected questionnaires were complete.
Data Analysis
All statistics were performed using SPSS 22.0 (IBM Corp). Means, standard deviations (SDs), medians, percentiles, and percentages were used in descriptive statistics. Independent samples t test and post hoc one-way analysis of variance (ANOVA) with Bonferroni correction were employed to determine the differences in participant characteristics. Pearson's correlation analysis was used to identify whether there were correlations among social support, coping style, and PTG. Multiple stepwise regression analysis was applied to assess the predictors of PTG. Statistically significant variables from the univariate analysis and correlation analysis were included in the model. 36 Additionally, cleft type was included in the regression analysis with cleft palate selected as the reference group, since previous studies revealed that cleft type predicts health risks and mortality of adults born with an oral cleft 37 and the family quality of life, parental quality of life, and psychological status differed with respect to the cleft types of their children.3,4,10 The bilateral test level was α = 0.05, and P < .05 was considered to be statistically significant.
Results
Sample Characteristics
Detailed information of sample characteristics is listed in Table 1. The sample was comprised of 107 fathers and 281 mothers. The ages of the participants ranged from 19 to 58 (median = 33, P25 = 29, P75 = 39). The educational background of most participants was high school or less. Approximately half of the participants (44.59%, 173/388) reported that their employment status had changed due to the