
Abstract
Background
California Senate Bill 630 (SB630) enacted statutorily mandated health plan coverage for orthodontic care of patients with cleft palate and craniofacial anomalies in 2009, which was effective from July 1, 2010. In this qualitative analysis, third-party compliance with SB630 in a university-based cleft and craniofacial orthodontic program is evaluated.
Methods
Privately insured patients that experienced a coverage delay or denial of orthodontic treatment for cleft lip and palate in the University of California, San Francisco Cleft and Craniofacial Orthodontic Program between July 1, 2010 and October 28, 2020 were identified. A thematic analysis of reasons for delay or denial was conducted.
Results
Nearly three quarters of patients experienced coverage delay and/or denials. The most common reason given was that services were not covered.
Conclusions
Despite state-mandated coverage, inappropriate denials of orthodontic care for patients with cleft lip and palate by private insurers persist in California.
Introduction
Children born with cleft lip and/or palate (CL/P) require timely orthodontic care to achieve proper occlusion, function, and esthetics as an integral part of the habilitation and rehabilitation process restoring their physical and emotional well-being 1 . Orthodontic care may include preoperative treatment, palate expansion, dentition alignment, and malocclusion correction, and typically occurs in 2 phases 2 . Around 7 to 9 years of age, patients begin phase I orthodontic treatment in preparation for alveolar bone graft surgery which is typically done around 8 to 10 years of age before the eruption of the permanent canine. The main treatment objective during phase I orthodontic treatment is to prepare the maxillary segments for available grafting which is essential to provide bony continuity of the maxilla. The timing of alveolar bone grafting is critical typically performed around 8 to 10 years of age before the eruption of the permanent canine into the cleft defect. Between the ages of 12 to 14 years, after the eruption of the permanent second molars, patients receive phase II orthodontic treatment with or without the need for bone-anchored maxillary protraction in preparation for lip and nose revision surgery 2 . However, if the patient is a candidate for orthognathic surgery due to maxillary hypoplasia, orthodontic treatment is typically delayed closer to growth completion between the ages of 16 to 18 years 3 .
Coverage denials by private insurers are a significant barrier to delivering critical orthodontic care to children with CL/P4–6. After July 1, 2010, California Senate Bill 630 (SB630) statutorily mandated all health care service plan contracts to cover reconstructive surgery, which includes “medically necessary dental or orthodontic services that are an integral part of reconstructive surgery for cleft palate procedures” 7 . Therefore, since this mandate, every patient with medical insurance coverage diagnosed with CL/P should have had the opportunity to have orthodontic treatment in preparation for reconstructive surgery covered by medical insurance plan contracts.
The UCSF Cleft and Craniofacial Orthodontic Program see patients from more than 25 Northern California counties for orthodontic care related to CL/P. When submitting medical claims, UCSF created a protocol that was published on the California Association of Orthodontists (CAO) website to include (1) a letter from the treating clinic emphasizing the medical necessity of the reconstructive procedure(s), (2) a copy of any photos, (3) the treatment plan accompanied by the estimated cost, and (4) a copy of SB630 for reference, 8 . In some cases, CAO recommends including relevant scans such as panoramic and cephalometric radiographs, a report from the craniofacial team including a recommendation for medically necessary orthodontic treatment, and for HMO insurance plans, a copy of letter of agreement, and a referral from primary care. In all cases, it is advisable to document all correspondence with the insurer. CAO developed these recommendations to address coverage denials by encouraging a systematic submission process. Since the enactment of SB630, the clinic has continued to experience third-party denials of medically necessary orthodontic coverage for CL/P patients. The purpose of this study was to systematically assess medical claims to determine rationales provided for the delay and/or denials of medically necessary orthodontic services.
Methods
Patients that received medically necessary orthodontic treatment in the UCSF Cleft and Craniofacial Orthodontic Program between July 1, 2010 and October 28, 2020 were identified. Two investigators (RA, LH) conducted a review of the patients’ dental records in the axiUm electronic clinical management system. Data were reviewed in 4 axiUm modules: Patient/Patient card (third-party insurance affiliate and plan), electronic health record (chart notes), transactions (financial notes, general transactions, payments), and attachments/consents (ortho documents, scanned documents). Patients who: (1) initiated and completed medically necessary orthodontic treatment between July 1, 2010 and October 28, 2020; (2) had these services billed to a private medical insurance provider; and (3) experienced a claim delay or denial were identified for further analysis. Services billed to dental or public medical insurance providers were excluded.
