
Abstract
Objective
Palatal fistulae are challenging complications following cleft palate repair. The addition of acellular dermal matrix (ADM) to cleft palate repair has been shown to reduce fistula formation in previous studies. The use of autologous dermal graft has all the structural advantages of ADM, has less rejection and immunogenic potential, and is cost effective.
Design
A prospective study.
Participants
Patients with Group II and III cleft palate (Nagpur Classification) without prior intervention for palatal repair in the Department of Plastic Surgery at PGIMER from January 2020 till June 2021.
Intervention
The addition of autologous dermal graft for palatoplasty.
Main outcome
Outcome of the study was fistula development or exposure of dermal graft.
Results
Autologous dermal graft was harvested of average dimension of 8.73 cm2 (range 5.25-18 cm2) from groin region. Sixteen patients were included in the study. Among them, 2 patients (12.5%) developed postoperative fistula (Type III &V Pittsburgh Classification).
Conclusion
Our study showed that the rates of postoperative fistula formation are comparable with prior literature using artificial dermal matrices.
Introduction
The art of the cleft palate surgery lies in obtaining a tension free, watertight closure in 2 layers. 1 The core technique for obtaining better results involves release of aberrant muscular attachments and backward transposition of levator veli palatini muscle from its abnormal insertion. Despite the performance of a time-tested technique, palatal fistula formation remains a major surgical complication for the cleft surgeon.
Palatal fistula usually develops in areas where tension is maximum while doing repair, for example, at the junction of hard and soft palate, where cleft width is widest and tension on repair is greatest. 2 Amaratunga et al. reported a 21% fistula rate in 346 cleft palates repaired by von Langenbeck method. 3 Palatal fistulas are difficult to repair due to compromised vascularity, fibrosis, and limited mobility of palatal tissue, and have a high recurrence rate (33%-50%).
Addition of acellular dermal matrix (ADM) to the repair site is becoming quite popular in western world. Clark et al. first introduced ADM in cleft palate surgery in the year 2003. Kirschner et al. (2006) described placement of ADM for repairing palatal fistula. Initial published studies showed beneficial effect of ADM in decreasing fistula rate but subsequently published meta-analysis demonstrated insufficient evidence regarding the benefits. 4
However, the major barrier to use of ADM in a developing country like India is its availability and cost. Ultrathin ADM of a size approximating 2 × 4 cm2 piece costs about $150. 5 Autologous dermal graft has all the structural advantages of ADM and can be harvested from the patient. Further, it is devoid of rejection and immunogenic potential. It adds no cost to the surgical procedure. Hence, we envisaged a study to assess the use of autologous dermis as an interposition graft during palatoplasty.
Materials and Methods
We performed a prospective observational study, approved by Institute Ethics Committee (IEC) of PGIMER in the Department of Plastic Surgery, from January 2020 till June 2021. Informed consent was obtained from parents of all eligible candidates after a detailed discussion regarding potential advantage and risk of using autologous dermis. Subjects were examined clinically and classified according to Nagpur classification. Patients of cleft palate Group II, Group III were included in the study. Exclusion Criteria was Group I cleft lip palate, prior palatoplasty, and fistula from previous surgery, and those who were not willing for the procedure.
Surgical Technique: Palatoplasty With Autologous Dermis
A traditional Bardach's 2 long flap palatoplasty with intravelar veloplasty was done in all the cases. The mucoperiosteal flaps were undermined on the oral side. Undermining was done by inserting the elevator into the lateral incision and slipping it between the bone and periosteum until it reached the incision at the medial edge of the cleft. With blunt dissection, undermining of the flap at the posterior edge of hard palate was completed. The greater palatine pedicles were dissected to obtain greater mobility of the flap. The nasal mucoperiosteum was widely undermined using sharp periosteal elevator. After raising the flaps, the nasal layer was closed from posterior to anterior. A vomerine flap was used when necessary for complete nasal layer closure in case of the relatively wide cleft palate. Thereafter, the abnormally directed palatal muscles were freed from the posterior border of the hard palate and were dissected off the nasal mucosa with sharp dissection. The dissected muscles were reoriented medially and the muscles of the 2 sides were sutured together to form a levator muscle sling in the posterior one-third region of the soft palate. Following nasal layer closure and creation of nasal sling dermal graft was placed at the junction of hard and soft palate over nasal mucosa.