medical conditions of their children. Approximately 60% (232/388) of the participants responded that their family income was not enough to cover the medical expenses of their children's surgeries. Medical expenses of participant's children were paid through national insurance, a stipend from an international cleft charity organization, and out-of-pocket money. The reimbursement rate for national insurance is around 60% to 80% according to provincial policy. The stipend of the international cleft charity was about 600 to 700 dollars. Most of the respondents (64.17%, 249/388) thought the medical condition of their children was “serious.” The ages of the participants’ children ranged from 3 months to 18 years old (median = 3, P25 = 1, P75 = 11). Approximately half (48.45%, 188/388) of the children of the participants were attending school.
Demographics and Clinical Characteristics of Participants and Participants’ Children (n = 388).
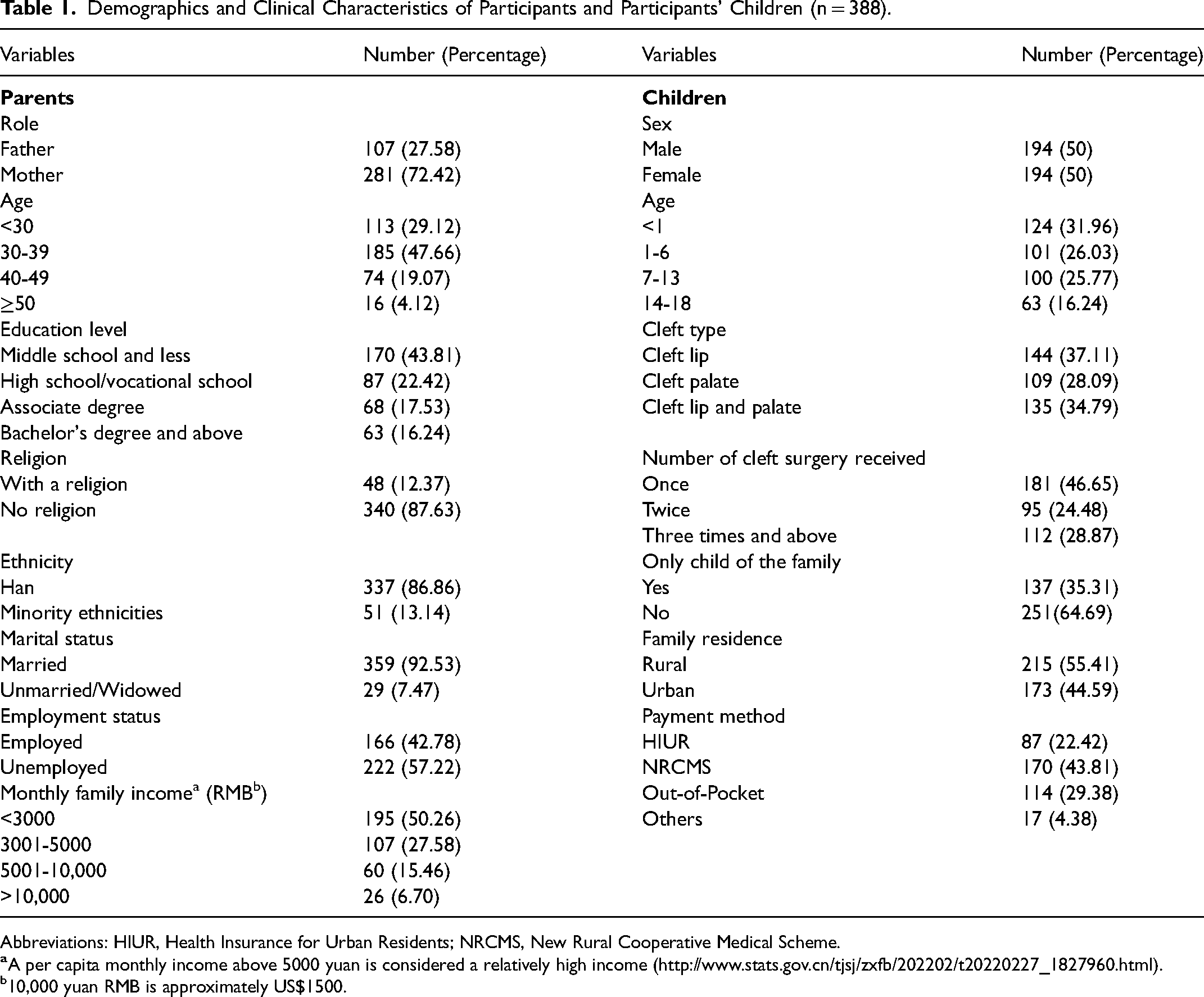
Abbreviations: HIUR, Health Insurance for Urban Residents; NRCMS, New Rural Cooperative Medical Scheme.
10,000 yuan RMB is approximately US$1500.
Univariate analyses showed significant differences between PTG by participants’ gender, ethnicity, and educational background, but there were no significant differences between PTG by parent age, employment status, family income, number of children, urban/rural setting and the age, sex, and cleft type of the children. Fathers had significantly higher PTG total mean scores (T = 2.26, P = .025, 95% CI [0.45, 6.56]), Relating to Others dimension mean scores (T = 2.93, P = .004, 95% CI [0.57, 2.91]), and Spiritual Change