The research team created a data abstraction instrument in Microsoft Excel. Data abstracted included insurance claims submitted for pre-authorization or treatment for medically necessary phase I and phase II orthodontic care, medical insurance provider, outcome of insurance claim, reason for claim delay or denial, and documentation of telephonic or written correspondence between the clinic and insurance companies related to the claims. The reviewers manually abstracted and evaluated the data in tandem. Each patient's record was assessed 3 times. A third expert investigator (SO) verified the accuracy of the abstracted and evaluated data by conducting an audit on 10 randomly selected patients and cross-referencing it with the 2 reviewers (100% agreement). Reasons provided by medical insurance providers for delay or denial of claims were organized into themes. Study procedures were approved by the UCSF Institutional Review Board (#20-32563) and the requirement for HIPAA Authorization was waived for all subjects.
Results
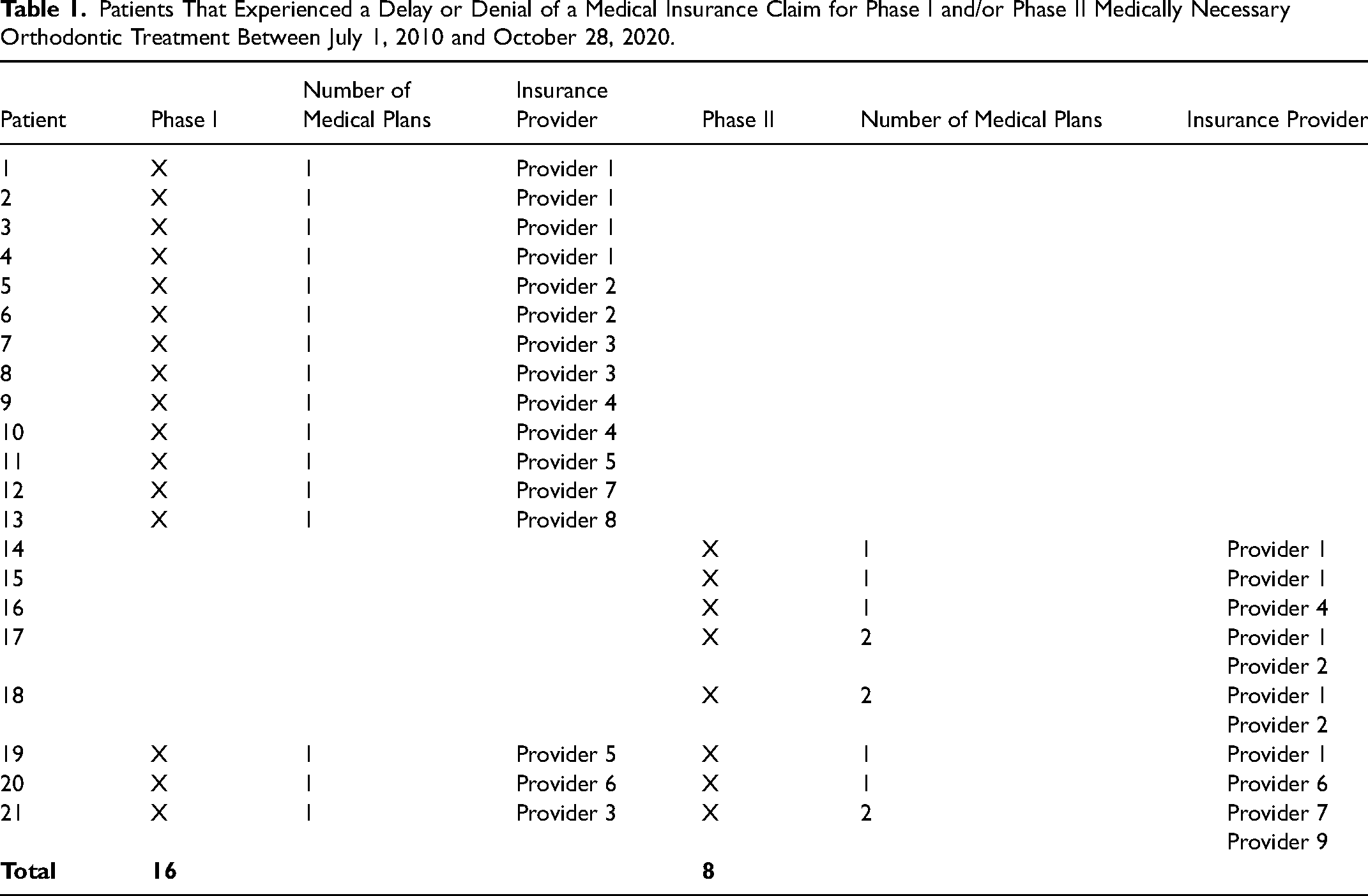
Twenty-nine patients had services billed to a private medical insurance provider for medically necessary orthodontic treatment completed in the UCSF Cleft and Craniofacial Orthodontic Program between July 1, 2010 and October 28, 2020. Twenty-one patients experienced a delay and/or denial of an insurance claim (Table 1): 13 related to phase I treatment only, 5 related to phase II treatment only, and 3 related to phase I and phase II treatment. Delayed/denied claims were received from 9 different medical insurance providers.
