
Abstract
Background
Many cleft centers incorporate NasoAlveolar Molding (NAM) into their presurgical treatment protocols. However, there are limited data on eligible patients who do not receive or complete NAM. This study characterizes the demographics associated with non-utilization or completion of NAM.
Methods
A single-institution retrospective review was performed of all patients with cleft lip and alveolus undergoing primary unilateral and bilateral cleft lip repair from 2012-2020. Patients were grouped based on utilization or non-utilization of NAM. Demographic and treatment data were collected, including documented reasons for not pursuing or completing NAM.
Results
Of 230 eligible patients, 61 patients (27%) did not undergo or complete NAM (no-NAM). In this group, 37 (60.7%) received no presurgical intervention, 12 (19.7%) received presurgical nostril retainers, 3 (4.9%) received lip taping, 1 (1.6%) received a combination of taping/nostril retainers, and 8 (13.1%) discontinued NAM. The most common reasons for not receiving NAM were sufficiently aligned cleft alveolus (21.3%), medical complexity (16.4%), late presentation (16.4%), and alveolar notching (18%). Compared to the NAM group, the no-NAM group had significantly lower rates of prenatal cleft diagnosis/consult, and significantly higher proportion of non-married and non-English speaking caregivers. Multivariable analysis controlling for insurance type, primary language, prenatal consult, marital status, and age at first appointment found that age at first appointment is the only statistically significant predictor of NAM utilization (P < .001).
Conclusions
Common reasons for non-utilization of NAM include well-aligned cleft alveolus, medical complexity, and late presentation. Early presentation is an important modifiable factor affecting rates of NAM utilization.
Keywords
Introduction
In cleft care, presurgical infant orthopedics (PSIO) aims to reduce the initial cleft deformity by approximating the alveolar cleft segments and correcting the nasal soft tissue deformity.1–3 A recent survey study reported that over half of the American Cleft Palate-Craniofacial Association (ACPA)-approved cleft teams offer some type of PSIO as part of the cleft treatment protocol, with a majority of these centers utilizing nasoalveolar molding (NAM) therapy.4–6 NAM has been shown to reduce cleft severity prior to primary surgical repair, facilitate gingivoperiosteoplasty (GPP) to decrease the need for secondary alveolar bone grafting, and improve lip and nasal form.7–11
However, despite reported improvements in aesthetic, functional, and psychological outcomes secondary to NAM treatment, the ease of access to and utilization of NAM has remained a topic of debate.12–17 The early start of treatment, frequency of visits, financial commitment, and management of potential complications required for successful completion of NAM has been bundled to represent the “burden of care” associated with NAM.18,19 Despite identifying such potential barriers to care, there is limited data on the reasons for and characteristics of the patient population that may be eligible for but ultimately do not receive NAM treatment. 20
Therefore, this study aims to investigate a single institution's experience with the cohort of patients with cleft lip and alveolus who are assessed for but do not receive NAM therapy. In addition, this patient group is compared to the cohort of patients undergoing NAM at this institution to identify demographic differences that may be contributing to the final treatment decision to participate in NAM therapy.
Methods
Patient Cohort
With institutional review board approval, we performed a single-institution, retrospective review of all patients with cleft lip and alveolus (with or without cleft palate) who underwent primary unilateral or bilateral cleft lip repair from 2012-2020. We excluded patients presenting for revision surgery, those with syndromic facial clefts, those who received NAM at an outside institution, and those whose presurgical assessment was unavailable within the medical record.