mean scores (T = 2.06, P = .037, 95% CI [0.02, 0.50]) than mothers. Participants who identified as minority ethnicities had higher Relating to Others dimension mean scores than Han ethnicity participants (T = −2.07, P = .045, 95% CI [−3.18, −0.81]). Spiritual Change mean scores differed among participants with different educational levels (F = 5.10, P = .002), and detailed information of post hoc pair comparison test (Bonferroni test) of the difference among 4 educational level subgroups is displayed in Table 2. More detailed information of univariate analyses is shown in Table 2.
PTG Among Different Sample Groups (N = 388).
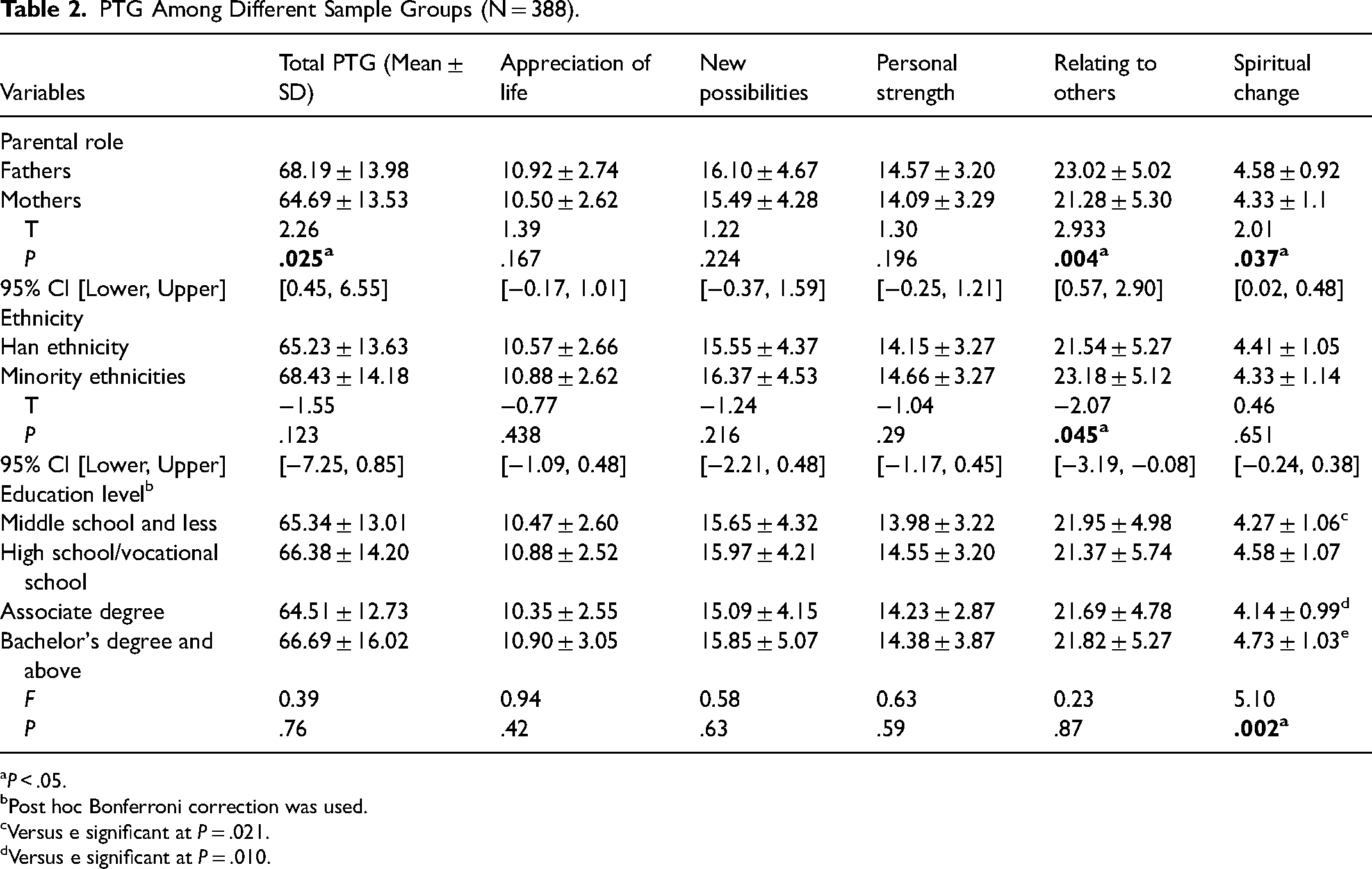
P < .05.
Post hoc Bonferroni correction was used.
Versus e significant at P = .021.
Versus e significant at P = .010.
Correlations of PTG, Social Support, and Coping Style
Mean total score and mean item score of PTG, social support, and coping are displayed in Table 3. In general, both the total scores and subscale scores of social support and PTG were positively and significantly correlated. Regarding the subscales of social support, Subjective Support had the strongest correlation with PTG total and subscale scores. The Objective Support scores were not significantly correlated with the total scores of PTG and its subscales, except for Relating to Others. Coping style was positively correlated with PTG and its subscales, and positive coping had a stronger correlation with PTG than negative coping. Details of the correlations between PTG and social support and coping style are shown in Table 3.
Correlations of PTG, Coping Style, and Social Support (n = 388).