Patients That Experienced a Delay or Denial of a Medical Insurance Claim for Phase I and/or Phase II Medically Necessary Orthodontic Treatment Between July 1, 2010 and October 28, 2020.
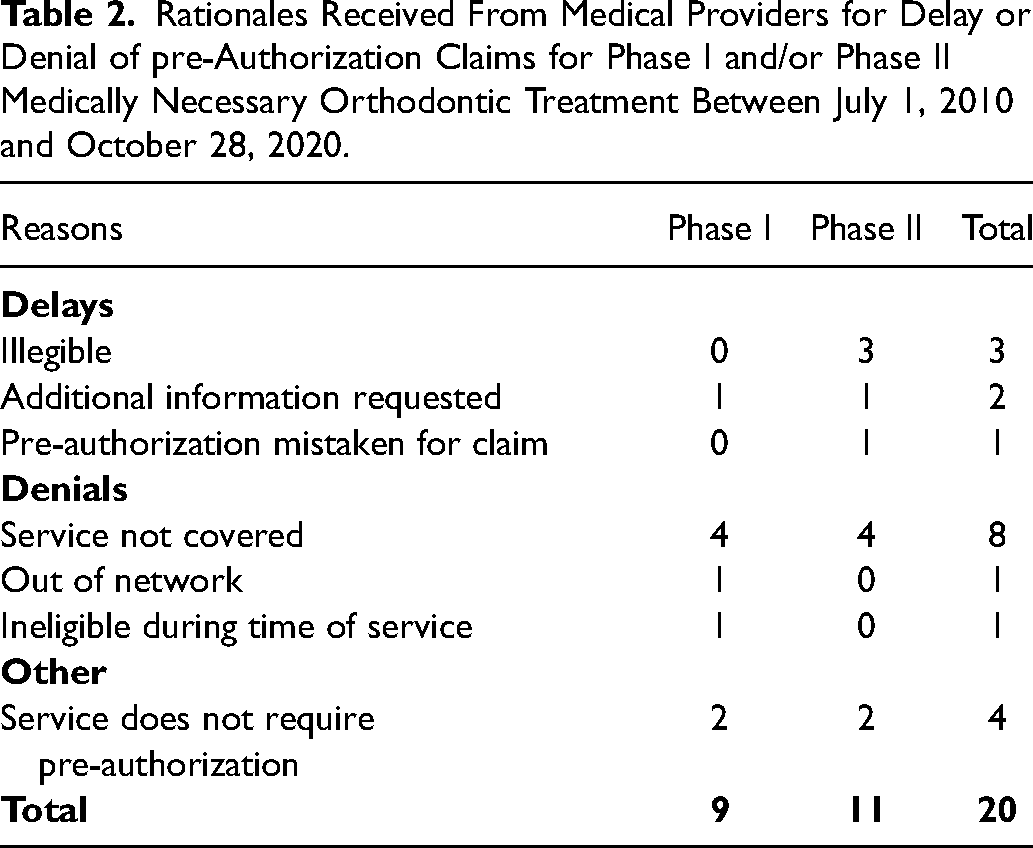
Twenty pre-authorization claims (9 for phase I treatment, 11 for phase II treatment) were delayed or denied (Table 2). Reasons for delays included that the claim was illegible (3 claims), more clinical information needed (2 claims), and in one instance, the pre-authorization claim was mistaken for a treatment claim. Reasons for denials included that the service was not covered (8 claims), that the provider was out of network (1 claim), and that the member was ineligible for coverage at the time of service (1 claim). Four claims did not receive pre-authorization with the rationale that pre-authorization was not required. Further analysis of clinic follow-up documentation revealed that the denials due to out of network and ineligibility reasons were invalid. The out-of-network patient had received documented approval to receive care at UCSF because the clinic was the only craniofacial orthodontic provider within a 25-mile radius of the patient's home. The patient deemed ineligible was later found to be eligible.
Rationales Received From Medical Providers for Delay or Denial of pre-Authorization Claims for Phase I and/or Phase II Medically Necessary Orthodontic Treatment Between July 1, 2010 and October 28, 2020.