Nasoalveolar Molding Protocol
The NAM treatment protocol utilized at this institution has been previously described.21,22 When possible, families are introduced to NAM at a prenatal visit, where they also meet with a surgeon, orthodontist, team nurse practitioner, feeding specialist, and social worker. Postnatally, patients are deemed eligible for NAM by a craniofacial plastic surgeon or a craniofacial orthodontist. Criteria for receiving NAM include patients with clefts involving significant nasal and alveolar deformity greater than 1-2 mm, whose presentation and impressions are completed before four weeks of age. An institution-specific four week cutoff is utilized to account for the ability of circulating maternal estrogens to aid in malleability of the nasal cartilages. Experience at our institution has suggested that NAM therapy initiated after four weeks likely extends to 4-6 months of age, at which point infants often learn to pull out the appliance; additionally, when NAM is initiated at a later age, infant's have greater difficulty adjusting to feeding with the appliance. In infants born preterm (37 weeks gestation), treatment is delayed until the corrected 40 week age to ensure there are no feeding or weight gain issues. For patients with incomplete cleft lip with minimal nasal deformity, no presurgical interventions are performed.
If NAM therapy is indicated and the caregiver chooses to pursue therapy, consent is obtained and a soft body polyvinyl siloxane (PVS) impressions is obtained of the maxillary gum pads to fabricate the molding plate. One week after the impression appointment, the alveolar molding plate is inserted and instructions on insertion, tapping, and feeding with the molding plate is reviewed with the caregiver. Depending on cleft severity, a nasal stent may be added to the molding plate 4-6 weeks into treatment. Patients received nostril retainer (Stryker) only if they presented with incomplete cleft lip with mild nasal deformity. Patients were offered lip taping only if they presented late for their initial visit.
In patients undergoing NAM therapy, progress is monitored regularly, and the NAM appliance is adjusted weekly to mold the alveolar segments and nose. The treatment continues for approximately three months for infants with UCLP and four months for infants with BCLP. In patients undergoing nostril retainer or lip taping, progress is monitored every two to three weeks. Patients who did not receive PSIO treatment are typically seen every four weeks before primary cleft lip repair, which occurs around three months for both unilateral and bilateral cleft lip.
Data Collection
Demographic variables collected included age at first clinic appointment, sex, race, family history of cleft, primary caregiver's marital status, caregiver's primary language, interpreter request, number of siblings, the distance of family commute from the cleft center, and insurance type. NAM-related variables included type of presurgical orthopedic intervention, any documented reason for not pursuing NAM, prenatal diagnosis, prenatal consult with plastic surgery, age at the start of presurgical treatment, duration of presurgical treatment, total visit history, complications, and postsurgical nasal stenting.
Statistical Analysis
Data was analyzed using Statistical Package for the Social Sciences (SPSS) software (version 28.0, IBM Corp. Armonk, NY). Categorical data points were analyzed by Chi squared analysis. Continuous variables were analyzed via independent samples t-test. Values were reported as mean ± standard deviation when appropriate. Logistic regression was used to analyze the relationship between NAM utilization and socioeconomic variables of insurance type, primary language, prenatal consult, marital status, and age at first appointment. Variables that were not available in >20% of the dataset were not included in the model. P-values of less than 0.05 were considered statistically significant.
Results
There were 230 patients eligible for NAM undergoing primary cleft repair. Of this group, there were 177 patients with unilateral cleft lip and 53 patients with bilateral cleft lip; 168 patients had a cleft palate. There were 61 (26.5%) patients who did not undergo NAM (no-NAM) and 169 (73.4%) patients who underwent NAM (NAM). There were no significant differences in sex or age distribution between groups (Table 1).
No-NAM vs NAM: Demographics and Prenatal preparation.