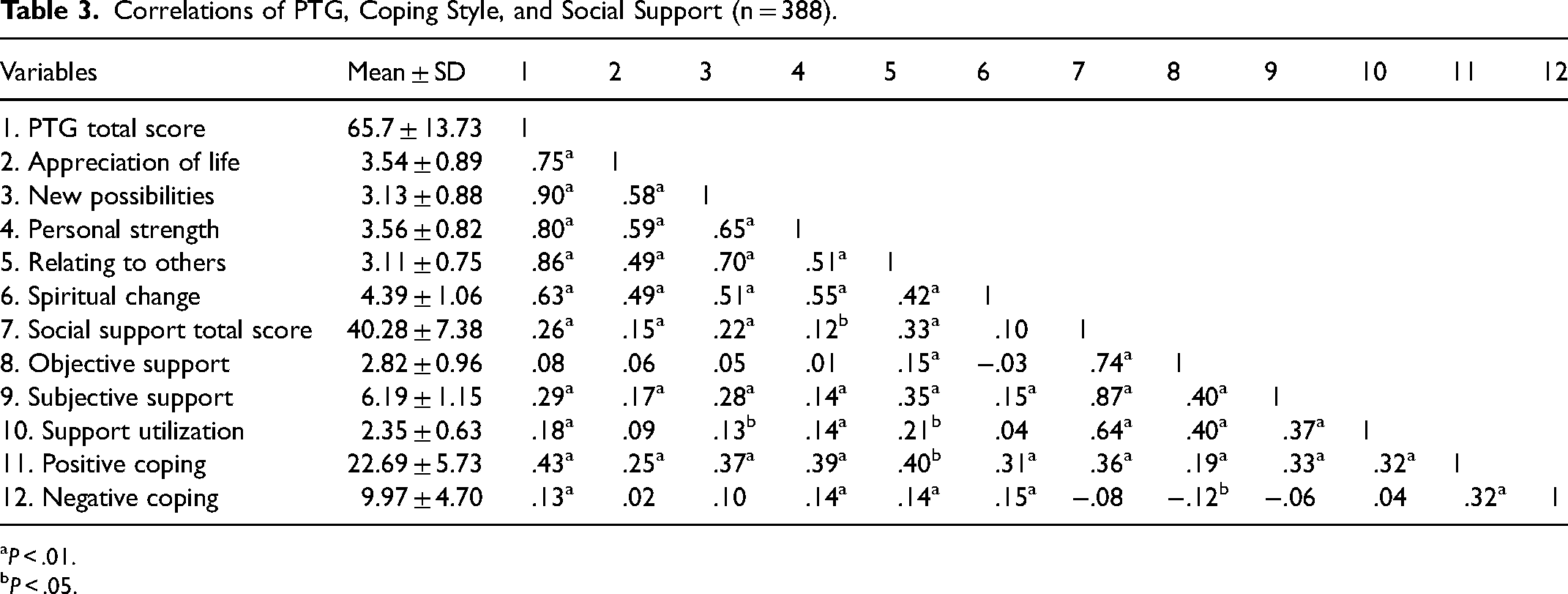
P < .01.
P < .05.
Correlates of PTG
A multiple regression analysis was conducted to identify correlates of PTG level of the participants. Variables with a P value less than .05 on univariate analysis or that had a statistically significant correlation with PTG were included in the multivariate model. Parent gender, ethnicity, education level, cleft type of the participants’ children, social support total score, positive coping score, and negative coping score were selected as independent predictors of the regression model. Although the PTG of the participants did not differ significantly with respect to the cleft type of their children in the univariate analysis, previous studies showed that health outcomes, family quality of life, parental quality of life, and psychological status differed with respect to the cleft types of their children.3,4,10,37 Hence, cleft type was put into the regression model with cleft palate designated as the reference group. The variance inflation factor (VIF) ranged from 1.00 to 1.172, which indicated the absence of multicollinearity. The model revealed that 20.6% of the variance in PTG was explained by positive coping, social support, and cleft type of the participants’ children. The regression model was significant (F(4, 383) = 26.14, P < .001). Positive coping was the strongest correlating factor of PTG (β = 0.349, P < .001). Significant results of the multiple regression are displayed in Table 4. To make sure that important variables being identified, we did a second analysis that included parental sex, education level, ethnicity, marital status, family income, employment status, number of children, child age, urban/rural setting, social support, coping in the multivariate model, and the same result was harvested.
Multiple Linear Regression Model (n = 388).
