
Abstract
Objective
Children with hypopituitarism (CwHP) can present with orofacial clefting, frequently in the setting of multiple midline anomalies. Hypopituitarism (HP) can complicate medical and surgical care; the perioperative risk in CwHP during the traditionally lower risk cleft lip and/or palate (CL/P) repair is not well described. The objective of this study is to examine the differences in complications and mortality of CL/P repair in CwHP compared to children without hypopituitarism (CwoHP).
Design
A retrospective cross-sectional analysis.
Setting
The 1997 to 2019 Kids’ Inpatient Databases (KID).
Patients
Children 3 years old and younger who underwent CL/P repair.
Main Outcome Measure(s)
Complications and mortality.
Results
A total of 34 106 weighted cases were analyzed, with 86 having HP. CwHP had a longer length of stay (3.0 days [IQR 2.0-10.0] vs 1.0 day [IQR 1.0-2.0], P < .001) and higher rates of complications and mortality (12.8% vs 2.9%, P < .001) compared to CwoHP. Controlling for demographic factors, CwHP had 6.61 higher odds of complications and mortality than CwoHP (95% CI 3.38-12.94, P < .001).
Conclusions
CwHP can present with a CL/P and other midline defects that can increase the complexity of their care. These data show a significant increase in length of stay, complications, and mortality in CwHP undergoing CL/P repair. Increased multidisciplinary attention and monitoring may be needed for these children peri- and postoperatively, especially if additional comorbidities are present. Further studies on perioperative management in this population are warranted to reduce morbidity and mortality.
Introduction
Cleft lip and/or palate (CL/P) is the most common congenital orofacial defect in the United States. 1 According to the American Cleft Palate-Craniofacial Association (ACPA), CL repair is recommended to be performed by 12 months and CP repair by 18 months of age. 2 CL/P repair has been shown to be safely performed with a low complication rate in the outpatient setting.3-6 However, because CL/P can be associated with a wide range of craniofacial or genetic syndromes, outcomes can vary depending on comorbidities and other patient-specific factors.7-9
CL/P can be present in children with congenital hypopituitarism (CwHP). This condition is rare, with an estimated incidence of 1 in 4000 to 10 000 live births.10,11 CwHP can have a variety of genetic defects that can lead to a range of comorbidities.11-13 Because congenital hypopituitarism can be caused by embryologic malformations of the pituitary gland, other midline defects can occur, such as abdominal wall defects, neural tube defects, absence of the corpus callosum, and midline CL/P.12,14 Moreover, CwHP can have significant hormonal abnormalities, further complicating their medical and surgical care.12,15 This condition has been shown previously to increase mortality, primarily through cardiovascular, respiratory, and cerebrovascular diseases.16,17 While CL/P repair is a surgical procedure with low morbidity and mortality, it is unknown if a similar level of risk can be assumed in patients with CwHP.
Since CwHP is a condition with low incidence and prevalence, a retrospective, cross-sectional analysis using a nationally representative dataset was performed to compare the complications and mortality of CL/P repair in CwHP to children without hypopituitarism (CwoHP). A secondary aim was to describe the demographic factors of the population of CwHP undergoing CL/P repair that may further increase their risk of complications and mortality. We hypothesized that CwHP would have higher complication and mortality rates than CwoHP after CL/P repair.
Materials and Methods
Data Source
The Kids’ Inpatient Database (KID), part of the Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality, is the largest publicly available all-payer pediatric inpatient database in the United States with data published every 3 to 4 years. 18 The database samples 80% of all complicated newborns and other pediatric discharges and 10% of all normal in-hospital births from reporting states. The KID had 22 states contributing to the database in 1997 to 48 states plus the District of Columbia in 2019. The database includes demographic information, including patient age at admission, sex, race, primary expected payer, and hospital region. Information on the hospital course is from the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) Diagnosis Codes (DC) and Procedures Codes (PC) for each admission. The database is weighted to enable its use to generate national estimates. Because all data in the KID are de-identified and are compliant with the Health Insurance Portability and Accountability Act.