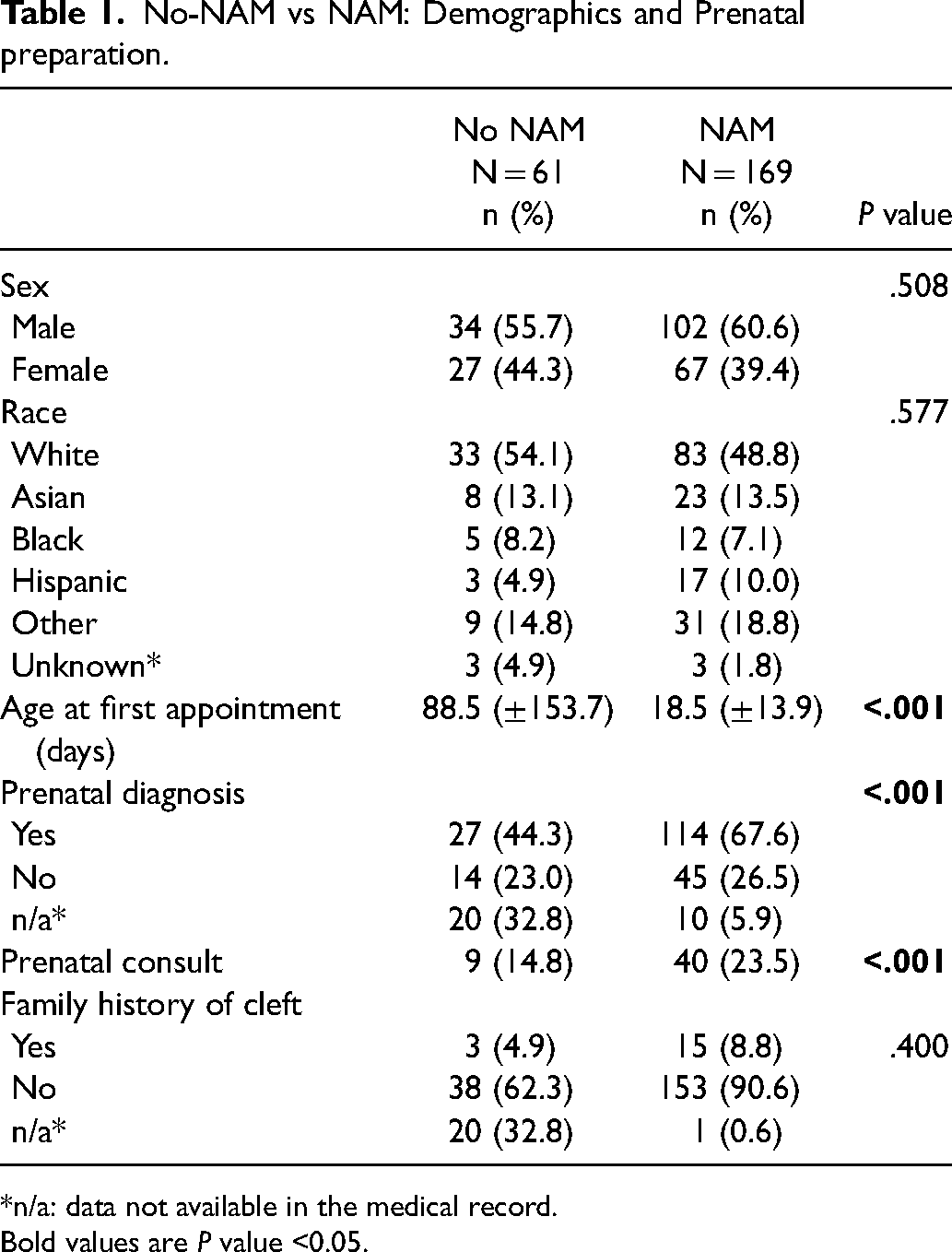
*n/a: data not available in the medical record.
Bold values are P value <0.05.
Prenatal Preparation and First Presentation
Mean age at first clinic appointment was significantly later in the no-NAM group 88.5 (±153.7) days no-NAM vs. 18.5 (±13.9) days NAM (P < .001)] (Table 1). In the NAM group, significantly more patients had a prenatal diagnosis of cleft (114/169, 67.5%) compared to the no-NAM group (27/61, 44.3%) (P < .05). Similarly, significantly more patients were seen for a prenatal consult in the NAM group (40/169, 23.7%) compared to the no-NAM group (9/61, 14.8%). There was no significant difference in the rate of family history of cleft between groups.