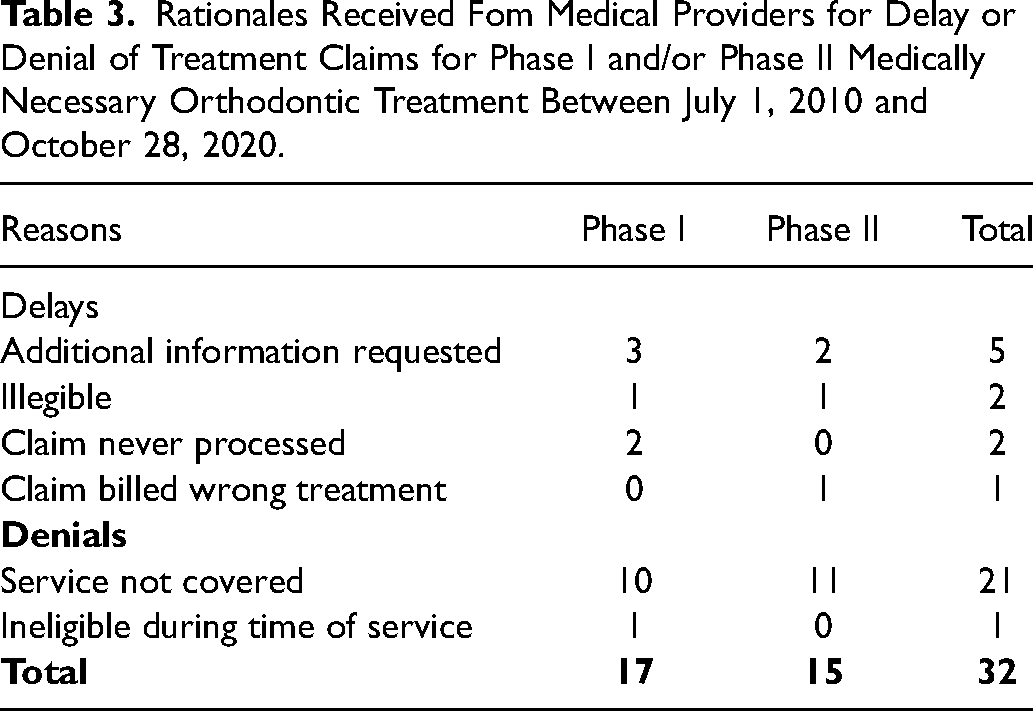
Thirty-two treatment claims (18 for phase I treatment, 15 for phase II treatment) were delayed or denied (Table 3). Reasons for delays included requests for additional information (5 claims), claim was illegible (2 claims), claim never processed (2 claims), and claim billed out for incorrect phase of treatment (1 claim). Reasons for denials included dental services not covered (21) and member ineligible for coverage at time of service. Further analysis of clinic follow-up documentation revealed that the denial for ineligibility was invalid, and it was later found that the patient was eligible.
Rationales Received Fom Medical Providers for Delay or Denial of Treatment Claims for Phase I and/or Phase II Medically Necessary Orthodontic Treatment Between July 1, 2010 and October 28, 2020.
Discussion
Although California SB630 has statutorily mandated health coverage of medically necessary dental or orthodontic services that are an integral part of reconstructive surgery for CL/P, 74% of privately insured patients seen for these services at the UCSF Cleft and Craniofacial Orthodontic Program between July 1, 2010 and October 28, 2020 have experienced delays and/or denial of coverage. Delays and denials were received from 9 different insurance companies operating in California. The most common reason given was that dental services were not covered. These results reflect continued challenges in billing dental services to medical insurance companies, which often require varying medical billing methods and written explanations to accompany the claim. The results also indicate routine, systematic denials in opposition to SB630. To overturn these denials, some patients had success through submitting additional supporting documents including radiographs, photographs, and study models numerous times, appealing the denial, and/or ensuring proper response within the timeframe specified by the insurance company in question. However, several patients were thorough in their resubmission process and were never able to rectify their denial.
California is one of the 32 states with mandates addressing the health care needs of children with CL/P 9 . The purpose of mandating specific services is to increase the medical coverage of the specified services. However, as this study indicates, mandating services is not enough to ensure insurance company compliance. One potential remedy would be for the state of California to institute an oversight mechanism. For example, the Department of Managed Health Care conducts a routine medical survey of each licensed full-service health plan required by California every 3 years to ensure compliance with the Knox-Keene Act to measure a health plan's compliance related to quality assurance, grievances and appeals, access and availability, utilization management, and overall plan performance, 10 . Compliance with SB630 could be assessed in a similar manner, in conjunction with the survey related to the Knox-Keene Act. This study indicates that efforts to enact a federal bill to mandate insurance coverage for children with congenital anomalies could also be a necessary step to reduce coverage denials 4 . A federal mandate would standardize medically necessary coverage and protocols.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cristin Kearns provided consulting services for Milliman Inc., a subcontractor with the California State Department of Managed Health Care between 2019 and 2020.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.