Autologous Dermal Graft Harvest
We have performed the surgery as a 2 team approach. One team operated on the palatal shelves and other team harvested the dermis simultaneously. It had the added advantage of saving time. Groin was chosen as donor site. After de-epithelization dermis was trimmed accordingly to put it over the repaired nasal layer. The donor area was closed primarily.
Placement of Autologous Dermis
Autologous dermal graft was placed over nasal side and sutured with absorbable suture Vicryl 4-0 (Figure 1). Resorbable sutures were used to stabilize dermal graft against nasal mucosa centrally and at corners posteriorly. Most cases dermal graft was tailored and trimmed according to cleft size and denuded area so that graft completely covered by vascularized oral mucoperiosteal flap. It was confirmed that dermal graft lies stable and flat without undulation. Hemostasis was achieved to prevent blood collection or hematoma formation surrounding the dermal graft. In all the cases, a complete layered closure was achieved.
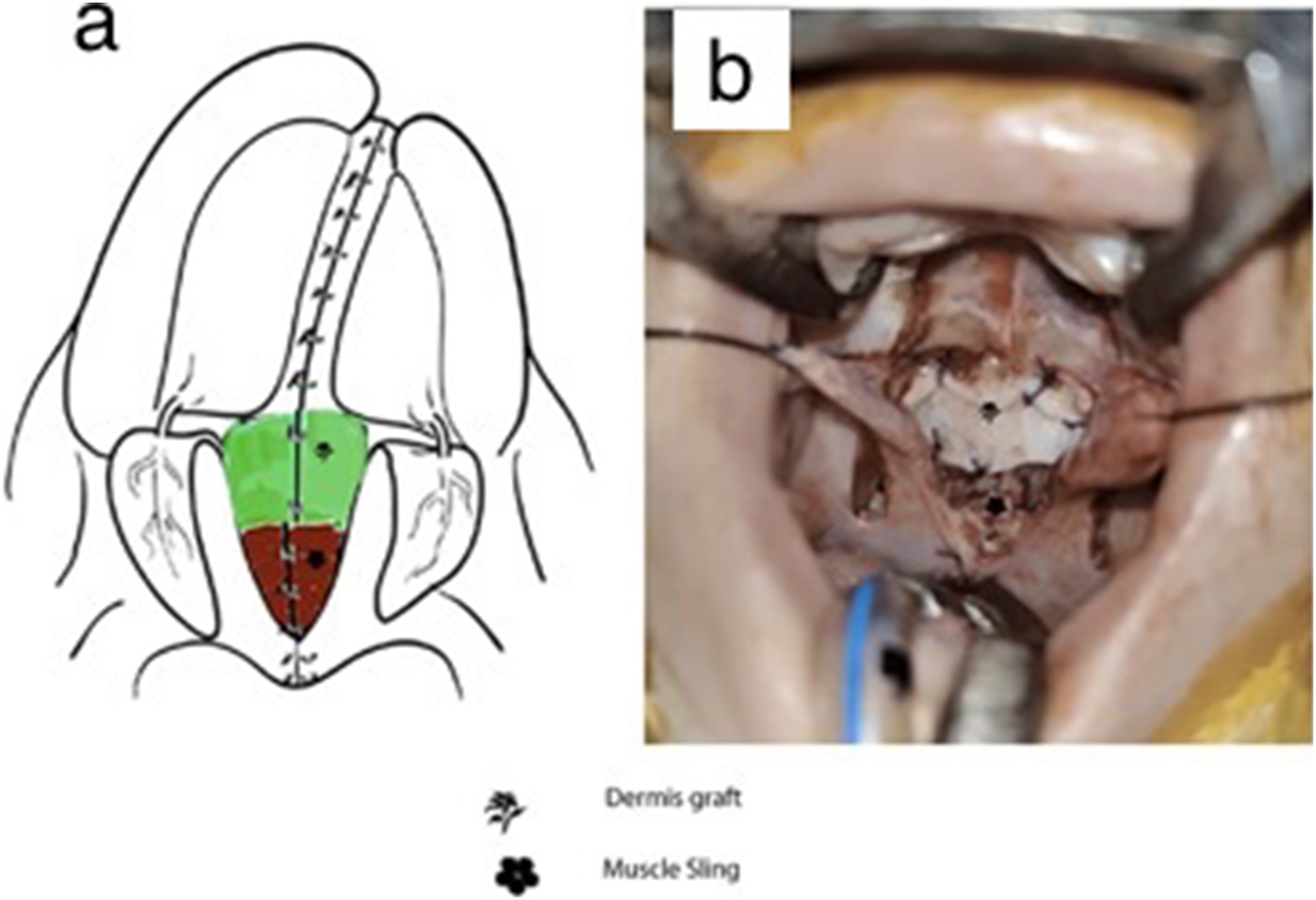
Placement of autologous dermis over the repaired nasal layer at the junction of soft and hard palate: (a) green square depicting placement of autologous dermis (left); (b) clinical picture (right).