Family Characteristics
There was a significantly greater proportion of married primary caregivers in the NAM group (142/169, 84.0%) compared to the no-NAM group (37/61, 60.7%) (P < .001) (Table 2). There were significantly more siblings in the families of the no-NAM group compared to the NAM group (P < .005). There were a significantly greater proportion of families where English was not the primary language in the no-NAM group (30.1%) compared to the NAM group (15.9%), and higher rates of interpreter request during appointments in the no-NAM group (27.9% no-NAM vs 7.6% NAM) (P < .001). There was no significant difference in the average distance of the family home from the hospital between groups (26.0 ± 24.2 miles no-NAM vs 28.4 ± 38.7 miles NAM). There was no significant difference in insurance payer type between groups, with 41% of the no-NAM group and 57.1% of the NAM group with private payer insurance.
No-NAM vs NAM: Family Characteristics.
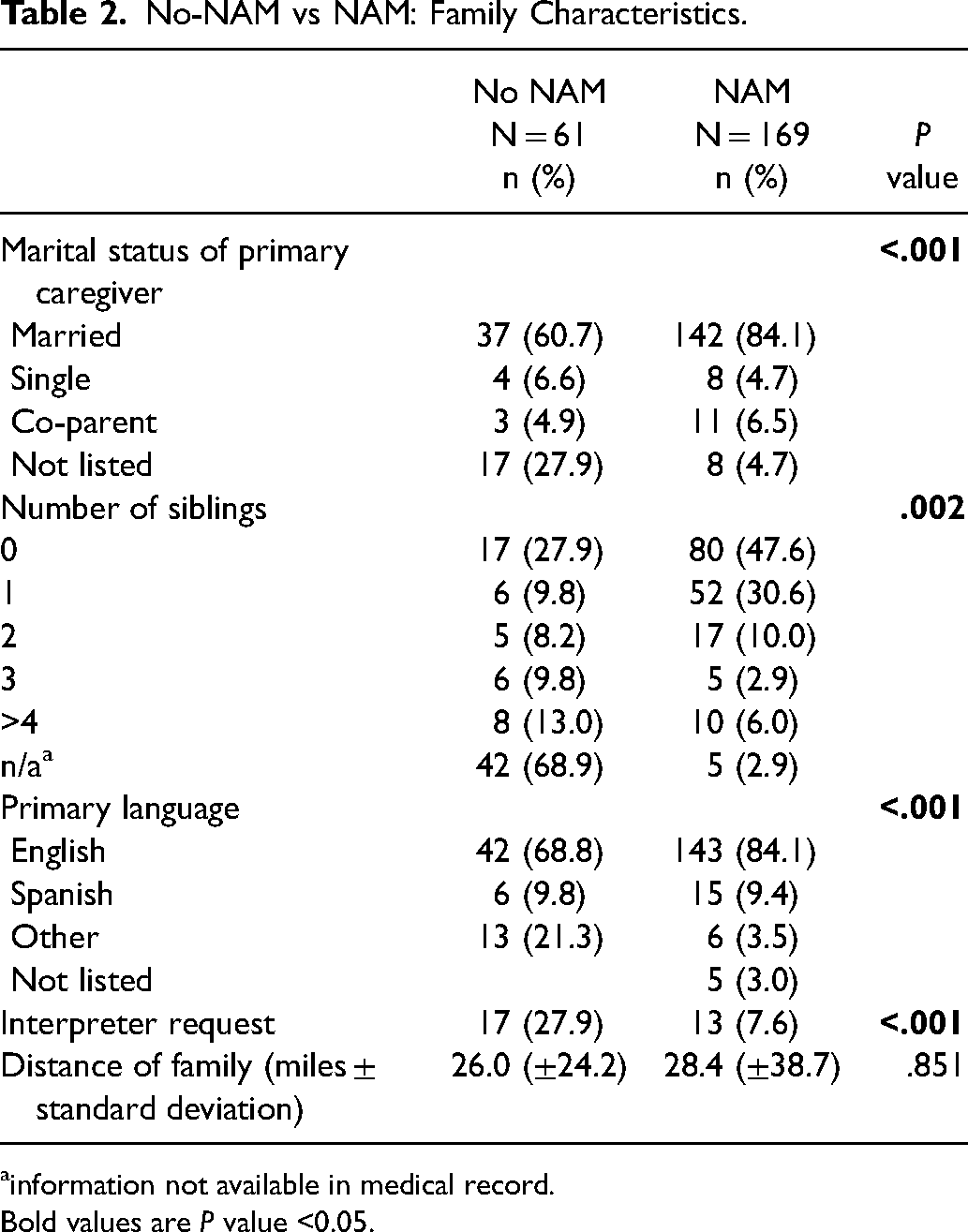
information not available in medical record.