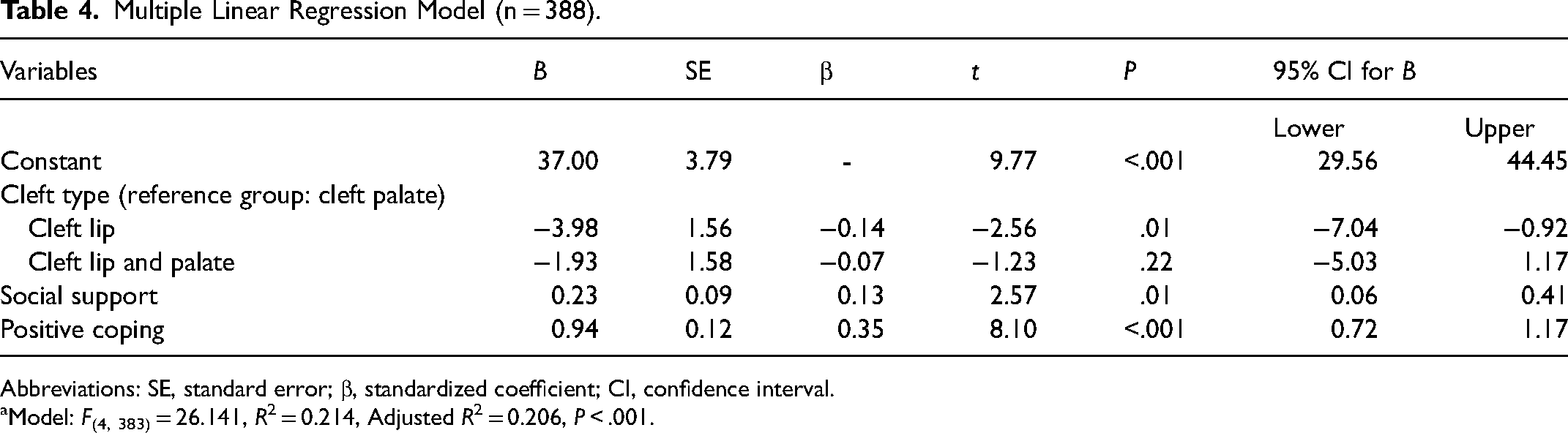
Abbreviations: SE, standard error; β, standardized coefficient; CI, confidence interval.
Model: F(4, 383) = 26.141, R2 = 0.214, Adjusted R2 = 0.206, P < .001.
Discussion
This study explored the PTG of parents of children with CL/P and its correlation with social support and coping style. The PTG of the parents was moderate. In parents of children with CL/P, PTG differed based on the participants’ gender, ethnicity, and education background. Social support and coping style were positively correlated with PTG. The multiple regression analysis showed that cleft type of the participants’ children, social support, and positive coping style were the correlates of PTG among parents of children with CL/P. The PTG of parents of children with cleft palate differed from parents of children with cleft lip but did not differed from parents of children with cleft lip and palate. The results of this study provide a practical guide for the development of effective psychological interventions for this population.
The mean PTG total scores of parents of children with CL/P were moderate (65.65 ± 13.73). Compared with parents of children with other illnesses, parents of children with CL/P in this study had a relatively higher PTG level. The mean total PTG scores of parents of children with critical illness, cancer, autism spectrum, cystic fibrosis, and children who underwent hematopoietic stem cell transplant fluctuated between 47.40 and 66.8.15,17–19,38,39 In the study of O'Hanlon et al, 25 parents (n = 54) of children with CL/P had a relatively lower PTG score (36.74 ± 25.82).
The multiple regression analysis showed that the cleft type of the participants’ children was a correlate of PTG (β = −0.14, P = .01). The PTG of parents of children with developmental disabilities did not differ depending on the children's diagnosis. 21 In parents of children with special needs (children with physical and developmental impairments), there were no significant differences in PTG according to the child's type of diagnosis. 40 However, for parents of children with CL/P, current literature suggested that their psychological parameters differed regarding the cleft types of the children, but it is debated which cleft type have a more severe impact. A longitudinal study revealed that mothers of children with cleft lip and palate and cleft palate had an increased risk of psychological distress. 3 The study of Agnew et al showed that the family impact (parental emotions, family activities, and family conflict) differed with respect to the cleft type of the children. 6 Hence, it may be helpful for healthcare professionals to take the cleft types of the children into consideration when providing psychological interventions to promote the PTG of parents. Further research is needed to determine the influence of the children's cleft type on the psychological aspects of their parents.