Postoperative Management and Follow-up
The children were discharged within 48 h postoperatively. An oral antibiotic, Amoxicillin 30 mg/kg was prescribed for 5 days. Regular diet was resumed 2 to 3 weeks postoperatively. The repair sides and palate were assessed postoperatively and followed up on outpatient basis. Due to COVID 19 pandemic and lockdown status in the country, a few patients were followed up telephonically also. Presence of any infection or fistula development or exposure of dermal graft, donor site healing (Figure 2) was noted in follow-up.
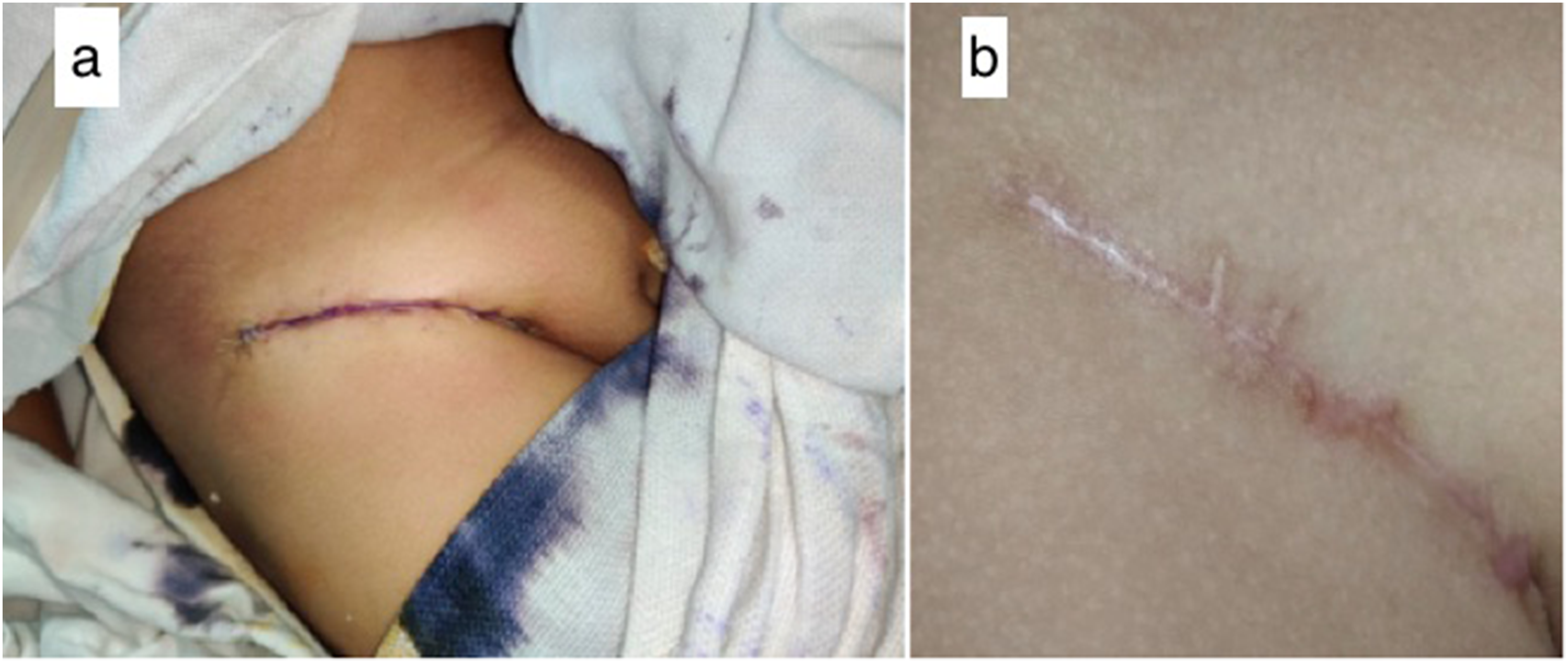
Donor area: (a) at the time of primary closure; (b) at 3 months follow-up.