Data Analysis
The 1997, 2000, 2003, 2006, 2009, 2012, 2016, and 2019 KID were queried for admission for CL/P repair. We included children 3 years of age and younger. This age group was selected to exclude patients receiving very late repairs. Children diagnosed with hypopituitarism were identified and compared to a CwoHP cohort within the study population. Age, sex, race, hospital region, hospital location, hospital size, expected primary payer, income quartile, length of stay, number of procedures, and charges during hospital admission were collected. The number of procedures was defined as a total number of ICD-9 CM or ICD-10-CM procedures coded on the discharge record. Complications for this study encompassed mortality, hemorrhage, hematoma, seroma, airway/respiratory failure, respiratory complication, infection, wound disruption, cardiac arrest, shock, pneumonia, fistula, cardiac complication, and other complications. The ICD-9-CM and ICD-10-CM codes used for the diagnoses and procedures are listed in Appendix 1.
Statistical Analysis
Statistical analyses were performed with SPSS 27.0 (IBM Corporation, Armonk, NY). Categorical variables were summarized by frequency and percentage. All continuous variables were tested for normal distribution as determined by the Kolmogorov-Smirnov test. Continuous variables were described as mean ± standard deviation (SD) or median with 25th to 75th interquartile range (IQR) based on normality. Comparisons of baseline characteristics and outcomes (categorical variables) were performed using Pearson's Chi-square test. Comparisons between continuous variables were performed with a t-test or Mann-Whitney test as appropriate. Multivariable logistic regression was performed to examine whether variables like age, gender, race and ethnicity, insurance, hospital size, hospital region, and income quartile play a role in certain complications for children who underwent CL/P repair. Independent variables with a frequency less than 11 were removed in order to protect patient identity, per HCUP policy, and were not included in multivariable analysis. A P-value of < .05 was considered to indicate a statistically significant difference for all statistical tests.
Results
Patient Characteristics
Of a total of 34 106 weighted cases who underwent CL/P repair, 86 had a diagnosis of hypopituitarism (Table 1). CwHP had higher rates of repair at 2 years of age (17.2% vs 8.0%, P = .009) compared to CwoHP, but lower rates at 1 year (19.5% vs 24.5%, P = .009) and 0 years of age (58.1% vs 64.7%, P = .009). In the CwHP, a higher proportion were females (66.3% vs 43.3%, P < .001), Black (14.0% vs 5.7%, p = .004), and Hispanic (25.6% vs 19.2%, P = .004). CwHP received their repair at urban nonteaching hospitals at higher rates (16.3% vs 8.9%, P = .019) than CwoHP. No statistical differences were seen in insurance, hospital region, hospital size, and income quartile between these groups.
Comparison of Demographic and Clinical Characteristics by Hypopituitarism Status for Children Who Underwent Cleft Lip and/or Palate Repair.