Coping style was correlated with PTG. Positive coping was positively correlated with PTG (r = 0.43, P < .01) and explained the most variance (β = 0.35, P < .001) of PTG in parents of children with CL/P. Similarly, the investigation of caregivers (parents and grandparents) of children with developmental disabilities revealed that a positive coping style was positively correlated with PTG. 21 Disengagement coping, characterized as avoidance and denial, is more related to the definition of negative coping style in this study. Disengagement coping was found to be positively correlated with PTG among parents of children who underwent hematopoietic stem cell transplantation, 15 which contradicted our results. Avoidance coping style has been positively related to PTG in prior studies.29,41,42 The fact that denial and avoidance were positively correlated with PTG might be explained because it could, in some individuals, alleviate the anxiety caused by the traumatic event and lead to the perception of growth. 43 Faced with traumatic events, individuals tend to adopt diversified coping strategies, and negative coping strategies such as denial and avoidance do not necessarily guarantee a negative psychological outcome. Hence, it is important that healthcare staff be aware of the varied coping approaches that parents might adopt and promote individualized coping strategies. More research is needed to investigate the coping style of parents of children with CL/P and its relationship with PTG.
Social support was another correlate of PTG (β = 0.13, P < .05) of parents of children with CL/P. In parents of children who underwent stem cell transplantation and caregivers of schizophrenia patients, social support was correlated with PTG to a similar extent as the results of our study.32,44 Social support was a strong and direct predictor of PTG among mothers of children with cancer. 19 The perceived social support of mothers of children with autism spectrum disorders (ASD) was strongly (r = 0.8, P < .05) correlated with PTG. 16 In the theoretical model of both Schaefer and Moo 45 and Tedeschi and Calhoun, 13 social support was considered as a key environmental resource. Social support can lead to personal growth through its effect on coping and adaptive behavior. Social support has been widely proven to boost individual positive adjustment and is commonly considered an important contributor to coping with adversities.46,47 Social support was related to reduced stress levels, increased psychological well-being, and feelings of encouragement and hope and was proven to be a protective factor when individuals suffer from trauma.48,49 It is thus important that healthcare staff evaluate the social support of parents of children with CL/P, including the actual social resources they can employ, perceived tangible and emotional support, and whether they have made full use of accessible resources. Moreover, healthcare staff are obliged to provide sufficient information to parents of children with CL/P about the available financial aid they can apply to subsidize the expense of surgeries for their children. The initial cleft repair surgery expenses of most of our participants’ children were subsidized both by the medical insurance of the government and an international cleft charity institution.
Limitations
Several limitations exist in this study. First, the survey took place during the COVID-19 pandemic, but we did not consider that the pandemic might has a potential impact on parental PTG. More investigations are needed to elucidate the possible relationship between COVID-19 and parental PTG. Second, the cross-sectional design did not provide evidence of causal relationships between PTG and the variables. Future longitudinal research is needed to prove whether there are causal relationships between PTG and coping style and social support in parents of children with CL/P. Third, for parents recruited from WeChat groups, there was a lack of information about their mental health and other potential traumatic experiences. In future research, mental status and previous traumatic experience of parents of children with CL/P should be considered as a potential correlating factor of parental PTG.
Conclusions
This study demonstrated that parents of children with CL/P experienced a moderate level of PTG. The multiple regression model showed that the cleft type of the participants’ children, social support, and positive coping were the correlates of PTG among parents of children with CL/P. Moreover, positive coping was the strongest correlating factor of PTG. This study helped increase understanding of psychological changes and the related factors of parents of children with CL/P in China.
The significant variables identified in this study provide targets for developing and launching future interventions to improve PTG in parents of children with CL/P. Cleft type of the child should be considered, and individualized interventions are needed when providing interventions that improve PTG in parents of children with CL/P. Results suggest that parents of children with cleft palate with or without cleft lip may vary in their PTG from parents of children with cleft lip only. Healthcare professionals should encourage parents of children with CL/P to seek support from family members, healthcare staff, and the community. It would be helpful that healthcare professionals provide information about charity and local public resources to parents of children with CL/P. Positive coping behaviors such as using distractions, seeking support, and talking about problems should be enhanced.
Further cross-sectional and prospective studies are needed to confirm the PTG level and its affecting factors in parents of children with CL/P. Interventional studies that aim to boost the PTG of parents of children with CL/P are also imperative.
Footnotes
Acknowledgments
The authors acknowledge all the participating parents and their children for their cooperation in this study.
Authors’ Note
The study was approved by the Biomedical Ethics Review Committee of the hospital (CT-2020-438).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.