Statistical Analysis
The statistical analysis was carried out using Statistical Package for Social Sciences (SPSS) software version 22. Qualitative and quantitative data was analyzed on the basis of data characteristics.
Results
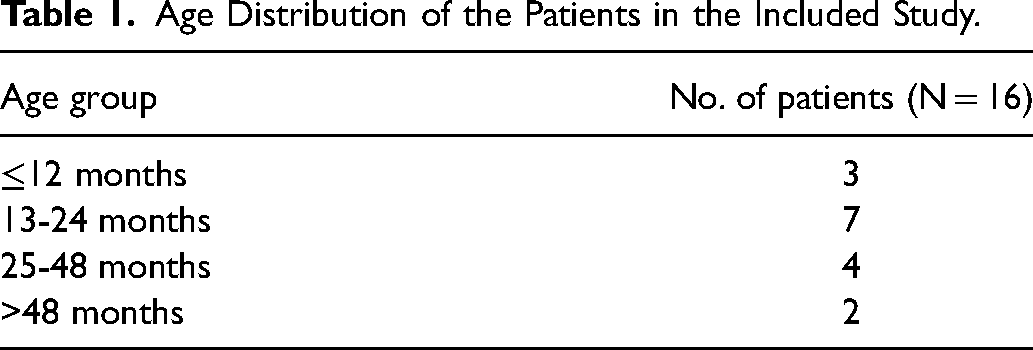
After assessing eligibility as per inclusion criteria, a total of sixteen (16) patients of cleft palate of Group II and Group III (according to Nagpur Classification) undergoing palatoplasty were recruited into the study (Table 1).
Age Distribution of the Patients in the Included Study.
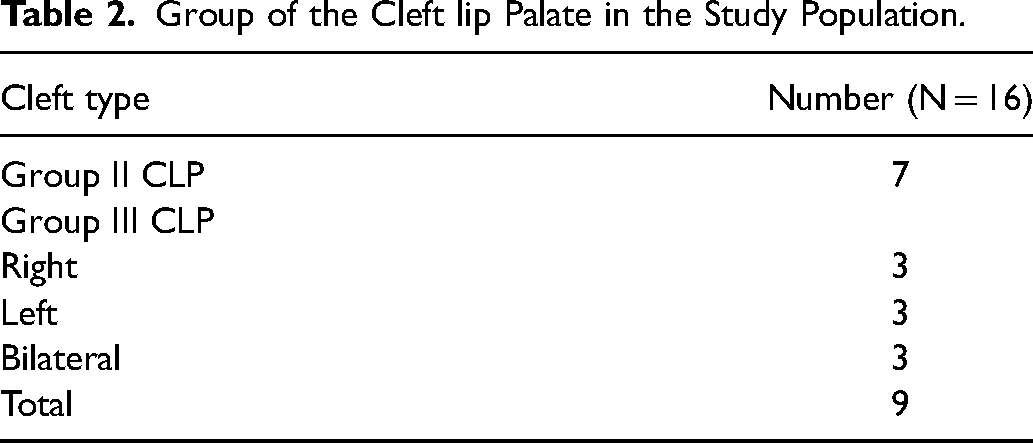
Among the cohort, the number of female children was 10 (62.5%) and male children was 6 (37.5%). The median age of the patient undergoing surgery in the present study was 22.5 months (range: 12 months-224 months). Out of 16 cases, 1 patient had Pierre Robin sequence; 1 patient had Total Anomalous Pulmonary Venous Return who underwent correctional surgery before the palatoplasty. In our study, 7 patients (43.75%) had Group II cleft palate and 9 patients (56.25%) had Group III cleft lip palate (Table 2). The 2 long flap palatoplasty technique was adopted in all the patients undergoing palatoplasty repair. The vomerine flap was performed in 5 patients for nasal layer closure. The mean duration of surgery was 119 min (range: 80-140 min). Autologous dermal graft was harvested of average dimension of 8.73 cm2 (range: 5.25-18 cm2) from groin. The mean postoperative hospital stay was for 2 days. There was no postoperative complication noted during hospital stay. The average follow-up duration was 10.18 months (range: 3-19 months). On follow-up, 2 patients (12.5%) developed oronasal fistula. The postoperative palatal fistula was graded according to Pittsburgh fistula classification. One patient developed palatal fistula at hard palate and the soft palate junction and the other one developed fistula at the primary palate and secondary palate junction.