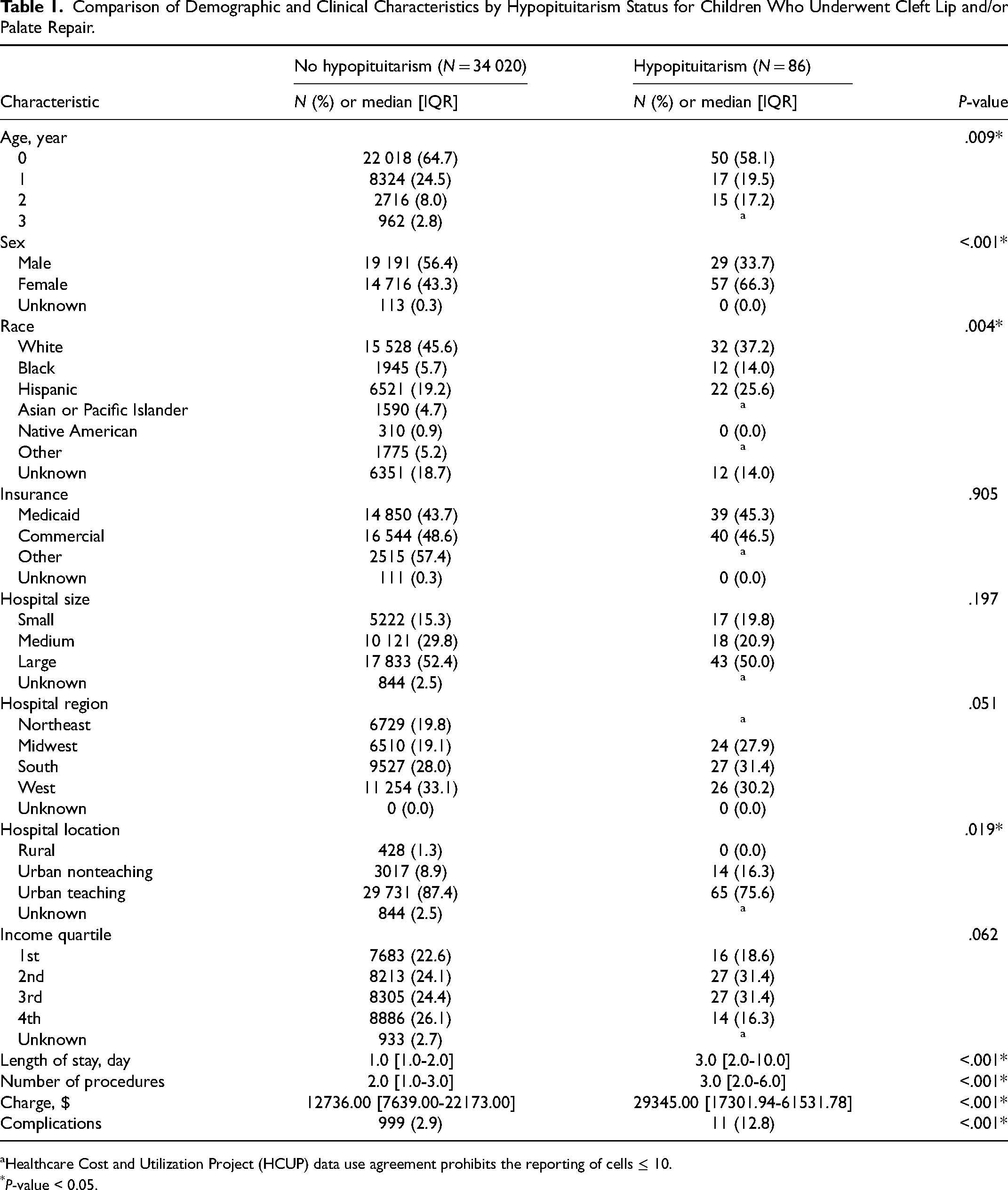
Healthcare Cost and Utilization Project (HCUP) data use agreement prohibits the reporting of cells ≤ 10.
P-value < 0.05.
Outcomes
CwHP had a longer length of stay (3.0 days [2.0-10.0] vs 1.0 days [1.0-2.0], P < .001), higher charges ($29345.00 [17301.94-61531.78] vs $12736.00 [73639.00-22173.00], P < .001), and more total number of procedures (3.0 [2.0-6.0] vs 2.0 [1.0-3.0], P < .001) than CwoHP during their hospitalization (Table 1). CwHP had higher rates of complications than CwoHP (12.8% vs 2.9%, P < .001) after CL/P repair.
Complications
A total of 1011 (3.0%) children in the cohort experienced a complication after CL/P repair (Table 2). More complications were seen in children aged 2 years (12.8% vs 7.9%, P < .001) and 3 years of age (4.3% vs 2.8%, P < .001) at the time of CL/P repair. Black children (8.0% vs 5.7%, P = .020), children insured under Medicaid (52.0% vs 43.4%, P < .001), and children in the first-income (24.0% vs 22.5%, P = .010) and second-income quartile (27.1% vs 24.1%, P = .010) accounted for a higher proportion of children with complications. Complications occurred more in children at large hospitals (57.0% vs 52.3%, P < .001) and in the South (32.9% vs 27.9%, P = .002). There were no statistical differences seen between sex and hospital location for these 2 groups.