Bold values are P value <0.05.
Modeling NAM Utilization in Relation to Socioeconomic Factors
Logistic regression was used to analyze the relationship between NAM utilization and socioeconomic variables of insurance type, primary language, prenatal consult, marital status, and age at first appointment. It was found that, when controlling for the above variables, only age at first appointment was a statistically significant predictor of NAM utilization, with an increase of 1 week in presentation age associated with 21% reduction in odds of receiving NAM therapy (β = –.237, P < .001; eβ = 0.789 [95% CI: 0.69-0.82]). Insurance type, primary language, prenatal consult, and marital status were not statistically significant predictors in the regression model.
Reasons for no NAM
In the no-NAM group, 37 (60.7%) received no presurgical intervention, 12 (19.7%) received presurgical nostril retainers only, 3 (2.9%) received lip taping only, 1 (1.6%) received combination of taping and nostril retainers, and 8 (13.1%) started but subsequently discontinued NAM treatment (Table 3). The most commonly documented reasons for not receiving NAM therapy were a cleft alveolus with sufficient alignment (13, 21.3%), medically complex patient (9, 14.8%), late presentation (10, 6.4%), and alveolar notching (11, 18%).
No-NAM vs NAM: Pre- and Post-Surgical Treatment.
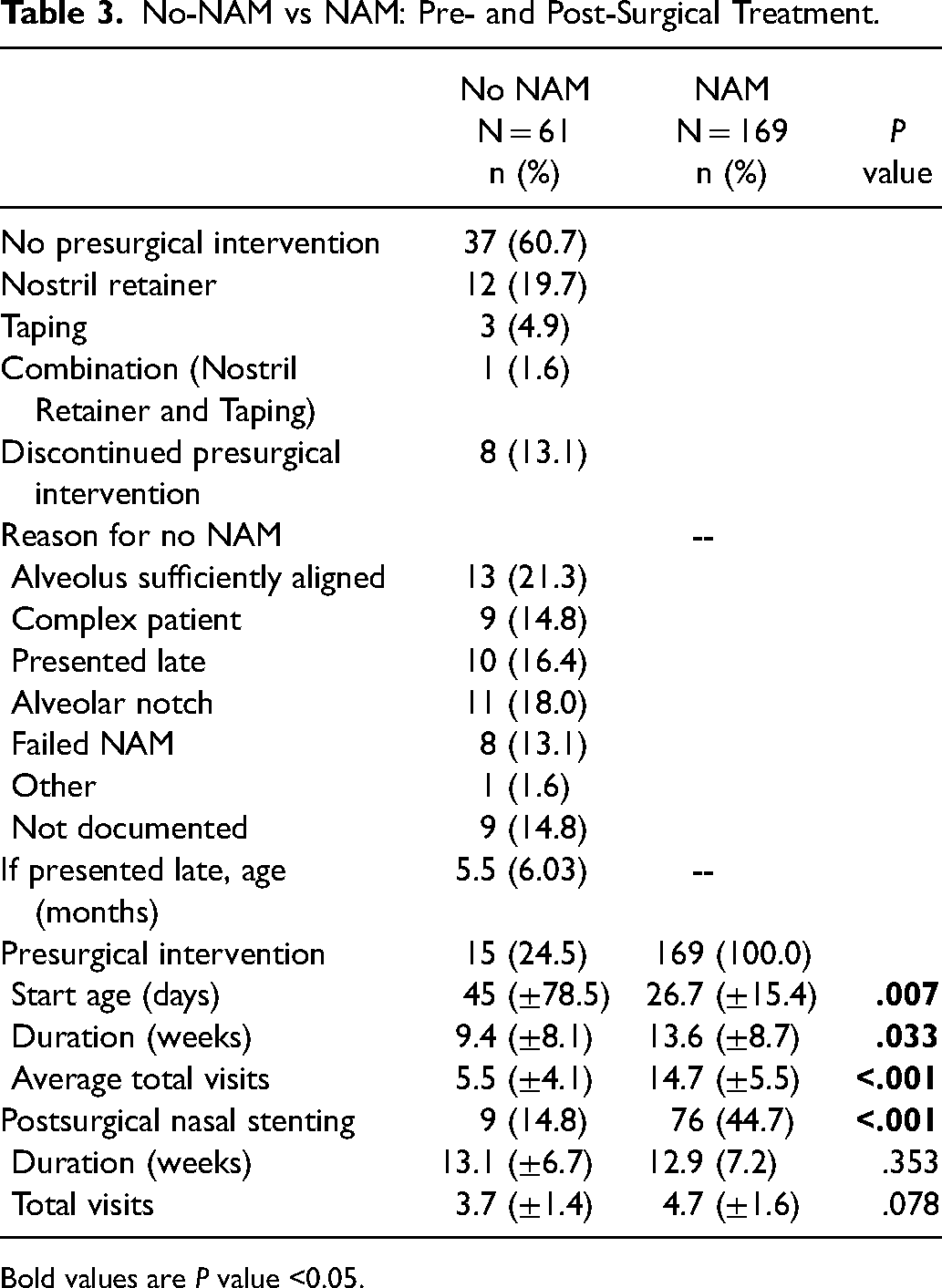
Bold values are P value <0.05.
Of those patients whose documented reason for no NAM was late presentation, average age at first appointment was 5.5 (±6.03) months. In these patients, 1 patient received taping and 9 patients received no presurgical intervention. Notably, 4/10 patients had traveled internationally for primary surgery.