Group of the Cleft lip Palate in the Study Population.
Discussion
Cleft lip and palate is a common congenital anomaly. One of the major goals of evolution of various surgical techniques was the prevention of fistula formation. The reported incidence of postoperative fistula following palate repair ranges from 11% to 23%. 3 Prevention is key because it is difficult to repair a fistula. Recurrence rate after fistula repair is as high as 65%. Further factors that compound the risk are the atrophic nature of mucosa, and the inadequacy of muscle layer centrally at the junction of hard palate and soft palate. 6
ADM as interposition graft in between the repaired nasal and oral mucosal layer has been used in the last 2 decades in many studies. ADM is derived from cadaveric human skin. Epidermal and dermal cellular elements are removed, the original dermal collagen and protein matrix retained. The resultant effect is a minimization of inflammation and rejection. The structure of the matrix is an acellular lattice consisting of collagen, elastin, glycosaminoglycan, and vascular channel. 7 The additional benefits are that the extracellular dermal matrix allows the allograft to have a good tensile strength, minimal contraction, and a provision of scaffold for cellular ingrowth and epithelization. Host cell infiltration, fibroblasts, and other precursor cells become incorporated into the matrix which results in revascularization. 8 Extending this premise, the autologous dermis has all the advantages of being non-immunogenic, no fear of the phenomenon of rejection, economic benefit, ease of harvest in a customized dimension, and no requirement for storage. Autologous dermis can serve as a scaffold, reducing wound contraction and scarring, which itself is beneficial to reduce the incidence of fistula formation. The dermal graft mechanically provides a fourth layer of tissue as a part of the deeper layer of repair. Other autologous options might include temporalis fascial grafts or fascia lata, both of which may have better donor site scars.
To the best of our knowledge, we have not come across similar studies involving autologous dermal graft in palatoplasty. We have used 2 long flap palatoplasty technique in all the cases, which usually allows better visualization of the surgical field so that dermal graft adaptation straightforward. With 2 long flap technique, closure of nasal and oral mucosal layer is technically easy and reliable and producible. Vomerine flap was used for nasal layer closure in cases where there was tissue deficiency. In the present study, we have performed the vomerine flap in 5 cases to repair the nasal layer. An adequately done nasal layer closure prevents exposure of dermal graft on the nasal side. For the oral side, complete closure of the long flaps was adequate to cover the dermal matrix with vascularized tissue. The dermal graft itself has mechanical and biological advantage while placing it in between repaired nasal and oral mucosal layer. It acts as mechanical barrier in between potential breakdown areas of overlapping suture line. It also provides thickness to already thinned areas caused by extensive muscle dissection and tensor aponeurosis release. It also takes care to cover small holes on nasal mucosa, which occasionally occur during meticulous dissection of the levator muscle. The dead space in between repaired nasal and oral mucosal layers is obliterated by dermal graft. The dermal graft following total integration may produce lesser amount of scar and decrease contracture. By this virtue, dermal graft placement is advantageous in cases of tight closure. 1