Univariate Analysis of Demographic and Clinical Characteristics by Complication for Children Who Underwent Cleft Lip and/or Palate Repair.
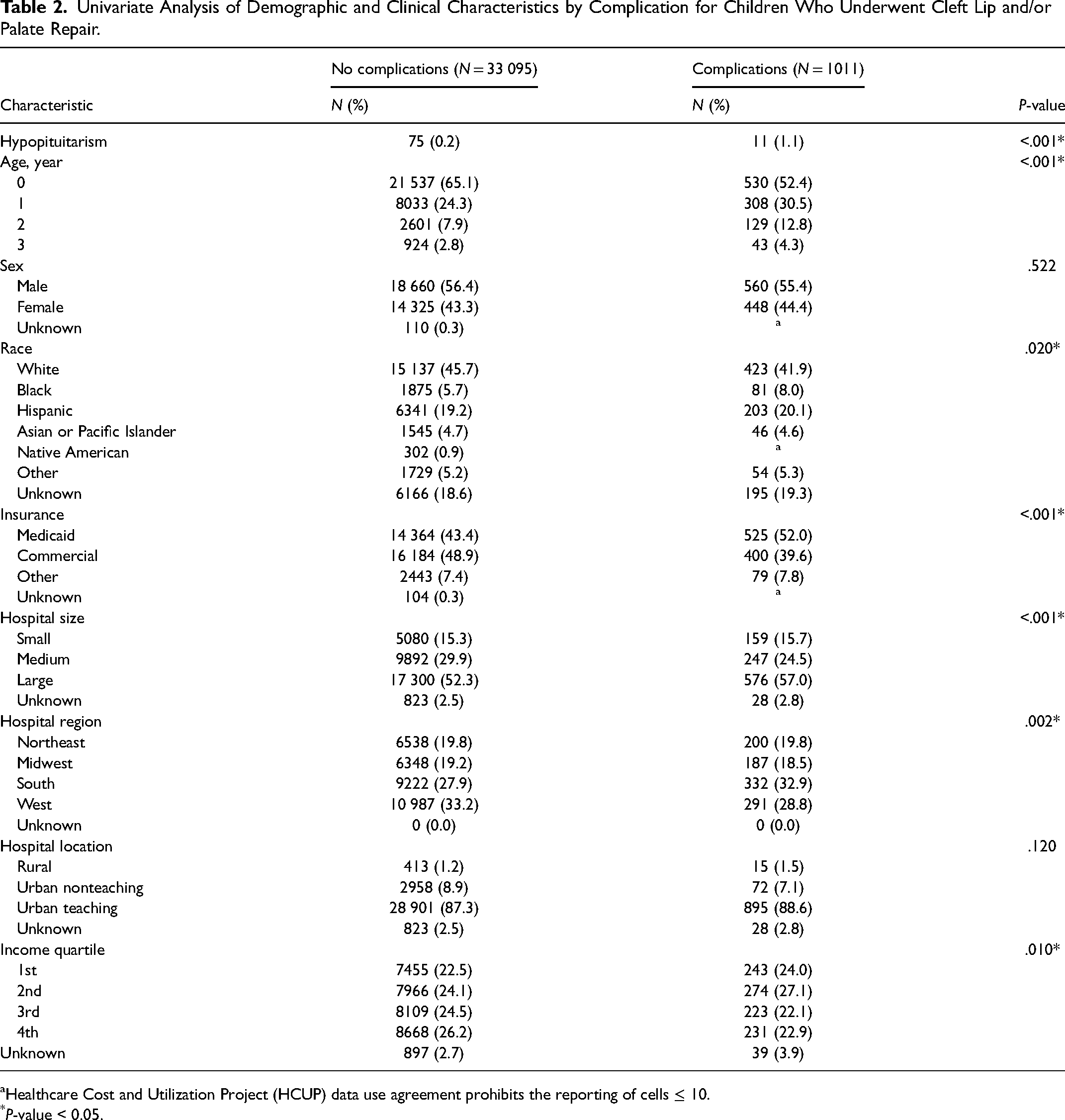
Healthcare Cost and Utilization Project (HCUP) data use agreement prohibits the reporting of cells ≤ 10.