Of those patients whose documented reason for no NAM was medical complexity, 5 patients had syndromic cleft with additional medical comorbidities, 2 patients had cardiac conditions requiring pediatric cardiology management, and 1 patient required management by multiple pediatric specialists. Of these patients, 1 patient attempted NAM but had to discontinue and change to taping only, 2 patients received taping, 1 patient received presurgical nostril retainers, and 6 patients received no presurgical intervention.
In the patients who discontinued NAM therapy, reasons for discontinuation were feeding difficulties (2/8), parental desire to discontinue (3/8), persistent oral mucosa ulceration (1/8), and difficulty managing NAM with medical comorbidities (1/8).
Presurgical Interventions in the No-NAM Group
In the patients that did not receive NAM but received a presurgical intervention in the form of lip taping or nostril retainers, age at start of treatment was significantly later [45 (±78.5) days] compared to the age at start for the NAM group [26.7 (±15.4) days] (Table 3). The duration of treatment was significantly shorter for no-NAM presurgical interventions, lasting an average of 9.4 (±8.1) weeks compared to average duration of 13.6 (±8.7) weeks for the NAM group (P < .01). On average, no-NAM presurgical interventions required fewer total visits at 5.5 (±4.1) visits compared to 14.7 (±5.5) visits for the NAM group (P < .05). No surgical lip adhesion was performed in any patient during this study period.
Postsurgical Interventions
In the no-NAM group, 9 (14.8%) patients received postsurgical nasal retainers, compared to 76 (44.7%) in the NAM group (P < .001). There were no significant differences in duration or total visits associated with postsurgical interventions between groups.