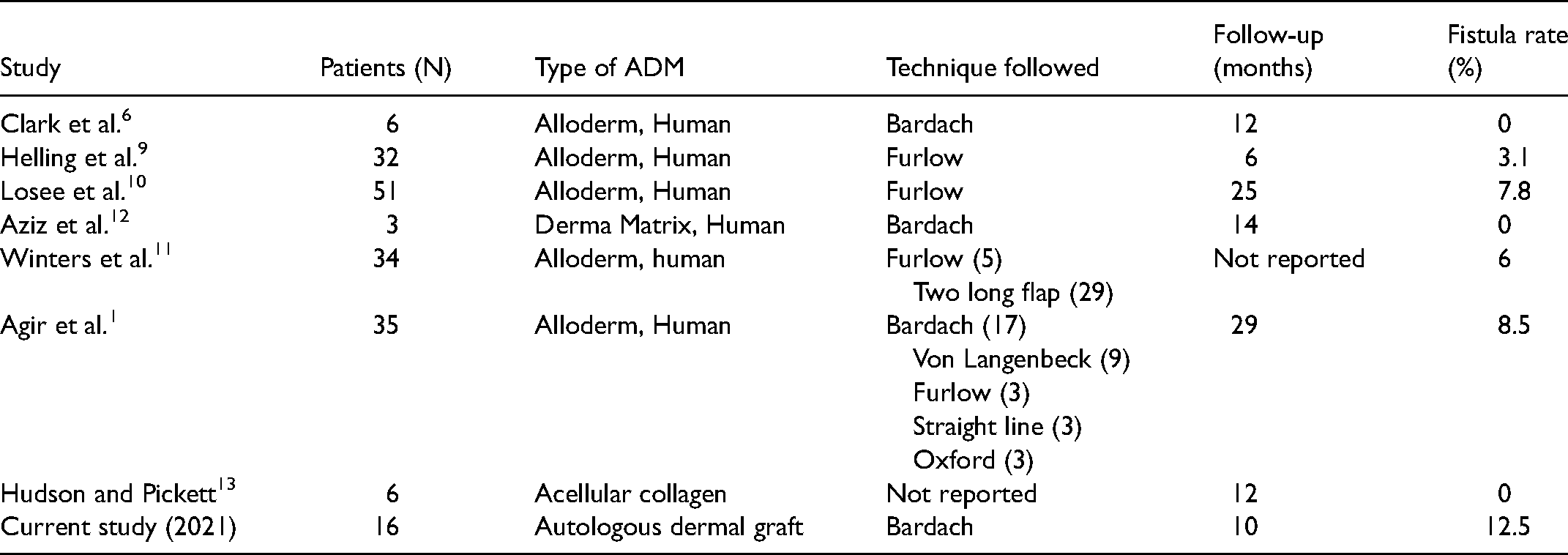
The recommended time of cleft palate repair is 9 to 12 months. 8 However, due to the pandemic scenario, the median age of the patient undergoing surgery in the present study was 22.5 months. Among them, 2 patients (12.5%) developed postoperative fistula. We have not found similar studies, which have done using autologous dermis. The reported incidence of fistula using ADM, Helling et al. 9 in their study of 32 patients undergoing primary cleft palate repair using ADM showed a fistula rate of 3.1%. Loose et al. 10 in a similar study of 51 patients showed a fistula rate of 7.8%. Winters et al. 11 studied 34 patients and found a fistula rate of 6%, whereas Agir et al. 1 had an 8.5% fistula rate using ADM. Remarkably, Clark et al., 6 Aziz et al. 12 , and Hudson et al. 13 had no fistula while using ADM in their cases.
A summary of the above-mentioned studies is described below.
Summary of Outcomes of Primary Cleft Palate Repair Using Acellular Dermal Matrix (ADM)
We also noted that even if there was a breakdown of oral layer, the underlying dermal layer permitted more efficient epithelialization and the fistula eventually became exceedingly small. This was confirmed in one case where the fistula was sequentially followed up over a period of 6 months. The dermal graft donor site healing was uneventful in all the patients.
Limitations
The study was initially planned for a larger cohort of cases, but because of Covid 19 pandemic, very few cases could be operated. We could include only 16 cases in our study. This small number cannot be used to form an opinion on the use of dermal autograft, however we feel that the results so far have been quite encouraging. The finding and the novelty of this study deserve wider analysis in the future. Further studies might also offer insight beforehand, in identifying the patients who could be the ideal candidates for the dermal graft interposition. However, the results of the present study need to be extrapolated with larger population with a control group and compared with data of different centers.
Conclusion
The placement of a dermal graft usually does not take significant additional time with minimal donor site morbidity. The rates of fistula formation are comparable to pre-existing published results with artificial dermal matrices. This study is validated by the fact that the autologous dermis retains all biological advantages of commercially available ADM along with economic feasibility, non-immunogenicity, and customisability of graft. It is safe to assume that placement of a dermal graft aids in structural integrity in those patients having a paucity of tissue at the junction of hard and soft palate. A longer follow-up in a larger subset of patients will elucidate the reasons of fistula formation.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656221121044 - Supplemental material for Outcome of Nasal Layer Reinforcement With Autologous Dermis in Cleft Palate Repair on Postoperative Fistula Formation
Supplemental material, sj-docx-1-cpc-10.1177_10556656221121044 for Outcome of Nasal Layer Reinforcement With Autologous Dermis in Cleft Palate Repair on Postoperative Fistula Formation by Subhendu Khan, Jerry R. John and Ramesh K. Sharma in The Cleft Palate Craniofacial Journal
Footnotes
Authors’ Note
It is a prospective observational study, approved by Institute Ethics Committee (IEC) of PGIMER and was performed in the Department of Plastic Surgery, from January 2020 till June 2021.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.