P-value < 0.05.
On multivariate logistic regression controlling for age, sex, race, insurance, hospital size, hospital region, and income quartile, CwHP had a 6.61 adjusted odds ratio (aOR) of experiencing a complication after CL/P repair than CwoHP (95% CI: 3.38-12.94, P < .001) (Table 3). In the entire cohort of patients undergoing CL/P repair, children 1, 2, and 3 years of age had increased odds over 0 years of age regarding complications (aOR 1.55, 95% CI: 1.32-1.83, P < .001; 1.85, 95% CI: 1.46-2.34, P < .001; 1.73, 95% CI: 1.17-2.56, P = .006, respectively). Black children had increased odds of a complication compared to White children (aOR 1.31, 95% CI: 1.02-1.70, P = .036). Compared to Medicaid, children with commercial insurance had reduced odds of complications (aOR 0.70, 95% CI: 0.59-0.97, P < .001). Children treated at a medium-sized hospital compared to a small hospital (aOR 0.76, 95% CI: 0.59-0.97, P = .026) and children in the Midwest compared to the Northeast (aOR 0.74, 95% CI: 0.57-0.95, P = .020) had reduced odds of a complication.
Multivariate Logistic Regression of Complications for Children Who Underwent Cleft Lip and/or Palate Repair.
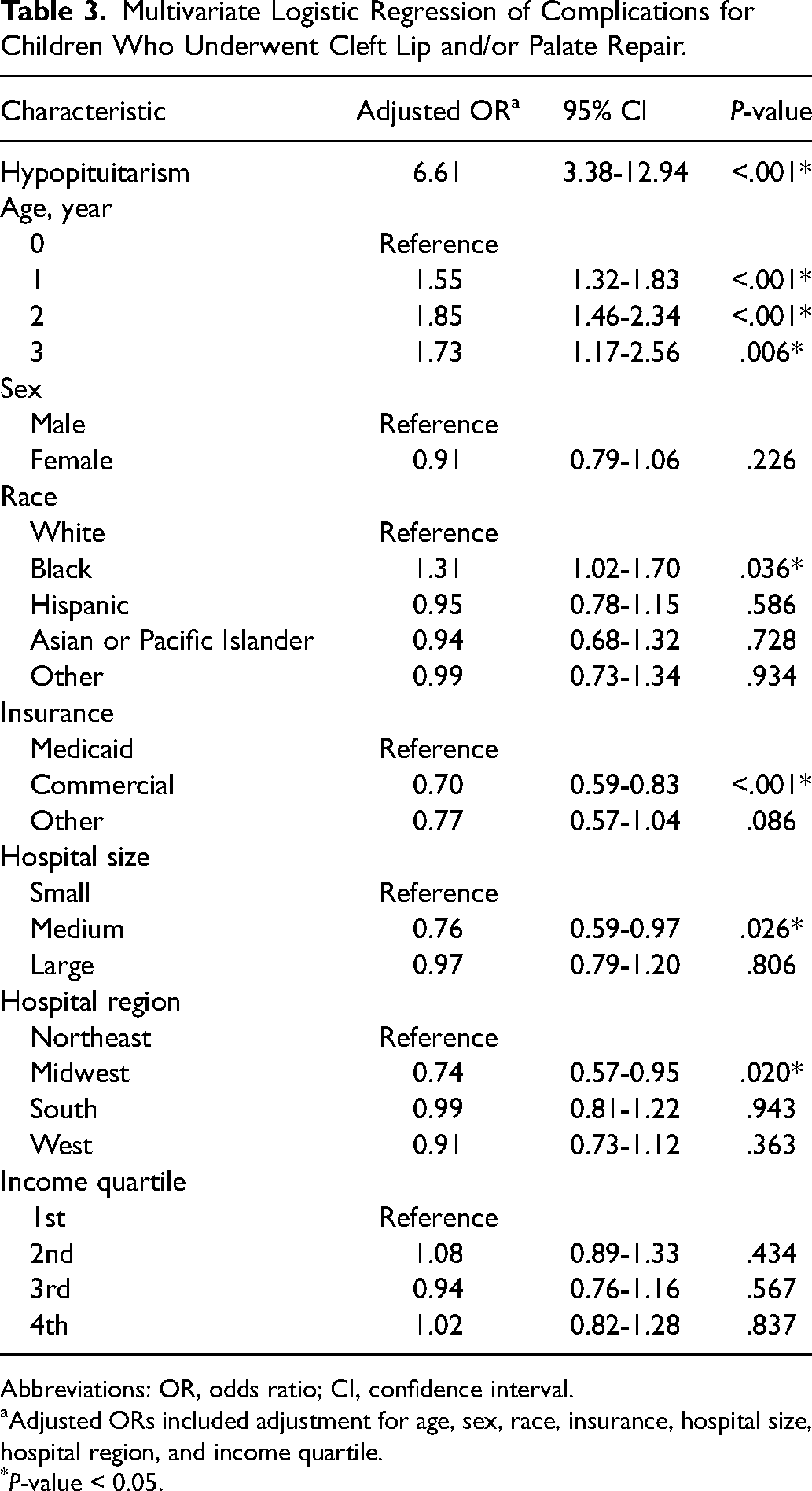
Abbreviations: OR, odds ratio; CI, confidence interval.
Adjusted ORs included adjustment for age, sex, race, insurance, hospital size, hospital region, and income quartile.
P-value < 0.05.
Discussion
CwHP is medically complex patients that may require CL/P repair. Even though CL/P repair has been shown to be safely performed, differing genetic syndromes and comorbidities can modulate this risk.3-9 Since children with CwHP are rare, this population's risk for CL/P repair is currently unknown.10,11 Our study found that CwHP required a longer length of stay in the hospital with an increased total number of procedures, charges, and complications than CwoHP. When controlling for demographic and hospital factors, CwHP had higher than 6 times the odds of experiencing a postoperative complication compared to all CwoHP. Therefore, this study suggests that CwHP are at greater risk of immediate postoperative adverse outcomes after CL/P repair and may warrant more perioperative monitoring and attention than CwoHP. Furthermore, with an increase in the number of outpatient CL/P repairs,19,20 the authors strongly suggest inpatient monitoring rather than ambulatory discharge or 23-h observation for CwHP, in line with the literature regarding other comorbid conditions associated with CL/P.4,19,21,22 Preoperative endocrine and hospitalist or intensivist consultations are a consideration to assess the need for preoperative admission and lab work. Setting appropriate family expectations on length of stay and associated risks is integral.