Discussion
This study investigates documented reasons for non-utilization or non-completion of NAM therapy at a high-volume urban cleft center. The most commonly reported reasons for not undergoing NAM included both those that are inherently patient-specific and not modifiable, such as anatomic alveolar cleft alignment/notching and medical comorbidities, as well as those that are modifiable, such as a late presentation. Furthermore, this study shows that the majority (73%) of patients assessed and considered eligible for NAM receive and successfully complete treatment at our institution. When removing those patients who were assessed for, but did not require NAM due to anatomic alignment or notching of the alveolar cleft, the rate of NAM utilization increases to 83%. This is higher than rates of NAM utilization reported in the literature. 23
The most important modifiable reason for not pursuing NAM in this patient cohort was late presentation, accounting for 16% of the no-NAM group. Furthermore, when statistically significant variables from the univariate analyses were modeled in a logistic regression for utilization of NAM, age at presentation was the only statistically significant predictor, suggesting that early presentation to a cleft center is an important modifiable factor to promote increased NAM utilization. In the domestic cohort, early diagnosis, consult, and prenatal family education can help promote connection with the cleft center that will ensure timely assessment for NAM therapy. Late presentation in the international patient cohort is more difficult to modify, as resources and regulations often limit families traveling internationally for care. Notably, patients in the no-NAM group had less prenatal preparation than the NAM group, with significantly lower rates of prenatal diagnosis and consult and significantly older age at the first clinic appointment. As parents who do not undergo prenatal diagnosis are unaware that their child is affected by a cleft, the time of delivery can be an emotionally intense and confusing time; this likely makes it difficult for new parents to educate themselves regarding cleft care and reconstruction. Parents may not fully appreciate the potential benefit of NAM and the importance of early implementation to for both intervention candidacy and success. Our data suggests that prenatal preparation is paramount to setting up timely access to care, and that there is a targetable gap in patient education that may be precluding participation in NAM.
Patients in the no-NAM group had higher rates of non-English speaking caregivers. There is evidence in the cleft care literature of delays in presentation occurring at disproportionate rates in families who are non-English speaking or of lower socioeconomic status.24–26 Studies have shown a trend towards delays in presentation or in time to cleft repair in minority patients compared to Caucasian patients.27–29 Although the results of this study show no significant differences in race or insurance type between NAM and no-NAM groups, the holistic interpretation of our results, in which no-NAM patients had less prenatal preparation, older age at presentation, higher proportion of non-English speaking primary caregivers, and larger family size than NAM patients, points to a broader picture of family resources and preparedness that affects NAM utilization. Recent literature has shown that creating dedicated roles for patient outreach and education in cleft care has resulted in earlier age at presentation, especially in nonwhite and publicly insured patients. 24 This suggests that targeted, education-based interventions in communities can positively impact disparities in cleft care.
As noted, insurance coverage and distance of families from the hospital, commonly cited as typical barriers to access to NAM treatment, were not significantly different between NAM and no-NAM groups in this study.23,30 The authors would note that the location of the study center is in a large metropolitan area with a robust public transportation system. Furthermore, the study center receives foundational grant funding for cleft care which includes financial support for NAM in cases when insurance will not cover costs. Marital status of parents and number of siblings, which have been identified in the literature as contributing to NAM adherence or completion, were significantly different between the NAM and no-NAM groups, with the no-NAM group having a lower proportion of married parents and higher average number of siblings. 30 This social support structure has been previously highlighted in analyses of smaller cohorts of our institutional data. 31 The variability seen across these measures in the literature may be due to regional differences in patient population, availability of public transportation, and density of available cleft centers. 31 However, our results and those reported in the literature underscore the significant role that family resources play in the successful completion of NAM.
The logistic regression model based on socioeconomic status variables (insurance type, primary language spoken, prenatal consult, age at first appointment, marital status) to predict the utilization of NAM therapy found that when controlling for interactions between variables, the only statistically significant predictor of NAM utilization was age at first appointment. Although the heterogeneity of the available dataset precluded addition of other statistically significant variables from the univariate analysis, such as number of siblings, the fact that the other socioeconomic status-related variables are not statistically significant predictors when controlling for related variability is promising. This finding suggests that there is not a single specific socioeconomic status-related factor that affects NAM utilization, and that once patients present to clinic in an appropriate time frame, utilization of NAM is equitable. The next step is research into the measures that affect early presentation to cleft care to aid in parsing out the socioeconomic factors that influence pursuit of early care.
For patients deemed medically complex or whose families could not meet all the demands of NAM treatment, this study showed that alternative presurgical interventions such as lip taping are feasible as they require fewer visits and have a shorter duration of treatment. Given recent data on the effects of lip taping on reduction of cleft width, alternative presurgical interventions to NAM should be considered in cases when NAM is indicated but cannot be managed due to medical or social issues. 32 However, it is important to note that lip taping only does not improve nasal deformity, and that the outcomes from this intervention are not comparable to what is achieved through NAM.
Interestingly, the NAM group in this study had higher rates of postsurgical retainer compared to the no-NAM group. Other institutions have reported higher rates of postsurgical stenting in patients who do not receive NAM, presumably because this population has an increased need for nasal shape retention. 6 In our experience, patients who do not undergo NAM tend to have a mild cleft deformity with a mild nasal deformity. The decision to use nostril retainers at our institution is made on postoperative week 3, after examination by the treating surgeon and orthodontist. Children with a mild preoperative cleft nasal deformity may not require a nostril retainer when assessed three weeks after surgery. The rates of postsurgical retainer use seen in our patient groups may also be reflective of the greater proportion of international patients in the no NAM group that are not available for postsurgical interventions, or may speak to a broader pattern of greater patient follow up in the NAM group. It is possible that families who have already undergone NAM are more comfortable with these at-home interventions, and may elect to participate more frequently than families who did not undergo presurgical interventions.
This study reports a NAM discontinuation rate of 4.5% due to feeding issues, parental desire to discontinue treatment, and oral mucosa ulceration. Reported noncompletion rates in the literature range from 13% to 16%, with most common reported reasons being device intolerance, feeding difficulties, or soft tissue complications.20,23
Although this study aims to report documented reasons for not pursuing NAM, limitations of this study include surgeon or orthodontist-dependent variations in the clinical assessment that cannot be measured in this study. Previous studies have shown that the treating surgeon can have a significant impact on the pursuit of NAM. Finally, in order to maintain consistency, this study only includes patients who presented for NAM assessment at our institution. It therefore excludes patients that received NAM at an outside institution, whether domestically or internationally, prior to undergoing primary surgical repair at our institution. Finally, though this study evaluates a large series of patients evaluated for NAM, and reviews records of all patients presenting to a single institution, there may be selection bias related to the patient population that seeks evaluation and treatment at this cleft center that affects generalizability of this study.
The goals of this study are twofold: (1) to report on NAM utilization patterns at a high-volume, urban cleft center, and (2) to identify potential barriers to care in utilization of NAM. These findings can help inform future efforts to maximize NAM utilization at our own institution and to encourage other cleft centers to be proactive in targeting the modifiable barriers to care identified here. To date, advocates of NAM have made significant efforts to educate the community of cleft professionals and to increase access to NAM both in the US and internationally.14,33 As the utility and benefits of NAM has progressively gained acceptance, the next step of NAM advocacy lies in widespread family education, increasing resources to support families through the NAM process, and potentially modifying the way NAM care is delivered, whether via incorporation of telemedicine, virtual reality education, or 3D printing of NAM appliances.34–38
Conclusion
Common reasons for non-utilization of NAM include well-aligned cleft alveolus, medical complexity, and late presentation. Late presentation is an important modifiable factor in increasing utilization of NAM. Socioeconomic factors such as caregiver marital status, number of children, and primary language may affect rates of NAM utilization. The identification of these potential predictors of NAM utilization should be used to guide efforts to improve access to care and technological advancement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Association of Orthodontic Foundation, (grant number Robert L. Boyd Biomedical Research Award 2020-2021).