Mortality after CL/P repair has been shown to be below 0.01%, with other complications such as hemorrhage, airway failure, and dehiscence between 1% and 3%.23,24 These results are similar to the complication rate in the CwoHP (2.9%) group, but CwHP had a much higher rate of 12.8%. The HCUP Data Use Agreement prohibits reporting on variables with a sample size less than 11, therefore we could not report on the specific complications. However, our analysis showed that mortality, hemorrhage, respiratory failure, wound disruption, and pneumonia were the specific adverse outcomes higher in CwHP. One possible explanation for the observed increase in complications is hormonal abnormalities.12,15 Surgery is a known major stressor that elevates cortisol and catecholamines from the hypothalamic-pituitary-adrenal (HPA) axis.25,26 Due to the disruption of the HPA axis in HP, perioperative management of these patients can be challenging. Measuring cortisol response and appropriate replacement of glucocorticoids is crucial to maintaining homeostasis and avoiding a potentially devastating adrenal crisis.27,28 Moreover, other endocrine complications must be monitored, such as polyuria from Diabetes insipidus or hyponatremia from Syndrome of inappropriate antidiuretic hormone secretion.27,29 These challenges were highlighted in a case report of a child with panhypopituitarism undergoing congenital heart disease surgery who developed massive pleural effusions and ascites postoperatively secondary to complex fluid management challenges. 30 These perioperative considerations for CwHP emphasize why these children could respond poorly to surgical stress, leading to higher rates of complications after CL/P repair. Another potential reason is the variety of additional abnormalities associated with HP. For example, children with differing craniofacial syndromes, difficult airways, central nervous system diagnoses, and cardiac abnormalities have been shown to have more perioperative complications and readmission rates after CL/P repair.31-34 With over fifty genetic transcription factors and signaling factors shown to be involved in CwHP, these additional comorbidities can include holoprosencephaly, septo-optic dysplasia, esophageal atresia, and neonatal hypoglycemia.10,16 The results of the present study support that CwHP is another abnormality that needs specific and multispecialty care during their CL/P repair course to reduce their risk of perioperative complications.
Another potential explanation for higher complications is the anatomical and surgical differences between the midline CL/P (Figure 1) typically seen in CwHP compared to the more common unilateral CL/P. Unfortunately, due to the rarity of midline CL/P, no studies directly compare the surgical and perioperative outcomes and complications between these 2 groups. The case reports on smaller midline CL describe various surgical techniques.35-38 For larger midline cleft lips, soft tissue and craniofacial bone repositioning are needed, which is a much more extensive repair.39,40 These case reports discuss that each child with midline CL is unique, thereby requiring unique surgical approaches,35-38 which may explain the higher rates of wound disruption and hemorrhage seen in CwHP. As the literature has shown that complication rates after CL/P repair are higher in low volume centers compared to high volume centers,5,41,42 less experience with midline CL/P could cause higher complications in the CwHP group. In contrast, one study described their repair of midline CL as “fairly straightforward.” 43 Furthermore, this hypothesis does not explain the higher rates of mortality, respiratory failure, and pneumonia seen in the CwHP group. A review argued that the anatomical classifications of midline CL could not appropriately determine outcomes in these patients. 44 Instead, they offered a new classification based on the CL being isolated or associated with other craniofacial abnormalities, such as hypo- or hypertelorism, or systemic abnormalities, such as orofaciodigital syndrome. 44 Overall, while the surgical procedures may be quite varied for patients with midline CL/P, the current literature suggests that the comorbidities and medical fragility of these children play a large role in their challenging perioperative care. 39

Midline cleft lip.
Demographic risk factors have shown some influence on complications after CL/P repair and could further compound the increased risk of CwHP. While delaying CP repair past the recommended timing per the ACPA has been associated with worse long-term outcomes, such as poor speech and velopharyngeal insufficiency, evidence is limited regarding immediate perioperative outcomes.2,45-48 Our study found that CwHP were older at the time of repair and that older children at CL/P repair had increased odds for postoperative complications. In considering patient sex, a single institution study has shown that females require more secondary CL/P surgeries compared to males, but a similar study did not endorse these results.49,50 In our study, while 66.3% of the CwHP were female, sex was not influential in the multivariate analysis of postoperative complications. For race, there is evidence that Black children are more likely to have postoperative complications from CP repair. 6 This analysis endorses these findings, as being Black was a significant factor in the multivariate analysis, and proportionally more CwHP were Black. Lastly, evidence shows that children in lower socioeconomic (SES) groups are more likely to have a CP and have worse outcomes after treatment.41,51 While being on Medicaid was associated with higher odds of postoperative complications, CwHP was not on Medicaid at higher rates than CwoHP. Interestingly, the income quartile was not significant in the multivariate analysis for complications. Overall, while having HP increases a child's risk of postoperative complications, these results suggest that Black children at an older age at the time of repair could compound on this elevated risk.
Several limitations need to be addressed for this study. First, while CwHP can present with a wide variety of additional comorbidities, this group could not be subdivided by these other anomalies or the severity of their phenotypes. Because of the limited number of CwHP and the HCUP Data Use Agreement restricting reporting on variables with small sample sizes, we were not able to report a subgroup analysis on which CwHP may be more likely to experience postoperative complications. As CwHP can have any number of the 6 main hormonal deficiencies from the pituitary, phenotypic presentations are likely heterogeneous. Moreover, these children could experience differing midline defects associated with their HP. Some midline abnormalities may influence complications after surgery more than others, introducing confounding into the analysis.
Furthermore, due to the small sample size and ICD-9-CM coding restrictions, the type of CL/P was not able to be elucidated. While ICD-10-CM does have a separate code for midline CL/P, the common type is seen in CwHP,13,14 the ICD-9-CM does not include this specific code. Therefore, all CLs and CPs were combined; it is unknown how many patients had, for example, a small midline cleft lip or more extensive abnormality involving the face such as a Veau IV CL/P. As these differences in orofacial cleft could affect complications rates on their own, this could be a potential source of confounding in this cohort.
Because this study used a large national database, inherent coding inaccuracies could be present where patients are erroneously included or excluded. Of particular concern in this study is the inconsistency in coding for complications of CL/P repair. Providers may vary in coding postoperative complications in their practice, suggesting they may be underestimated in this study. Furthermore, for ICD-10-CM PCs, used in KID 2016 and KID 2019, there were no specific CL/P repair codes. Therefore, codes describing repair and reposition of the upper lip, hard palate, and soft palate were queried to capture these children. We selected children 3 years and under to only include children receiving CL/P repair, but it is possible these codes included patients undergoing other procedures for other indications.
Since the KID does not contain patient identifiers, it is impossible to track patients once they have left the hospital. Therefore, if a child was discharged and returned later with a complication, those data would not have been captured. Specifically for this study, the rate of long-term complications, such as oronasal fistula or velopharyngeal insufficiency, is unknown once they were discharged from the hospital. The lack of longitudinal follow-up in this study represents another area where complications and mortality may be underrepresented in this study. Furthermore, the KID includes only inpatient claims. Therefore, children who underwent 23-h observation were not included in the analysis. 52 With some CL/P repairs occurring as an outpatient, the children in this study most likely had other comorbidities requiring inpatient hospitalization after their procedure. This fact suggests that the risk of complications in CwHP could be higher than in children with nonsyndromic or de novo CL/P. Ultimately, a more inclusive, prospective, multiinstitution observational study would further elucidate which specific CwHP are at higher risk and which postoperative complications are of most concern in this population.
Conclusion
CwHP can be medically complex due to their additional comorbidities and hormonal deficiency. CwHP undergoing CL/P repair have higher odds of experiencing complications after CL/P repair. Black children undergoing delayed CL/P in this population may further increase the risk of a perioperative complication. Clinicians need to counsel these patients appropriately preoperatively and provide additional perioperative care to attempt to reduce their elevated, multifactorial risk. Future investigation on perioperative management in CwHP is needed to reduce their complications and mortality from CL/P repair.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656221117435 - Supplemental material for Cleft Lip and/or Palate Repair in Children With Hypopituitarism: Analysis of the Kids’ Inpatient Database
Supplemental material, sj-docx-1-cpc-10.1177_10556656221117435 for Cleft Lip and/or Palate Repair in Children With Hypopituitarism: Analysis of the Kids’ Inpatient Database by Nicolas S. Poupore, Shreya Chidarala, Shaun A. Nguyen, Ronald J. Teufel, Krishna G. Patel, Phayvanh P. Pecha and William W. Carroll in The Cleft Palate Craniofacial Journal
Footnotes
Authors’ Note
Virtual Poster at 79th American Cleft Palate-Craniofacial Association Annual Meeting, March 29–April 2, 2022.
Acknowledgments
There was no financial support or funding for this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study did not require approval from the Office of Research Integrity at the Medical University of South Carolina. This study complies with the HCUP Data Use Agreement.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.